Abstract
Dental anxiety results in the neglect of oral hygiene and poor oral health, requiring an accurate screening tool for dental practitioners to evaluate dental anxiety. The Modified Dental Anxiety Scale (MDAS) is frequently used cross-culturally. The present study aimed to assess the reliability and validity of the Hebrew version of the MDSA. A total of 553 (mean age 35.87 years, SD = 13.14) Israeli participants were recruited through means of social media, mailing lists, and forums. The sample was randomly divided into two population sets. Dental anxiety was evaluated using the Hebrew version of the MDAS. The psychometric evaluation consisted of exploratory factor analysis (study 1, n = 274) and confirmatory factor analysis (study 2, n = 279). Cronbach’s alpha coefficient was used to assess internal consistency. Results showed high internal consistency (0.93) for the Hebrew version of the MDAS. Confirmatory factor analysis showed a single factor solution. Findings demonstrated 13.4% of Israeli participants with dental anxiety. Younger participants, females, participants with lower education, lower income, and more religious participants reported higher dental anxiety. In conclusion, the Hebrew version of the MDAS demonstrated high reliability and validity. It is recommended to use the Hebrew version of the MDAS to evaluate dental anxiety in Israeli dental settings.
1. Introduction
Dental anxiety may be described as an abnormal fear or dread of visiting the dentist, and unwarranted unease during any dental procedures []. Dental anxiety, at high intensity, is considered to be a specific phobia, as defined in both the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) [] and the International Statistical Classification of Diseases and Related Health Problems 11th Revision (ICD-11) []. Individuals suffering from elevated levels of dental anxiety are susceptible to a recognizable vicious cycle: their dental anxiety and fear lead to poor attendance at dental practices, which in turn leads to symptom-driven treatment, leading to increased anxiety and fear responsible for avoidance of dental treatment. Dentally anxious patients consequently avoid dental appointments [], neglect oral hygiene, and demonstrate poor oral health (e.g., high rates of dental caries) [,,,,].
In a recent review, Carter (2014) suggests five pathways through which dental anxiety may ensue: Cognitive conditioning, vicarious, verbal threat, informative, and parental. The author (Carter, 2014) also claimed that these pathways may be affected by different etiological factors such as genetic vulnerability, cognitive biases, cognitive content, operant conditioning, preparedness, negative affectivity, and anxiety vulnerability.
Assessment of dental anxiety can be favorably achieved using self-reported measurements []. Dental anxiety questionnaires completed by those who experience psychological difficulties in receiving any dental procedures enable dental care providers to make informed decisions regarding suitable treatment plans, considering their patient’s mental and psychological well-being [,,]. Despite the importance of such questionnaires, most dental care providers tend to trust their own clinical experience when estimating their patients’ levels of dental anxiety, perhaps due to their belief in their capability to ‘diagnose’ a dentally anxious patient or their reluctance to incorporate an additional form to their routine check-ups. Nonetheless, evidence has been reported to support the use of dental anxiety assessments in routine care for patient benefit [].
Factors that govern the usage of dental anxiety questionnaires in clinical practice and epidemiological studies are: number of questions, complexity, validity, reliability, and reproducibility []. Different self-reported questionnaires measure dental anxiety, a popular measurement being the Corah’s Dental Anxiety Scale (CDAS). It is a four-item questionnaire. It has been criticized for omitting the assessment of the respondent’s view to dental anesthesia and for having a complex answering scheme []. Studies that have evaluated dental anxiety among the Israeli population have frequently used the CDAS [,], showing mixed results regarding the gender effect on dental anxiety levels. Blumer et al. (2018) found that among post-graduate pediatric Israeli staff (instructors and students), females presented higher rates of dental anxiety, while Ratson et al. (2016) found that gender had no significant effect on dental anxiety levels among Israeli adults.
In order to overcome such limitations, a new tool was suggested in 1995, the Modified Dental Anxiety Scale (MDAS) [] was designed. The MDAS is a five-item questionnaire, with an additional single question regarding local anesthesia, along with uniform responses, thus simplifying the task for the respondent, and assisting the clinician in interpreting item scores. Each item of the MDAS has five consistent responses ranging in increasing order from “not anxious” to “extremely anxious”, with accompanying scores ranging from 1 to 5, corresponding to dental anxiety of increasing severity []. The results are then summed together to construct a Likert scale with a minimum score of 5 and a maximum score of 25 []. A score of 19 or higher is the cut-off that indicates an individual with elevated risk for dental anxiety []. The usage of the MDAS offers various advantages such as being simple, short completion time, and the process of completion does not increase the respondent’s anxiety []. The MDAS also has good cross-cultural validity [], and has been translated into many languages [,,].
In summary, there are currently no studies evaluating dental anxiety in the adult Israeli population using the MDAS, as it has yet to be translated to Hebrew and validated. The current study aims to validate the Hebrew version of the MDAS to provide Israeli dental staff an important tool to better estimate their dental patients’ levels of dental anxiety. Providing a dental treatment plan tailored to one’s well-being may aid in easing dental anxiety and eventually improve both the physical (dental) and psychological status of the patient, with additional benefits such as improvements in quality-of-life measures.
In the present study, the psychometric properties of the Hebrew version of the Modified Dental Anxiety Scale are presented. Study 1 aimed to perform exploratory factor analysis, whereas Study 2 aimed to perform confirmatory factor analysis. Both studies were conducted on a convenience sample from the adult Israeli general population.
The overall purpose of this study was to validate the Hebrew version of the MDAS questionnaire. The English version of the MDAS constructed in 1995 [] and reported a Cronbach’s alpha of 0.93 [,]. The MDAS incorporates a Likert rating scale with five possible responses to each question. The questions are related to the respondents’ emotional reactions to a visit to a dental clinic while waiting in its waiting hall, drilling, scaling, and prior to a local anesthesia injection. The responses range from ‘not anxious’ (scoring 1) to ‘extremely anxious’ (scoring 5). A Hebrew language version was produced and back translated by the authors (MS and MB-E). A native English speaker (LK-G) back translated the questionnaire into English and her version was compared with the version produced by the authors. Differences among the versions were resolved by consensus between the authors. In addition, an Israeli dentist and doctor (psychiatric resident) gave independent assessments of the translations.
2. Materials and Methods
2.1. Sampling and Procedure
We used an internet platform to conduct the survey (Google forms) after gaining approval for the study from the Institutional Review Board of the authors’ (MS, LG-K, MB-E) university. Inclusion criteria included Israeli adults older than 18 years of age, with exclusion criteria being younger than 18 years of age. During the period of 13 November to 7 December 2019, participants were approached using social media (Facebook, WhatsApp), dedicated mailing lists (MS), and forums (n = 553). The mean age of these participants was 35.87 years (SD = 13.14, range = 18–76), 62.9% were female (n = 348), 69.6% (n = 385) were in a committed relationship, 58.2% (n = 322) were secular in their degree of Judaism spirituality, and mean years of education was 14.99 (SD = 3.09). Each participant signed an electronic informed consent form. The sampling and procedure in Study 2 was identical to Study 1.
2.2. Measures
A basic socio-demographic questionnaire was used for the following: age (coded in years), gender (coded as ‘1 = male, 2 = female’), marital status (coded as ‘1 = not being in a committed relationship, 2 = being in a committed relationship’), years of education (coded in years), degree of Judaism spirituality (coded as ‘1 = secular, 2 = traditional, 3 = religious, 4 = ultra-orthodox’), and level of income relative to the average salary in Israel (coded as ‘1= highly below average, 2 = lower than average, 3 = average, 4 = higher than average, 5 = much higher than average’). In addition, as depicted previously, the Hebrew MDAS scale items were utilized. The measures in Study 2 were identical to study 1.
2.3. Statistical Analysis
Descriptive statistical analysis was conducted for sociodemographic factors. In addition, an exploratory factor analysis (EFA) was conducted (principal component analysis) using Horn’s Parallel Analysis (paran procedure) including the 5 MDAS items (items were rated on a 5-point scale ranging from 1 = ‘not anxious’, to 5 = ‘extremely anxious’), thereby producing a basic component matrix followed by an orthogonal (varimax) rotation method if more than a single factor indicated. Confirmatory factor analysis was run (sem procedure) with the conventional methodology of setting a single item to unitary loading to ‘scale’ the measure. Standardized solutions were requested and modification indices were examined for evidence of correlated residual errors. The total sample was randomly divided into two separate sub-samples for EFA (study 1, n = 274) and confirmatory factor analysis (CFA, study 2, n = 279). Data were analyzed utilizing STATA 15 (Stata CORP, College Station, TX, USA). Alpha level was 0.05 (2 sided) for all tests. The sample was divided into two separate sub-samples in order to better evaluate factor analyses. If both EFA and CFA were to be conducted on the same total sample, its results would be difficult to interpret as very similar results would be obtained. Thus, in order better interpret when conducting factor analyses, the total sample was divided.
The purpose of Study 2 was to conduct the confirmatory factor analysis (CFA) of the MDAS in the second sub-sample (n = 279). We performed a confirmatory factor analysis (CFA). The analysis was conducted using STATA 15 (Stata CORP, College Station, TX, USA). Overall goodness of fit for the analysis of the proposed unidimensional measurement model was assessed by a variety of indices: Tucker–Lewis index (TLI, recommended result should be higher than 0.95); comparative fit index (CFI, recommended result should be higher than 0.95); Standardized root mean square (SRMR, cut-off value 0.08 or below); Coefficient of determination (CD, ranged between 0 and 1 with closer to 1 suggesting better model fit); and the root mean square error of approximation (RMSEA, recommended result should be lower than 0.1) (for more information about the goodness of fit cutoffs, see [,,,,,]). Following the CFA, we conducted a correlation matrix for all the measures used in each sample. Beyond that, we conducted a regression analysis to learn of the association between demographic variables and dental anxiety. The demographic factors were age, sex, relationship status, education, income, and religiosity. The dependent variable was dental anxiety. An a priori test revealed no multicollinearity. The tolerance ranged from 0.634 to 0.905 and the Variation Inflation Factor (VIF) ranged from 1.105 to 1.577.
3. Results
3.1. Exploratory Factor Analysis—Component Matrix
Descriptive statistics about basic sociodemographic factors are presented in Table 1.

Table 1.
Descriptive presentation about basic sociodemographic data among current study participants (n = 553).
The cut-off for elevated risk for dental anxiety in the MDAS is 19 and above. In the current study, 74 participants out of 553 showed elevated risk for dental anxiety resulting in 13.4% of the sample.
The results of the linear regression showed that the model was significant. The R was 0.343 and the R2 was 0.118 (F change = 12.141; DF = 6545; p < 0.0001). The results revealed the dental anxiety was associated with younger age (β = −0.118; t = −2.563; p = 0.011), being a female (β = 0.204; t = 4.825; p < 0.001), and being more religious (β = 0.122; t = −2.829; p = 0.005). Relationship status, education, and income were not found to be associated with dental anxiety.
The exploratory factor analysis result revealed only one factor. In order to ensure that we did not have more than one concept underlying the Hebrew version of the MDAS, the exploratory factor analysis of the five-item MDAS found only one eigenvalue was greater than 1.00: 3.82 (explained variance = 78%), with a smooth continuous drop for the remaining eigenvalues. This feature made the clearest break in the Scree Plot between the first and second factor, again highly suggestive of a one-factor solution. See Table 2 and Figure 1 for further information.
Table 2.
Exploratory Factor Analyses of the Hebrew Version of MDAS Factor Loadings (Study 1).
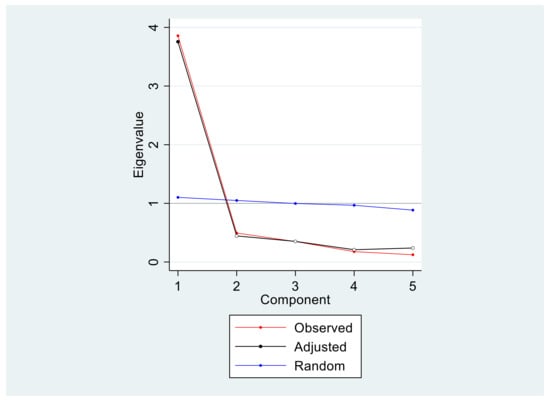
Figure 1.
Scree plot (Study 1). As can be noted, one-component solution was found for the Hebrew version of the MDAS. The observed (red) and adjusted (black) both illustrate and support the one-component solution.
3.2. Confirmatory Factor Analysis (CFA)
The results of the CFA showed that a one-factor solution showed a good fit. This solution incorporated a single correlated error into the model as indicated by a high modification index for this covariance parameter estimate (>10). See Table 3 for further information. The Cronbach’s alpha for the MDAS in the current study was 0.93.
Table 3.
Model Evaluation Overall Fit Measurement for the Hebrew Version of MDAS, data analyzed with STATA 15.
4. Discussion
Dental anxiety can result in the negligence of oral hygiene and poor oral health [,,,]. An accurate screening tool is advocated that will easily meet the needs of dental care providers to make informed decisions regarding suitable treatment plans with patients with dental anxiety. The MDAS has many advantages for such screening [], has good cross-cultural validity [], and has been translated into many languages [,,]. Nevertheless, there is no translated and validated Hebrew version to date. The present study, therefore, examined the psychometric properties of the Hebrew version of the MDAS. The first study aimed to determine the dimensionality of validate the Hebrew version of the MDAS questionnaire, while the second study performed confirmatory factor analysis.
A factor analysis of demonstrated singular dimensionality of the Hebrew version of the MDAS. Results revealed that Cronbach’s alpha coefficient for the Hebrew version of the MDAS was high (0.925–95% CI’s 0.905–0.941), which is similar to the Cronbach’s alpha value of the Italian (0.92; []) and Greek (0.9; []) versions, and the original English version of the United Kingdom (0.9; []). Moreover, Cronbach’s alpha value of the Hebrew version was higher than the Nepali (0.78; []), Indian (0.78; []), Arabic (0.87; [], Spanish (0.88; []), and Japanese (0.88; []) versions. The results clearly demonstrated a unidimensional solution.
The Confirmatory Factor Analysis showed a single factor solution. Of interest was the inclusion of a single correlated error introduced into the model between items one and two. These two items have been identified previously as a subscale of anticipatory dental anxiety []. The remaining three items refer to specific dental procedures. Hence, the researcher may consider this as a subscale of dental treatment anxiety. Investigators are recommended to report the total score but use the two subscales as exploratory for detailed analysis.
In the present study, 13.4% percent of participants reported phobic levels of dental anxiety according to cut off scores. The prevalence of dental anxiety in the current study, i.e., in the Israeli population, is higher than studies conducted among populations in Nepal [], Japan [], India [], Finland [], and Malaysia [], yet lower than those in Northern Ireland [] and Italy []. It was recently noted that this diversity may stem from variations in sampling methods across populations []. The present study demonstrated that age was inversely linked with dental anxiety, namely, younger participants had higher MDAS scores. This finding supports some studies [,,], while others found higher dental anxiety among older participants [] or no differences in MDSA scores by age [,]. In the current study females reported higher levels of dental anxiety than males, which is consistent with findings in samples in the UK [], Japan [], Italy [], Greece [], Saudi Arabia [], Malaysia [], Turkey [,], and China []. However, sex differences were not reported in the Nepali sample []. A negative correlation was found between dental anxiety and education in the present study, namely, those with lower education reported higher dental anxiety. This finding corresponds with previous studies [,,]; furthermore, a negative link was found between lower income with dental anxiety, namely, those with lower income reported higher dental anxiety. This finding supports those of previous studies [,,,]; nevertheless, is it contrary to a study demonstrating a positive correlation between dental anxiety and higher income [], as well as studies that demonstrated no differences in dental anxiety and participants’ monthly income [,,]. Finally, in the present study a correlation was found between the participants’ level of religiosity and their level of dental anxiety, namely, those who were more religious reported higher dental anxiety.
The present study has some limitations; therefore, findings should be interpreted cautiously. First, the study was based on self-report questionnaires; therefore, recall bias may affect the results. Second, participants were recruited via web-based platforms; as a result, the study sample may be biased towards those who are active on these networks.
5. Conclusions
The Hebrew version of the MDAS demonstrated high reliability and some evidence for validity. Therefore, it is recommended that the Hebrew version of the MDSA be used to quantify dental anxiety in the Israeli population. This is essential as the Hebrew version of the MDAS is likely to provide Israeli dental staff a vital tool for a more accurate assessment of their dental patients’ levels of dental anxiety.
Author Contributions
Conceptualization, M.S., L.G.-K. and M.B.-E.; methodology, M.S., G.H. and M.B.-E.; software, M.S., G.H. and M.B.-E.; validation, G.H. and E.M.; formal analysis, M.S., L.G.-K., G.H. and M.B.-E.; investigation, M.S. and M.B.-E.; data curation, M.S., L.G.-K., G.H., M.B.-E. and E.M.; writing—original draft preparation, M.S., L.G.-K. and M.B.-E.; writing—review and editing, M.S., L.G.-K., G.H., M.B.-E. and E.M.; visualization, M.S., L.G.-K., G.H., M.B.-E. and E.M.; supervision, M.B.-E.; project administration, M.S., M.B.-E. and E.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Ariel University (protocol code AU-SOC-MBE-20191110, date of approval 10 November 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sitheeque, M.; Massoud, M.; Yahya, S.; Humphris, G. Validation of the Malay version of the Modified Dental Anxiety Scale and the prevalence of dental anxiety in a Malaysian population. J. Investig. Clin. Dent. 2015, 6, 313–320. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD-11), 11th ed.; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Carter, A.E. Pathways of fear and anxiety in dentistry: A review. World J. Clin. Cases 2014, 2, 642. [Google Scholar] [CrossRef] [PubMed]
- Armfield, J.M.; Stewart, J.F.; Spencer, A.J. The vicious cycle of dental fear: Exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health 2007, 7, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Eitner, S.; Wichmann, M.; Paulsen, A.; Holst, S. Dental anxiety—An epidemiological study on its clinical correlation and effects on oral health. J. Oral Rehabil. 2006, 33, 588–593. [Google Scholar] [CrossRef]
- Kruger, E.; Thomson, W.M.; Poulton, R.; Davies, S.; Brown, R.H.; Silva, P.A. Dental caries and changes in dental anxiety in late adolescence. Community Dent. Oral Epidemiol. 1998, 26, 355–359. [Google Scholar] [CrossRef]
- Thom, A.; Sartory, G.; Jöhren, P. Comparison between one-session psychological treatment and benzodiazepine in dental phobia. J. Consult. Clin. Psychol. 2000, 68, 378. [Google Scholar] [CrossRef]
- Facco, E.; Zanette, G. The odyssey of dental anxiety: From prehistory to the present. A narrative review. Front. Psychol. 2017, 8, 1155. [Google Scholar] [CrossRef]
- Milgrom, P.; Weinstein, P. Dental fears in general practice: New guidelines for assessment and treatment. Int. Dent. J. 1993, 43, 288–293. [Google Scholar]
- Crawford, F. Clinical trials in dental primary care: What research methods have been used to produce reliable evidence? Br. Dent. J. 2005, 199, 155–160. [Google Scholar] [CrossRef][Green Version]
- De Jongh, A.; Adair, P.; Meijerink-Anderson, M. Clinical management of dental anxiety: What works for whom? Int. Dent. J. 2005, 55, 73–80. [Google Scholar] [CrossRef]
- Dailey, Y.; Humphris, G.; Lennon, M. The use of dental anxiety questionnaires: A survey of a group of UK dental practitioners. Br. Dent. J. 2001, 190, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, MI, USA, 2008; ISBN 9780191724015. [Google Scholar]
- Haugejorden, O.; Klock, K.S. Avoidance of dental visits: The predictive validity of three dental anxiety scales. Acta Odontol. Scand. 2000, 58, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Ratson, T.; Blumer, S.; Peretz, B. Dental anxiety of parents in an israeli kibbutz population and their prediction of their children’s behavior in the dental office. J. Clin. Pediatr. Dent. 2016, 40, 306–3011. [Google Scholar] [CrossRef] [PubMed]
- Blumer, S.; Ram, D.; Costa, L.; Peretz, B. Dental anxiety among Israeli postgraduate pediatric dental students and their instructors. J. Clin. Pediatr. Dent. 2018, 42, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.; Morrison, T.; Lindsay, S. The Modified Dental Anxiety Scale: Validation and United Kingdom norms. Community Dent. Health 1995, 12, 143–150. [Google Scholar] [PubMed]
- Humphris, G.; Dyer, T.; Robinson, P. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health 2009, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.; Hull, P. Do dental anxiety questionnaires raise anxiety in dentally anxious adult patients? A two-wave panel study. Prim. Dent. Care 2007, 14, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.; Freeman, R.; Campbell, J.; Tuutti, H.; D’Souza, V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int. Dent. J. 2000, 50, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Abu-Ghazaleh, S.B.; Rajab, L.D.; Sonbol, H.N.; Aljafari, A.K.; Elkarmi, R.F.; Humphris, G. The Arabic version of the modified dental anxiety scale. Psychometrics and normative data for 15-16 year olds. Saudi Med. J. 2011, 32, 725–729. [Google Scholar] [PubMed]
- Yuan, S.; Freeman, R.; Lahti, S.; Lloyd-Williams, F.; Humphris, G. Some psychometric properties of the Chinese version of the Modified Dental Anxiety Scale with cross validation. Health Qual. Life Outcomes 2008, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- Newton, J.; Edwards, J. Psychometric properties of the Modified Dental Anxiety Scale: An independent replication. Community Dent. Health 2005, 22, 40–42. [Google Scholar]
- Marsh, H.W.; Hocevar, D. Application of Confirmatory Factor Analysis to the Study of Self-Concept. First- and Higher Order Factor Models and Their Invariance Across Groups. Psychol. Bull. 1985, 97, 562–582. [Google Scholar] [CrossRef]
- Marsh, H.W.; Balla, J.R.; McDonald, R.P. Goodness-of-Fit Indexes in Confirmatory Factor Analysis: The Effect of Sample Size. Psychol. Bull. 1988, 103, 391–410. [Google Scholar] [CrossRef]
- Burke, M.J.; Brief, A.P.; George, J.M.; Roberson, L.; Webster, J. Measuring affect at work: Confirmatory analyses of competing mood structures with conceptual linkage to cortical regulatory systems. J. Pers. Soc. Psychol. 1989, 57, 1091–1102. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Evaluating model fit. In Structural Equation Modeling. Concepts, Issues, and Applications; Hoyle, R.H., Ed.; Sage: London, UK, 1995; pp. 76–99. [Google Scholar]
- Facco, E.; Agrillo, C.; Greyson, B. Epistemological implications of near-death experiences and other non-ordinary mental expressions: Moving beyond the concept of altered state of consciousness. Med. Hypotheses 2015, 85, 85–93. [Google Scholar] [CrossRef]
- Coolidge, T.; Arapostathis, K.N.; Emmanouil, D.; Dabarakis, N.; Patrikiou, A.; Economides, N.; Kotsanos, N. Psychometric properties of Greek versions of the Modified Corah Dental Anxiety Scale (MDAS) and the Dental Fear Survey (DFS). BMC Oral Health 2008, 8, 29. [Google Scholar] [CrossRef]
- Giri, J.; Pokharel, P.R.; Gyawali, R.; Bhattarai, B. Translation and Validation of Modified Dental Anxiety Scale: The Nepali Version. Int. Sch. Res. Not. 2017, 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S. Factors affecting dental anxiety and beliefs in an Indian population. J. Oral Rehabil. 2008, 35, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Coolidge, T.; Hillstead, M.B.; Farjo, N.; Weinstein, P.; Coldwell, S.E. Additional psychometric data for the Spanish Modified Dental Anxiety Scale, and psychometric data for a Spanish version of the Revised Dental Beliefs Survey. BMC Oral Health 2010, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, M.; Sago, T.; Furukawa, H. The Reliability and Validity of the Japanese Version of the Modified Dental Anxiety Scale among Dental Outpatients. Sci. World J. 2020, 2020, 8734946. [Google Scholar] [CrossRef] [PubMed]
- Lahti, S.M.; Tolvanen, M.M.; Humphris, G.; Freeman, R.; Rantavuori, K.; Karlsson, L.; Karlsson, H. Association of depression and anxiety with different aspects of dental anxiety in pregnant mothers and their partners. Community Dent. Oral Epidemiol. 2020, 48, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G.; Shanbhag, N.; Puranik, M.P. Cross-cultural adaptation of Kannada version of modified dental anxiety scale among an adult Indian population. J. Clin. Diagnostic Res. 2015, 9, ZC34. [Google Scholar] [CrossRef] [PubMed]
- Tunc, E.P.; Firat, D.; Onur, O.D.; Sar, V. Reliability and validity of the Modified Dental Anxiety Scale (MDAS) in a Turkish population. Community Dent. Oral Epidemiol. 2005, 33, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Gisler, V.; Bassetti, R.; Mericske-Stern, R.; Bayer, S.; Enkling, N. A cross-sectional analysis of the prevalence of dental anxiety and its relation to the oral health-related quality of life in patients with dental treatment needs at a university clinic in Switzerland. Gerodontology 2012, 29, e290–e296. [Google Scholar] [CrossRef] [PubMed]
- Malvania, E.A.; Ajithkrishnan, C.G. Prevalence and socio-demographic correlates of dental anxiety among a group of adult patients attending a dental institution in Vadodara city, Gujarat, India. Indian J. Dent. Res. 2011, 22, 179. [Google Scholar] [CrossRef]
- Humphris, G.; Crawford, J.R.; Hill, K.; Gilbert, A.; Freeman, R. UK population norms for the modified dental anxiety scale with percentile calculator: Adult dental health survey 2009 results. BMC Oral Health 2013, 13, 1–11. [Google Scholar] [CrossRef]
- Bahammam, M.A.; Hassan, M.H. Validity and reliability of an Arabic version of the modified dental anxiety scale in Saudi adults. Saudi Med. J. 2014, 35, 1384. [Google Scholar] [PubMed]
- Buldur, B.; Armfield, J.M. Development of the Turkish version of the Index of Dental Anxiety and Fear (IDAF-4C+): Dental anxiety and concomitant factors in pediatric dental patients. J. Clin. Pediatr. Dent. 2018, 42, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Appukuttan, D.; Datchnamurthy, M.; Deborah, S.P.; Hirudayaraj, G.J.; Tadepalli, A.; Victor, D.J. Reliability and validity of the Tamil version of Modified Dental Anxiety Scale. J. Oral Sci. 2012, 54, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Hakeberg, M.; Berggren, U.; Carlsson, S.G. Prevalence of dental anxiety in an adult population in a major urban area in Sweden. Community Dent. Oral Epidemiol. 1992, 20, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.; Birn, H.; Kirkegaard, E.; Brødsgaard, I.; Scheutz, F. Prevalence and characteristics of dental anxiety in Danish adults. Community Dent. Oral Epidemiol. 1993, 21, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Kanegane, K.; Penha, S.S.; Munhoz, C.D.; Rocha, R.G. Dental anxiety and salivary cortisol levels before urgent dental care. J. Oral Sci. 2009, 51, 515–520. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).