
Public Awareness of Bowel Cancer Risk Factors, Symptoms and Screening in Tasmania, Australia: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Sample Characteristics
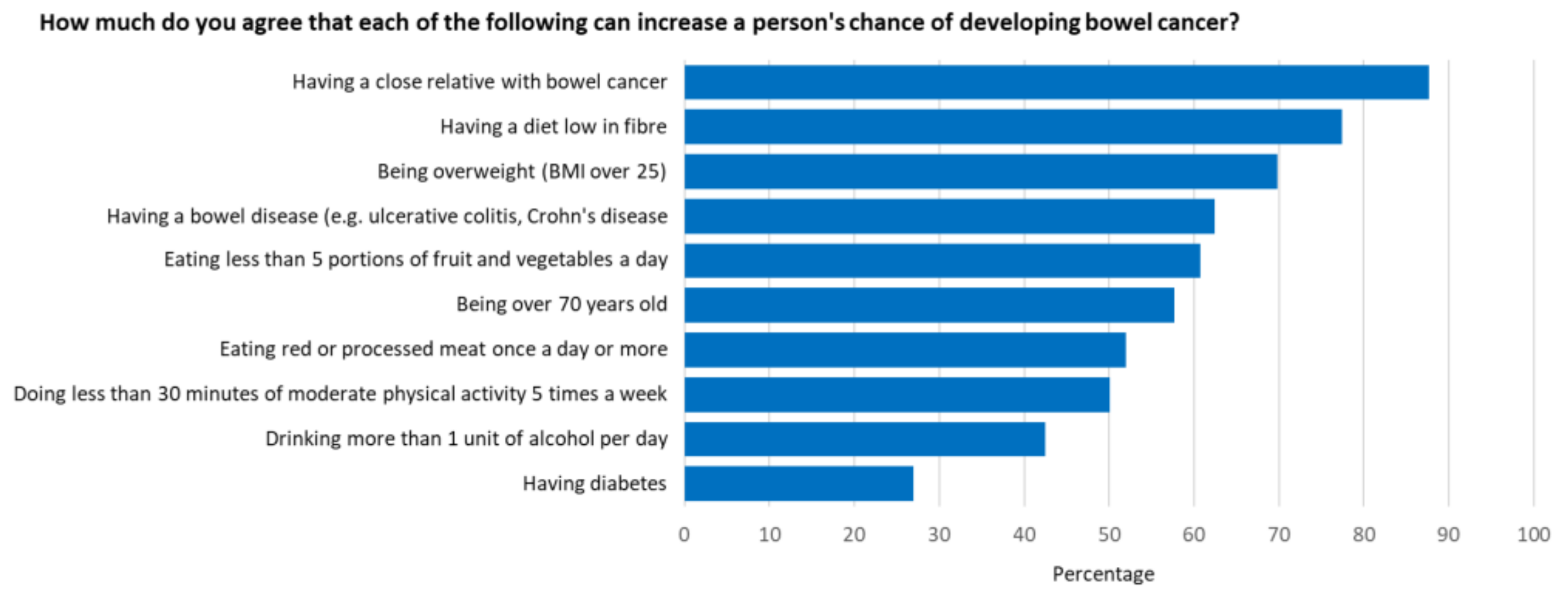
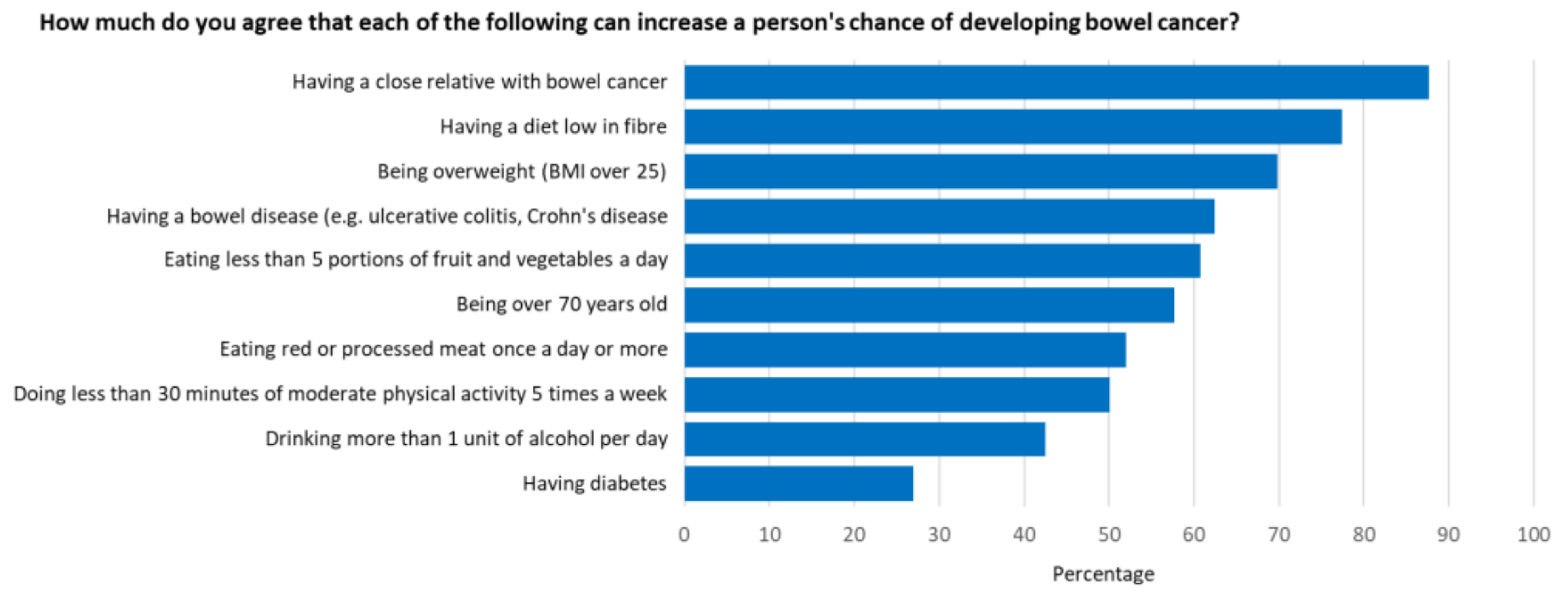
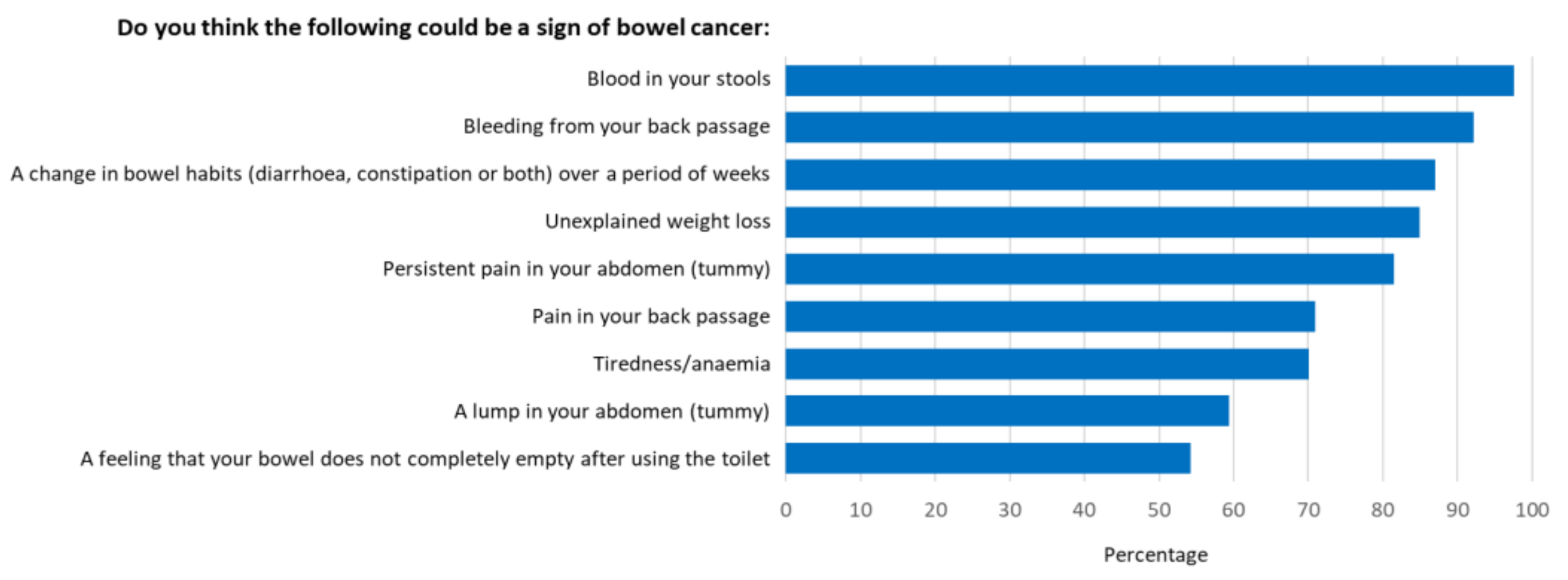
3.2. Levels of Bowel Cancer Awareness
3.3. Predictors of Bowel Cancer Awareness
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GLOBOCAN. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf (accessed on 12 May 2020).
- Australian Institute of Health and Welfare 2020. National Bowel Cancer Screening Program: Monitoring Report 2020; Cancer series no. 128. Cat. no. CAN 133; AIHW: Canberra, Australia, 2020. Available online: https://www.aihw.gov.au/getmedia/da6be503-6185-4b05-9724-953f81ad31de/aihw-can-133_31July2020.pdf.aspx?inline=true (accessed on 24 March 2021).
- Whiteman, D.C.; Webb, P.M.; Green, A.C.; Neale, R.E.; Fritschi, L.; Bain, C.J.; Parkin, D.M.; Wilson, L.F.; Olsen, C.M.; Nagle, C.M.; et al. Cancers in Australia in 2010 attributable to modifiable factors: Summary and conclusions. Aust. N. Z. J. Public Health 2015, 39, 477–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Australia. Available online: https://ncci.canceraustralia.gov.au/outcomes/relative-survival-rate/relative-survival-stage-diagnosis-colorectal-cancer (accessed on 14 May 2020).
- AIHW 2019. Cancer Data in Australia. Available online: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia/data (accessed on 14 May 2020).
- National Health Service 2007. Cancer Reform Strategy. Available online: https://www.nhs.uk/NHSEngland/NSF/Documents/Cancer%20Reform%20Strategy.pdf (accessed on 12 May 2020).
- Australian Institute of Health and Welfare. Available online: https://www.aihw.gov.au/reports/overweight-obesity/overweight-and-obesity-an-interactive-insight/contents/what-is-overweight-and-obesity (accessed on 12 May 2020).
- Australian Bureau of Statistics. 4364.0.55.001—National Health Survey: First Results, 2017–2018. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4364.0.55.001~2017-18~Main%20Features~Alcohol%20consumption~100 (accessed on 12 May 2020).
- Australian Institute of Health and Welfare 2019. Poor Diet. Cat. No. PHE 249; AIHW: Canberra, Australia, 2019. Available online: https://www.aihw.gov.au/reports/food-nutrition/poor-diet (accessed on 14 May 2020).
- Australian Institute of Health and Welfare 2019. Insufficient Physical Activity. Cat. No. PHE 248; AIHW: Canberra, Australia, 2019. Available online: https://www.aihw.gov.au/reports/risk-factors/insufficient-physical-activity (accessed on 14 May 2020).
- Cancer Australia. Distribution of Cancer Stage. Available online: https://ncci.canceraustralia.gov.au/diagnosis/distribution-cancer-stage/distribution-cancer-stage (accessed on 14 May 2020).
- Kippen, R.; James, E.; Ward, B.; Buykx, P.; Shamsullah, A.; Watson, W.; Chapman, K. Identification of cancer risk and associated behaviour: Implications for social marketing campaigns for cancer prevention. BMC Cancer 2017, 17, 550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macleod, U.; Mitchell, E.D.; Burgess, C.; MacDonald, S.; Ramirez, A.J. Risk factors for delayed presentation and referral of symptomatic cancer: Evidence for common cancers. Br. J. Cancer 2009, 101, s92–s101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forbes, L.J.L.; Warburton, F.; Richards, M.A.; Ramirez, A.J. Risk factors for delay in symptomatic presentation: A survey of cancer patients. Br. J. Cancer 2014, 111, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Koo, J.H.; Arasaratnam, M.M.; Liu, K.; Redmond, D.M.; Connor, S.J.; Sung, J.J.; Leong, R.W. Knowledge, perception and practices of colorectal cancer screening in an ethnically diverse population. Cancer Epidemiol. 2010, 34, 604–610. [Google Scholar] [CrossRef]
- MacTiernan, A.; Fritschi, L.; Slevin, T.; Jalleh, G.; Donovan, R.; Heyworth, J. Public perceptions of cancer risk factors: A Western Australian study. Health Promot. J. Austr. 2014, 25, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.C.; Magee, C.A.; Barrie, L.R.; Iverson, D.C.; Gregory, P.; Hanks, E.L.; Nelson, A.E.; Nehill, C.L.; Zorbas, H.M. Australian women’s perceptions of breast cancer risk factors and the risk of developing breast cancer. Womens Health Issues 2011, 21, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Jalleh, G.; Donovan, R.J.; Lin, C.; Slevin, T.; Clayforth, C.; Pratt, I.S.; Ledger, M. Beliefs about bowel cancer among the target group for the National Bowel Cancer Screening Program in Australia. Aust. N. Z. J. Public Health 2010, 34, 187–192. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics, 2016 Census Quick Stats. Available online: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/6?opendocument (accessed on 19 June 2021).
- Australian Bureau of Statistics 2018. National Health Survey: State and Territory Findings. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-state-and-territory-findings/latest-release#:~:text=In%202017%2D18%2C%2067.0%25,%25)%20who%20had%20the%20lowest. (accessed on 24 March 2021).
- Versace, V.L.; Skinner, T.C.; Bourke, L.; Harvey, P.; Barnett, T. National analysis of the Modified Monash Model, population distribution and a socio-economic index to inform rural health workforce planning. Aust. J. Rural Health 2021, 29, 801–810. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics 2018. Socio-Economic Indexes for Areas. Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 1 August 2021).
- University College London and Cancer Research UK 2011. Bowel Cancer Awareness Measure Toolkit Version 2.1. Available online: https://www.cancerresearchuk.org/sites/default/files/health_professional_bowel_cam_toolkit_version_2.1_09.02.11.pdf (accessed on 24 March 2021).
- Jensen, J.D.; Carcioppolo, N.; King, A.J.; Scherr, C.L.; Jones, C.L.; Niederdieppe, J. The cancer information overload (CIO) scale: Establishing predictive and discriminant validity. Patient Educ. Couns. 2014, 94, 90–96. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics 2021. Australian Statistical Geography Standard (ASGS): Volume 1—Main Structure and Greater Capital City Statistical Areas, July 2016. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/1270.0.55.001~July%202016~Main%20Features~Statistical%20Area%20Level%202%20(SA2)~10014 (accessed on 1 August 2021).
- Australian Bureau of Statistics 2018. Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA), Australia. 2016. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2033.0.55.001~2016~Main%20Features~IRSAD~20 (accessed on 1 August 2021).
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obamiro, K.; West, S.; Lee, S. Like, comment, tag, share: Facebook interactions in health research. Int. J. Med. Inform. 2020, 137, 104097. [Google Scholar] [CrossRef] [PubMed]
- Power, E.; Simon, A.; Juszczyk, D.; Hiom, S.; Wardle, J. Assessing awareness of colorectal cancer symptoms: Measure development and results from a population survey in the UK. BMC Cancer 2011, 11, 366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Summary-of-Third-Expert-Report-2018.pdf (accessed on 27 May 2020).
- Pandeya, N.; Wilson, L.F.; Webb, P.M.; Neale, R.E.; Bain, C.J.; Whiteman, D.C. Cancers in Australia in 2010 attributable to the consumption of alcohol. Aust. N. Z. J. Public Health 2015, 39, 408–413. [Google Scholar] [CrossRef] [Green Version]
- National Health and Medical Research Council; Australian Research Council and Universities Australia. Australian Guidelines to Reduce Health Risks from Drinking Alcohol; NHMRC: Canberra, Australia, 2020. [Google Scholar]
- Torrens University Australia Public Health Information Development Unit. Social health atlas of Australia: Population Health Areas. Available online: https://phidu.torrens.edu.au/social-health-atlases/data#social-health-atlas-of-australia-population-health-areas (accessed on 20 June 2021).
- Department of Health. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines#npa1864 (accessed on 27 May 2020).
- Olsen, C.M.; Wilson, L.F.; Nagle, C.M.; Kendall, B.J.; Bain, C.J.; Pandeya, N.; Webb, P.M.; Whiteman, D.C. Cancers in Australia in 2010 attributable to insufficient physical activity. Aust. N. Z. J. Public Health 2015, 39, 458–463. [Google Scholar] [CrossRef]
- American Institute for Cancer Research. The AICR 2013 Cancer Risk Awareness Survey Report. 2013. Available online: http://www.aicr.org/assets/docs/pdf/education/aicrcancer-awareness-report-2012.pdf (accessed on 28 May 2020).
- Waters, E.A.; Hawkins, E. Awareness of Health Outcomes Associated with Insufficient Physical Activity and Associations with Physical Activity Intentions and Behavior. J. Health Commun. 2018, 23, 634–642. [Google Scholar] [CrossRef]
- Lagerlund, M.; Hvidberg, L.; Hajdarevic, S.; Fischer Pedersen, A.; Runesdotter, S.; Vedsted, P.; Tishelman, C. Awareness of risk factors for cancer: A comparative study of Sweden and Denmark. BMC Public Health 2015, 15, 1156. [Google Scholar] [CrossRef] [Green Version]
- Tfaily, M.A.; Naamani, D.; Kassir, A.; Sleiman, S.; Ouattara, M.; Moacdieh, M.P.; Jaffa, M.A. Awareness of Colorectal Cancer and Attitudes Towards Its Screening Guidelines in Lebanon. Ann. Glob. Health 2019, 85, 75. [Google Scholar] [CrossRef]
- Peeters, P.J.; Bazelier, M.T.; Leufkens, H.G.; de Vries, F.; De Bruin, M.L. The risk of colorectal cancer in patients with type 2 diabetes: Associations with treatment stage and obesity. Diabetes Care 2015, 38, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Berster, J.M.; Göke, B. Type 2 diabetes mellitus as risk factor for colorectal cancer. Arch. Physiol. Biochem. 2008, 114, 84–98. [Google Scholar] [CrossRef]
- Schliemann, D.; Paramasivam, D.; Dahlui, M.; Cardwell, C.R.; Somasundaram, S.; Tamin, N.S.B.I.; Donnelly, C.; Su, T.T.; Donnelly, M. Change in public awareness of colorectal cancer symptoms following the Be Cancer Alert Campaign in the multi-ethnic population of Malaysia. BMC Cancer 2020, 20, 252. [Google Scholar] [CrossRef] [PubMed]
- Versace, V.L.; Forsyth, A.D.; Vaughan, R.; Morrice, M.G.; Morphett, B.J. Evidence of elevated colorectal cancer and adenoma rates for regional National Bowel Cancer Screening Program participants. Aust. J. Rural Health 2018, 26, 63–64. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Available online: https://www.dhhs.tas.gov.au/__data/assets/pdf_file/0004/375025/The_State_of_Public_Health_Tasmania_2018_v10.pdf (accessed on 23 September 2021).
- Durkin, S.J.; Broun, K.; Spittal, M.J.; Wakefield, M.A. Impact of a mass media campaign on participation rates in a National Bowel Cancer Screening Program: A field experiment. BMJ Open 2019, 9, e024267. [Google Scholar] [CrossRef] [PubMed]
- Durkin, S.; Broun, K.; Guerin, N.; Morley, B.; Wakefield, M. Impact of a mass media campaign on participation in the Australian bowel cancer screening program. J. Med. Screen. 2020, 27, 18–24. [Google Scholar] [CrossRef]
- Messina, C.R.; Lane, D.S.; Anderson, J.C. Body mass index and screening for colorectal cancer: Gender and attitudinal factors. Cancer Epidemiol. 2012, 36, 400–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardozo, E.R.; Dune, T.J.; Neff, L.M.; Brocks, M.E.; Ekpo, G.E.; Barnes, R.B.; Marsh, E.E. Knowledge of obesity and its impact on reproductive health outcomes among urban women. J. Community Health 2013, 38, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Anderson, A.S.; Birch, J.; Forster, A.S.; Rosenberg, G.; Bauld, L.; Vohra, J. Public awareness and healthcare professional advice for obesity as a risk factor for cancer in the UK: A cross-sectional survey. J. Public Health 2018, 40, 797–805. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, S.C.; Waller, J.; Jarvis, M.J.; Humphries, S.E.; Wardle, J. Awareness of lifestyle risk factors for cancer and heart disease among adults in the UK. Patient Educ. Couns. 2009, 74, 221–227. [Google Scholar] [CrossRef]
- Schliemann, D.; Ismail, R.; Donnelly, M.; Cardwell, C.R.; Su, T.T. Cancer symptom and risk factor awareness in Malaysia: Findings from a nationwide cross-sectional study. BMC Public Health 2020, 20, 464. [Google Scholar] [CrossRef]
- West, R.; Alkhatib, M.N.; McNeill, A.; Bedi, R. Awareness of mouth cancer in Great Britain. Br. Dent. J. 2006, 200, 167–169. [Google Scholar] [CrossRef] [Green Version]
- Ayanian, J.Z.; Cleary, P.D. Perceived risks of heart disease and cancer among cigarette smokers. JAMA 1999, 281, 1019–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- TMarteau, h.M.; Hankins, M.; Collins, B. Perceptions of risk of cervical cancer and attitudes towards cervical screening: A comparison of smokers and non-smokers. Fam. Pract. 2002, 19, 18–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.C.; Hirai, H.W.; Luk, A.K.; Lam, T.Y.; Ching, J.Y.; Griffiths, S.M.; Chan, F.K.; Sung, J.J. The knowledge of colorectal cancer symptoms and risk factors among 10,078 screening participants: Are high risk individuals more knowledgeable? PLoS ONE 2013, 8, e60366. [Google Scholar] [CrossRef] [PubMed]
- Obamiro, K.O.; Chalmers, L.; Lee, K.; Bereznicki, B.J.; Bereznicki, L.R.E. Anticoagulation knowledge in patients with atrial fibrillation: An Australian survey. Int. J. Clin. Pract. 2018, 72, e13072. [Google Scholar] [CrossRef]
- Eysenbach, G.; Wyatt, J. Using the Internet for surveys and health research. J. Med. Internet Res. 2002, 4, E13. [Google Scholar] [CrossRef]
- Bidmon, S.; Terlutter, R. Gender differences in searching for health information on the internet and the virtual patient-physician relationship in Germany: Exploratory results on how men and women differ and why. J. Med. Internet Res. 2015, 17, e156. [Google Scholar] [CrossRef]
- Aziz, I.; Simrén, M. The overlap between irritable bowel syndrome and organic gastrointestinal diseases. Lancet Gastroenterol. Hepatol. 2021, 6, 139–148. [Google Scholar] [CrossRef]
- Dancey, C.P.; Fox, R.; Devins, G.M. The measurement of irritable bowel syndrome (IBS)-related misconceptions in people with IBS. J. Psychosom. Res. 1999, 47, 269–276. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Parameter | Number and Percentage of Participants—n (%) |
|---|---|
| Gender | |
| Male | 892 (24.1) |
| Female | 2806 (75.8) |
| Other | 5 (0.1) |
| Age | |
| 18–49 years | 1712 (46.2) |
| 50–74 years | 1925 (52.0) |
| 75+ years | 61 (1.6) |
| Missing | 5 (0.1) |
| Highest education completed | |
| Year 12 and below | 987 (26.7) |
| Certificate | 649 (17.5) |
| Diploma | 631 (17.0) |
| Bachelors | 1073 (29) |
| Masters | 282 (7.6) |
| PhD | 79 (2.1) |
| Missing | 2 (0.1) |
| Current employment status | |
| Not currently working | 1225 (33.1) |
| Currently employed | 2478 (66.9) |
| Annual income bracket (AUD) | |
| 0 to 18,200 | 646 (17.5) |
| 18,201 to 37,000 | 859 (23.2) |
| 37,001 to 90,000 | 1618 (43.7) |
| 90,001 to 180,000 | 540 (14.6) |
| >180,000 | 38 (1.0) |
| Missing | 2 (0.1) |
| Ethnicity | |
| Caucasian descent | 3504 (94.6) |
| Non-Caucasian descent | 199 (5.4) |
| Remoteness area | |
| MM2 (regional centres) | 2419 (65.4) |
| MM3 (large rural towns) | 557 (15.0) |
| MM4 (medium rural towns) | 7 (0.2) |
| MM5 (small rural towns) | 637 (17.2) |
| MM6 (remote communities) | 47 (1.3) |
| MM7 (very remote communities) | 15 (0.4) |
| Missing | 21 (0.5) |
| Index of relative socio-economic advantage and disadvantage | |
| 1–5 (most disadvantaged) | 2460 (66.4) |
| 6–10 (most advantaged) | 1233 (33.3) |
| Missing | 10 (0.3) |
| Body mass index | |
| Under weight | 46 (1.2) |
| Healthy weight | 1066 (28.7) |
| Overweight and obese | 2523 (68.1) |
| Missing | 68 (1.8) |
| Smoking status | |
| Current smoker | 333 (9.0) |
| Non-smoker | 3365 (90.9) |
| Missing | 5 (0.1) |
| Family history of bowel cancer | |
| Positive history | 1259 (34.0) |
| No history | 2442 (66.0) |
| Missing | 2 (0.1) |
| Parameter | Estimate | p Value |
|---|---|---|
| Age (years) | 0.007 (−0.002–0.170) | 0.123 |
| Gender (female) | 0.094 (−0.201–0.389) | 0.533 |
| Higher educational level | 0.548 (0.470–0.626) | <0.001 |
| Higher income bracket | 0.572 (0.441–0.703) | <0.001 |
| Modified Monash Model (increasing rurality) ranking) | 0.004 (−0.103–0.110) | 0.947 |
| Currently employed | 0.897 (0.626–1.168) | <0.001 |
| Ethnicity (non-Caucasian) | −0.626 (−1.195–−0.058) | 0.031 |
| BMI (overweight and obese) | −0.662 (−0.939–−0.384) | <0.001 |
| SEIFA IRSAD score | −0.014 (−0.064–0.036) | 0.586 |
| Current smoker | −1.052 (−1.497–−0.608) | <0.001 |
| Positive family history of cancer (any type) | 0.208 (−0.071–0.486) | 0.144 |
| Positive family history of bowel cancer | 0.201 (−0.068–0.471) | 0.143 |
| Higher information overload | −0.246 (−0.280–−0.213) | <0.001 |
| Variable | B (95% Confidence Interval) | p Value |
|---|---|---|
| Age | 0.010 (0.001–0.019) | 0.024 |
| Education level | 0.406 (0.324–0.488) | <0.001 |
| Income bracket | 0.196 (0.049–0.344) | 0.009 |
| Currently employed | 0.401 (0.110–0.692) | 0.007 |
| Ethnicity (non-Caucasian) | −0.546 (−1.091–0.000) | 0.050 |
| Current smoker | −0.535 (−0.965–−0.105) | 0.015 |
| BMI (overweight and obese) | −0.339 (−0.607–−0.070) | 0.014 |
| Positive family history of cancer (any type) | 0.059 (−0.233–0.351) | 0.692 |
| Positive family history of bowel cancer | 0.229 (−0.053–0.512) | 0.112 |
| Information overload score (higher score) | −0.214 (−0.247–−0.181) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.M.; Versace, V.L.; Obamiro, K. Public Awareness of Bowel Cancer Risk Factors, Symptoms and Screening in Tasmania, Australia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1497. https://doi.org/10.3390/ijerph19031497
Lee SM, Versace VL, Obamiro K. Public Awareness of Bowel Cancer Risk Factors, Symptoms and Screening in Tasmania, Australia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1497. https://doi.org/10.3390/ijerph19031497
Chicago/Turabian StyleLee, Simone M., Vincent L. Versace, and Kehinde Obamiro. 2022. "Public Awareness of Bowel Cancer Risk Factors, Symptoms and Screening in Tasmania, Australia: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 3: 1497. https://doi.org/10.3390/ijerph19031497
APA StyleLee, S. M., Versace, V. L., & Obamiro, K. (2022). Public Awareness of Bowel Cancer Risk Factors, Symptoms and Screening in Tasmania, Australia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(3), 1497. https://doi.org/10.3390/ijerph19031497