
Spatial Differences in the Effect of Communities’ Built Environment on Residents’ Health: A Case Study in Wuhan, China


Abstract
:1. Introduction
2. Literature Review
2.1. Health Effects of the Built Environment
2.2. Health Impacts of Community Differentiation
3. Data and Methodology
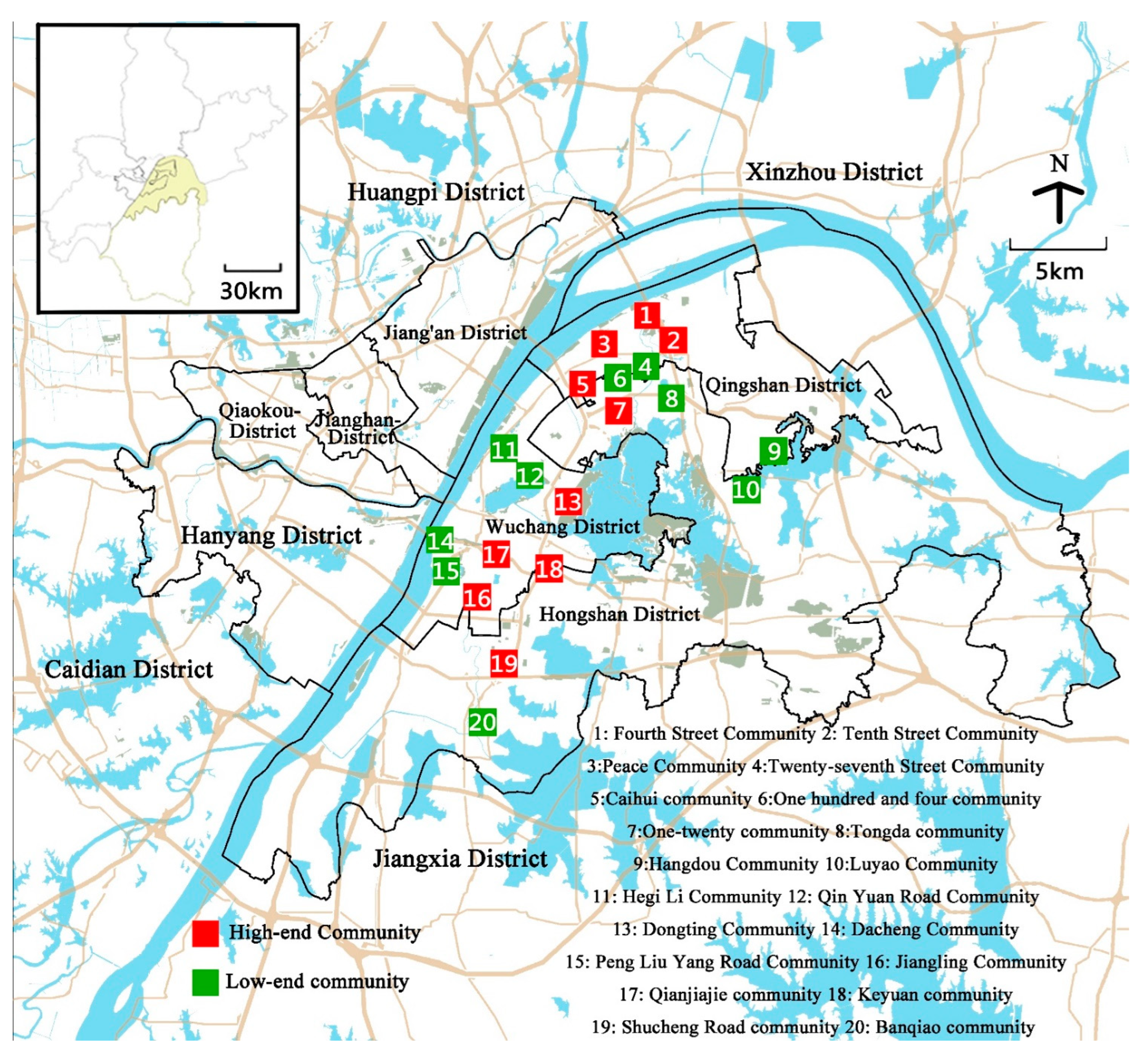
3.1. Study Area and Data
3.2. Indicator Selection and Research Framework
3.3. Community Type Classification
3.4. Research Methodology and Model Construction
3.5. Descriptive Statistics of the Sample
4. Results
4.1. Community Effects Test
4.2. Influence of Individual Characteristics
4.3. Influence of the Built Environment
4.4. Community Differentiation
5. Discussion
5.1. High Density Built Environment
5.2. Community Differentiation Problems
5.3. Policy Implications
5.4. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, X.; Sun, Y. Investigating Institutional Integration in the Contexts of Chinese City-regionalization: Evidence from Shenzhen-Dongguan-Huizhou. Land Use Policy 2019, 88, 104170. [Google Scholar] [CrossRef]
- Zhang, X.; Cheung, D.M.; Sun, Y.; Tan, J. Political Decentralization and the Path Dependent Characteristics of the State Authoritarianism: An Integrated Conceptual Framework to Understand China’s Territorial Fragmentation. Eurasian Geogr. Econ. 2019, 60, 548–581. [Google Scholar] [CrossRef]
- Yuan, M.; Song, Y.; Huang, Y.; Hong, S.; Huang, L. Exploring the Association between Urban Form and Air Quality in China. J. Plan. Educ. Res. 2018, 38, 413–426. [Google Scholar] [CrossRef]
- Gu, C. Urban Sociology; Southeast University Press: Nanjing, China, 2002. [Google Scholar]
- Yuan, Y. Research on Stabilization of Spatiality of Urban Poverty against the Background of Social-spatial Reconstruction. Mod. Urban Res. 2011, 26, 14–18. [Google Scholar]
- Yu, Y.; Hu, Y. Progress of International Research on Health Impact of the Built Environment of Communities: Literature Review and Reflections from a Perspective of Physical Activities. Archit. J. 2017, 2, 33–38. [Google Scholar]
- Wang, L.; Liao, S.; Zhao, X. Exploration of Approaches and Factors of Healthy City Planning. Urban Plan. Int. 2016, 31, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Ouyang, W.; Tian, L. Study on the Scale and Method of Impacts of Built Environment on Public Health. Shanghai Urban Plan. Rev. 2020, 2, 38–43. [Google Scholar]
- Cervero, R.; Kockelman, K. Travel demand and the 3Ds: Density, diversity, and design. Transp. Res. Part D 1997, 2, 199–219. [Google Scholar] [CrossRef]
- Ewing, R.; Cervero, R. Travel and the built environment: A meta-analysis. J. Am. Plan. Assoc. 2010, 76, 265–294. [Google Scholar] [CrossRef]
- Lu, F.; Tan, S. Built Environment’s Influence on Physical Activity: Review and Thought. Urban Plan. Int. 2015, 30, 62–70. [Google Scholar]
- Frank, L.D.; Schmid, T.L.; Sallis, J.F.; Chapman, J.; Saelens, B.E. Linking objectively measured physical activity with objectively measured urban form: Findings from SMARTRAQ. Am. J. Prev. Med. 2005, 28 (Suppl. 2), 117–125. [Google Scholar] [CrossRef] [PubMed]
- Aday, L.A.; Andersen, R. A framework for the study of access to medical care. Health Serv. Res. 1974, 9, 208–220. [Google Scholar] [PubMed]
- Yang, X.S.; Liu, H.L. Health Resource Geographic Allocation and Health Outcome: An Empirical Analysis Based on Cross-province Data. Chin. Health Econ. 2016, 35, 63–65. [Google Scholar]
- Irvine, K.N.; Warber, S.L.; Patrick, D.W.; Gaston, K.J. Understanding urban green space as a health resource: A qualitative comparison of visit motivation and derived effects among park users in Sheffield, UK. Int. J. Environ. Res. Public Health 2013, 10, 417–442. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Siu, K.M.W.; Gong, X.Y.; Gao, Y.; Lu, D. Where do networks really work? The effects of the Shenzhen greenway network on supporting physical activities. Landsc. Urban Plan. 2016, 152, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Tao, Y.-H.; Cai, Y.-W. Neighborhood Built Environment, Community Cohesion and Public Health: The Moderating Effect of Transport-Related Physical Activity. Urban Dev. Stud. 2019, 26, 17–25. [Google Scholar]
- Wang, U.; Kwan, M. An Analytical Framework for Integrating the Spatiotemporal Dynamics of Environmental Context and Individual Mobility in Exposure Assessment: A Study on the Relationship between Food Environment Exposures and Body Weight. Int. Ournal Environ. Res. Public Health 2018, 15, 2022. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Yang, J. Built Environment And Public Health Review And Planning ln North American Metropolitan Areas. Planners 2015, 31, 12–19. [Google Scholar]
- Zhang, Y.; Liu, N.; Long, Y. Research on Healthy Neighborhood Evaluation System Based on the Combined Perspectives of Urban Planning and Public Health. Landsc. Archit. 2020, 27, 96–103. [Google Scholar]
- Wang, K. Investigation Research on the Current Situation of Physical Activities among Residents in Varieties of Community of Cities in China. J. Beijing Sport Univ. 2005, 8, 1009–1013. [Google Scholar]
- Li, H.; Zhang, Z. Passive suburbanization of urban low-income people. Urban Probl. 2011, 10, 97–101. [Google Scholar]
- Browning, C.; Cagney, K. Collective efficacy and health: Neighborhood social capital and self-rated physical functioning in an urban setting. J. Health Soc. Behav. 2002, 43, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.W.; Smith, G.D.; Kaplan, G.A.; House, J.S. Income inequality and mortality: Importance to health of individual income, psychosocial environment, or material conditions. Br. Med. J. 2000, 320, 1200–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, Y.; Zhu, Z.; Zhou, S. The Effects of Green Space on Leisure Time Physical Activities from the Perspective of Community Differentiation: A Case Study of Guangzhou, China. Trop. Geogr. 2019, 39, 237–246. [Google Scholar]
- Deeg, D.; Gcf, T. Discrepancies between personal income and neighborhood status: Effects on physical and mental health. Eur. J. Ageing 2005, 2, 98–108. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H. On the Status Quo and the Development Tendency of Community Differentiation and Transformation in Contemporary Chinese Cities. Planners 2002, 8, 5–8. [Google Scholar]
- Chai, Y.W.; Ma, J.; Zhang, W.J. The residential differentiation of tour-based spatio-temporal decision-making of travel behavior in Beijing City. Geogr. Res. 2010, 29, 1725–1734. [Google Scholar]
- Li, X.Y.; Zhu, C.G. A summary of the studies on separation of urban communities in China. Urban Dev. Stud. 2005, 5, 76–81. [Google Scholar]
- Gao, J.B.; Zhou, C.S.; Jiang, H.Y.; Ye, C.D. The research on the spatial differentiation of the urban public service facilities distribution in Guangzhou. Hum. Geogr. 2010, 25, 78–83. [Google Scholar]
- Dou, X. Study on Residential Space Structure of Wuhan; Central China Normal University: Wuhan, China, 2011. [Google Scholar]
- Li, M.; Luo, N. European Five Dimensional Health Scale (EQ-5D) Chinese application introduction. China J. Pharm. Econ. 2009, 1, 49–57. [Google Scholar]
- Wang, L.; Sun, W.; Wu, Y. Study on the impact of subjective perception of urban environment on residents’ health: Based on a large sample survey of 60 counties and cities in China. Hum. Geogr. 2020, 35, 55–64. [Google Scholar]
- Miilunpalo, S.; Vuori, I.; Oja, P.; Pasanen, M.; Urponen, H. Self-rated health status as a health measure: The predictive value of self-reported health status on the use of physician services and on mortality in the working age population. J. Clin. Epidemiol. 1997, 50, 517–528. [Google Scholar] [CrossRef]
- DeSalvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality prediction with a single general self-rated health question: A meta-analysis. J. Gen. Intern. Med. 2006, 21, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y. The predictive value of self assessed general, physical, and mental health on functional decline and mortality in older adults. J. Epidemiol. Community Health 2000, 54, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Yu, Y. A study on the social influencing factors of residents’ self-rated health. Dong Yue Trib. 2019, 40, 31–41. [Google Scholar]
- Zhu, Z.; Tao, X.; Zhou, S. The Residential Differentiation of Residents’ Overweight: A Case Study of Guangzhou. Trop. Geogr. 2020, 40, 487–497. [Google Scholar]
- Dong, X.; Zang, W. The Effect of Retirement on the Health of Middle-aged and Elderly People. Popul. J. 2017, 39, 76–88. [Google Scholar]
- Yang, C. Empirical Study on the Impact of Unemployment on Health of Different Age Groups-Take CFPS Data as an Example; Nanjing University: Nanjing, China, 2020. [Google Scholar]
- Zhao, S.; Zang, W.; Fu, S.; Liu, G. Health of the Uninsured under Mandatory Medical Insurance System. Econ. Res. J. 2013, 48, 118–131. [Google Scholar]
- Zhang, X. Analysis of the Importance of Regular Physical Examination. Med. Soc. 2011, 24, 54–56. [Google Scholar]
- Tian, L.; Li, J.; Ouyang, W.; Chen, W.; Zeng, H.; Xiao, Y. Relationships between urban-rural planning and public health and somethoughts on a inter-disciplinary research framework. Urban Plan. Forum 2016, 2, 111–116. [Google Scholar]
- Gan, L.; Yu, W.; Wang, L. Spatial Characteristics of Urban Green Space under Different Health Impact Pathways. Landsc. Archit. 2020, 27, 95–100. [Google Scholar]
- Rundle, A.; Roux, A.V.D.; Freeman, L.M.; Miller, D.; Neckerman, K.M.; Weiss, C.C. The Urban Built Environment and Obesity in New York City: A Multilevel Analysis. Am. J. Health Promot. 2007, 21 (Suppl. 4), 326–334. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Zheng, Y.; Li, Z.; An, Z. Influence of urban high-density living environment on stroke risk: A case study of Wuhan. City Plan. Rev. 2021, 45, 30–39. [Google Scholar]
- Shan, Z.; An, Y.; Yuan, M. High-Temperature Disaster Risk Assessment for Urban Communities: A Case Study in Wuhan, China. Int. J. Environ. Res. Public Health 2022, 19, 183. [Google Scholar] [CrossRef]
- Wang, L.; Yirui, D. Research progress overview on the impact of built environment on physical activity. Sci. Technol. Rev. 2020, 38, 53–60. [Google Scholar]
- Walden, M.L. Magnet Schools and the Differential Impact of School Quality on Residential Property Values. J. Real Estate Res. 1990, 5, 221–230. [Google Scholar] [CrossRef]
- Tse, R.Y.C.; Love, P.E.D. Measuring residential property values in Hong Kong. Prop. Manag. 2000, 18, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Chau, K.W. The pricing of “luckiness” in the apartment market. J. Real Estate Lit. 2001, 9, 29–40. [Google Scholar] [CrossRef]
- Wen, H.Z.; Zhang, L.; Peng, L.F. Spatial Variation of Housing Prices in Hangzhou City: Two-Dimensional Analysis Based on Hedonic Prices. China Land Sci. 2010, 24, 51–56. [Google Scholar]
- Li, M.X. An Empirical Study on Residential Spatial Differentiation: Based on Residential Choice Perspective; Zhejiang University: Hangzhou, China, 2011. [Google Scholar]
- Yu, Y.; Yu, T. The Differences in the Impact of Food Environment on the Physiological Health of Different Income Groups: A Case Study of Nanjing. Mod. Urban Res. 2020, 11, 110–117. [Google Scholar]
- Qiu, Y.Z.; Chen, H.S.; Li, Z.G.; Wang, R.Y.; Liu, Y.; Qin, X.F. Exploring neighborhood environmental effects on mental health: A case study in Guangzhou, China. Prog. Geogr. 2019, 38, 283–295. [Google Scholar]
- Craig, D.; Kelvyn, J.; Graham, M. Context, composition and heterogeneity: Using multilevel models in health research. Soc. Sci. Med. 1998, 46, 97–117. [Google Scholar]
- Zhou, S.; Song, J.; Song, G. Examining the dual-levels impact of neighbourhood and individual variables on car use on weekdays in Guangzhou. Acta Geogr. Sin. 2017, 72, 1444–1457. [Google Scholar]
- Jie, L. Study on the Evaluation of the Life Convenience of Typical Differentiated Communities from the Perspective of Life Circle—Take Center Optimization District of Chengdu as an Example; Chengdu University of Technology: Chengdu, China, 2019. [Google Scholar]
- Huang, F.L. Multilevel modeling myths. Sch. Psychol. Q. 2018, 33, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Wang, M. Socioeconomic Status, Lifestyle, and Residents’ Self-Rated Health; Shandong University: Jinan, China, 2019. [Google Scholar]
- Chen, L. The Health Status of Residents in a Community from Yuzhong District of Chongqing and the Relevant Factors; Third Military Medical University: Wuhan, China, 2016. [Google Scholar]
- Zhang, Y. The Influence of Built Environment on Chronic Disease: Review and Enlightment. Urban Plan. Int. 2019, 34, 82–88. [Google Scholar] [CrossRef]
- Yao, Y.; Li, S. Review on Research of Urban Green Space Based on Public Health. Chin. Landsc. Archit. 2018, 34, 118–124. [Google Scholar]
- Shan, Z.; Wu, Z.; Yuan, M. Exploring the Influence Mechanism of Attractiveness on Wuhan’s Urban Commercial Centers by Modifying the Classic Retail Model. ISPRS Int. J. Geo-Inf. 2021, 10, 652. [Google Scholar] [CrossRef]
- Samimi, A.; Mohammadiana, A.K.; Madanizadeh, S. Effects of transportation and built environment on general health and obesity. Transp. Res. Part D 2009, 14, 67–71. [Google Scholar] [CrossRef]
- Wang, L.; Jiang, X.; Sun, W.; Zhao, X.; Tang, J. Impact of urban built environment on respiratory health and its planning strategy: A case study of a district in Shanghai. City Plan. Rev. 2018, 42, 15–22. [Google Scholar]
- Bao, Z.; Li, C. Progress on the Study of Urban Architecture FAR. Prog. Geogr. 2010, 29, 396–402. [Google Scholar]
- Li, J.; Wang, X.; Xue, L.; Gao, X.; Sun, L.; Wang, W. Study on pollution characteristics and the influencing factors of exhaust particles from typical. Acta Sci. Circumstantiae 2019, 39, 35–43. [Google Scholar]
- Zhang, Y.; Qin, B.; Tang, J. The impact of urban built environment on residential physical health: Based on propensity score matching. Acta Geogr. Sin. 2018, 73, 333–345. [Google Scholar]
- Guo, L.; Luo, J.; Yuan, M.; Huang, Y.; Shen, H.; Li, T. The influence of urban planning factors on PM 2.5 pollution exposure and implications: A case study in China based on remote sensing, LBS, and GIS data. Sci. Total Environ. 2019, 659, 1585–1596. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J. Development of sustainable urban forms for high-density low-income Asian countries: The case of Vietnam. Cities 2012, 29, 77–87. [Google Scholar] [CrossRef]
- Yuan, C.F.; Li, J.; Mao, R.Y. Research on and Improvement Measures for Building Volume of Residential Quarters in Chongqing, P.R. China. J. Civ. Environ. Eng. 2008, 1, 26–29. [Google Scholar]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City planning and population health: A global challenge. Lancet 2016, 388, 2912–2924. [Google Scholar] [CrossRef]
- Zhao, P.; Kwan, M.; Zhou, S. The Uncertain Geographic Context Problem in the Analysis of the Relationships between Obesity and the Built Environment in Guangzhou. Int. J. Environ. Res. Public Health 2018, 15, 308. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Shen, J.; Gao, X. Towards a comprehensive understanding of intercity cooperation in China’s city-regionalization: A comparative study of Shenzhen-Hong Kong and Guangzhou-Foshan city groups. Land Use Policy 2021, 103, 105339. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, S.; Luan, X.; Yuan, M. Understanding China’s City-regionalization: Spatial Structure and Relationships between Functional and Institutional Spaces in the Pearl River Delta. Urban Geogr. 2020, 42, 312–339. [Google Scholar] [CrossRef]
- Yuan, M.; Huang, Y.; Shen, H.; Li, T. Effects of urban form on haze pollution in China: Spatial regression analysis based on PM 2.5 remote sensing data. Appl. Geogr. 2018, 98, 215–223. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Variable | Interpretation | Data Source |
|---|---|---|---|
| Health facilities | Health/unhealthy food store ratio | Ratio of the number of unhealthy food stores to healthy food stores in the buffer zone | poi |
| Density of medical facilities | Density of medical service providers in the buffer zone | poi | |
| Parks and squares area | Parks and squares area in the buffer zone | Land Data | |
| Transportation facilities | Density of traffic stations | Density of traffic stations in the buffer zone | poi |
| Density of road intersections | Density of road intersections in the buffer zone | Road Data | |
| Community density | Building density | Sample Community Building Density | Construction Data |
| Floor area ratio | Sample Community Floor Area Ratio | Construction Data | |
| Individual attributes | Gender | 0 = male; 1 = female | survey |
| Age | Respondents’ biological age | survey | |
| Education | 0 = Junior high school and below; 1 = High School/Junior College; 2 = College/bachelor and above | survey | |
| Employment status | 0 = Employed; 1 = retied, 2 = Unemployed | survey | |
| Health insurance | 0 = No; 1 = Yes | survey | |
| Medical checkup | 0 = No; 1 = Yes | survey | |
| Per capita annual income | Continuous Variables | survey | |
| Per capita housing area | Continuous Variables | survey | |
| Self-rated health status | Self-assessment value (0–100) | survey |
| Type of Features | Evaluation Indicators | Interpretation | Indicator Direction |
|---|---|---|---|
| Architectural Features | House price | Sale price per square meter of residential units, from Anjuke website data, with a score of 1–5 according to equal intervals | Positive |
| Building Age | The time between the completion of the residence and the present, according to the equal interval, assigned 1–5 scores | Negative | |
| Neighborhood Features | Green Environment | The green space rate within the 800 m buffer zone of the community is assigned 1–5 scores according to the equal interval | Positive |
| Supporting facilities | The number of poi in the community’s 800 m buffer is assigned a score of 1–5 based on equal intervals | Positive | |
| Location Features | Traffic Location | The Euclidean distance of the community from the nearest transportation station, according to the equal interval, assigning a score of 1–5 | Negative |
| Geographical location | Community distance from Wuhan central activity area in European style, according to the equal interval, assigned 1–5 scores | Negative |
| Variable | Definition and Units | Full Sample | Low-End Community Sample | High-End Community Sample | |
|---|---|---|---|---|---|
| Gender | Male (%) | 45.8 | 46.1 | 45.6 | |
| Female (%) | 54.2 | 53.9 | 54.4 | ||
| Age | Age 18–25 (%) | 6.2 | 6.3 | 6.2 | |
| Age 25–40 (%) | 30.3 | 26.7 | 33.5 | ||
| Age 40–60 (%) | 47.8 | 50 | 45.7 | ||
| Over 60 years old (%) | 15.7 | 17 | 14.6 | ||
| Education | Junior high school and below (%) | 25 | 30.7 | 14 | |
| High School/Junior College (%) | 36.5 | 40.1 | 33.2 | ||
| College/bachelor and above (%) | 38.5 | 29.2 | 52.8 | ||
| Employment status | Employed (%) | 61.9 | 56.5 | 67 | |
| Unemployed (%) | 8.7 | 11.2 | 6.4 | ||
| Retired (%) | 29.4 | 32.3 | 26.6 | ||
| Health insurance | Yes (%) | 79.3 | 76.8 | 81.5 | |
| No (%) | 20.7 | 23.2 | 18.5 | ||
| Medical checkup | Yes (%) | 47.8 | 38 | 56.8 | |
| No (%) | 52.2 | 62 | 43.2 | ||
| Per capita annual income (10,000 CNY) | <1 (%) | 6.7 | 8.8 | 4.8 | |
| 1–3 (%) | 39.3 | 46 | 33.2 | ||
| 3–5 (%) | 26.9 | 24 | 29.5 | ||
| 5–10 (%) | 21.4 | 17.3 | 25.2 | ||
| >10 (%) | 5.7 | 3.9 | 7.3 | ||
| Per capita housing area (m2) | <30 (%) | 35.5 | 38.7 | 32.6 | |
| 30–60 (%) | 36 | 31.9 | 39.8 | ||
| >60 (%) | 28.5 | 29.4 | 27.6 | ||
| Density of medical facilities | Number per km2 in the buffer (units/km2) | Means | 12.80 | 11.00 | 14.60 |
| Standard deviation | 5.74 | 6.01 | 5.16 | ||
| Health/unhealthy food store ratio | Ratio of healthy to unhealthy food stores in the buffer zone (%) | Means | 37.97 | 38.2 | 37.77 |
| Standard deviation | 13.82 | 15.80 | 12.49 | ||
| Density of traffic stations | Number per km2 in the buffer (units/km2) | Means | 6.01 | 7.51 | 4.51 |
| Standard deviation | 2.87 | 2.06 | 2.85 | ||
| Density of road intersections | Number per km2 in the buffer (units/km2) | Means | 11.77 | 12.78 | 10.76 |
| Standard deviation | 3.63 | 3.36 | 3.79 | ||
| Parks and squares area | Area of the park square in the buffer zone (hm2) | Means | 8.30 | 7.28 | 9.33 |
| Standard deviation | 4.57 | 4.44 | 4.72 | ||
| Building density | Building density in the community (%) | Means | 28.64 | 30.8 | 26.50 |
| Standard deviation | 10.17 | 10.96 | 9.45 | ||
| Floor area ratio | Volume ratio in the community (dimensionless) | Means | 1.45 | 1.26 | 1.64 |
| Standard deviation | 0.53 | 0.47 | 0.51 | ||
| Average self-assessed health status | Means | 82.02 | 80.73 | 83.33 | |
| Standard deviation | 13.02 | 13.49 | 12.16 | ||
| Sample size | 1764 | 840 | 924 | ||
| Explanatory Variables | Full Sample | High-End Community Sample | Low-End Community Sample | ||
|---|---|---|---|---|---|
| Individual attributes | Gender (Refer to: male) | Female | 0.608 | 0.992 | 0.037 |
| Age | −0.268 *** | −0.280 *** | −0.254 *** | ||
| Education (Refer to: Junior high school and below) | School/Junior College | 0.499 | −0.088 | 0.771 | |
| College/bachelor and above (%) | 1.158 * | 0.998 * | 1.148 | ||
| Employment status (Refer to: Employed) | Retired | −2.867 *** | −3.150 *** | −3.408 ** | |
| Unemployed | −6.716 *** | −3.819 * | −9.667 * | ||
| Per capita annual income | 0.101 | 0.131 | 0.122 | ||
| Per capita housing area | −0.047 *** | −0.037 *** | −0.056 | ||
| Medical checkup (Refer to: No) | Yes | 0.835 *** | 0.519 * | 1.131 *** | |
| Health insurance (Refer to: No) | Yes | 0.451 * | 0.263 | 0.593 ** | |
| Environment Variables | Health/unhealthy food store ratio | 0.812 *** | 0.475 | 1.281 *** | |
| Density of medical facilities | 1.606 *** | 1.931 | 1.359 *** | ||
| Parks and squares area | 3.478 *** | 2.587 | 3.909 *** | ||
| Density of traffic stations | 1.015 *** | 1.848 ** | 0.359 *** | ||
| Density of road intersections | −0.899 ** | 1.023 * | −1.291 ** | ||
| Building density | −0.331 *** | −0.256 | −0.418 *** | ||
| Floor area ratio | −0.903 | −2.934 *** | −0.685 * | ||
| Null model | Variance between groups | 12.727 | 3.39121 | 23.679 | |
| Within-group variance | 152.148 | 124.566 | 183.888 | ||
| ICC | 7.713% | 2.649% | 11.408% | ||
| Complete model | Variance between groups | 2.943 | 2.894 | 1.697 | |
| Within-group variance | 127.169 | 103.284 | 153.284 | ||
| ICC | 2.264% | 2.730% | 1.094% | ||
| Between-group variance reduction ratio | 76.8% | 14.7% | 92.8% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, M.; Pan, H.; Shan, Z.; Feng, D. Spatial Differences in the Effect of Communities’ Built Environment on Residents’ Health: A Case Study in Wuhan, China. Int. J. Environ. Res. Public Health 2022, 19, 1392. https://doi.org/10.3390/ijerph19031392
Yuan M, Pan H, Shan Z, Feng D. Spatial Differences in the Effect of Communities’ Built Environment on Residents’ Health: A Case Study in Wuhan, China. International Journal of Environmental Research and Public Health. 2022; 19(3):1392. https://doi.org/10.3390/ijerph19031392
Chicago/Turabian StyleYuan, Man, Haolan Pan, Zhuoran Shan, and Da Feng. 2022. "Spatial Differences in the Effect of Communities’ Built Environment on Residents’ Health: A Case Study in Wuhan, China" International Journal of Environmental Research and Public Health 19, no. 3: 1392. https://doi.org/10.3390/ijerph19031392
APA StyleYuan, M., Pan, H., Shan, Z., & Feng, D. (2022). Spatial Differences in the Effect of Communities’ Built Environment on Residents’ Health: A Case Study in Wuhan, China. International Journal of Environmental Research and Public Health, 19(3), 1392. https://doi.org/10.3390/ijerph19031392