
A Game-Based Approach to Lower Blood Pressure? Comparing Acute Hemodynamic Responses to Endurance Exercise and Exergaming: A Randomized Crossover Trial


 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Baseline Assessments
2.4. Incremental Exercise Test
2.5. Hemodynamic Measurements
2.6. ExerCube
2.7. Moderate Endurance Exercise
2.8. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global disparities of hypertension prevalence and control. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Goodman, J.; Nolan, R.; Lacombe, S.; Thomas, S.G. Blood pressure responses to acute and chronic exercise are related in prehypertension. Med. Sci. Sports Exerc. 2012, 4, 1644–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hecksteden, A.; Grütters, T.; Meyer, T. Association between postexercise hypotension and long-term training-induced blood pressure reduction: A pilot study. Clin. J. Sport Med. 2013, 23, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Halliwill, J.R. Mechanisms and Clinical Implications of Post-exercise Hypotension in humans. Exerc. Sport Sci. Rev. 2001, 29, 65–70. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef]
- Sween, J.; Wallington, S.F.; Sheppard, V.; Taylor, T.; Llanos, A.A.; Adams-Campbell, L.L. The Role of Exergaming in Improving Physical Activity: A Review. J. Phys. Act. Health 2014, 11, 864–870. [Google Scholar] [CrossRef] [Green Version]
- Howe, C.A.; Barr, M.W.; Winner, B.C.; Kimble, J.R.; White, J.B. The physical activity energy cost of the latest active video games in young adults. J. Phys. Act. Health 2015, 12, 171–177. [Google Scholar] [CrossRef]
- Biddiss, E.; Irwin, J. Active video games to promote physical activity in children and youth: A systematic review. Arch. Pediatr. Adolesc. Med. 2010, 164, 664–672. [Google Scholar] [CrossRef]
- Martin-Niedecken, A.L.; Segura, E.M.; Rogers, K.; Niedecken, S.; Vidal, L.T. Towards socially immersive fitness games: An exploratory evaluation through embodied sketching. In Proceedings of the CHI Play 2019—Annual Symposium on Computer-Human Interaction in Play, Barcelona, Spain, 22–25 October 2019; pp. 525–534. [Google Scholar]
- Martin-Niedecken, A.L.; Mahrer, A.; Rogers, K.; de Bruin, E.D.; Schättin, A. “HIIT” the ExerCube: Comparing the Effectiveness of Functional High-Intensity Interval Training in Conventional vs. Exergame-Based Training. Front. Comput. Sci. 2020, 2, 33. [Google Scholar] [CrossRef]
- Martin-Niedecken, A.L.; Rogers, K.; Vidal, L.T.; Mekler, E.D.; Segura, E.M. Exercube vs. Personal trainer: Evaluating a ho-listic, immersive, and adaptive fitness game setup. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems, Glasgow, Scotland, UK, 4–9 May 2019; pp. 1–15. [Google Scholar]
- Wang, K.L.; Cheng, H.M.; Chuang, S.Y.; Spurgeon, H.A.; Ting, C.T.; Lakatta, E.G.; Yin, F.C.; Chou, P.; Chen, C.-H. Central or peripheral systolic or pulse pressure: Which best relates to target organs and future mortality? J. Hypertens. 2009, 27, 461–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esformes, J.I.; Norman, F.; Sigley, J.; Birch, K.M. The influence of menstrual cycle phase upon postexercise hypotension. Med. Sci. Sports Exerc. 2006, 38, 484–491. [Google Scholar] [CrossRef]
- Dickhuth, H.-H.; Huonker, M.; Münzel, T.; Drexler, H.; Berg, A.; Keul, J. Individual Anaerobic Threshold for Evaluation of Competitive Athletes and Patients with Left Ventricular Dysfunction. In Advances in Ergometry; Bachl, N., Graham, T.E., Löllgen, H., Eds.; Springer: Berlin/Heidelberg, Germany, 1991; pp. 173–179. [Google Scholar]
- Franssen, P.M.; Imholz, B.P. Evaluation of the Mobil-O-Graph new generation ABPM device using the ESH criteria. Blood Press. Monit. 2010, 15, 229–231. [Google Scholar] [CrossRef]
- Weisell, R.C. Body mass index as an indicator of obesity. Asia Pac. J. Clin. Nutr. 2002, 11, S681–S684. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Halliwill, J.R.; Buck, T.M.; Lacewell, A.N.; Romero, S.A. Postexercise hypotension and sustained postexercise vasodilatation: What happens after we exercise? Exp. Physiol. 2013, 98, 7–18. [Google Scholar] [CrossRef]
- Bond, B.; Hind, S.; Williams, C.A.; Barker, A.R. The Acute Effect of Exercise Intensity on Vascular Function in Adolescents. Med. Sci. Sports Exerc. 2015, 47, 2628–2635. [Google Scholar] [CrossRef] [Green Version]
- Carpio-Rivera, E.; Moncada-Jiménez, J.; Salazar-Rojas, W.; Solera-Herrera, A. Acute effects of exercise on blood pressure: A meta-analytic investigation. Arq. Bras. Cardiol. 2016, 106, 422–433. [Google Scholar] [CrossRef]
- Milatz, F.; Ketelhut, S.; Ketelhut, R.G. Favorable effect of aerobic exercise on arterial pressure and aortic pulse wave velocity during stress testing. Vasa—Eur. J. Vasc. Med. 2015, 44, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; Guidry, M.A.; Blanchard, B.E.; Kerr, A.; Taylor, A.L.; Johnson, A.N.; Maresh, C.M.; Rodriguez, N.; Thompson, P.D. Exercise intensity alters postexercise hypotension. J. Hypertens. 2004, 22, 1881–1888. [Google Scholar] [CrossRef]
- Pierce, D.R.; Doma, K.; Raiff, H.; Golledge, J.; Leicht, A.S. Influence of exercise mode on post-exercise arterial stiffness and pressure wave measures in healthy adult males. Front. Physiol. 2018, 9, 1468. [Google Scholar] [CrossRef] [Green Version]
- Ketelhut, S.; Milatz, F.; Heise, W.; Ketelhut, R.G. Influence of a high-intensity interval training session on peripheral and central blood pressure at rest and during stress testing in healthy individuals. Vasa—Eur. J. Vasc. Med. 2016, 45, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Middeke, M. Zentraler aortaler Blutdruck: Bedeutender Parameter für Diagnostik und Therapie. Dtsch. Med. Wochenschr. 2017, 142, 1430–1436. [Google Scholar] [CrossRef]
- Goeder, D.; Böhm, B.; Renate, O.; Müller, J. Postexercise changes in peripheral and central blood pressure during a 24-hour ambulatory blood pressure monitoring in healthy young men. J. Sports Med. Phys. Fit. 2019, 59, 1593–1598. [Google Scholar] [CrossRef]
- Romero, S.A.; Minson, C.T.; Halliwill, X.R. The cardiovascular system after exercise. J. Appl. Physiol. 2017, 122, 925–932. [Google Scholar] [CrossRef]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [Green Version]
- Jones, H.; Taylor, C.E.; Lewis, N.C.S.; George, K.; Atkinson, G. Post-exercise blood pressure reduction is greater following intermittent than continuous exercise and is influenced less by diurnal variation. Chronobiol. Int. 2009, 26, 293–306. [Google Scholar] [CrossRef]
- Casonatto, J.; Goessler, K.F.; Cornelissen, V.A.; Cardoso, J.R.; Polito, M.D. The blood pressure-lowering effect of a single bout of resistance exercise: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Prev. Cardiol. 2016, 23, 1700–1714. [Google Scholar] [CrossRef]
- Polito, M.D.; Farinatti, P.T.V. The Effects of Muscle Mass and Number of Sets During Resistance Exercise on Postexercise Hypotension. J. Strength Cond. Res. 2009, 23, 2351–2357. [Google Scholar] [CrossRef]
- Alves da Cruz, M.M.; Ricci-Vitor, A.L.; Bonini Borges, G.L.; Fernanda da Silva, P.; Ribeiro, F.; Marques Vanderlei, L.C. Acute Hemodynamic Effects of Virtual Reality–Based Therapy in Patients of Cardiovascular Rehabilitation: A Cluster Randomized Crossover Trial. Arch. Phys. Med. Rehabil. 2020, 101, 642–649. [Google Scholar] [CrossRef]
- Mills, A.; Rosenberg, M.; Stratton, G.; Carter, H.H.; Spence, A.L.; Pugh, C.J.A.; Green, D.J.; Naylor, L.H. The effect of exergaming on vascular function in children. J. Pediatr. 2013, 163, 806–810. [Google Scholar] [CrossRef]
- McBain, T.; Weston, M.; Crawshaw, P.; Haighton, C.; Spears, I. Development of an exergame to deliver a sustained dose of high-intensity training: Formative pilot randomized trial. JMIR Serious Games 2018, 6, e4. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, M.S.; De Carvalho, L.C.; Menezes, F.D.S.; Frazin, A.; Gomes, E.D.C.; Lunes, D.H. Effects of Exergames in Women with Fibromyalgia: A Randomized Controlled Study. Games Health J. 2020, 9, 358–367. [Google Scholar] [CrossRef]
- Staiano, A.E.; Beyl, R.A.; Guan, W.; Hendrick, C.A.; Hsia, D.S.; Newton, L.R. Home-based exergaming among children with overweight and obesity: A randomized clinical trial. Pediatr. Obes. 2018, 13, 724–733. [Google Scholar] [CrossRef]
- Baranowski, T.; Maddison, R.; Maloney, A.; Medina, E.; Simons, M. Building a Better Mousetrap (Exergame) to Increase Youth Physical Activity. Games Health J. 2014, 3, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Röglin, L.; Ketelhut, S.; Ketelhut, K.; Kircher, E.; Ketelhut, R.G.; Martin-Niedecken, A.L.; Hottenrott, K.; Stoll, O. Adaptive High-Intensity Exergaming: The More Enjoyable Alternative to Conventional Training Approaches Despite Working Harder. Games Health J. 2021, 10, 400–407. [Google Scholar] [CrossRef]
- Carpes, L.; Costa, R.; Schaarschmidt, B.; Reichert, T.; Ferrari, R. High-intensity interval training reduces blood pressure in older adults: A systematic review and meta-analysis. Exp. Gerontol. 2022, 158, 111657. [Google Scholar] [CrossRef]
- Pocatello, L.S.; MacDonald, H.V.; Ash, G.I.; Lamberti, L.M.; Farquhar, W.B.; Arena, R.; Johnson, B.T. Assessing the existing professional exercise recommendations for hypertension: A review and recommendations for future research priorities. Mayo Clin. Proc. 2015, 90, 801–812. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome | Mean ± SD |
|---|---|
| Age (y) | 24.8 ± 3.9 |
| Gender (f/m) | 13/15 |
| Body mass (kg) | 68.9 ± 10.7 |
| Height (cm) | 171.9 ± 9.7 |
| Body-Mass-Index (kg/m2) | 23.2 ± 2.3 |
| Waist-to-height-ratio | 0.4 ± 0.1 |
| HRmax (bpm) | 194.1 ± 7.7 |
| Exergaming Session | p-Value * | Moderate Endurance Exercise | p-Value * | |
|---|---|---|---|---|
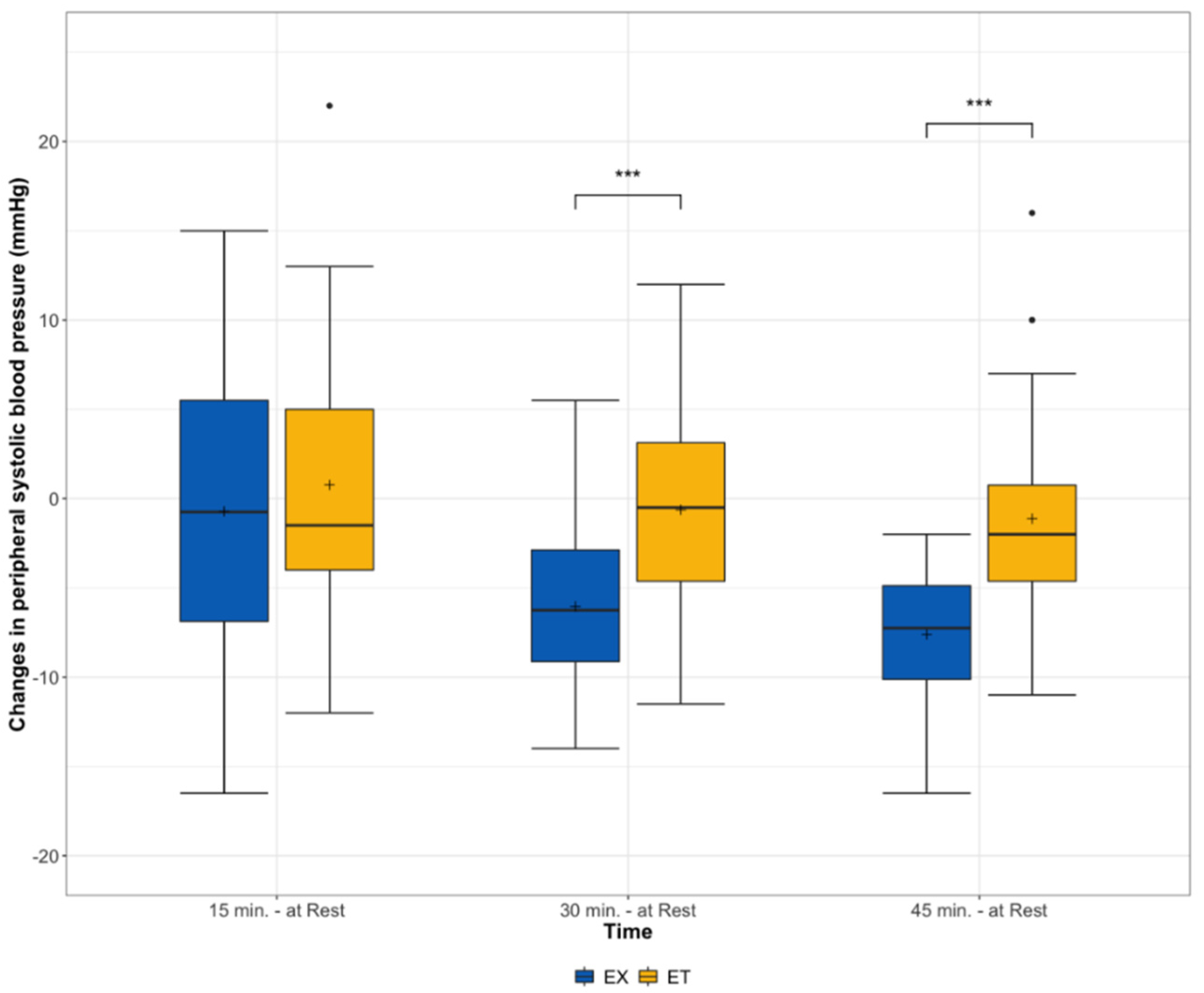
| Peripheral SBP (mmHg) | ||||
| At rest (reference) | 119.8 (115.1, 129.8) | 118.8 (111.3, 124.6) | ||
| 15 min | 122.5 (107.0, 129.5) | p = 0.615 | 119.5 (107.0, 128.3) | p = 0.969 |
| 30 min | 116.5 (107.8, 121.5) | p < 0.001 | 118.0 (110.5, 124.3) | p = 0.544 |
| 45 min | 113.5 (106.0, 119.0) | p < 0.001 | 117.0 (111.8, 122.3) | p = 0.137 |
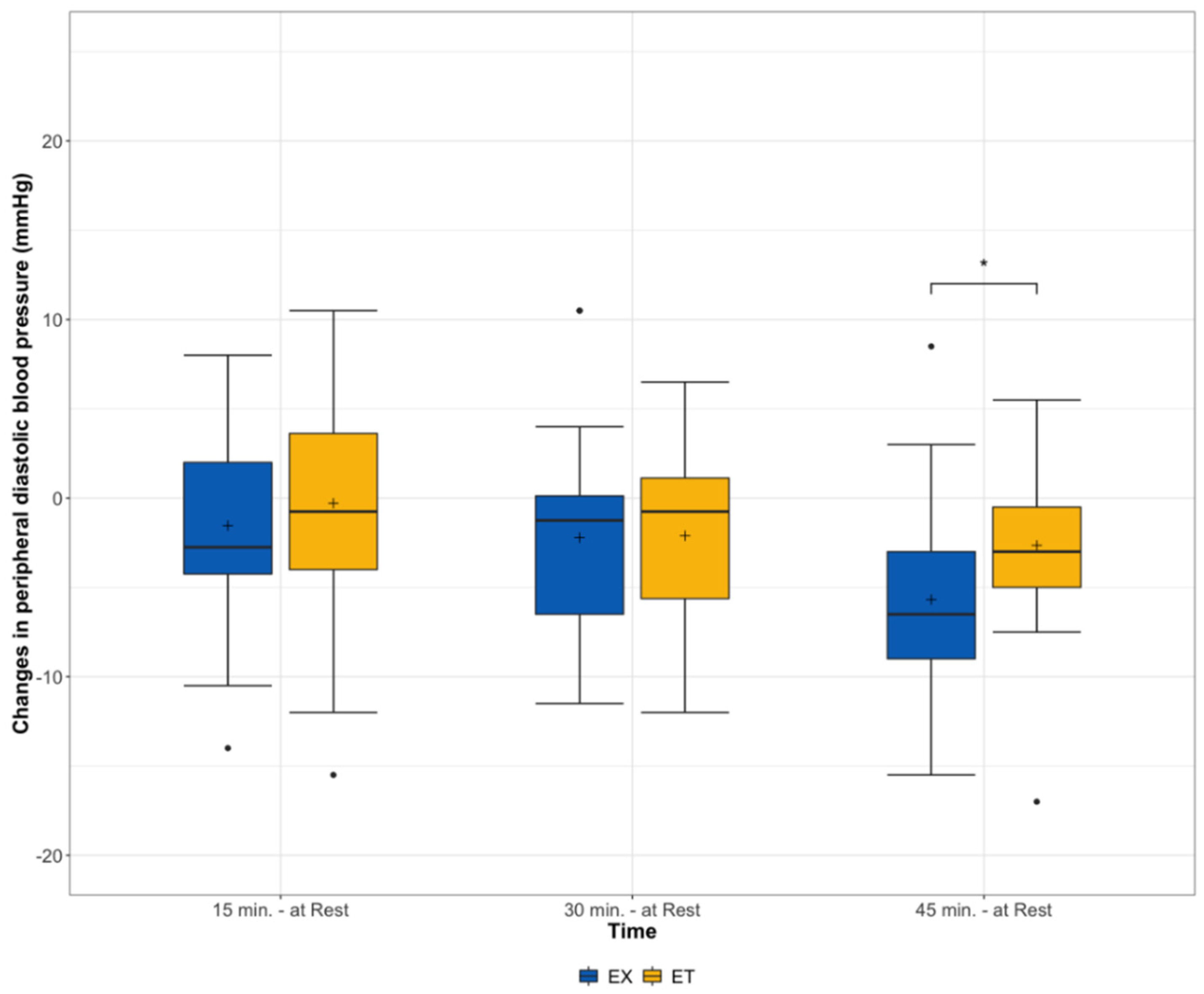
| Peripheral DBP (mmHg) | ||||
| At rest (reference) | 69.8 (66.0, 74.1) | 67.8 (64.4, 74.3) | ||
| 15 min | 68.5 (62.5, 73.3) | p = 0.158 | 70.0 (63.8, 74.3) | p = 0.985 |
| 30 min | 69.5 (61.0, 73.0) | p = 0.028 | 68.0 (61.8, 71.0) | p = 0.060 |
| 45 min | 65.0 (59.8, 69.3) | p < 0.001 | 67.0 (61.0, 72.0) | p = 0.003 |
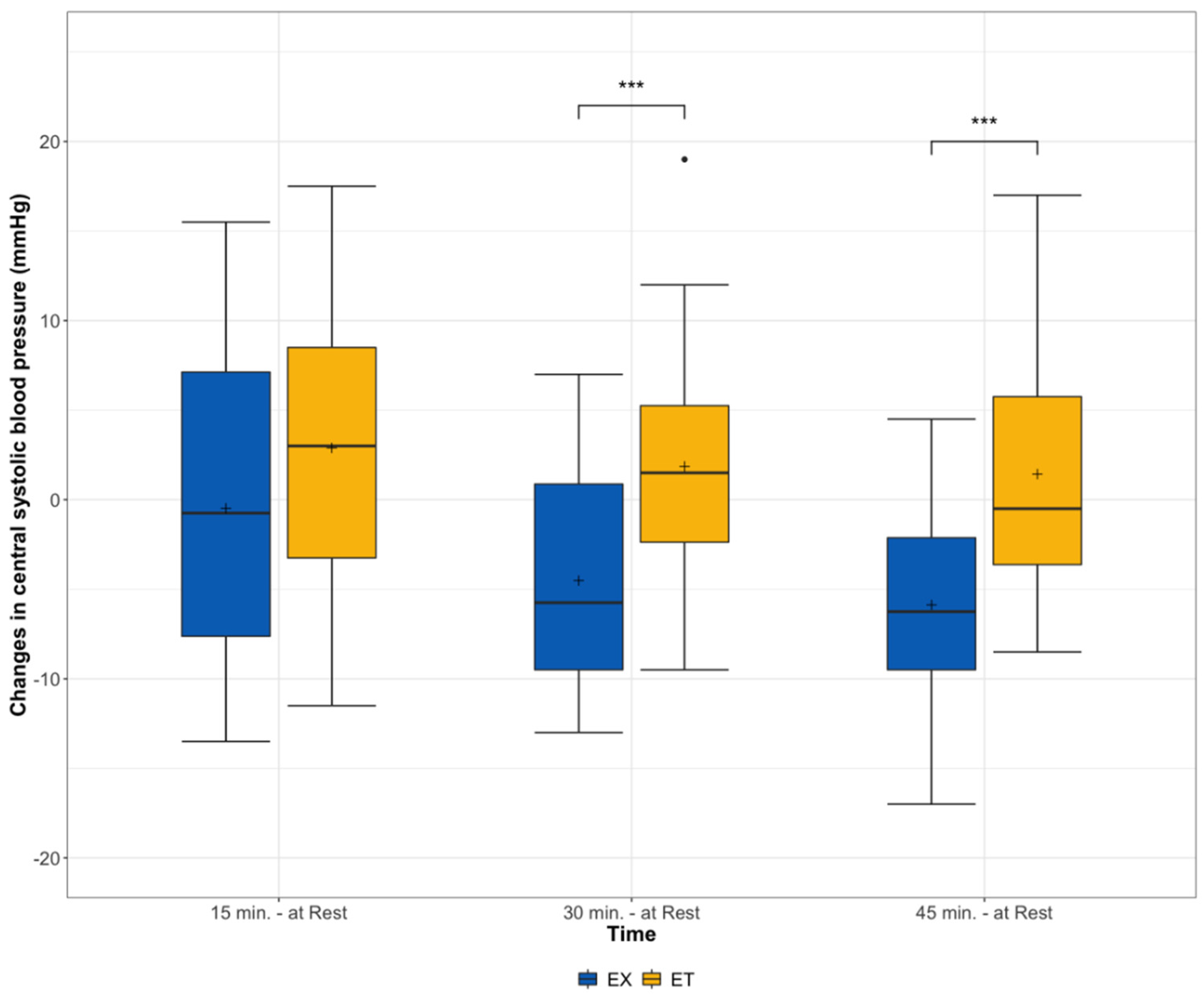
| Central SBP (mmHg) | ||||
| At rest (reference) | 109.8 (103.5, 120.1) | 107.3 (102.8, 113.5) | ||
| 15 min | 110.0 (100.0, 119.3) | p = 0.701 | 111.0 (99.0, 119.0) | p = 0.083 |
| 30 min | 109.5 (99.3, 113.0) | p = 0.001 | 112.5 (100.0, 118.0) | p = 0.195 |
| 45 min | 104.0 (97.8, 112.8) | p < 0.001 | 109.5 (102.0, 114.3) | p = 0.648 |
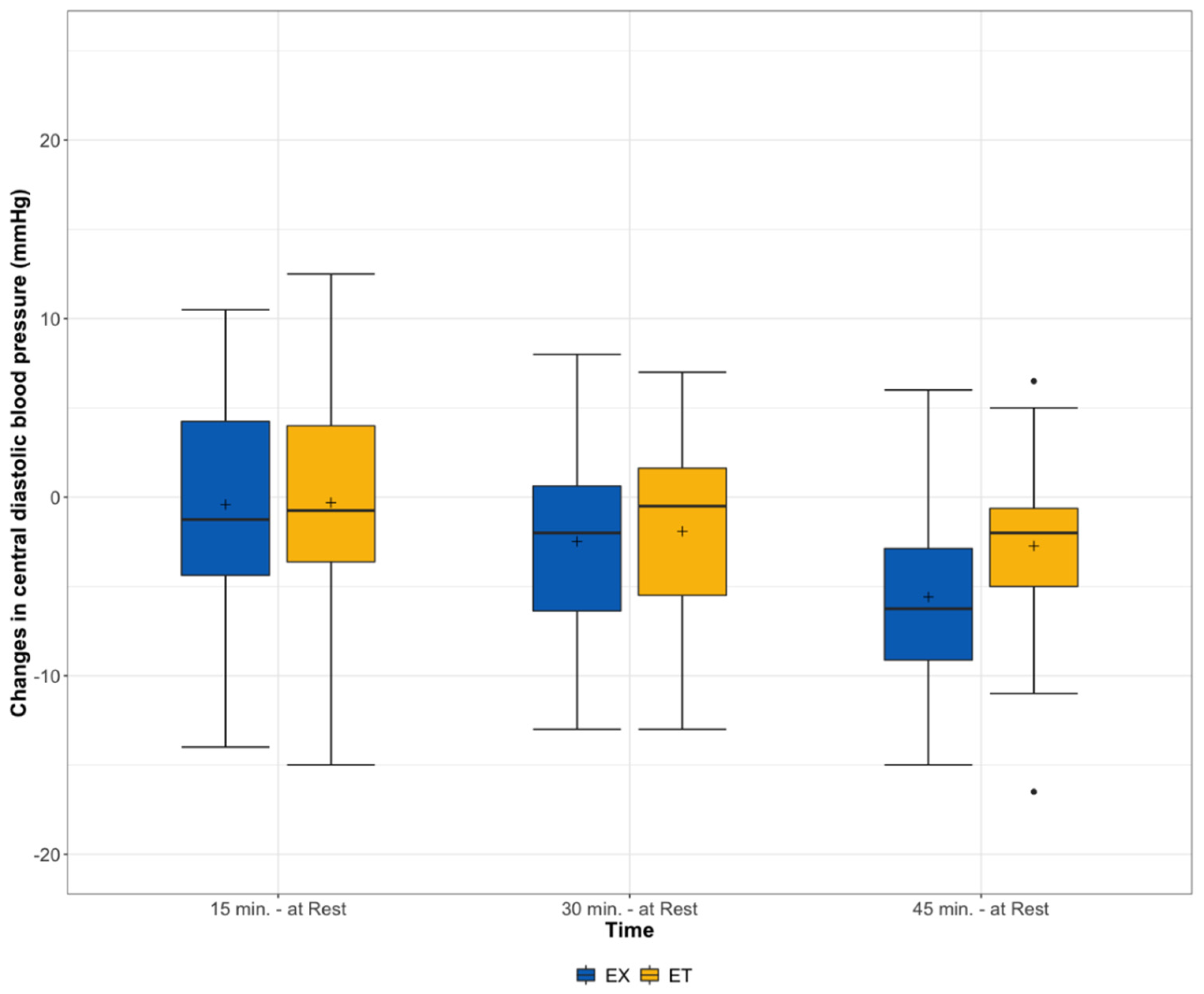
| Central DBP (mmHg) | ||||
| At rest (reference) | 71.3 (67.1, 75.0) | 69.0 (65.4, 75.0) | ||
| 15 min | 72.0 (63.0, 77.3) | p = 0.175 | 70.0 (64.5, 74.3) | p = 0.995 |
| 30 min | 70.0 (62.8, 75.0) | p = 0.024 | 69.0 (62.0, 72.3) | p = 0.102 |
| 45 min | 66.0 (60.5, 70,3) | p < 0.001 | 67.5 (61.0, 70.3) | p = 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kircher, E.; Ketelhut, S.; Ketelhut, K.; Röglin, L.; Hottenrott, K.; Martin-Niedecken, A.L.; Ketelhut, R.G. A Game-Based Approach to Lower Blood Pressure? Comparing Acute Hemodynamic Responses to Endurance Exercise and Exergaming: A Randomized Crossover Trial. Int. J. Environ. Res. Public Health 2022, 19, 1349. https://doi.org/10.3390/ijerph19031349
Kircher E, Ketelhut S, Ketelhut K, Röglin L, Hottenrott K, Martin-Niedecken AL, Ketelhut RG. A Game-Based Approach to Lower Blood Pressure? Comparing Acute Hemodynamic Responses to Endurance Exercise and Exergaming: A Randomized Crossover Trial. International Journal of Environmental Research and Public Health. 2022; 19(3):1349. https://doi.org/10.3390/ijerph19031349
Chicago/Turabian StyleKircher, Eva, Sascha Ketelhut, Kerstin Ketelhut, Lisa Röglin, Kuno Hottenrott, Anna Lisa Martin-Niedecken, and Reinhard G. Ketelhut. 2022. "A Game-Based Approach to Lower Blood Pressure? Comparing Acute Hemodynamic Responses to Endurance Exercise and Exergaming: A Randomized Crossover Trial" International Journal of Environmental Research and Public Health 19, no. 3: 1349. https://doi.org/10.3390/ijerph19031349
APA StyleKircher, E., Ketelhut, S., Ketelhut, K., Röglin, L., Hottenrott, K., Martin-Niedecken, A. L., & Ketelhut, R. G. (2022). A Game-Based Approach to Lower Blood Pressure? Comparing Acute Hemodynamic Responses to Endurance Exercise and Exergaming: A Randomized Crossover Trial. International Journal of Environmental Research and Public Health, 19(3), 1349. https://doi.org/10.3390/ijerph19031349