
Role of Infodemics on Social Media in the Development of People’s Readiness to Follow COVID-19 Preventive Measures


Abstract
:1. Introduction
2. Research Context, Hypotheses, and Methods
2.1. Health Infodemic
2.2. Role of Social Media during COVID-19 Pandemic
2.3. Research Hypotheses
2.3.1. Trust and Citizens’ Perception to Follow COVID-19 Preventive Measures
2.3.2. Attitude and Citizens’ Readiness to Follow COVID-19 Preventive Measures
2.3.3. Perceived Benefit and Citizens’ Readiness to Follow COVID-19 Preventive Measures
2.3.4. Personal Innovativeness and Citizens’ Readiness to Follow COVID-19 Preventive Measures
2.3.5. Peer Referent and Citizens’ Readiness to Follow COVID-19 Preventive Measures
2.3.6. Moderating Effect of Health Infodemic
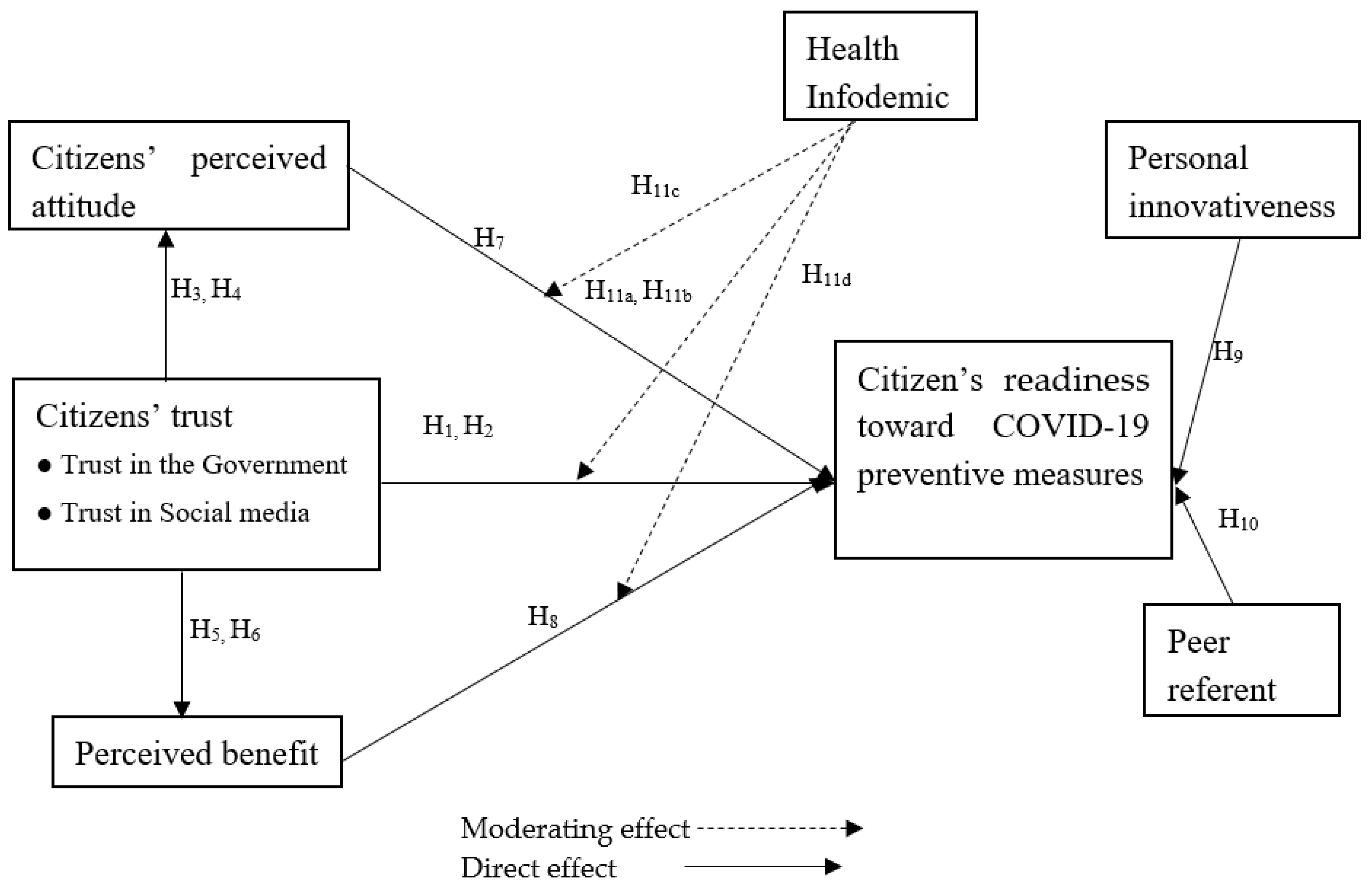
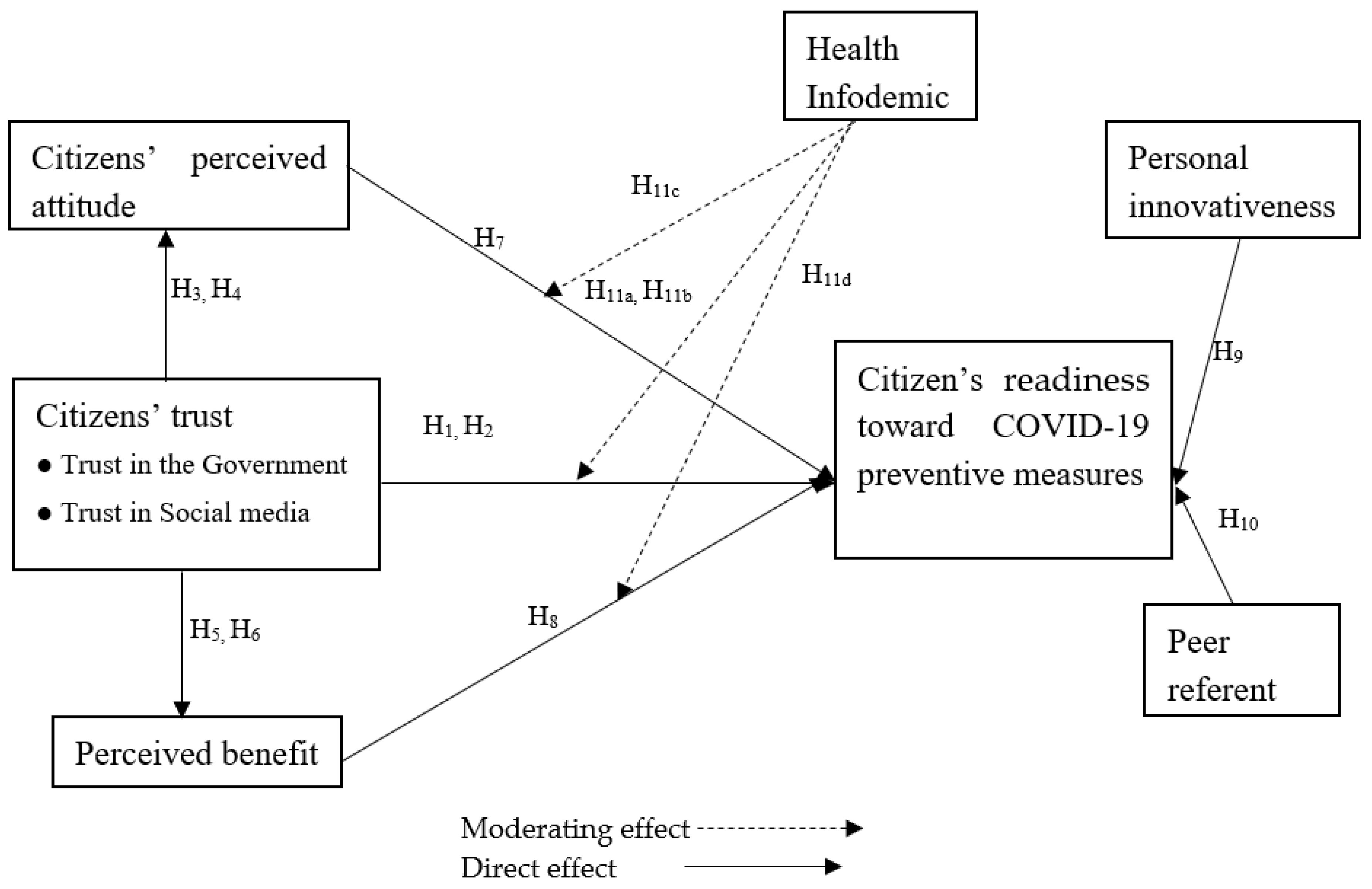
2.3.7. Research Model
3. Materials and Methods
3.1. Measurement and Survey Design
3.2. The Delphi Method
3.3. Data Collection
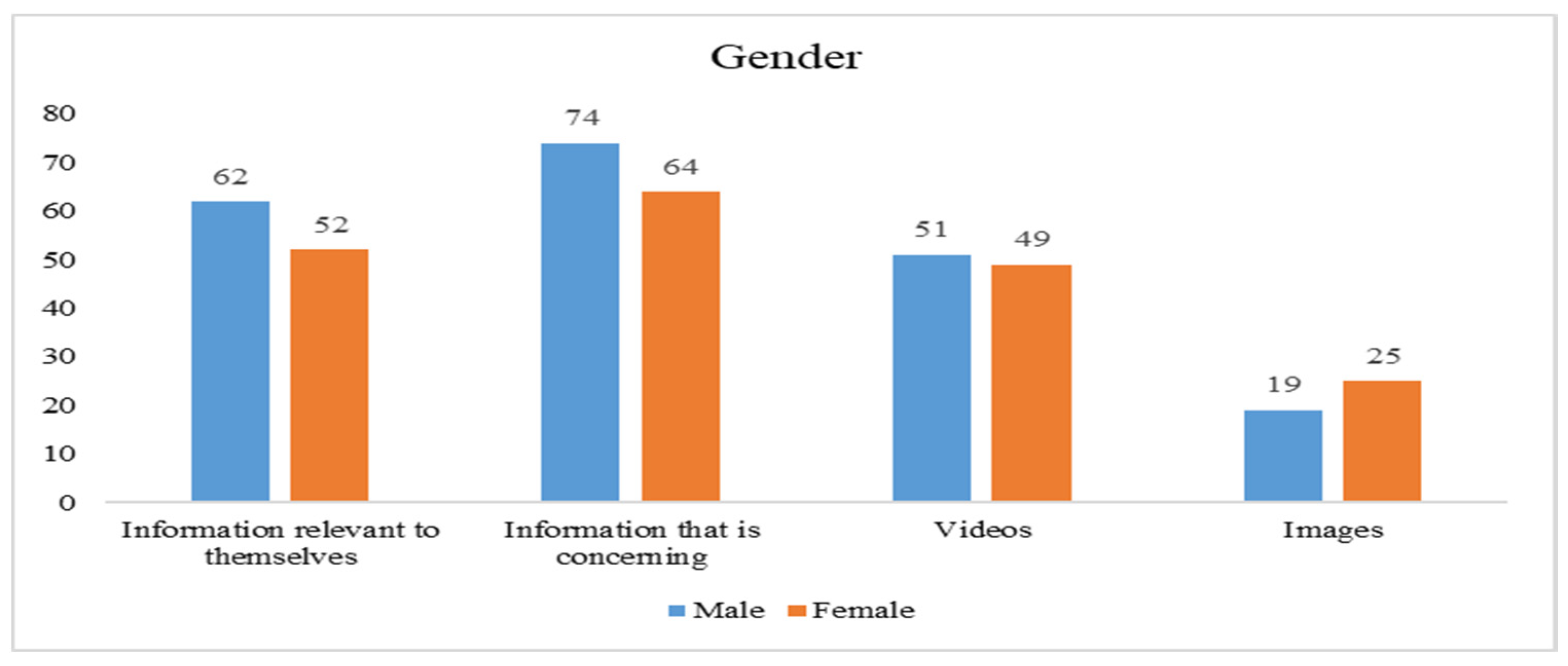
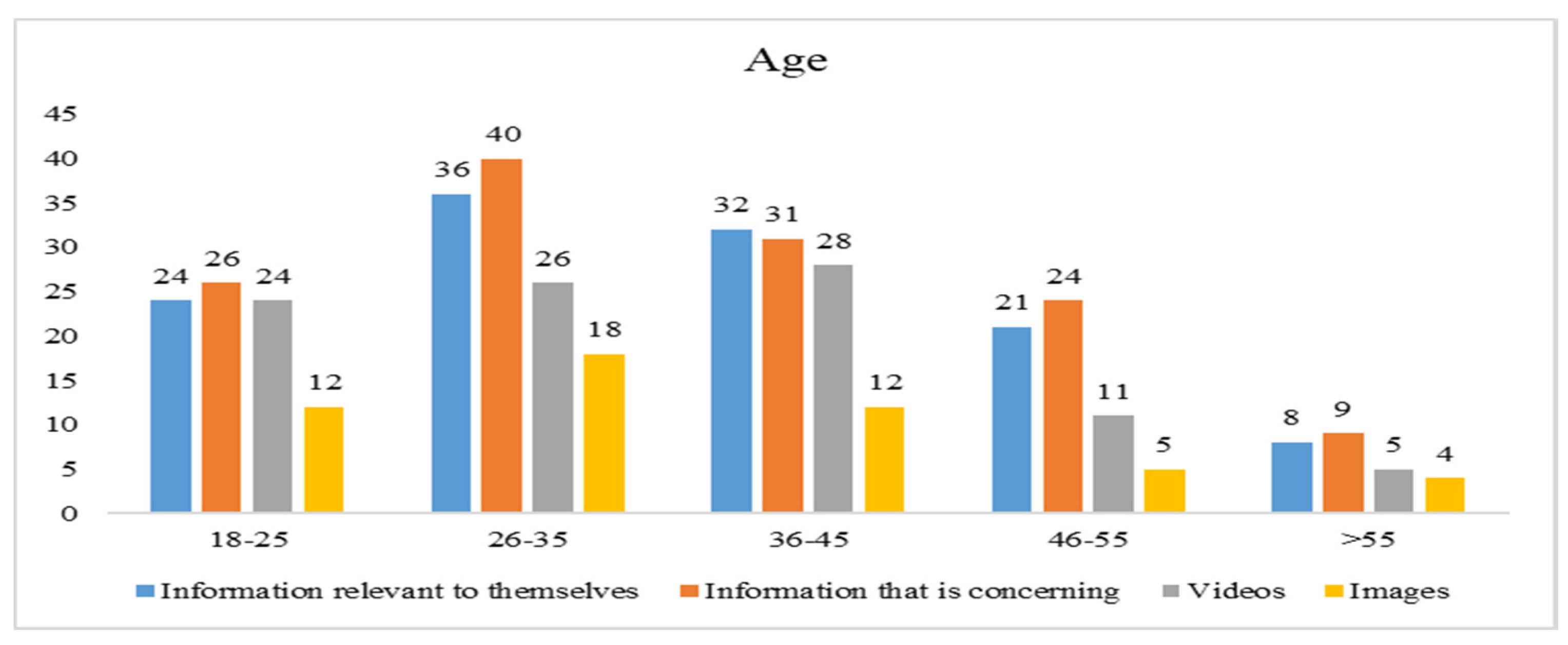
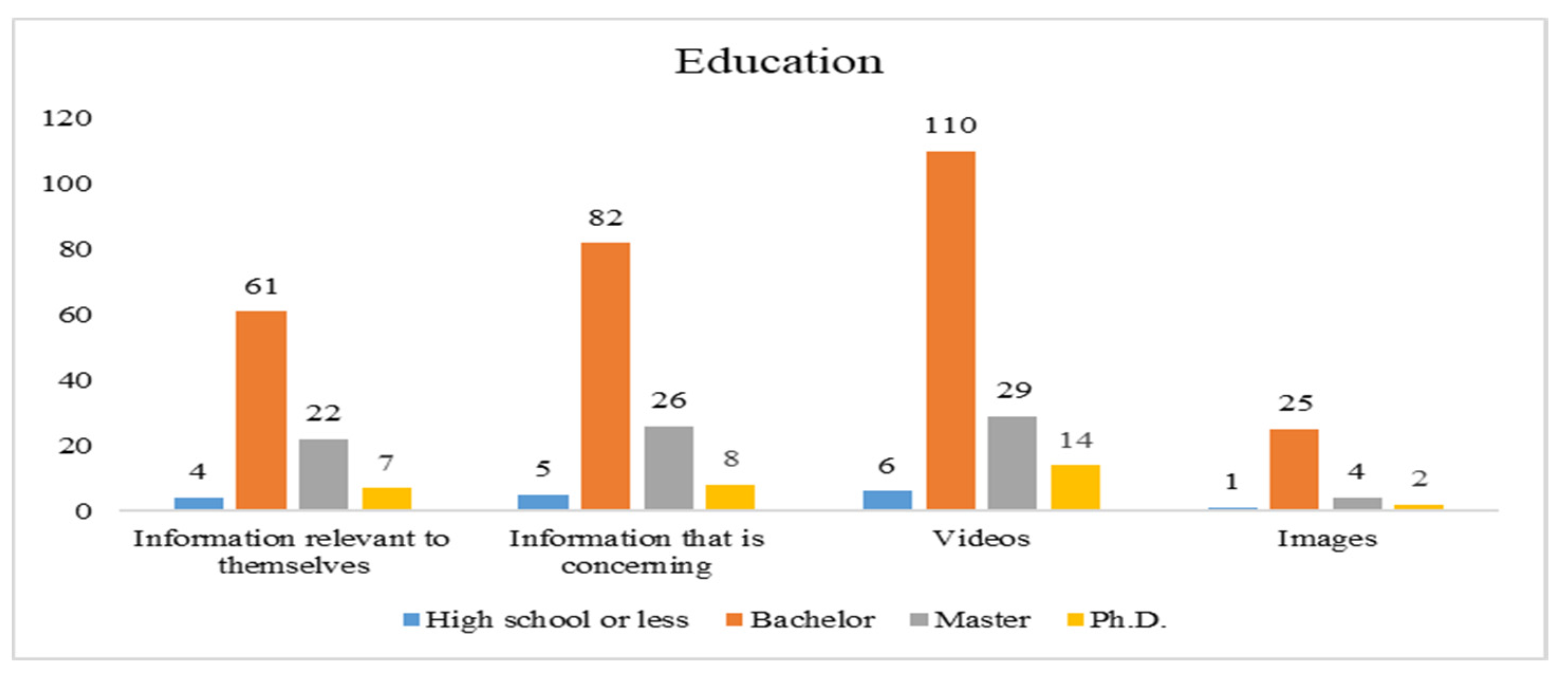
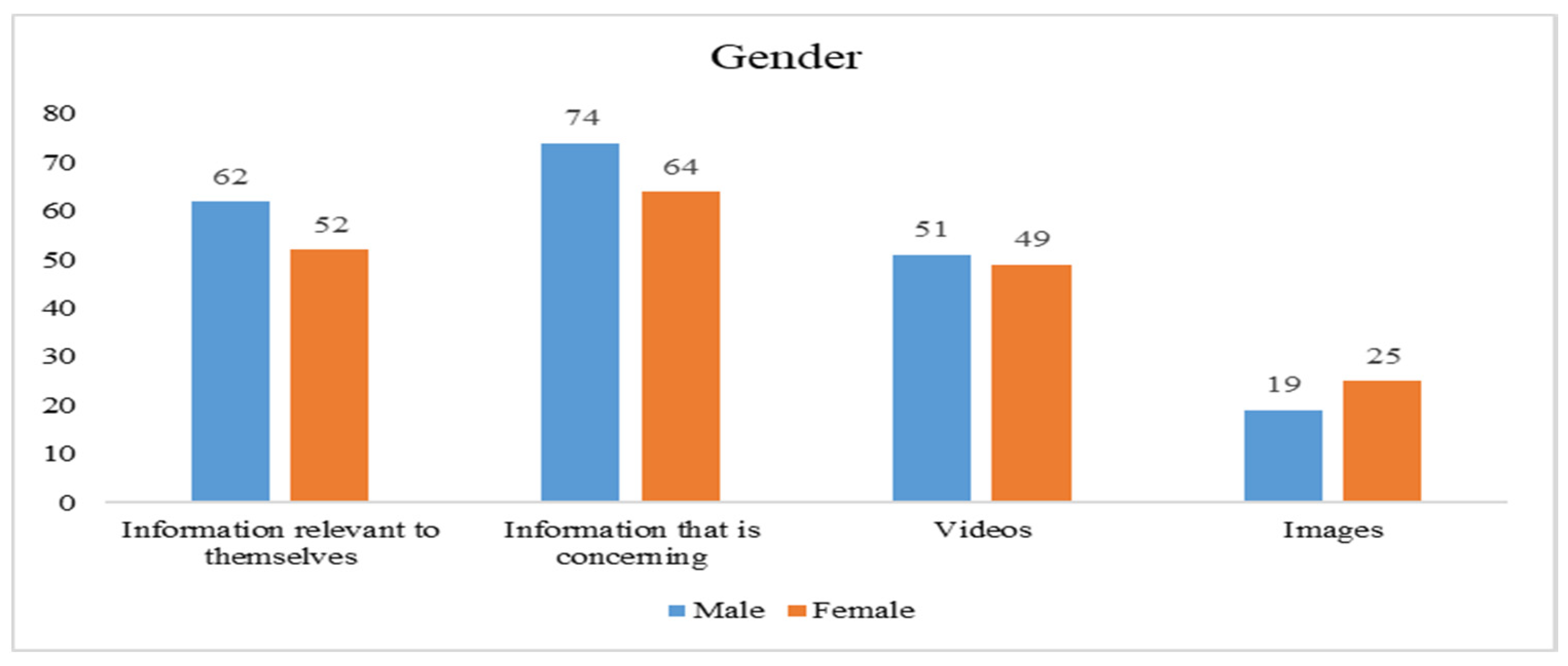
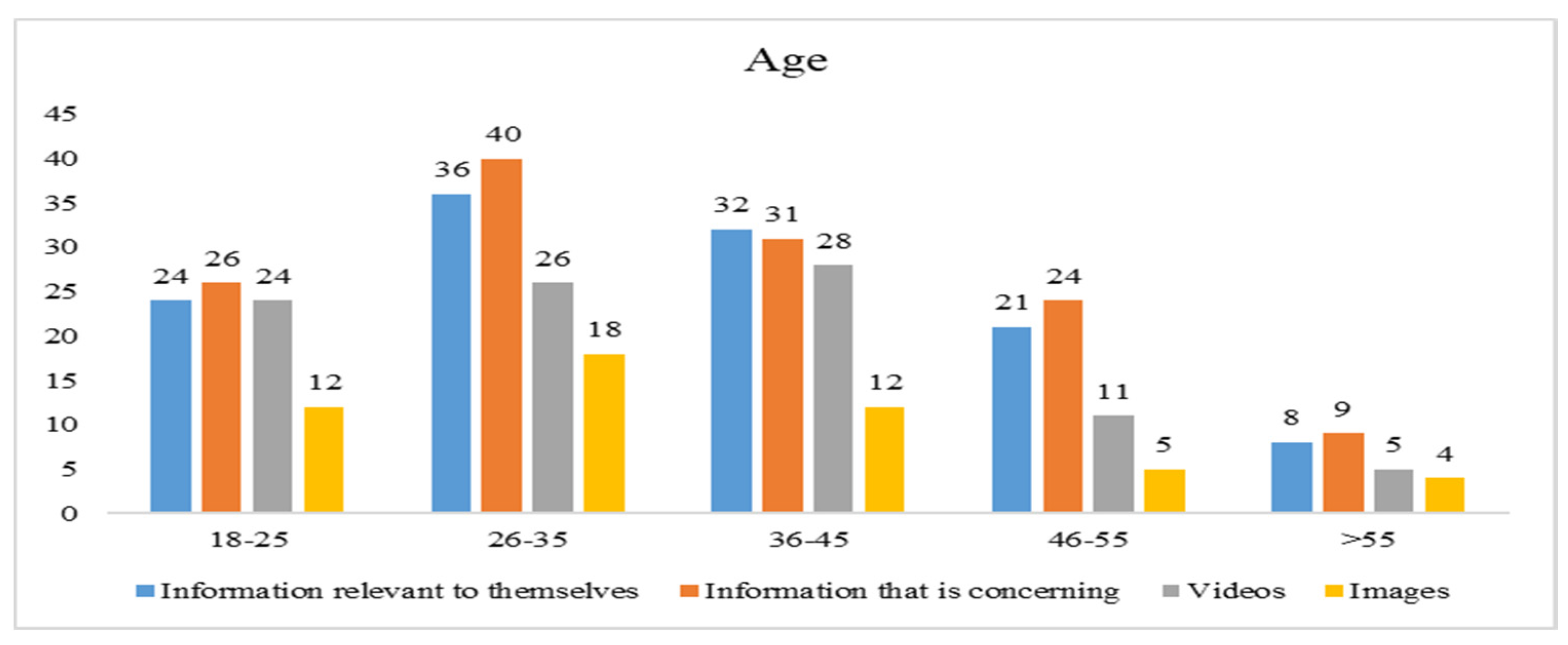
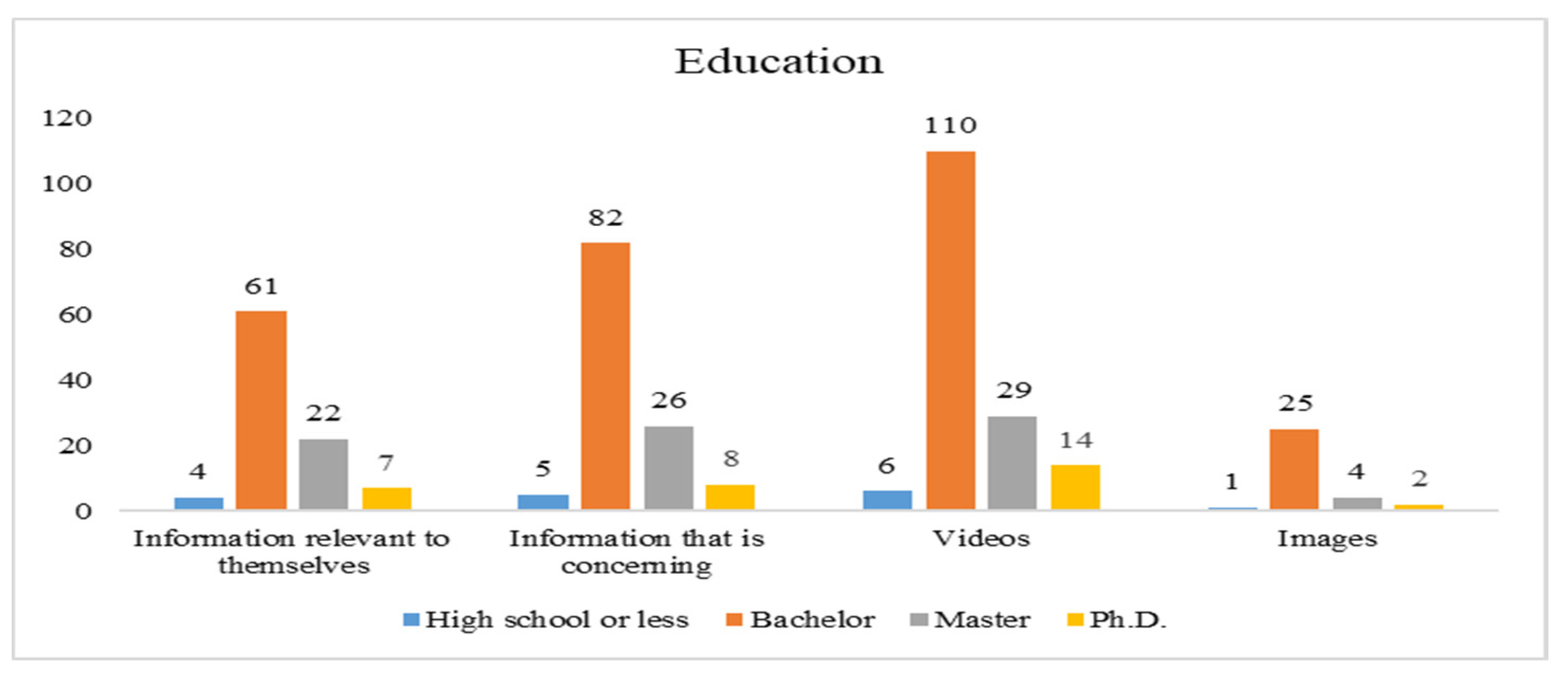
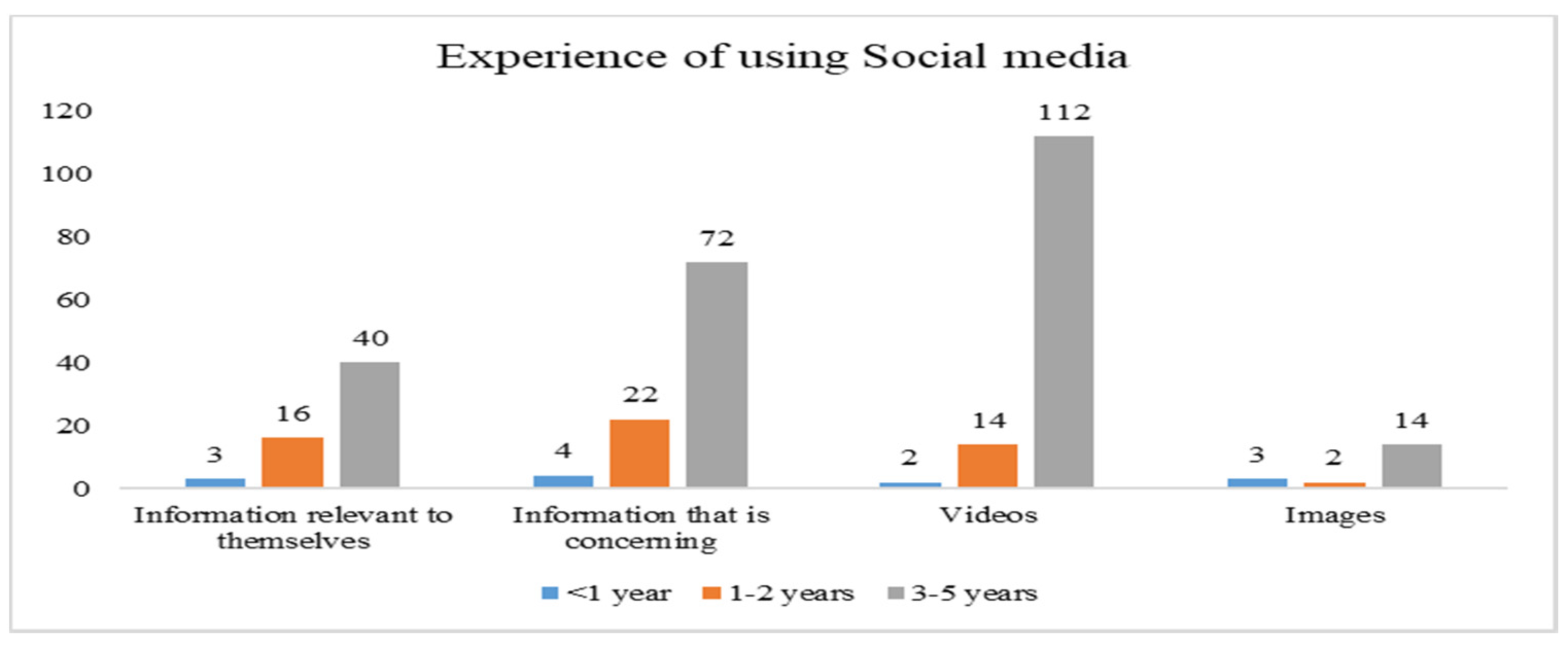
3.4. Demographic Information of Participants
4. Data Analysis
4.1. Descriptive Statistics and Correlation
4.2. Structural Equation Model
4.2.1. Measurement Model
4.2.2. Structural Model Testing
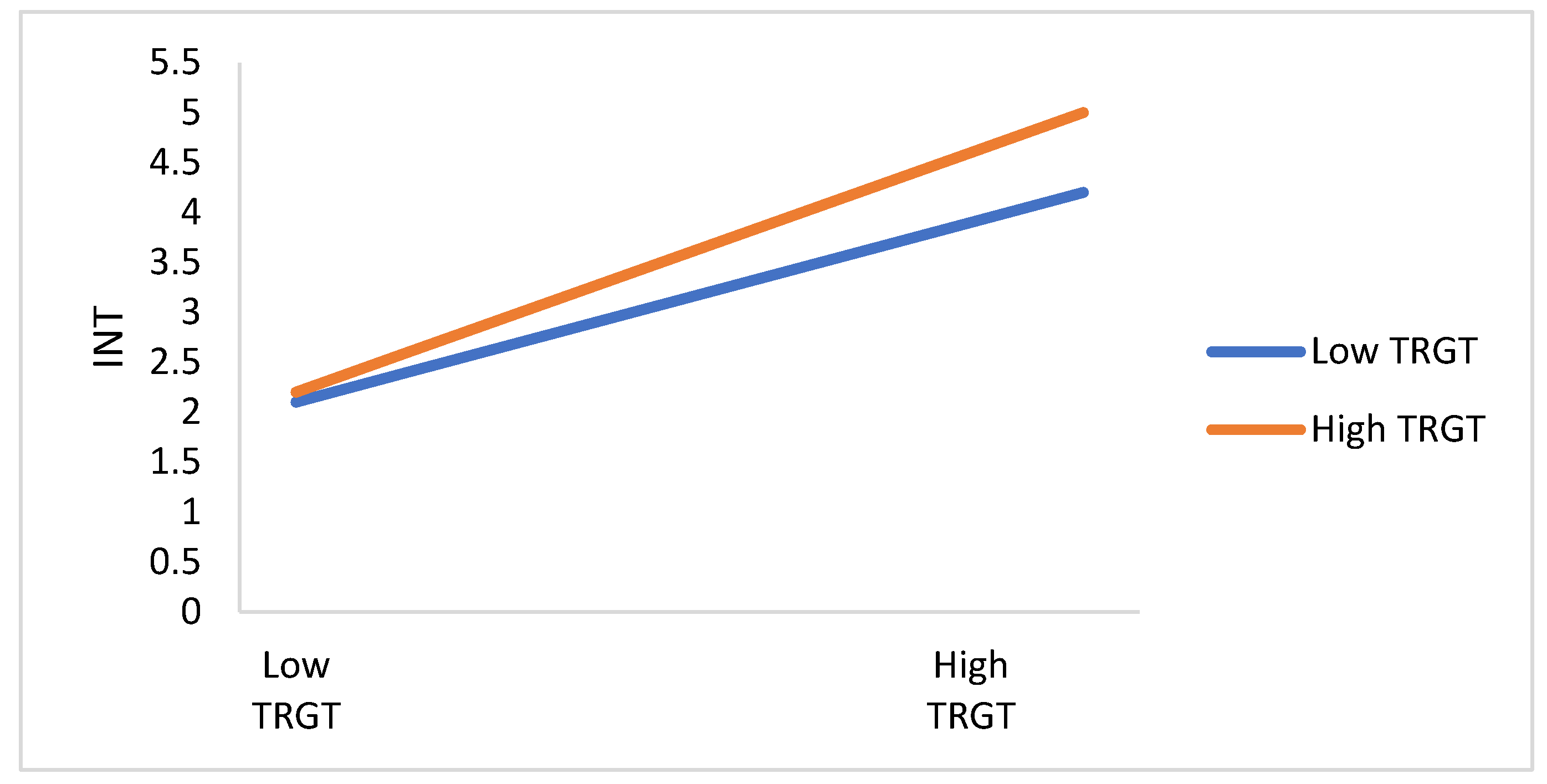
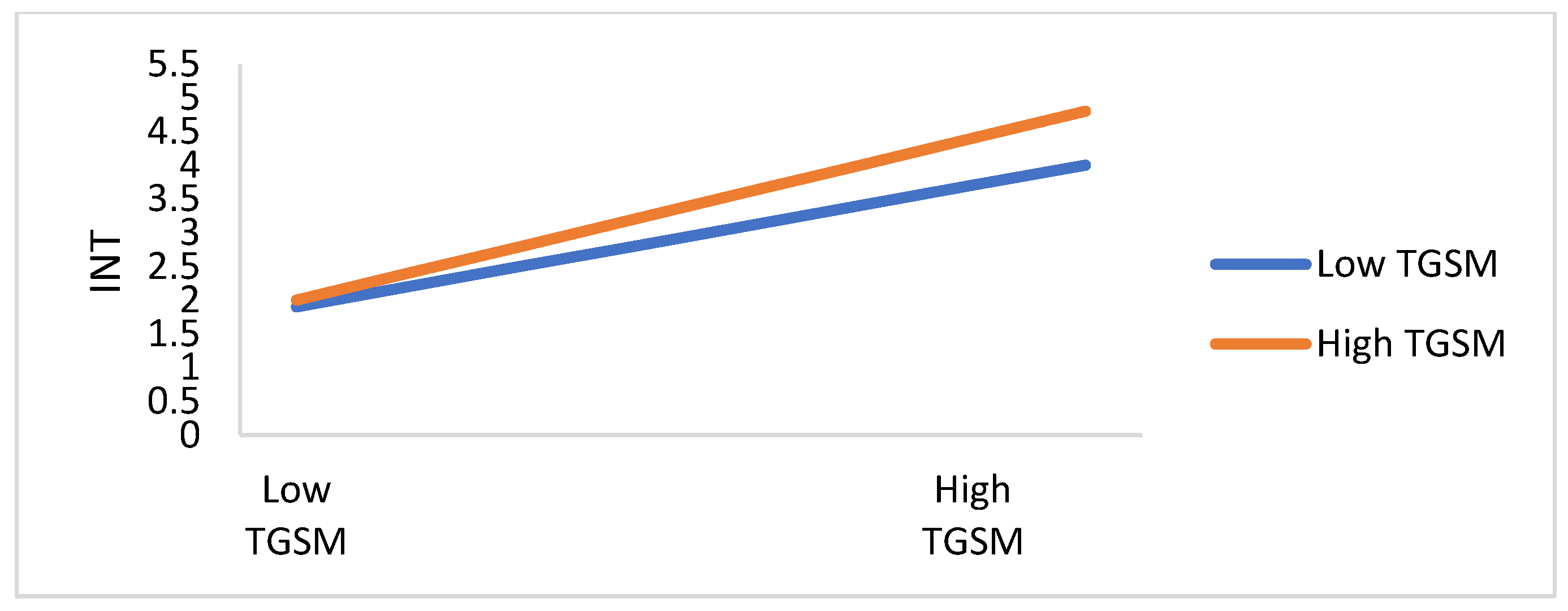
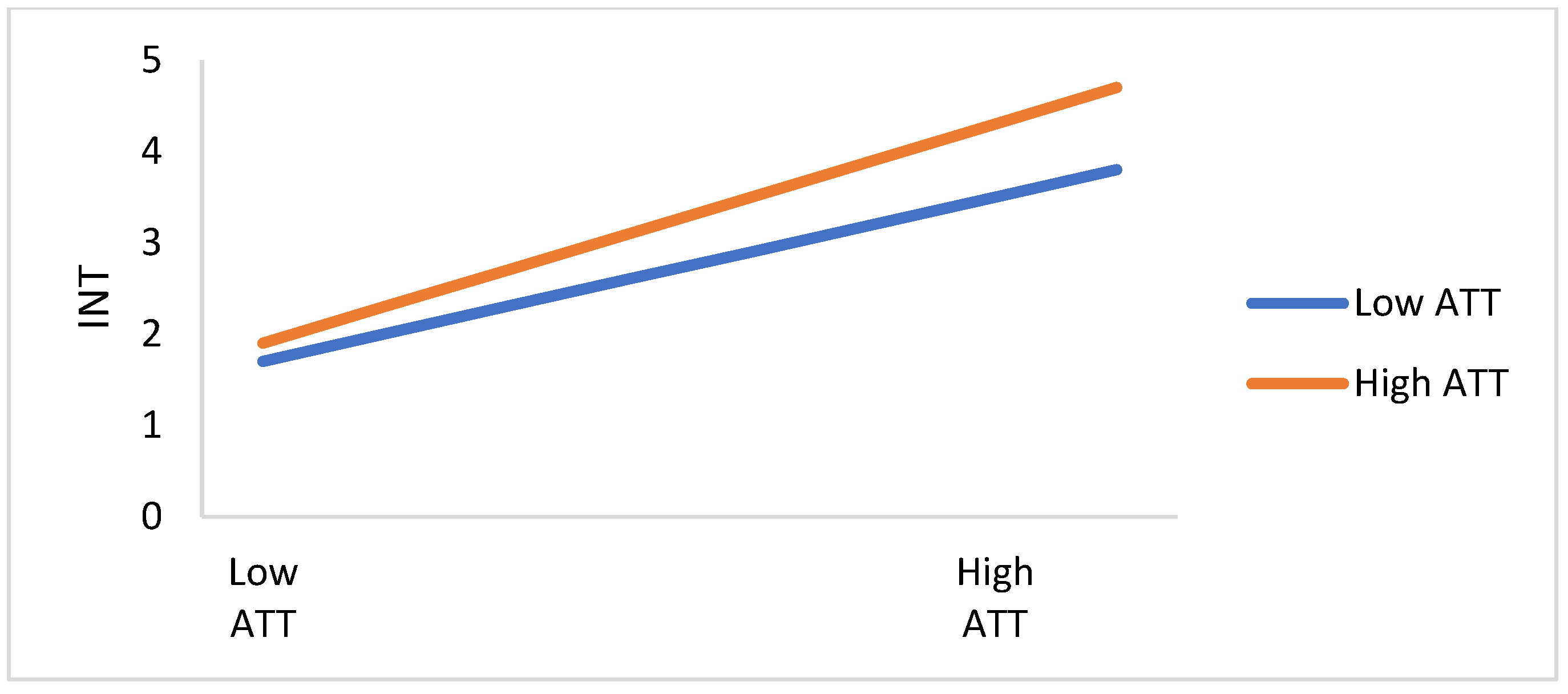
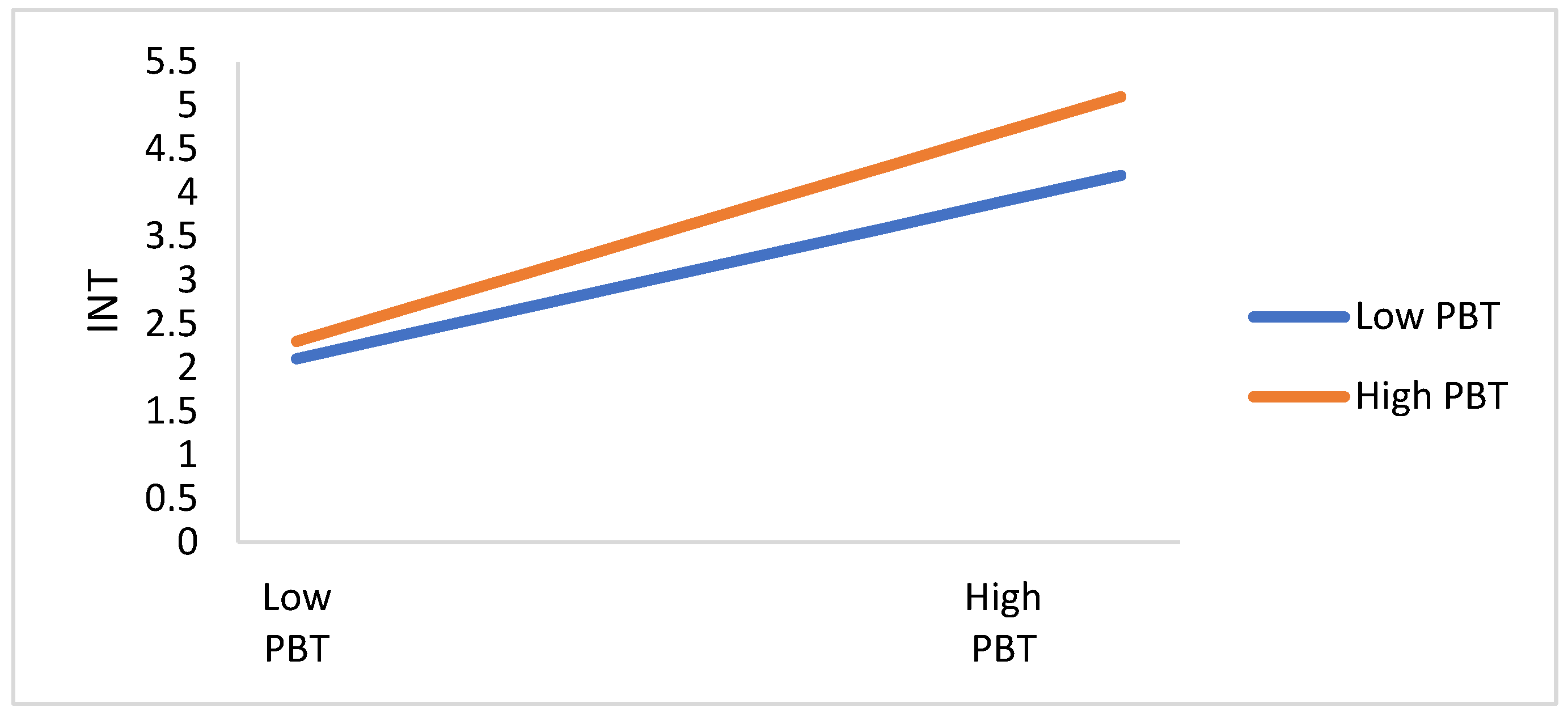
4.2.3. Moderating Investigation
5. Discussion and Conclusions
5.1. Discussion
5.2. Theoretical Implications
5.3. Practical Implications
5.4. Limitations and Future Studies
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Perlman, S. Another decade, another coronavirus. N. Engl. J. Med. 2020, 382, 760–762. [Google Scholar] [CrossRef]
- Prasetyo, Y.T.; Castillo, A.M.; Salonga, L.J.; Sia, J.A.; Seneta, J.A. Factors affecting perceived effectiveness of COVID-19 prevention measures among Filipinos during Enhanced Community Quarantine in Luzon, Philippines: Integrating Protection Motivation Theory and extended Theory of Planned Behavior. Int. J. Infect. Dis. 2020, 99, 312–323. [Google Scholar] [CrossRef]
- Al Kaabi, N.; Zhang, Y.; Xia, S.; Yang, Y.; Al Qahtani, M.M.; Abdulrazzaq, N.; Al Nusair, M.; Hassany, M.; Jawad, J.S.; Abdalla, J.; et al. Effect of 2 Inactivated SARS-CoV-2 Vaccines on Symptomatic COVID-19 Infection in Adults. JAMA 2021, 326, 35–45. [Google Scholar] [CrossRef]
- García, L.F. Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Front. Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef]
- Bauchner, H.; Fontanarosa, P.B.; Livingston, E.H. Conserving Supply of Personal Protective Equipment—A Call for Ideas. JAMA 2020, 323, 1911. [Google Scholar] [CrossRef] [Green Version]
- Taiwan Centers for Disease Control. Available online: https://www.cdc.gov.tw/En (accessed on 1 November 2021).
- Chen, X.; Sin, S.C.J. ‘Misinformation? What of it?’ Motivations and individual differences in misinformation sharing on social media. Proc. Assoc. Inf. Sci. Technol. 2013, 50, 1–4. [Google Scholar] [CrossRef]
- Karlova, N.A.; Fisher, K.E. A social diffusion model of misinformation and disinformation for understanding human information behaviour. Inf. Res. 2013, 18, 1–17. [Google Scholar]
- Budak, C.; Agrawal, D.; Abbadi, A.E. Limiting the spread of misinformation in social networks. In Proceedings of the International World Wide Web Conference, Hyderabad, India, 28 March–1 April 2011. [Google Scholar]
- Potarca, G. The demography of swiping right. An overview of couples who met through dating apps in Switzerland. PLoS ONE 2020, 15, e0243733. [Google Scholar] [CrossRef]
- Birkhäuer, J.; Gaab, J.; Kossowsky, J.; Hasler, S.; Krummenacher, P.; Werner, C.; Gerger, H. Trust in the health care professional and health outcome: A meta-analysis. PLoS ONE 2017, 12, e0170988. [Google Scholar]
- Sun, S.L.; Hwang, H.G.; Dutta, B.; Peng, M.H. Exploring critical factors influencing nurses’ intention to use tablet P.C. in Patients’ care using an integrated theoretical model. Libyan J. Med. 2019, 14, 1648963. [Google Scholar] [CrossRef] [Green Version]
- Alkawsi, G.; Ali, N.; Baashar, Y. The Moderating Role of Personal Innovativeness and Users Experience in Accepting the Smart Meter Technology. Appl. Sci. 2021, 11, 3297. [Google Scholar] [CrossRef]
- WHO Situation Report 13. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200202-sitrep-13-ncov-v3.pdf?sfvrsn=195f4010_6 (accessed on 1 November 2021).
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- World Health Organization. Director-General’s Remarks at the Media Briefing on 2019 Novel Coronavirus on 8 February 2020. Available online: https://www.who.int/dg/speeches/detail/director-general-s-remarks-at-the-media-briefing-on-2019-novel-coronavirus---8-february-2020 (accessed on 1 November 2021).
- Mendoza, M.; Poblete, B.; Castillo, C. Twitter under Crisis: Can We Trust What We RT? Available online: https://dl.acm.org/doi/10.1145/1964858.1964869 (accessed on 1 November 2021).
- Starbird, K.; Maddock, J.; Orand, M.; Achterman, P.; Mason, R.M. Rumors, false flags, and digital vigilantes: Misinformation on twitter after the 2013 boston marathon bombing. IConference 2014 Proc. 2014, 654–662. [Google Scholar] [CrossRef] [Green Version]
- Kim, L.; Fast, S.M.; Markuzon, N. Incorporating media data into a model of infectious disease transmission. PLoS ONE 2019, 14, e0197646. [Google Scholar] [CrossRef] [Green Version]
- Mian, A.; Khan, S. Coronavirus: The spread of misinformation. BMC Med. 2020, 18, 89. [Google Scholar] [CrossRef]
- Yeo-The, N.S.L.; Tang, B.L. An alarming retraction rate for scientific publications on Coronavirus Disease 2019 (COVID-19). Account. Res. 2021, 28, 47–53. [Google Scholar] [CrossRef]
- MattRidly. Available online: https://www.rationaloptimist.com/blog/what-the-pandemic-has-taught-us/ (accessed on 1 November 2021).
- Cinelli, M.; Quattrociocchi, W.; Galeazzi, A.; Valensise, C.M.; Brugnoli, E.; Schmidt, A.L.; Zola, P.; Zollo, F.; Scala, A. The COVID-19 social media infodemic. Sci. Rep. 2020, 10, 16598. [Google Scholar] [CrossRef]
- Infodemic-World Health Organization. Available online: https://www.who.int/health-topics/infodemic#tab=tab_1 (accessed on 1 November 2021).
- Sharot, T.; Sunstein, C.R. How people decide what they want to know. Nat. Hum. Behav. 2020, 4, 14–19. [Google Scholar] [CrossRef]
- Chou, W.Y.; Hunt, Y.M.; Beckjord, E.B.; Moser, R.P.; Hesse, B.W. Social media use in the United States: Implications for health communication. J. Med. Internet Res. 2009, 11, e48. [Google Scholar] [CrossRef]
- McNab, C. What social media offers to health professionals and citizens. Bull. World Health Organ. 2009, 87, 566. [Google Scholar] [CrossRef]
- Salathé, M.; Khandelwal, S. Assessing vaccination sentiments with online social media: Implications for infectious disease dynamics and control. PLoS Comput. Biol. 2011, 7, e1002199. [Google Scholar] [CrossRef] [Green Version]
- Hawn, C. Take two aspirin and tweet me in the morning: How Twitter, Facebook, and other social media are reshaping health care. Health Aff. 2009, 28, 361–368. [Google Scholar] [CrossRef]
- Centola, D. Social Media and the Science of Health Behavior. Circulation 2013, 127, 21. [Google Scholar] [CrossRef] [Green Version]
- White, M.; Dorman, S.M. Receiving social support online: Implications for health education. Health Educ. Res. 2001, 16, 693–707. [Google Scholar] [CrossRef] [Green Version]
- Thackeray, R.; Neiger, B.L.; Hanson, C.L.; McKenzie, J.F. Enhancing promotional strategies within social marketing programs: Use of Web 2.0 social media. Health Promot. Pract. 2008, 9, 338–343. [Google Scholar] [CrossRef]
- Kawachi, I.; Berkman, L.A. Neighborhoods and Health; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Krieger, N. A glossary for social epidemiology. J. Epidemiol. Community Health 2001, 55, 693–700. [Google Scholar] [CrossRef] [Green Version]
- Correll, S.J.; Ridgeway, C.L. Handbook of Social Psychology; Delamater, J., Ed.; Kluwer Academic Publishers: New York, NY, USA, 2003; pp. 29–51. [Google Scholar]
- Hyland-Wood, B.; Gardner, J.; Leask, J.; Ecker, U.K.H. Toward effective government communication strategies in the era of COVID-19. Hum. Soc. Sci. Commun. 2021, 8, 30. [Google Scholar] [CrossRef]
- Enria, L.; Waterlow, N.; Rogers, N.T.; Brindle, H.; Lal, S.; Eggo, R.M.; Lees, S.; Roberts, C.H. Trust and transparency in times of crisis: Results from an online survey during the first wave (April 2020) of the COVID-19 epidemic in the U.K. PLoS ONE 2021, 16, e0239247. [Google Scholar] [CrossRef]
- Kapoor, K.K.; Tamilmani, K.; Rana, N.P.; Patil, P.P.; Dwivedi, Y.K.; Nerur, S. Advances in Social Media Research: Past, Present and Future. Inf. Syst. Front. 2018, 20, 531–558. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, H. The Interactive Effect of Positive Psychological Capital and Organizational Trust on Organizational Citizenship Behavior. SAGE Open 2019, 9, 2158244019862661. [Google Scholar] [CrossRef]
- Elnadi, H.; Odetokun, I.A.; Bolarinwa, O.; Ahmed, Z.; Okechukwu, O.; Al-Mustapha, A.I. Correction: Knowledge, attitude, and perceptions towards the 2019 Coronavirus Pandemic: A bi-national survey in Africa. PLoS ONE 2021, 16, e0247351. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the U.K. and U.S.A. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Woelfert, F.S.; Kunst, J.R. How Political and Social Trust Can Impact Social Distancing Practices During COVID-19 in Unexpected Ways. Front. Psychol. 2020, 11, 572966. [Google Scholar] [CrossRef]
- Kim, D.J.; Ferrin, D.L.; Rao, H.R. A trust-based consumer decision-making model in electronic commerce: The role of trust, perceived risk, and their antecedents. Decis. Support Syst. 2008, 44, 544–564. [Google Scholar] [CrossRef]
- Naqvi, M.H.A.; Jiang, Y.; Miao, M.; Naqvi, M.H. The effect of social influence, trust, and entertainment value on social media use: Evidence from Pakistan. Cogent Bus. Manag. 2020, 7, 1723825. [Google Scholar] [CrossRef]
- Warner-Søderholm, G.; Bertsch, A.; Sawe, E.; Lee, D.; Wolfe, T.; Meyer, J.; Fatilua, U.N. Who trusts social media? Comput. Hum. Behav. 2018, 81, 303–315. [Google Scholar] [CrossRef]
- Li, W.; Xue, L. Analyzing the Critical Factors Influencing Post-Use Trust and Its Impact on Citizens’ Continuous-Use Intention of E-Government: Evidence from Chinese Municipalities. Sustainability 2021, 13, 7698. [Google Scholar] [CrossRef]
- Dutta, B.; Peng, M.H.; Sun, S.L. Modeling the adoption of personal health record (PHR) among individual: The effect of healthcare technology self-efficacy and gender concern. Libyan J. Med. 2018, 13, 1500349. [Google Scholar] [CrossRef] [Green Version]
- Hwang, H.G.; Dutta, B.; Chang, H.C. The Differing Effect of Gender and Clinical Specialty on Physicians’ Intention to Use Electronic Medical Record. Methods Inf. Med. 2019, 58, e58–e71. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. Manag. Inf. Syst. Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Jiang, B.; Guo, R. Factors Affecting Public Adoption of COVID-19 Prevention and Treatment Information During an Infodemic: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e23097. [Google Scholar] [CrossRef]
- Gong, Z.; Han, Z.; Li, X.; Yu, C.; Reinhardt, J.D. Factors Influencing the Adoption of Online Health Consultation Services: The Role of Subjective Norm, Trust, Perceived Benefit, and Offline Habit. Front. Public Health 2019, 7, 286. [Google Scholar] [CrossRef]
- Qin, Z.; Huo, C. Research on the continuous intention of health information seeking via social media: Bade on the view of revenue-expenditure. J. Mod. Inf. 2020, 40, 66–77. [Google Scholar]
- Hong, Z.; Deng, Z.; Zhang, W. Examining factors affecting patients trust in online healthcare services in China: The moderating role of the purpose of use. Health Inform. J. 2019, 25, 1647–1660. [Google Scholar] [CrossRef]
- Cao, J.; Shang, Y.; Mok, Q.; Lai, I.K.W. The Impact of Personal Innovativeness on the Intention to Use Cloud Classroom: An Empirical Study in China. In Proceedings of the ICTE 2019, Guangzhou, China, 15–17 March 2019; Communications in Computer and Information Science. Springer: Singapore, 2019; p. 1048. [Google Scholar]
- Chen, C.; Choi, H.; Charoen, D. Drone Delivery Services: An Evaluation of Personal Innovativeness, Opinion Passing and Key Information Technology Adoption Factors. J. Inf. Syst. Appl. Res. 2019, 12, 4–16. [Google Scholar]
- Sakallaris, B.R.; Miller, W.L.; Saper, R.; Kreitzer, M.J.; Jonas, W. Meeting the Challenge of a More Person-centered Future for U.S. Healthcare. Glob. Adv. Health Med. 2016, 5, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Dutta, B.; Hwang, H.G. The adoption of electronic medical record by physicians: A PRISMA-compliant systematic review. Medicine 2020, 99, e19290. [Google Scholar] [CrossRef]
- Barbounak, S.G.; Gourounti, K.; Sarantaki, A. Advances of Sentiment Analysis Applications in Obstetrics/Gynecology and Midwifery. Mater. Sociomed-Med. 2021, 33, 225–230. [Google Scholar] [CrossRef]
- Wu, M.L. Statistical Analysis and Practice of Questionnaire-SPSS Operation and Application; Chongqing University Press: Chongqing, China, 2010; pp. 100–125. [Google Scholar]
- Busetto, L.; Wick, W.; Gumbinger, G. How to use and assess qualitative research methods. Neurol. Res. Pract. 2020, 2, 1–10. [Google Scholar] [CrossRef]
- Statista. Available online: https://www.statista.com/statistics/319808/taiwan-sex-ratio/ (accessed on 11 October 2021).
- Podsakoff, P.M.; MacKenzie, S.; Podsakoff, N.P. Sources of method bias in social science research and recommendations on how to control it. Annu. Rev. Psychol. 2012, 63, 539–569. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis; Prentice-Hall, Inc.: Hoboken, NJ, USA, 1998. [Google Scholar]
- Bagozzi, R.P.; Yi, Y. On the evaluation of structural equation models. J. Acad. Marking Sci. 1988, 16, 74–94. [Google Scholar] [CrossRef]
- Zahid, H.; Haji Din, B. Determinants of Intention to Adopt E-Government Services in Pakistan: An Imperative for Sustainable Development. Resources 2019, 8, 128. [Google Scholar] [CrossRef] [Green Version]
- Carter, L.; Weerakkody, V.; Phillips, B.; Dwivedi, Y.K. Citizen Adoption of E-Government Services: Exploring Citizen Perceptions of Online Services in the United States and United Kingdom. Inform. Syst. Manag. 2016, 33, 124–140. [Google Scholar] [CrossRef] [Green Version]
- Yi, M.Y.; Yoon, J.J.; Davis, J.M.; Lee, T. Untangling the antecedents of initial trust in web-based health information: The roles of argument quality, source expertise, and user perceptions of information quality and risk. Decis. Support Syst. 2013, 55, 284–295. [Google Scholar] [CrossRef]
- Rana, N.P.; Dwivedi, Y.K.; Lal, B.; Williams, M.D.; Clement, M. Citizens’ adoption of an electronic government system: Towards a unified view. Inf. Syst. Front. 2015, 19, 549–568. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kwon, S.A.; Lee, J.E.; Ahn, B.C.; Lee, J.H.; An, C.; Kitagawa, K.; Kim, D.; Wang, J. Analyzing the Role of Resource Factors in Citizens’ Intention to Pay for and Participate in Disaster Management. Sustainability 2020, 12, 3377. [Google Scholar] [CrossRef] [Green Version]
- Barua, Z.; Barua, S.; Aktar, S.; Kabir, N.; Li, M. Effects of misinformation on COVID-19 individual responses and recommendations for resilience of disastrous consequences of mis-information. Prog. Disaster Sci. 2020, 8, 100119. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ATT | TRGT | TRSM | PBT | PIIT | PRT | HID | INT | |
|---|---|---|---|---|---|---|---|---|
| ATT | 1 | |||||||
| TRGT | 0.265 ** | 1 | ||||||
| TRSM | 0.412 ** | −0.235 ** | 1 | |||||
| PBT | 0.312 ** | −0.318 ** | 0.430 ** | 1 | ||||
| PIIT | 0.321 ** | −0.187 ** | 0.260 ** | 0.432 ** | 1 | |||
| PRT | 0.124 ** | 0.486 ** | −0.176 ** | −0.217 ** | −0.249 ** | 1 | ||
| HID | −0.187 ** | −0.156 ** | −0.425 ** | −0.459 ** | −0.458 ** | −0.217 ** | 1 | |
| INT | 0.246 ** | 0.272 ** | 0.321 ** | 0.421 ** | 0.287 ** | 0.318 ** | 0.417 ** | 1 |
| Mean | 3.712 | 3.215 | 3.427 | 3.518 | 3.316 | 3.628 | 3.845 | 3.582 |
| S.D. | 0.928 | 0.956 | 0.967 | 1.000 | 0.868 | 0.891 | 0.948 | 0.986 |
| Construct. | Code | Cronbach’s α | Factor Loadings | CR | AVE |
|---|---|---|---|---|---|
| Attitude | ATT1 | 0.841 | 0.865 | 0.812 | 0.816 |
| ATT2 | 0.923 | ||||
| ATT3 | 0.905 | ||||
| Trust on the Government | TRGT1 | 0.926 | 0.881 | 0.891 | 0.646 |
| TRGT2 | 0.941 | ||||
| TRGT3 | 0.913 | ||||
| Trust in Social media | TRSM1 | 0.852 | 0.856 | 0.686 | 0.756 |
| TRSM2 | 0.841 | ||||
| TRSM3 | 0.876 | ||||
| Perceived benefit | PBT1 | 0.868 | 0.912 | 0.781 | 0.742 |
| PBT2 | 0.889 | ||||
| PBT3 | 0.891 | ||||
| Personal innovativeness | PIIT1 | 0.872 | 0.912 | 0.824 | 0.708 |
| PIIT2 | 0.872 | ||||
| PIIT3 | 0.946 | ||||
| Peer referent | PRT1 | 0.787 | 0.932 | 0.746 | 0.684 |
| PRT2 | 0.856 | ||||
| PRT3 | 0.862 | ||||
| Health infodemic | HID1 | 0.792 | 0.878 | 0.821 | 0.748 |
| HID2 | 0.892 | ||||
| HID3 | 0.849 | ||||
| HID4 | 0.870 | ||||
| HID5 | 0.858 | ||||
| Readiness toward COVID-19 preventive measures | INT1 | 0.897 | 0.907 | 0.868 | 0.657 |
| INT2 | 0.895 | ||||
| INT3 | 0.916 | ||||
| INT4 | 0.894 |
| Path Coefficient | C.R. | p-Value | Result | ||
|---|---|---|---|---|---|
| H1 | TRGT→INT | −0.026 | −0.516 | 0.716 | Rejected |
| H2 | TRSM→INT | 0.252 ** | 3.156 | 0.001 | Supported |
| H3 | TRGT→ATT | 0.217 ** | 3.126 | 0.014 | Supported |
| H4 | TRSM→ATT | 0.116 ** | 2.635 | 0.007 | Supported |
| H5 | TRGT→PBT | 0.256 *** | 4.846 | 0.000 | Supported |
| H6 | TRSM→PBT | 0.340 *** | 6.642 | 0.000 | Supported |
| H7 | ATT→INT | 0.120 ** | 3.178 | 0.001 | Supported |
| H8 | PBT→INT | 0.264 *** | 5.662 | 0.000 | Supported |
| H9 | PIIT→INT | 0.418 *** | 8.217 | 0.000 | Supported |
| H10 | PRT→INT | 0.284 *** | 5.517 | 0.000 | Supported |
| Construct | R2 |
|---|---|
| ATT | 0.317 |
| PBT | 0.486 |
| INT | 0.547 |
| TRGT | TRSM | ATT | PBT | PIIT | PRT | |
|---|---|---|---|---|---|---|
| ATT | 0.116 | 0.256 | ||||
| PBT | 0.120 | 0.264 | ||||
| INT | −0.026 | 0.252 | 0.217 | 0.340 | 0.418 | 0.284 |
| TRGT | TRSM | ATT | PBT | PIIT | PRT | |
|---|---|---|---|---|---|---|
| ATT | ||||||
| PBT | ||||||
| INT | 0.089 | 0.116 |
| TRGT | TRSM | ATT | PBT | PIIT | PRT | |
|---|---|---|---|---|---|---|
| ATT | 0.116 | 0.256 | ||||
| PBT | 0.120 | 0.264 | ||||
| INT | 0.063 | 0.372 | 0.217 | 0.340 | 0.418 | 0.284 |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 | Model 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Gender | 0.099 * (0.05) | 0.101 * (0.046) | 0.097 * (0.046) | 0.113 * (0.047) | 0.107 * (0.047) | 0.113 * (0.049) | 0.095 * (0.049) | 0.097 * (0.048) | 0.115 * (0.048) |
| Age | −0.041 * (0.026) | −0.063 * (0.025) | −0.062 * (0.024) | −0.045 * (0.024) | −0.045 (0.024) | −0.061 * (0.023) | −0.064 * (0.026) | −0.043 * (0.026) | −0.043 (0.026) |
| Education | 0.031 (0.028) | 0.031 * (0.027) | 0.034 (0.027) | 0.038 * (0.027) | 0.040 * (0.027) | 0.042 * (0.029) | 0.044 (0.029) | 0.047 * (0.029) | 0.050 * (0.029) |
| Experience of using Social media | 0.216 *** (0.037) | 0.224 *** (0.035) | 0.221 *** (0.035) | 0.218 *** (0.035) | 0.219 *** (0.035) | 0.217 *** (0.035) | 0.226 *** (0.035) | 0.223 *** (0.035) | 0.220 *** (0.035) |
| HID | −0.096 *** (0.028) | −0.092 *** (0.028) | −0.063 * (0.029) | −0.065 * (0.029) | −0.094 *** (0.030) | −0.090 *** (0.030) | −0.061 * (0.031) | −0.063 * (0.031) | |
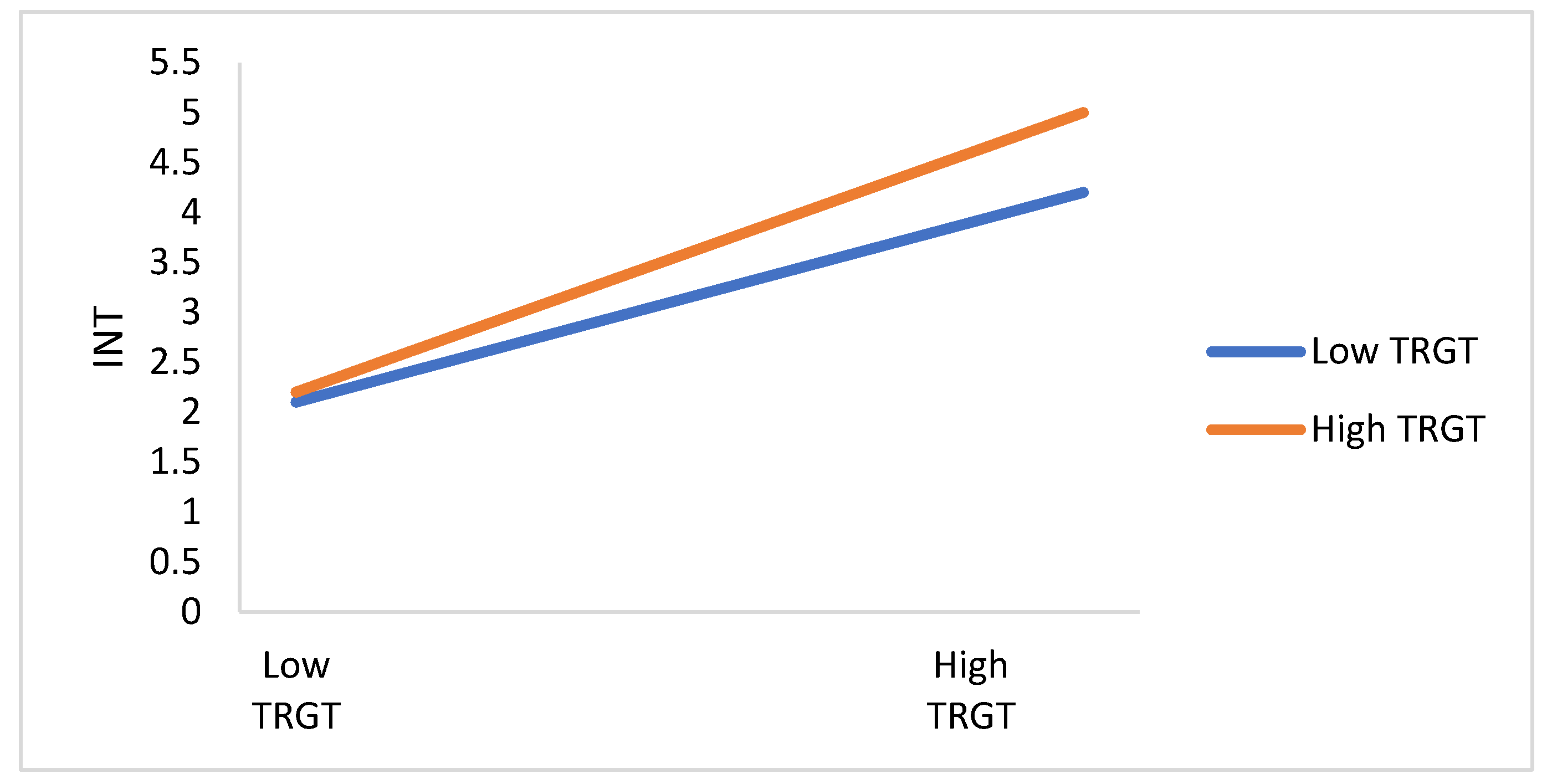
| TRGT | 0.242 *** (0.029) | 0.25796 *** (0.030) | |||||||
| HID × TRGT | −0.062 * (0.024) | ||||||||
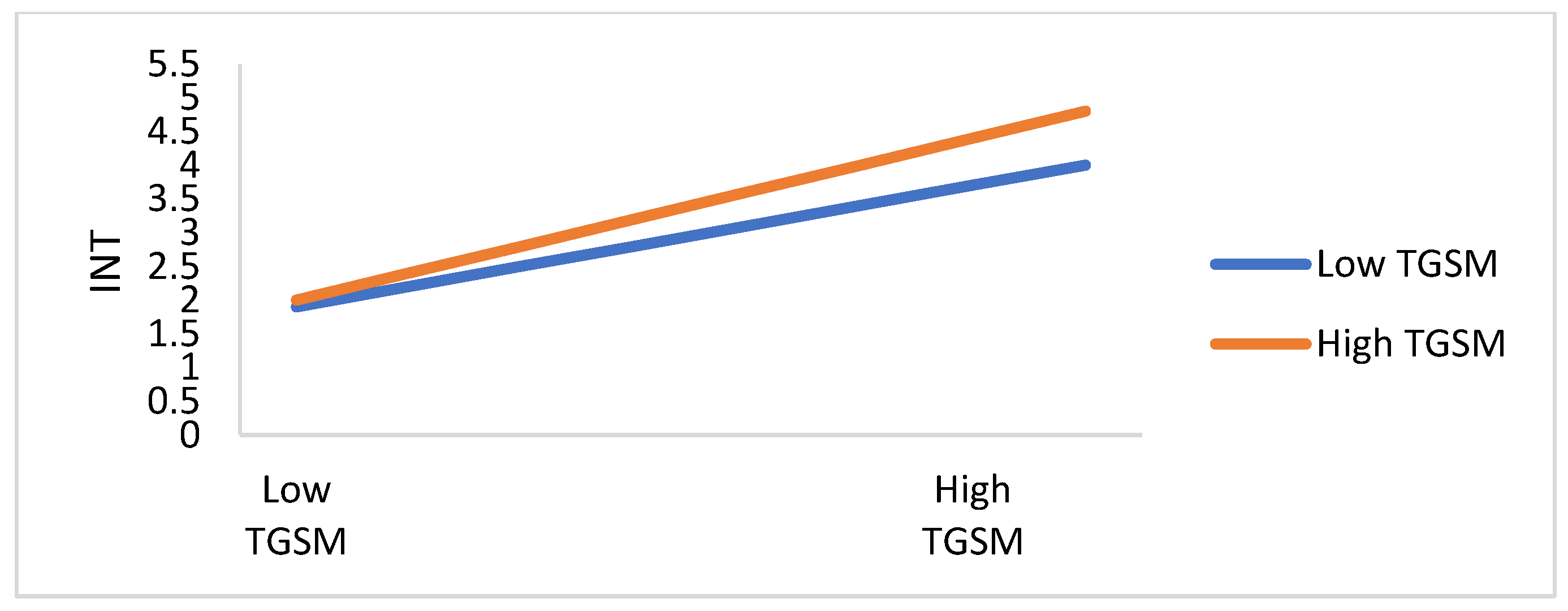
| TRSM | 0.269 *** (0.032) | 0.269 *** (0.032) | |||||||
| HID × TRSM | 0.041 * (0.022) | ||||||||
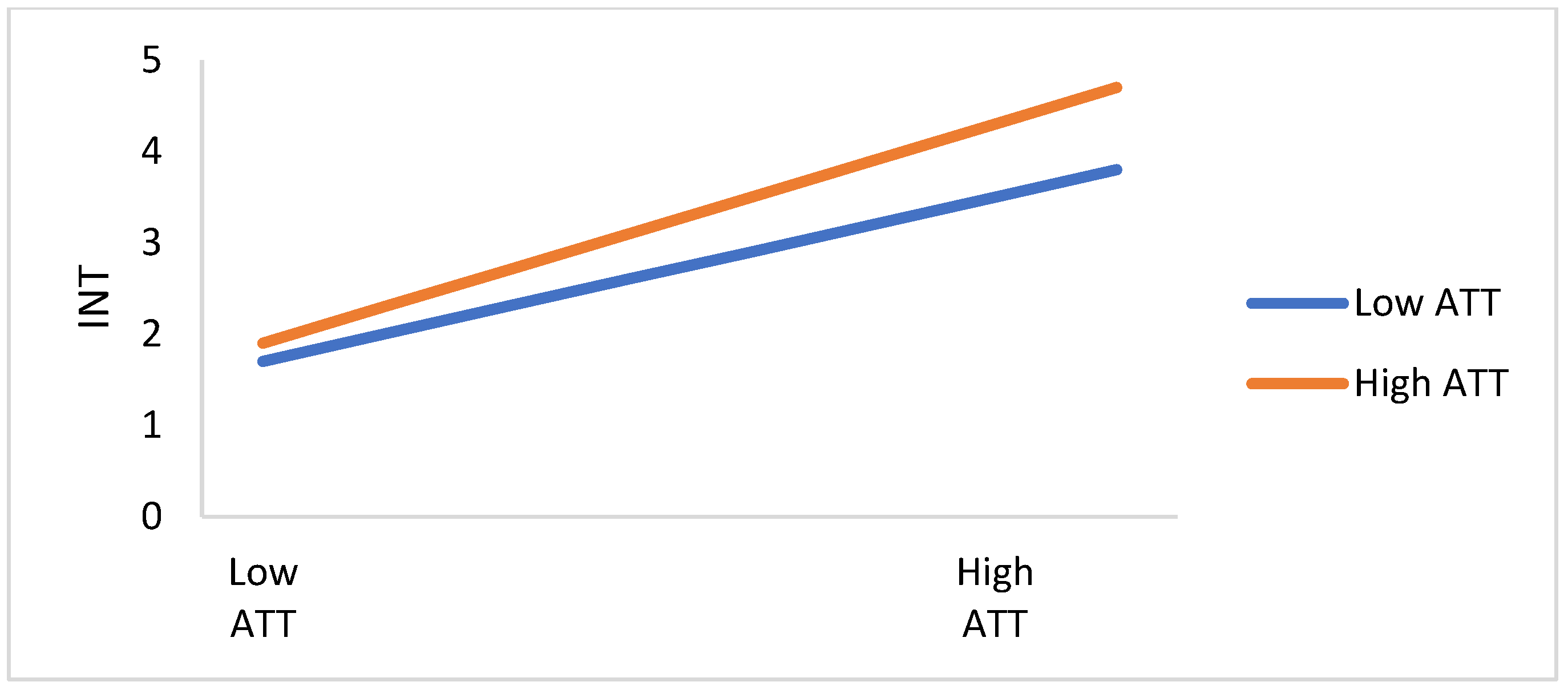
| ATT | 0.277 *** (0.034) | 0.277 *** (0.034) | |||||||
| HID × ATT | −0.039 * (0.021) | ||||||||
| PBT | 0.289 *** (0.036) | 0.289 *** (0.036) | |||||||
| HID × PBT | −0.039 * (0.019) | ||||||||
| R2 | 0.068 | 0.162 | 0.168 | 0.172 | 0.175 | 0.182 | 0.188 | 0.192 | 0.195 |
| Adjusted R2 | 0.064 | 0.157 | 0.162 | 0.166 | 0.170 | 0.177 | 0.182 | 0.187 | 0.190 |
| ∆R2 | 0.068 *** | 0.115 *** | 0.03 * | 0.124 *** | 0.005 * | 0.119 *** | 0.005 * | 0.128 *** | 0.03 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dutta, B.; Peng, M.-H.; Chen, C.-C.; Sun, S.-L. Role of Infodemics on Social Media in the Development of People’s Readiness to Follow COVID-19 Preventive Measures. Int. J. Environ. Res. Public Health 2022, 19, 1347. https://doi.org/10.3390/ijerph19031347
Dutta B, Peng M-H, Chen C-C, Sun S-L. Role of Infodemics on Social Media in the Development of People’s Readiness to Follow COVID-19 Preventive Measures. International Journal of Environmental Research and Public Health. 2022; 19(3):1347. https://doi.org/10.3390/ijerph19031347
Chicago/Turabian StyleDutta, Bireswar, Mei-Hui Peng, Chien-Chih Chen, and Shu-Lung Sun. 2022. "Role of Infodemics on Social Media in the Development of People’s Readiness to Follow COVID-19 Preventive Measures" International Journal of Environmental Research and Public Health 19, no. 3: 1347. https://doi.org/10.3390/ijerph19031347
APA StyleDutta, B., Peng, M.-H., Chen, C.-C., & Sun, S.-L. (2022). Role of Infodemics on Social Media in the Development of People’s Readiness to Follow COVID-19 Preventive Measures. International Journal of Environmental Research and Public Health, 19(3), 1347. https://doi.org/10.3390/ijerph19031347