
The Social Acceptance of Smart Health Services in Japan

 ,
,
Abstract
:1. Introduction
1.1. Background and Purpose
1.2. Literature Review
1.3. Overview
2. Materials and Methods
2.1. Participants
2.2. Vignette
2.3. Items
2.4. Procedure and Analysis
3. Results
3.1. Data Screening
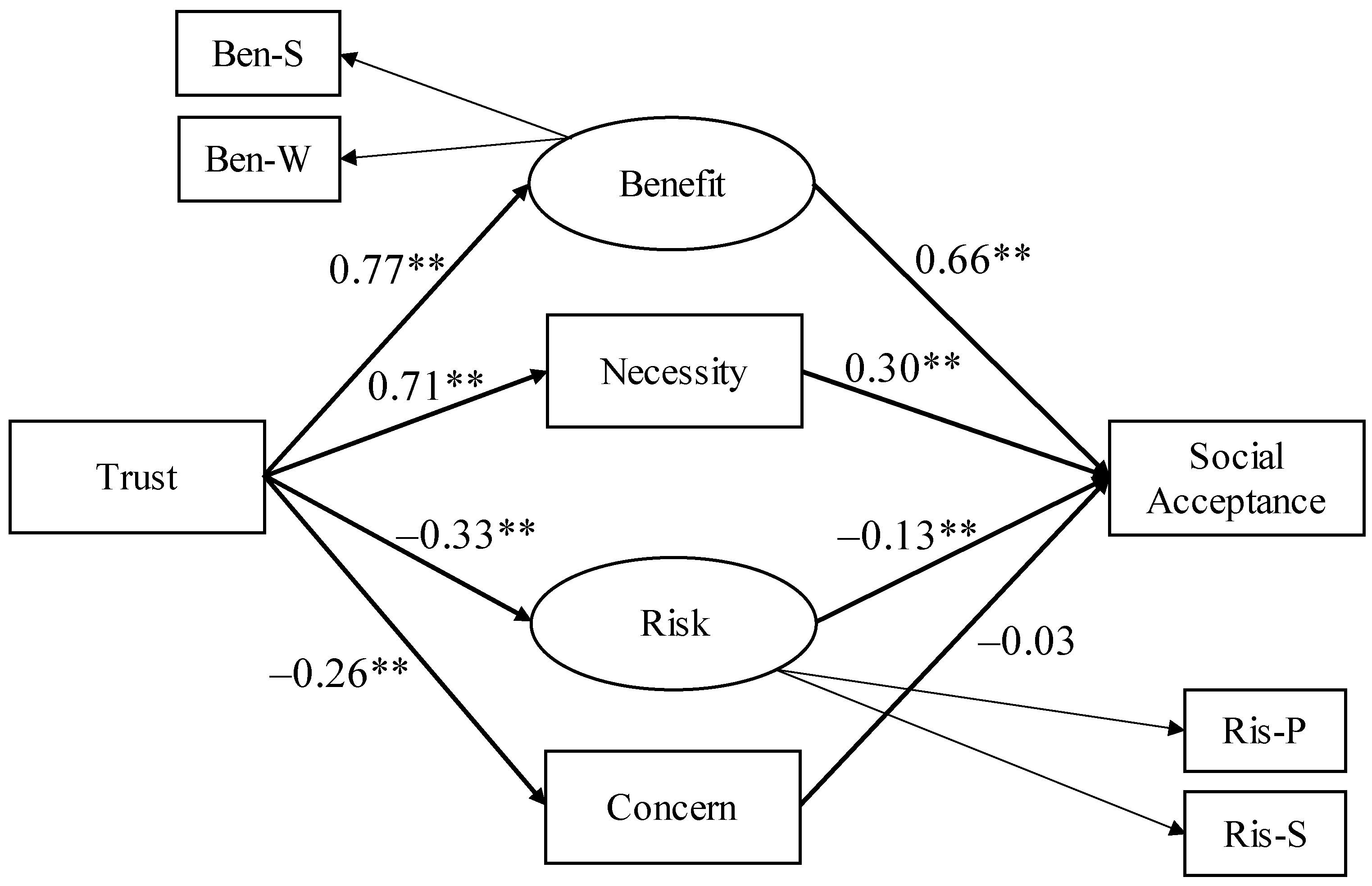
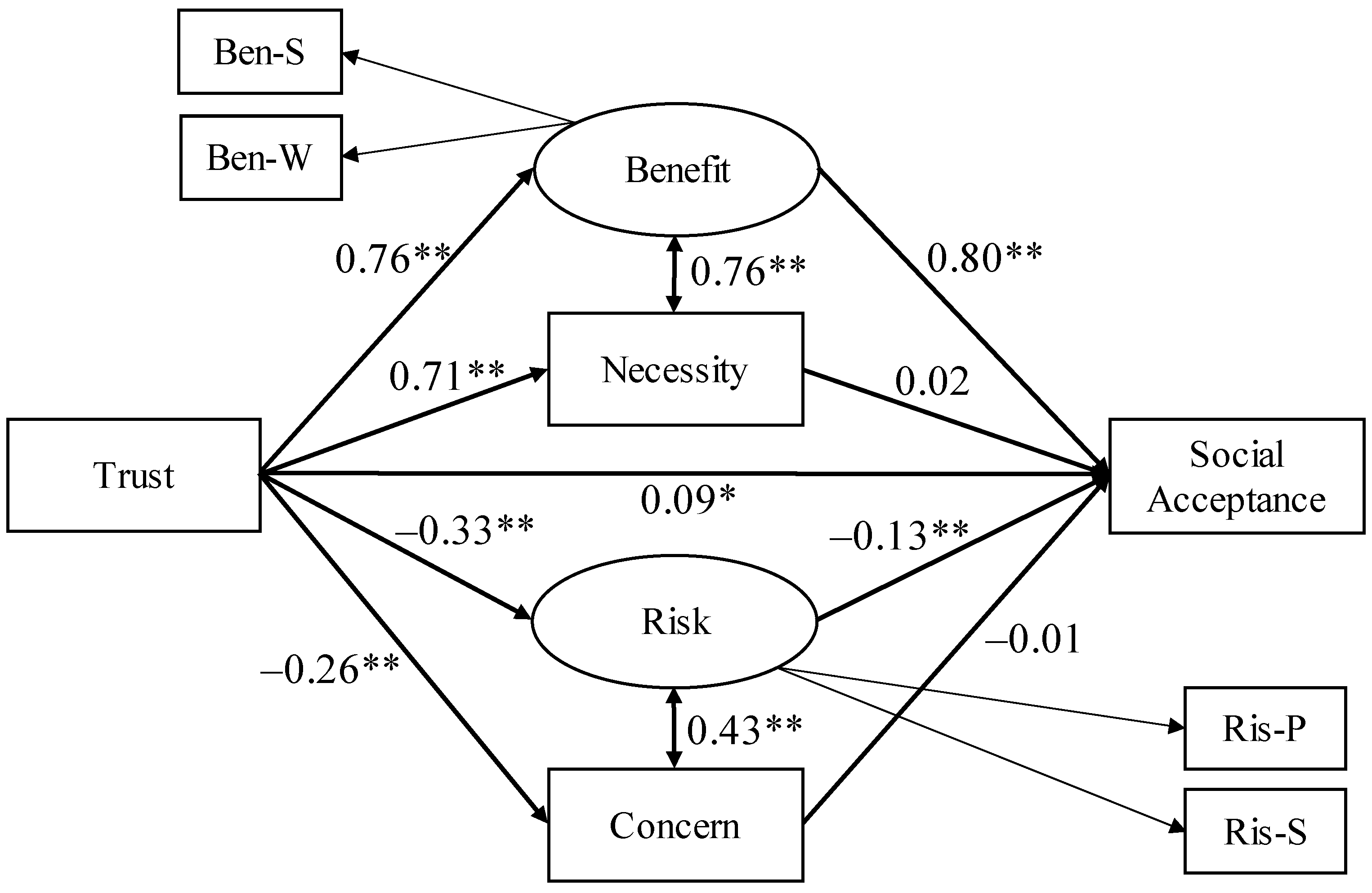
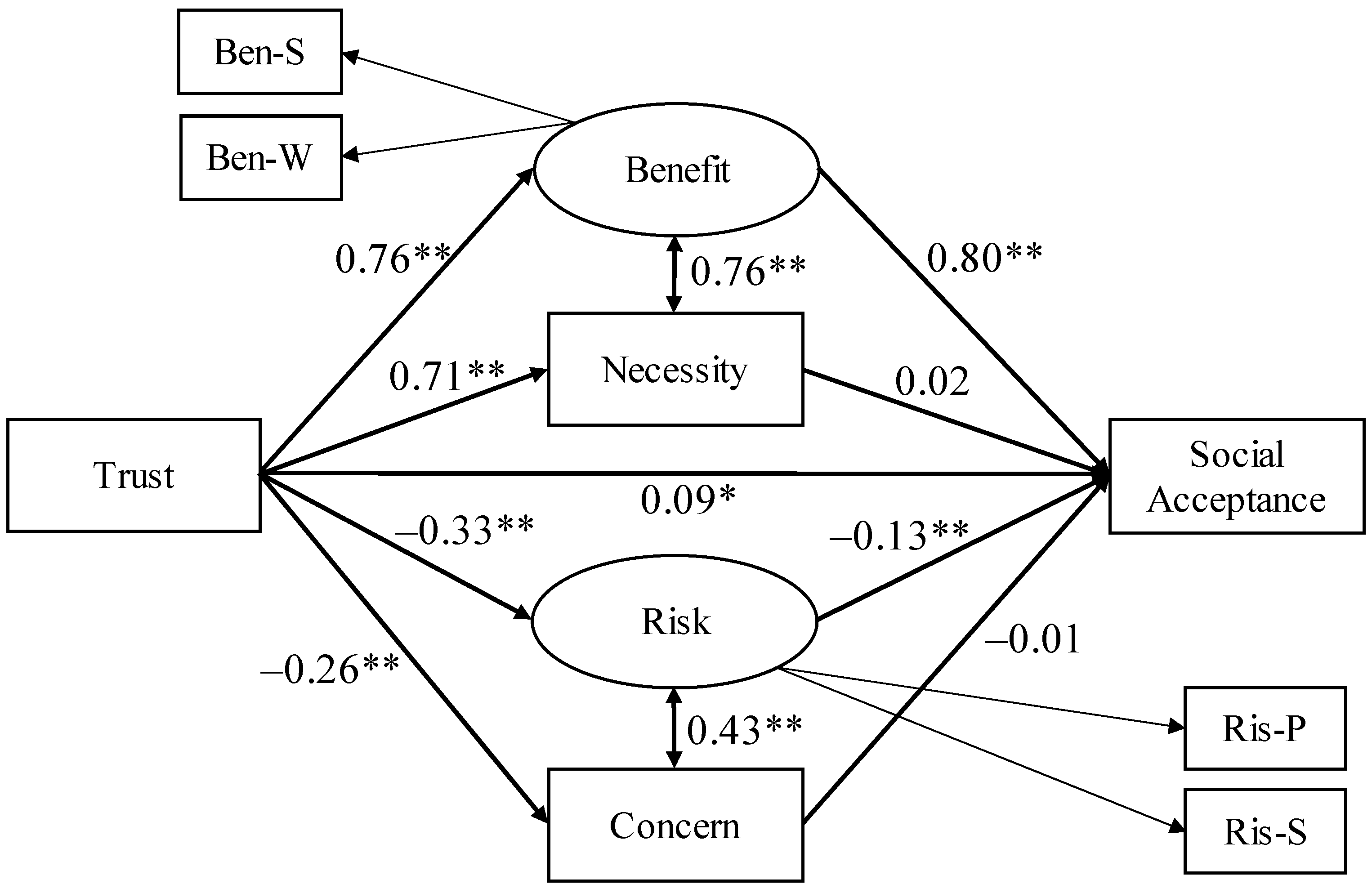
3.2. Structural Equation Modeling
4. Discussion
4.1. Various Factors Related to the Social Acceptance of s-Health Services
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Vignette
References
- Granier, B.; Kudo, H. How are citizens involved in smart cities? Analysing citizen participation in Japanese “Smart Communities”. Sci. Inf. Policy 2016, 21, 61–76. [Google Scholar] [CrossRef]
- Khansari, N.; Mostashari, A.; Mansouri, M. Impacting sustainable behavior and planning in smart city. Int. J. Sustain. Land Use Urban Plan. 2013, 1, 46–61. [Google Scholar] [CrossRef]
- Neirotti, P.; De Marco, A.; Cagliano, A.C.; Mangano, G.; Scorrano, F. Current trends in Smart City initiatives: Some stylised facts. Cities 2014, 38, 25–36. [Google Scholar] [CrossRef] [Green Version]
- Japan Cabinet Office. Society 5.0. 2021. Available online: https://www8.cao.go.jp/cstp/society5_0/index.html (accessed on 30 November 2021).
- Al-Azzam, M.; Alazzam, M.B. Smart city and smart-health framework, challenges and opportunities. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Trencher, G.; Karvonen, A. Stretching “smart”: Advancing health and well-being through the smart city agenda. Local Environ. 2019, 24, 610–627. [Google Scholar] [CrossRef]
- Lohachab, A. Bootstrapping urban planning: Addressing big data issues in smart cities. In Research Anthology on Big Data Analytics, Architectures, and Applications; IGI Global: Hershey, PA, USA, 2022; pp. 1329–1358. [Google Scholar] [CrossRef]
- Sicari, S.; Rizzardi, A.; Grieco, L.A.; Piro, G.; Coen-Porisini, A. A policy enforcement framework for Internet of Things applications in the smart health. Smart Health 2017, 3, 39–74. [Google Scholar] [CrossRef]
- Solanas, A.; Patsakis, C.; Conti, M.; Vlachos, I.S.; Ramos, V.; Falcone, F.; Postolache, O.; Perez-Martinez, P.A.; Pietro, R.D.; Perrea, D.N.; et al. Smart health: A context-aware health paradigm within smart cities. IEEE Commun. Mag. 2014, 52, 74–81. [Google Scholar] [CrossRef]
- Abdellatif, A.A.; Mohamed, A.; Chiasserini, C.F.; Tlili, M.; Erbad, A. Edge computing for smart health: Context-aware approaches, opportunities, and challenges. IEEE Netw. 2019, 33, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Ahad, A.; Tahir, M.; Aman Sheikh, M.; Ahmed, K.I.; Mughees, A.; Numani, A. Technologies trend towards 5G network for smart health-care using IoT: A review. Sensors 2020, 20, 4047. [Google Scholar] [CrossRef]
- Kashiwanoha Smart City. Kashiwanoha Smart City: Action Plan. 2020. Available online: https://www.kashiwanoha-smartcity.com/images/pdf/kashiwanoha-smartcity-action-plan.pdf (accessed on 30 November 2021).
- Japan Ministry of Internal Affairs and Communications. Supplementary Budget for IoT Service Creation: Result Report in 2015. 2017. Available online: https://www.soumu.go.jp/midika-iot/admin/wp-content/uploads/2016/07/H27-4_Report.pdf (accessed on 30 November 2021).
- Soma, K.; Haggett, C. Enhancing social acceptance in marine governance in Europe. Ocean Coast. Manag. 2015, 117, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Sonnberger, M.; Ruddat, M. Local and socio-political acceptance of wind farms in Germany. Technol. Soc. 2017, 51, 56–65. [Google Scholar] [CrossRef]
- Tenney, M.; Garnett, R.; Wylie, B. A theatre of machines: Automata circuses and digital bread in the smart city of Toronto. Can. Geogr. 2020, 64, 388–401. [Google Scholar] [CrossRef]
- Keymolen, E.; Voorwinden, A. Can we negotiate? Trust and the rule of law in the smart city paradigm. Int. Rev. Law Comput. Technol. 2020, 34, 233–253. [Google Scholar] [CrossRef] [Green Version]
- Hamamatsu City. Results of public comment on the Hamamatsu City Digital Smart City Concept (Draft). 2021. Available online: https://www.city.hamamatsu.shizuoka.jp/dsc/dejisuma_kousou/kangaekata/top.html (accessed on 30 November 2021).
- Ding, D.; Conti, M.; Solanas, A. A smart health application and its related privacy issues. In Proceedings of the 2016 Smart City Security and Privacy Workshop (SCSP-W), Vienna, Austria, 11 April 2016; pp. 1–5. [Google Scholar] [CrossRef]
- Liu, H.; Yao, X.; Yang, T.; Ning, H. Cooperative privacy preservation for wearable devices in hybrid computing-based smart health. IEEE Internet Things J. 2018, 6, 1352–1362. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, D.; Deng, R.H. Security and privacy in smart health: Efficient policy-hiding attribute-based access control. IEEE Internet Things J. 2018, 5, 2130–2145. [Google Scholar] [CrossRef]
- Gerber, N.; Reinheimer, B.; Volkamer, M. Investigating people’s privacy risk perception. Proc. Priv. Enhancing Technol. 2019, 3, 267–288. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, S.; Zhang, W.; Evans, R. Why people adopt smart transportation services: An integrated model of TAM, trust and perceived risk. Transp. Plan. Technol. 2021, 44, 629–646. [Google Scholar] [CrossRef]
- Wiegard, R.B.; Breitner, M.H. Smart services in healthcare: A risk-benefit-analysis of pay-as-you-live services from customer perspective in Germany. Electron. Mark. 2019, 29, 107–123. [Google Scholar] [CrossRef]
- Shimizu, Y.; Osaki, S.; Hashimoto, T.; Karasawa, K. The social acceptance of collecting and utilizing personal information in smart cities. Sustainability 2021, 13, 9146. [Google Scholar] [CrossRef]
- Choi, J.K.; Ji, Y.G. Investigating the importance of trust on adopting an autonomous vehicle. Int. J. Hum.-Comput. Interact. 2015, 31, 692–702. [Google Scholar] [CrossRef]
- Hashimoto, T.; Tham, Y.J.; Karasawa, K.; Tai, M. Understanding people’s attitudes toward a “data-driven” society based on trust and technology acceptance models. In Proceedings of the 84th Annual Convention Japanese Psychological Association, Tokyo, Japan, 8 September 2020. PQ-003. [Google Scholar]
- Neupane, C.; Wibowo, S.; Grandhi, S.; Deng, H. A trust-based model for the adoption of smart city technologies in Australian regional cities. Sustainability 2021, 13, 9316. [Google Scholar] [CrossRef]
- Hitachi and U-Tokyo Joint Research. Society 5.0: A Human-Centered, Super-Smart Society; Nikkei Business Publications: Tokyo, Japan, 2018. [Google Scholar]
- Shimizu, Y.; Osaki, S.; Hashimoto, T.; Karasawa, K. How do people view various kinds of smart city services? Focus on the acquisition of personal information. Sustainability 2021, 13, 11062. [Google Scholar] [CrossRef]
- Oh, S.R.; Seo, Y.D.; Lee, E.; Kim, Y.G. A comprehensive survey on security and privacy for electronic health data. Int. J. Environ. Res. Public Health 2021, 18, 9668. [Google Scholar] [CrossRef]
- Xiang, D.; Cai, W. Privacy protection and secondary use of health data: Strategies and methods. BioMed Res. Int. 2021, 2021, 6967166. [Google Scholar] [CrossRef]
- Mani, Z.; Chouk, I. Impact of privacy concerns on resistance to smart services: Does the ‘Big Brother effect’ matter? J. Mark. Manag. 2019, 35, 1460–1479. [Google Scholar] [CrossRef]
- Panchatcharam, P.; Vivekanandan, S. Internet of things (IOT) in healthcare: Smart health and surveillance, architectures, security analysis and data transfer: A review. Int. J. Softw. Innov. 2019, 7, 21–40. [Google Scholar] [CrossRef]
- Beck, K.H. The effects of risk probability, outcome severity, efficacy of protection and access to protection on decision making: A further test of protection motivation theory. Soc. Behav. Pers. 1984, 12, 121–125. [Google Scholar] [CrossRef]
- CrowdWorks. One of the Largest Crowdsourcing Services. 2021. Available online: https://crowdworks.jp/ (accessed on 17 January 2022).
- Krasnova, H.; Veltri, N.F. Privacy calculus on social networking sites: Explorative evidence from Germany and USA. In Proceedings of the 2010 43rd Hawaii International Conference on System Sciences, Honolulu, HI, USA, 5–8 January 2010; pp. 1–10. [Google Scholar] [CrossRef]
- Togari, T.; Yamazaki, Y.; Koide, S.; Miyata, A. Reliability and validity of the modified Perceived Health Competence Scale (PHCS) Japanese version. Jpn. J. Public Health 2006, 53, 51–57. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Chen, S.; Duckworth, K.; Chaiken, S. Motivated heuristic and systematic processing. Psychol. Inq. 1999, 10, 44–49. [Google Scholar] [CrossRef]
- Katz, S.J.; Erkkinen, M.; Lindgren, B.; Hatsukami, D. Assessing the impact of conflicting health warning information on intentions to use e-cigarettes: An application of the Heuristic-Systematic model. J. Health Commun. 2018, 23, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Camarero, C.; José, R.S. Does involvement matter in online shopping satisfaction and trust? Psychol. Mark. 2011, 28, 145–167. [Google Scholar] [CrossRef]
- Yang, S.C.; Hung, W.C.; Sung, K.; Farn, C.K. Investigating initial trust toward e-tailers from the elaboration likelihood model perspective. Psychol. Mark. 2006, 23, 429–445. [Google Scholar] [CrossRef]
- Yen, Y.S. Route factors influencing trust and attitude toward TV shopping. Serv. Ind. J. 2018, 38, 402–430. [Google Scholar] [CrossRef]
- Firestone, J.; Hirt, C.; Bidwell, D.; Gardner, M.; Dwyer, J. Faring well in offshore wind power siting? Trust, engagement and process fairness in the United States. Energy Res. Soc. Sci. 2020, 62, 101393. [Google Scholar] [CrossRef]
- Liebe, U.; Bartczak, A.; Meyerhoff, J. A turbine is not only a turbine: The role of social context and fairness characteristics for the local acceptance of wind power. Energy Policy 2017, 107, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Tabi, A.; Wüstenhagen, R. Keep it local and fish-friendly: Social acceptance of hydropower projects in Switzerland. Renew. Sustain. Energy Rev. 2017, 68, 763–773. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.; Matsuoka, S. The relationship between trust, procedural justice, and distributive justice in high-level radioactive waste (HLW) management. J. Environ. Inf. Sci. 2020, 2020, 33–44. [Google Scholar] [CrossRef]
- Goedkoop, F.; Devine-Wright, P. Partnership or placation? The role of trust and justice in the shared ownership of renewable energy projects. Energy Res. Soc. Sci. 2016, 17, 135–146. [Google Scholar] [CrossRef]
- Huijts, N.M.; Molin, E.J.; Steg, L. Psychological factors influencing sustainable energy technology acceptance: A review-based comprehensive framework. Renew. Sustain. Energy Rev. 2012, 16, 525–531. [Google Scholar] [CrossRef]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Ghazizadeh, M.; Lee, J.D.; Boyle, L.N. Extending the technology acceptance model to assess automation. Cogn. Technol. Work. 2012, 14, 39–49. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Chadborn, N.H.; Blair, K.; Creswick, H.; Hughes, N.; Dowthwaite, L.; Adenekan, O.; Pérez Vallejos, E. Citizens’ juries: When older adults deliberate on the benefits and risks of smart health and smart homes. Healthcare 2019, 7, 54. [Google Scholar] [CrossRef] [Green Version]
- Ebihara, J.; Nakamura, S. Smart City 5.0: Urban Operating Systems to Accelerate Regional Development; Impress Books: Tokyo, Japan, 2019. [Google Scholar]
- Jovanović, M.; De Angeli, A.; McNeill, A.; Coventry, L. User requirements for inclusive technology for older adults. Int. J. Hum.-Comput. Interact. 2021, 37, 1947–1965. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Soc-A | 4.02 | 0.96 | ― | ||||||
| 2 | Tru | 3.71 | 0.92 | 0.75 | ― | |||||
| 3 | Ben-S | 4.13 | 0.96 | 0.84 | 0.67 | ― | ||||
| 4 | Ben-W | 4.17 | 0.86 | 0.75 | 0.64 | 0.73 | ― | |||
| 5 | Nec | 3.81 | 0.96 | 0.83 | 0.71 | 0.80 | 0.72 | ― | ||
| 6 | Ris-P | 4.11 | 1.11 | −0.33 | −0.26 | −0.24 | −0.20 | −0.27 | ― | |
| 7 | Ris-S | 4.57 | 1.20 | −0.26 | −0.20 | −0.15 | −0.15 | −0.19 | 0.51 | ― |
| 8 | Con | 3.42 | 1.14 | −0.31 | −0.26 | −0.25 | −0.23 | −0.26 | 0.35 | 0.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, Y.; Ishizuna, A.; Osaki, S.; Hashimoto, T.; Tai, M.; Tanibe, T.; Karasawa, K. The Social Acceptance of Smart Health Services in Japan. Int. J. Environ. Res. Public Health 2022, 19, 1298. https://doi.org/10.3390/ijerph19031298
Shimizu Y, Ishizuna A, Osaki S, Hashimoto T, Tai M, Tanibe T, Karasawa K. The Social Acceptance of Smart Health Services in Japan. International Journal of Environmental Research and Public Health. 2022; 19(3):1298. https://doi.org/10.3390/ijerph19031298
Chicago/Turabian StyleShimizu, Yuho, Aimi Ishizuna, Shin Osaki, Takaaki Hashimoto, Mitsuharu Tai, Tetsushi Tanibe, and Kaori Karasawa. 2022. "The Social Acceptance of Smart Health Services in Japan" International Journal of Environmental Research and Public Health 19, no. 3: 1298. https://doi.org/10.3390/ijerph19031298
APA StyleShimizu, Y., Ishizuna, A., Osaki, S., Hashimoto, T., Tai, M., Tanibe, T., & Karasawa, K. (2022). The Social Acceptance of Smart Health Services in Japan. International Journal of Environmental Research and Public Health, 19(3), 1298. https://doi.org/10.3390/ijerph19031298