
Effects of Exercise Programs on Physical Factors and Safety in Adult Patients with Cancer and Haematopoietic Stem Cell Transplantation: A Systematic Review

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection of the Studies
2.3. Data Extraction
2.4. Risk of Bias Assessment
3. Results
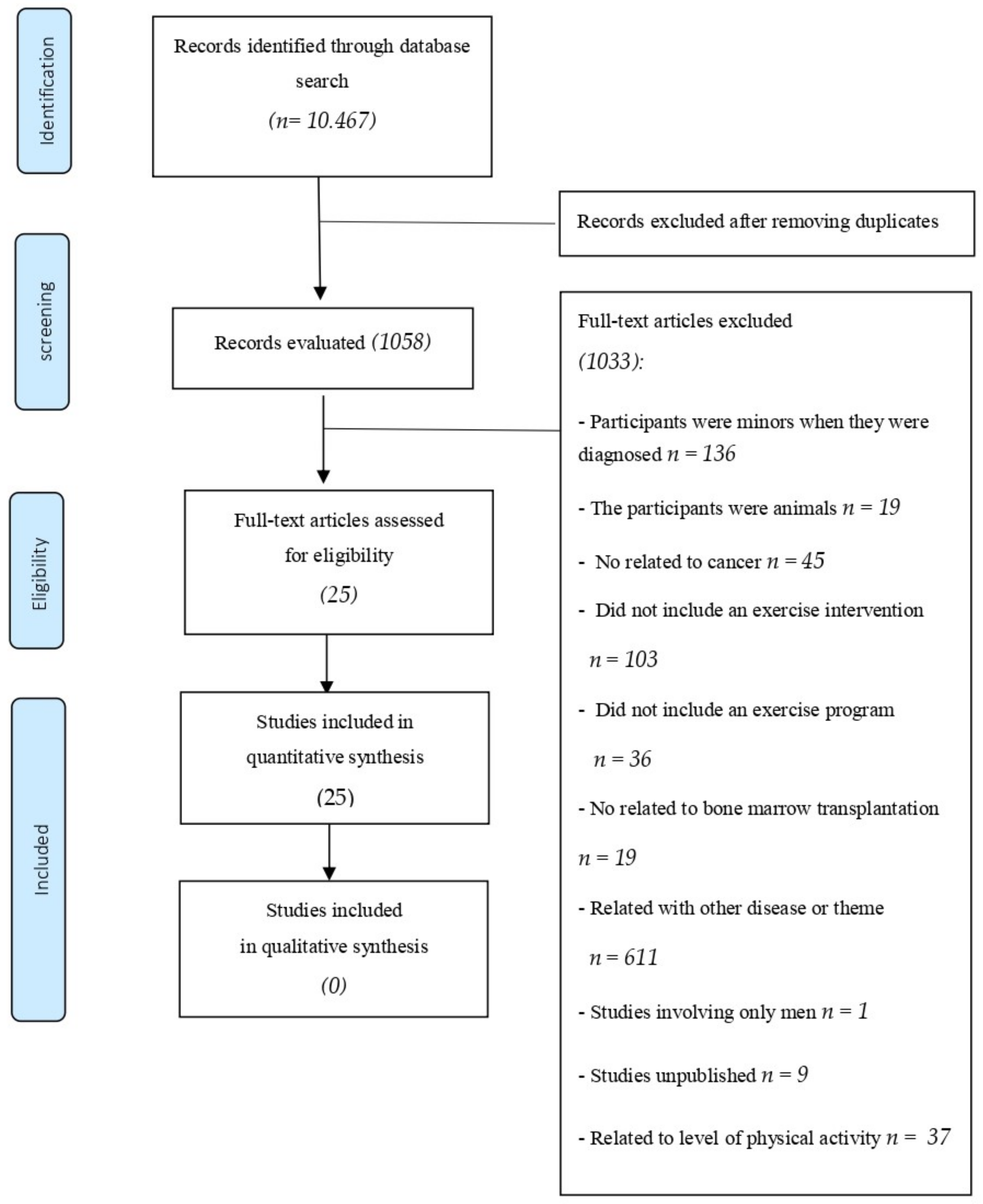
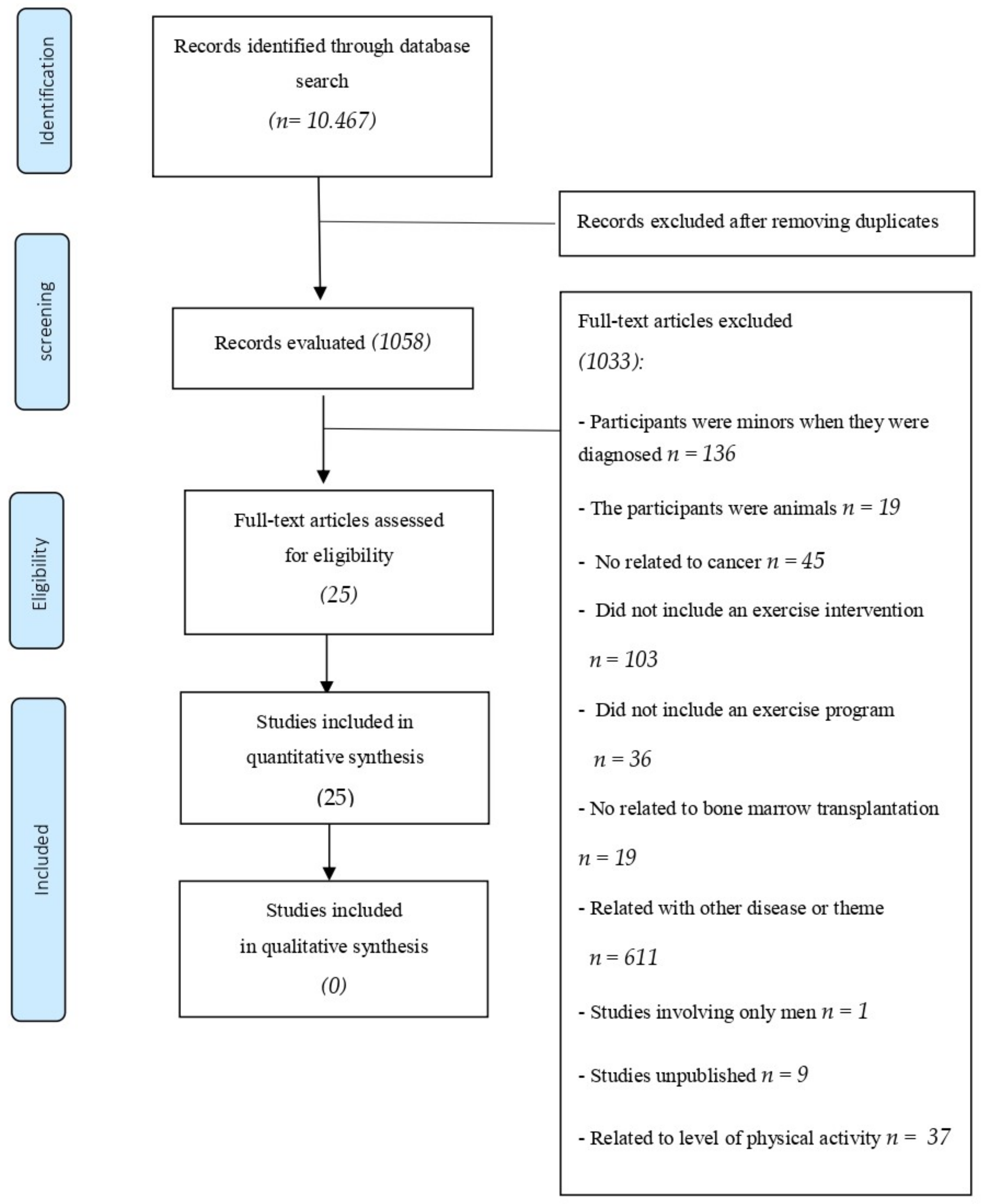
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment and Publication Bias
3.4. Characteristics of Participants
3.5. Characteristics of Exercise Interventions
3.6. Exercise Safety—Related Adverse Events
3.7. Compliance Rate
3.8. Endpoints and Exercise Intervention Results
3.8.1. Cardiorespiratory Fitness (CRF)
3.8.2. Muscle Strength and Power
3.8.3. Functional Mobility State
3.8.4. Body Composition
3.9. Immune System
4. Discussion
4.1. Cardiorespiratory Fitness
4.2. Muscle Strength and Power
4.3. Functional Mobility and Functional State
4.4. Body Composition
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Battaglini, C.L.; Hackney, A.C.; Garcia, R.; Groff, D.; Evans, E.; Shea, T. The Effects of an Exercise Program in Leukemia Patients. Integr. Cancer Ther. 2009, 8, 130–138. Available online: http://journals.sagepub.com/doi/10.1177/1534735409334266 (accessed on 24 February 2021). [CrossRef] [PubMed]
- Moya, R.; Espigado, I.; Parody, R.; Carmona, M.; Márquez, F.; De Blas, J.M. Evaluation of Readmissions in Hematopoietic Stem Cell Transplant Recipients. Transplant. Proc. 2006, 38, 2591–2592. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; Keats, M.R.; Turner, A.R. Physical exercise and quality of life in cancer patients following high dose chemotherapy and autologous bone marrow transplantation. Psychooncology 2000, 9, 127–136. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10767750 (accessed on 22 August 2019). [CrossRef]
- Weisdorf, D.; Haake, R.; Blazar, B.; Miller, W.; McGlave, P.; Ramsay, N.; Kersey, J.; Filipovich, A. Treatment of moderate/severe acute graft-versus-host disease after allogeneic bone marrow transplantation: An analysis of clinical risk features and outcome. Blood 1990, 75, 1024–1030. Available online: https://pubmed.ncbi.nlm.nih.gov/2302454/ (accessed on 27 August 2020). [CrossRef] [PubMed]
- Copelan, E.A. Hematopoietic stem-cell transplantation. N. Engl. J. Med. 2006, 354, 1813–1826. Available online: https://pubmed.ncbi.nlm.nih.gov/16641398/ (accessed on 27 August 2020). [CrossRef]
- Bhatia, S.; Francisco, L.; Carter, A.; Sun, C.-L.; Baker, K.S.; Gurney, J.G.; McGlave, P.B.; Nademanee, A.; O’Donnell, M.; Ramsay, N.K.C.; et al. Late mortality after allogeneic hematopoietic cell transplantation and functional status of long-term survivors: Report from the Bone Marrow Transplant Survivor Study. Blood 2007, 110, 3784–3792. Available online: https://ashpublications.org/blood/article-pdf/110/10/3784/1290674/zh802207003784.pdf (accessed on 30 August 2020). [CrossRef]
- Sun, C.L.; Francisco, L.; Kawashima, T.; Leisenring, W.; Robison, L.L.; Baker, K.S.; Weisdorf, D.J.; Forman, S.J.; Bhatia, S. Prevalence and predictors of chronic health conditions after hematopoietic cell transplantation: A report from the Bone Marrow Transplant Survivor Study. Blood 2010, 116, 3129–3139. Available online: https://pubmed.ncbi.nlm.nih.gov/20656930/ (accessed on 30 August 2020). [CrossRef] [Green Version]
- Decker, W.; McTurner-McGlade, J.; Fehir, K. Psychosocial aspects and the physiological effects of a cardiopulmonary exercise program in patients undergoing bone marrow transplantation (BMT) for acute leukemia (AL). Transplant. Proc. 1989, 21 Pt 3, 3068–3069. Available online: https://pubmed.ncbi.nlm.nih.gov/2650427/ (accessed on 27 August 2020). [CrossRef] [Green Version]
- Curt, G.A.; Breitbart, W.; Cella, D.; Groopman, J.E.; Horning, S.J.; Itri, L.M.; Johnson, D.H.; Miaskowski, C.; Scherr, S.L.; Portenoy, R.K.; et al. Impact of Cancer-Related Fatigue on the Lives of Patients: New Findings From the Fatigue Coalition. Oncologist 2000, 5, 353–360. Available online: https://pubmed.ncbi.nlm.nih.gov/11040270/ (accessed on 27 August 2020). [CrossRef] [Green Version]
- Hacker, E.D.; Ferrans, C.; Verlen, E.; Ravandi, F.; Van Besien, K.; Gelms, J.; Dieterle, N. Fatigue and Physical Activity in Patients Undergoing Hematopoietic Stem Cell Transplant. Oncol. Nurs. Forum 2006, 33, 614–625. Available online: https://pubmed.ncbi.nlm.nih.gov/16676017/ (accessed on 27 August 2020). [CrossRef] [Green Version]
- Hayes, S.; Davies, P.S.W.; Parker, T.; Bashford, J. Total energy expenditure and body composition changes following peripheral blood stem cell transplantation and participation in an exercise programme. Bone Marrow Transplant. 2003, 31, 331–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumann, F.; Zimmer, P.; Finkenberg, K.; Hallek, M.; Bloch, W.; Elter, T. Influence of endurance exercise on the risk of pneumonia and Fever in leukemia and lymphoma patients undergoing high dose chemotherapy. A pilot Study. J. Sports Sci. Med. 2012, 11, 638–642. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24150073 (accessed on 28 August 2020).
- Thonnard, J.L.; Penta, M. Functional assessment in physiotherapy. A literature review. Eura Medicophys. 2007, 43, 525–541. [Google Scholar] [PubMed]
- Haig, A.J.; Jayarajan, S.; Maslowski, E.; Yamakawa, K.S.; Tinney, M.; Beier, K.P.; Juang, D.; Chan, L.; Boggess, T.; Loar, J.; et al. Development of a language-independent functional evaluation. Arch. Phys. Med. Rehabil. 2009, 90, 2074–2080. Available online: https://pubmed.ncbi.nlm.nih.gov/19969171/ (accessed on 18 February 2021). [CrossRef] [PubMed]
- Hayes, S.; Davies, P.S.W.; Parker, T.; Bashford, J.; Newman, B. Quality of life changes following peripheral blood stem cell transplantation and participation in a mixed-type, moderate-intensity, exercise program. Bone Marrow Transplant. 2004, 33, 553–558. Available online: http://www.ncbi.nlm.nih.gov/pubmed/14716346 (accessed on 10 September 2019). [CrossRef] [Green Version]
- Velasco Rami, J.A.; Maroto Montero, J.M. Cardiac rehabilitation. Its historical evolution and current situation. Rev. Esp. Cardiol. 1995, 48 (Suppl. 1), 1–7. [Google Scholar]
- Winningham, M.L.; MacVicar, M.G. Exercise as a tension reduction mechanism in cancer patients. Ohio J. Sci. 1983, 83, 75. [Google Scholar]
- MacVicar, M.G.; Winningham, M.L.N.J. Effects of aerobic interval training on cancer patients functional capacity. Nurs. Res. 1989, 38, 348–351. Available online: https://pubmed.ncbi.nlm.nih.gov/2587289/ (accessed on 24 December 2021). [CrossRef]
- Lucia, A.; Earnest, C.; Perez, M. Cancer-related fatigue: Can exercise physiology assist oncologists? Lancet Oncol. 2003, 4, 616–625. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Dimeo, F.; Bertz, H.; Finke, J.; Fetscher, S.; Mertelsmann, R.; Keul, J. An aerobic exercise program for patients with haematological malignancies after bone marrow transplantation. Bone Marrow Transplant. 1996, 18, 1157–1160. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8971388 (accessed on 30 August 2019). [PubMed]
- Papasavvas, T.; Bonow, R.O.; Alhashemi, M.; Micklewright, D. Depression Symptom Severity and Cardiorespiratory Fitness in Healthy and Depressed Adults: A Systematic Review and Meta-Analysis. Sport Med. 2016, 46, 219–230. Available online: https://link.springer.com/article/10.1007/s40279-015-0409-5 (accessed on 22 April 2021). [CrossRef] [PubMed]
- Baumann, F.T.; Kraut, L.; Schüle, K.; Bloch, W.; Fauser, A.A. A controlled randomized study examining the effects of exercise therapy on patients undergoing haematopoietic stem cell transplantation. Bone Marrow Transplant. 2010, 45, 355–362. Available online: https://pubmed.ncbi.nlm.nih.gov/19597418/ (accessed on 27 August 2020). [CrossRef] [PubMed] [Green Version]
- Wilk, M.; Gepfert, M.; Krzysztofik, M.; Mostowik, A.; Filip, A.; Hajduk, G.; Zajac, A. Impact of duration of eccentric movement in the one-repetition maximum test result in the bench press among women. J. Sport Sci. Med. 2020, 19, 317–322. [Google Scholar]
- Drum, S.N.; Klika, R.J.; Carter, S.D.; Sprod, L.K.; Donath, L. A feasibility study related to inactive cancer survivors compared with non-cancer controls during aerobic exercise training. J. Sport Sci. Med. 2016, 15, 592–600. Available online: http://www.jssm.org (accessed on 24 February 2021).
- Fiuza-Luces, C.; Simpson, R.J.; Ramírez, M.; Lucia, A.; Berger, N.A. Physical function and quality of life in patients with chronic GvHD: A summary of preclinical and clinical studies and a call for exercise intervention trials in patients. Bone Marrow Transplant. 2016, 51, 13–26. Available online: http://www.nature.com/articles/bmt2015195 (accessed on 27 August 2019). [CrossRef] [PubMed]
- Dimeo, F.; Tilmann, M.H.M.; Bertz, H.; Kanz, L.; Mertelsmann, R.; Keul, J. Aerobic exercise in the rehabilitation of cancer patients after high dose chemotherapy and autologous peripheral stem cell transplantation. Cancer 1997, 79, 1717–1722. [Google Scholar] [CrossRef]
- Dimeo, F.; Fetscher, S.; Lange, W.; Mertelsmann, R.; Keul, J. Effects of Aerobic Exercise on the Physical Performance and Incidence of Treatment-Related Complications After High-Dose Chemotherapy. Blood 1997, 90, 3390–3394. Available online: https://pubmed.ncbi.nlm.nih.gov/9345021/ (accessed on 27 August 2020). [CrossRef]
- Hacker, E.D.; Kim, I.; Park, C.; Peters, T. Real-time Fatigue and Free-Living Physical Activity in Hematopoietic Stem Cell Transplantation Cancer Survivors and Healthy Controls. Cancer Nurs. 2017, 40, 259–268. Available online: http://journals.lww.com/00002820-201707000-00002 (accessed on 10 August 2020). [CrossRef]
- DeFor, T.E.; Burns, L.J.; Gold, E.A.; Weisdorf, D.J. A Randomized Trial of the Effect of a Walking Regimen on the Functional Status of 100 Adult Allogeneic Donor Hematopoietic Cell Transplant Patients. Biol. Blood Marrow Transplant. 2007, 13, 948–955. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1083879107002480 (accessed on 12 August 2020). [CrossRef] [Green Version]
- Jarden, M.; Hovgaard, D.; Boesen, E.; Quist, M.; Adamsen, L. Pilot study of a multimodal intervention: Mixed-type exercise and psychoeducation in patients undergoing allogeneic stem cell transplantation. Bone Marrow Transplant. 2007, 40, 793–800. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17704795 (accessed on 15 July 2019). [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Elkins, M.R.; Moseley, A.M.; Sherrington, C.; Herbert, R.D.; Maher, C.G. Growth in the Physiotherapy Evidence Database (PEDro) and use of the PEDro scale. Br. J. Sports Med. 2013, 47, 188–189. Available online: http://bjsm.bmj.com/lookup/doi/10.1136/bjsports-2012-091804 (accessed on 25 August 2020). [CrossRef]
- Shelton, M.L.; Lee, J.Q.; Morris, G.S.; Massey, P.R.; Kendall, D.G.; Munsell, M.F.; Anderson, K.O.; Simmonds, M.J.; Giralt, S.A. A randomized control trial of a supervised versus a self-directed exercise program for allogeneic stem cell transplant patients. Psychooncology 2009, 18, 353–359. Available online: http://doi.wiley.com/10.1002/pon.1505 (accessed on 15 August 2020). [CrossRef]
- Barğı, G.; Güçlü, M.B.; Arıbaş, Z.; Akı, Ş.Z.; Sucak, G.T. Inspiratory muscle training in allogeneic hematopoietic stem cell transplantation recipients: A randomized controlled trial. Support Care Cancer 2016, 24, 647–659. Available online: http://link.springer.com/10.1007/s00520-015-2825-3 (accessed on 16 August 2020). [CrossRef]
- Wiskemann, J.; Dreger, P.; Schwerdtfeger, R.; Bondong, A.; Huber, G.; Kleindienst, N.; Ulrich, C.M.; Bohus, M. Effects of a partly self-administered exercise program before, during, and after allogeneic stem cell transplantation. Blood 2011, 117, 2604–2613. [Google Scholar] [CrossRef]
- Hacker, E.D.; Larson, J.; Kujath, A.; Peace, D.; Rondelli, D.; Gaston, L. Strength Training Following Hematopoietic Stem Cell Transplantation. Cancer Nurs. 2011, 34, 238–249. Available online: http://journals.lww.com/00002820-201105000-00011 (accessed on 15 August 2020). [CrossRef] [Green Version]
- Baumann, F.; Zopf, E.M.; Nykamp, E.; Kraut, L.; Schüle, K.; Elter, T.; Fauser, A.; Bloch, W. Physical activity for patients undergoing an allogeneic hematopoietic stem cell transplantation: Benefits of a moderate exercise intervention. Eur. J. Haematol. 2011, 87, 148–156. Available online: http://doi.wiley.com/10.1111/j.1600-0609.2011.01640.x (accessed on 15 August 2020). [CrossRef]
- Coleman, E.A.; Coon, S.; Hall-Barrow, J.; Richards, K.; Gaylor, D.; Stewart, B. Feasibility of Exercise During Treatment for Multiple Myeloma. Cancer Nurs. 2003, 26, 410–419. Available online: http://journals.lww.com/00002820-200310000-00012 (accessed on 16 August 2020). [CrossRef]
- Jarden, M.; Nelausen, K.; Hovgaard, D.; Boesen, E.; Adamsen, L. The Effect of a Multimodal Intervention on Treatment-Related Symptoms in Patients Undergoing Hematopoietic Stem Cell Transplantation: A Randomized Controlled Trial. J. Pain Symptom Manag. 2009, 38, 174–190. [Google Scholar] [CrossRef]
- Kim, S.D.; Kim, H.S. A series of bed exercises to improve lymphocyte count in allogeneic bone marrow transplantation patients. Eur. J. Cancer Care 2006, 15, 453–457. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17177902 (accessed on 16 August 2019). [CrossRef]
- Jarden, M.; Baadsgaard, M.; Hovgaard, D.; Boesen, E.; Adamsen, L. A randomized trial on the effect of a multimodal intervention on physical capacity, functional performance and quality of life in adult patients undergoing allogeneic SCT. Bone Marrow Transplant. 2009, 43, 725–737. [Google Scholar] [CrossRef]
- Knols, R.H.; de Bruin, E.D.; Uebelhart, D.; Aufdemkampe, G.; Schanz, U.; Stenner-Liewen, F.; Hitz, F.; Taverna, C.; Aaronson, N.K. Effects of an outpatient physical exercise program on hematopoietic stem-cell transplantation recipients: A randomized clinical trial. Bone Marrow Transplant. 2011, 46, 1245–1255. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21132025 (accessed on 31 August 2019). [CrossRef] [Green Version]
- Schumacher, H.; Stüwe, S.; Kropp, P.; Diedrich, D.; Freitag, S.; Greger, N.; Junghanss, C.; Freund, M.; Hilgendorf, I. A prospective, randomized evaluation of the feasibility of exergaming on patients undergoing hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018, 53, 584–590. [Google Scholar] [CrossRef] [Green Version]
- Wiskemann, J.; Kuehl, R.; Dreger, P.; Schwerdtfeger, R.; Huber, G.; Ulrich, C.M.; Jaeger, D.; Bohus, M. Efficacy of exercise training in SCT patients-who benefits most? Bone Marrow Transplant. 2014, 49, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Mello, M.; Tanaka, C.; Dulley, F.L. Effects of an exercise program on muscle performance in patients undergoing allogeneic bone marrow transplantation. Bone Marrow Transplant. 2003, 32, 723–728. Available online: http://www.ncbi.nlm.nih.gov/pubmed/13130321 (accessed on 31 August 2019). [CrossRef]
- Wiskemann, J.; Kleindienst, N.; Kuehl, R.; Dreger, P.; Schwerdtfeger, R.; Bohus, M. Effects of physical exercise on survival after allogeneic stem cell transplantation. Int. J. Cancer. 2015, 137, 2749–2756. Available online: http://doi.wiley.com/10.1002/ijc.29633 (accessed on 17 August 2020). [CrossRef]
- Peters, T.; Erdmann, R.; Hacker, E.D. Exercise intervention: Attrition, compliance, adherence, and progression following hematopoietic stem cell transplantation. Clin. J. Oncol. Nurs. 2018, 22, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Pahl, A.; Wehrle, A.; Kneis, S.; Gollhofer, A.; Bertz, H. Feasibility of whole body vibration during intensive chemotherapy in patients with hematological malignancies—A randomized controlled pilot study. BMC Cancer 2018, 18, 920. Available online: https://bmccancer.biomedcentral.com/articles/10.1186/s12885-018-4813-8 (accessed on 19 November 2020). [CrossRef] [Green Version]
- Persoon, S.; ChinAPaw, M.; Buffart, L.; Liu, R.K.; Wijermans, P.; Koene, H.; Minnema, M.; Lugtenburg, P.; Marijt, E.W.A.; Brug, J.; et al. Randomized controlled trial on the effects of a supervised high intensity exercise program in patients with a hematologic malignancy treated with autologous stem cell transplantation: Results from the EXIST study. PLoS ONE 2017, 12, 15. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28727771 (accessed on 18 August 2020). [CrossRef] [Green Version]
- Bird, L.; Arthur, A.; Niblock, T.; Stone, R.; Watson, L.; Cox, K. Rehabilitation programme after stem cell transplantation: Randomized controlled trial. J. Adv. Nurs. 2010, 66, 607–615. Available online: http://doi.wiley.com/10.1111/j.1365-2648.2009.05232.x (accessed on 16 August 2020). [CrossRef] [PubMed]
- Oechsle, K.; Aslan, Z.; Suesse, Y.; Jensen, W.; Bokemeyer, C.; de Wit, M. Multimodal exercise training during myeloablative chemotherapy: A prospective randomized pilot trial. Support Care Cancer 2014, 22, 63–69. Available online: http://link.springer.com/10.1007/s00520-013-1927-z (accessed on 18 November 2020). [CrossRef] [PubMed]
- Van Dongen, J.M.; Persoon, S.; Jongeneel, G.; Bosmans, J.E.; Kersten, M.J.; Brug, J.; Nollet, F.; Chinapaw, M.J.M.; Buffart, L.M. Long-term effectiveness and cost-effectiveness of an 18-week supervised exercise program in patients treated with autologous stem cell transplantation: Results from the EXIST study. J. Cancer Surviv. 2019, 13, 558–569. Available online: http://link.springer.com/10.1007/s11764-019-00775-9 (accessed on 18 November 2020). [CrossRef] [PubMed] [Green Version]
- Pahl, A.; Wehrle, A.; Kneis, S.; Gollhofer, A.; Bertz, H. Whole body vibration training during allogeneic hematopoietic cell transplantation—The effects on patients’ physical capacity. Ann. Hematol. 2020, 99, 635–648. [Google Scholar] [CrossRef] [Green Version]
- De Almeida, L.B.; Trevizan, P.F.; Laterza, M.C.; Neto, A.E.H.; de São José, A.C.A.; Martinez, D.G. Safety and feasibility of inspiratory muscle training for hospitalized patients undergoing hematopoietic stem cell transplantation: A randomized controlled study. Support Care Cancer. 2020, 28, 3627–3635. [Google Scholar] [CrossRef]
- Van Haren, I.E.P.M.; Timmerman, H.; Potting, C.M.; Blijlevens, N.M.A.; Staal, J.B.; Nijhuis-van der Sanden, M.W.G. Physical exercise for patients undergoing hematopoietic stem cell transplantation: Systematic review and meta-analyses of randomized controlled trials. Phys. Ther. 2013, 93, 514–528. Available online: https://pubmed.ncbi.nlm.nih.gov/23224217/ (accessed on 21 July 2021). [CrossRef]
- Persoon, S.; Kersten, M.J.; van der Weiden, K.; Buffart, L.M.; Nollet, F.; Brug, J.; Chinapaw, M.J.M. Effects of exercise in patients treated with stem cell transplantation for a hematologic malignancy: A systematic review and meta-analysis. Cancer Treat. Rev. 2013, 39, 682–690. [Google Scholar] [CrossRef]
- Issues, S.; Test, M.W.; Equipment, R.; Preparation, P. American Thoracic Society ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar]
- Convertino, V.A. Cardiovascular consequences of bed rest: Effect on maximal oxygen uptake. Med. Sci. Sports Exerc. 1997, 29, 191–196. Available online: https://pubmed.ncbi.nlm.nih.gov/9044222/ (accessed on 29 May 2021). [CrossRef]
- Al-Majid, S.; Mccarthy, D.O. Cancer-Induced Fatigue and Skeletal Muscle Wasting: The Role of Exercise. Biol. Res. Nurs. 2001, 2, 186–197. Available online: https://pubmed.ncbi.nlm.nih.gov/11547540/ (accessed on 2 July 2021). [CrossRef]
- Morishita, S.; Kaida, K.; Yamauchi, S.; Wakasugi, T.; Ikegame, K.; Ogawa, H.; Domen, K. Relationship of physical activity with physical function and health-related quality of life in patients having undergone allogeneic haematopoietic stem-cell transplantation. Eur. J. Cancer Care 2017, 26, e12669. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.; Friedenreich, C.M. Physical exercise and quality of life following cancer diagnosis: A literature review. Ann. Behav. Med. 1999, 21, 171–179. Available online: https://academic.oup.com/abm/article/21/2/171-179/4631432 (accessed on 27 August 2020). [CrossRef] [PubMed]
- Van Haren, I.E.P.M.; Staal, J.B.; Potting, C.M.; Atsma, F.; Hoogeboom, T.J.; Blijlevens, N.M.A.; Nijhuis-van der Sanden, M.W.G. Physical exercise prior to hematopoietic stem cell transplantation: A feasibility study. Physiother. Theory Pract. 2018, 34, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Hacker, E.D.; Mjukian, M. Review of attrition and adherence in exercise studies following hematopoietic stem cell transplantation. Eur. J. Oncol. Nurs. 2014, 18, 175–182. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Items | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score |
| (Baumann et al., 2010) [23] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (Jarden et al., 2007) [31] | + | + | + | + | + | ? | ? | + | + | + | + | 9 |
| (Shelton et al., 2009) [34] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (DeFor et al., 2007) [30] | + | + | + | ? | ? | ? | ? | + | + | + | + | 6 |
| (Barğı et al., 2016) [35] | + | + | + | + | + | + | - | + | + | + | + | 9 |
| (Wiskemann et al., 2011) [36] | + | + | + | + | ? | ? | ? | + | + | + | + | 7 |
| (Hacker et al., 2011) [37] | + | + | + | + | ? | ? | ? | + | + | + | + | 7 |
| (Baumann et al., 2011) [38] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (Coleman et al., 2003) [39] | + | + | + | + | ? | ? | ? | + | + | + | + | 7 |
| (Jarden et al., 2009) [40] | + | + | + | + | + | - | - | + | + | + | + | 8 |
| (KIM & KIM, 2006) [41] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (Jarden et al., 2009) [42] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (Knols et al., 2011) [43] | + | + | + | + | + | - | + | + | + | + | + | 10 |
| (Schumacher et al., 2018) [44] | + | + | + | + | + | ? | ? | + | + | + | + | 8 |
| (Wiskemann et al., 2014) [45] | + | + | + | + | + | - | - | + | + | + | + | 8 |
| (Mello et al., 2003) [46] | + | + | ? | + | ? | ? | ? | + | + | + | + | 6 |
| (Wiskemann et al., 2015) [47] | + | + | ? | + | ? | ? | ? | + | + | + | + | 6 |
| (Peters et al., 2018) [48] | + | + | + | + | + | - | - | + | + | + | + | 8 |
| (Pahl et al., 2018) [49] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (Persoon et al., 2017) [50] | + | + | + | + | + | + | + | + | + | + | + | 10 |
| (Bird et al., 2010) [51] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (Oechsle et al., 2014) [52] | + | + | - | + | - | - | - | + | + | + | + | 6 |
| (Van Dongen et al., 2019) [53] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| (Pahl et al., 2020) [54] | + | + | + | + | + | - | - | + | + | + | + | 8 |
| (Almeida et al., 2020) [55] | + | + | + | + | + | - | - | + | + | + | + | 8 |
| Study | Study Design | Sample Size by Group (Sex), Age (Mean ± SD; Range) | Primary Cancer | Intervention | Main Results in Physical Related Variables |
|---|---|---|---|---|---|
| (DeFor et al., 2007) [30] | RCT T1: Pre HSCT (A) T2: Post HSCT (100 days) | - EXP: n = 51 (22 female), 46 years (18–68) - CT: n = 49 (17 female), 49 years (22–64) | AA, ALL, AML, CML, HL, LHN, MDS | Type: AT (walking on treadmill) Duration: 100 days Intensity: Comfortable speed Supervised: not Frequency: 7 times/week Setting: Clinic/home | T1-T2: - ↓ KPS: ↓ EXP (-10 pts/100 pts) ↓ CT (-20 pts/100 pts) - ↔ Immune system |
| (Wiskemann et al., 2011) [36] | RCT T1: Pre HSCT (medical checkup)-Pre HSCT (4 week A) T2: Post HSCT (H)-Post HSCT (D) T3: Post HSCT (D)-Post HSCT (D 6–8 weeks) | - EXP: n = 52 (21 female), 47.6 years (18–70) - CT: n = 53, (13 female), 50 years (20–71) | AA, ALL, AML, CLL, CML, MDS, MM, MPS, Others | Type: AT (walking, stationary bicycle), ST (elastic bands) Duration: 18 weeks Intensity and volume: AT 1–4 week to (A) 3 times a week, from (H) 3–5 times a week RPE (12–14/20), DCT: color codes (Red 15–20 min, yellow 20–30 min, green 30–40 min), from 1–8 week rehabilitation 3 times a week. ST 1–4 week to (A) twice a week, from (H) twice a week (2–3 sets of 8–20 reps RPE 14–16/20), from 1–8 week rehabilitation twice a week. Supervised: yes T2 and self-directed T1 and T3 Setting: Home/Hospital | T1 - ↑ 6MWT (∆-0.19%) - ↔ Immune system |
| (Baumann et al., 2011) [38] | RCT T1:Pre HSCT (A) T2:Post HSCT (7–8 weeks) | - EXP: n = 17, (6 female), 41.41 ± 11.78 a years - CT = n = 16, (11 female), 42.81 ± 14.04 a years | ALL, AML, CLL, CML, MDS, MM, MPS, PID | Type: AT (stationary bicycle), ADL, stretching, coordination Duration: 7–8 weeks Volume and intensity: AT (H) once-twice a week (10–20 min/day continuous or interval training at HRmax 80%); ADL-training (H) 5 times a day (20 min a day, 5 × 20 steps with 1 min break of slightly strenuous or strenuous); mobilization passive and active 1 day after HSCT until 1 day before hospital discharge daily except on weekends Low intensity; or not strenuous (CT) 20 min a day Cadence: AT cycle (since 25 W with 25 W increment every 2 min) Supervised: yes Setting: hospital | T1-T2: - Endurance: ↓ CT (∆-23.5%) - Relative endurance: ↓ CT/↑ EXP (∆-15.8%; ∆11.02%) - Strength lower extremities: ↓ CT (∆-26.8%) - BMI: ↓ CT/↓ EXP (∆-8.2%; ∆-13.2%) - ↔ Immune system |
| (Coleman et al., 2003) [39] | RCT with RM T1:Pre HSCT (A) T2: Post HSCT (3 months) | - EXP: n = 14 - CT: n = 10; (10 female), 55 years (42–74) | MM | Type: AT (walking), ST (elastic bands) Duration: 6 months Intensity and volume: AT 3 times a week (18 min fast-paced walking at RPE 12–15/20), ST 3 times a week with color bands (1 set of 8 red 9–15 Ib, 1 set of 8 green 5–9 Ib) and (2 sets of 8 chair stands of 1 RM) Supervised: not Setting: home | T1-T2: - LBW: ↑ EXP/↓ CT (∆0.1%; ∆-3.6%) - Strenght: ↑ EXP/↓ CT (∆2.4%; ∆-12.6%) - ↔ Immune system |
| (Jarden et al., 2009) [42] | RCT T1: Pre HSCT (A) T2: Post HSCT (6 weeks) | - EXP: n = 21, (8 female), 40.9 years (18–60) - CT: n = 21, (8 female), 37.4 years (18–55) | AA, ALL, AML, CML, MDS, MF, PNH, WM | Type: AT (stationary bicycle), ST (hand and ankle weights), stretching, relaxation Duration: 4–6 weeks Intensity and volume: AT 5 times a week (HRmax 50–75% Low to moderate RPE 10/13), stretching (Dynamic: 1–2 sets of 10–12 reps; Static: 1 set/15–30 seg), ST 3 times a week (1–2 sets of 10–12 reps at low to moderate, RPE 10/13) and relaxation twice a week (Low RPE 6/9) Cadence: 30–70 cycles/min and range at 30–75 W. Supervised: yes Setting: Hospital | T1-T2: - ↔ Immune system |
| (Jarden et al., 2009) [40] | RCT T1: Pre HSCT (A) T2: PostHSCT (D) | - EXP: n = 21 (8 female), 45.0 years (18–60) - CT: n = 21 (8 female), 38.0 years (18–55) | AA, ALL, AML, CML, MDS, MF, PNH, WM | Type: AT (stationary bicycle), ST (hand and ankle weights), stretching, relaxation Duration:4–6 weeks Intensity and volume: AT 5 times a week Low to moderate (HRmax 50–75% of RPE 10/13), stretching (Dynamic: 1–2 sets of 10–12 reps; Static: 1 set/15–30 sg), ST 3 times a week low to moderate, (1–2 sets of 10–12 reps at RPE 10/13) and relaxation twice a week (Low RPE 6/9) Cadence: 30–70 cycles/min and range of 30–75 W. Volume: ST, stretching and relaxation (Dynamic: (1–2 sets of 10–12 reps); Static: (1 set 15–30 sg) Supervised: yes Setting: Hospital | T1-T2: - VO2: ↑ EXP/↓ CT (∆3.1%; ∆-28.6%) - Chest press: ↑ EXP/↓ CT (∆5.3%; ∆-18.6%) - Leg extension: ↑ EXP/↓ CT (∆4.3%; ∆-30.3%) - Right elbow flexor: ↑ EXP/↓ CT (∆6.4%; ∆-23.1%) - Right knee extensor: ↑ EXP/↓ CT (∆3.5%; (∆-21.3%) - 2MWT: ↓ EXP/↓ CT (∆-26.0%; ∆-11.3%) - ↔ Immune system |
| (Wiskemann et al., 2014) [45] | Multicenter RCT T1: Pre HSCT (baseline)-Pre HSCT (A) T2: Pre HSCT (A)-Post HSCT (D) T3: Post HSCT (D)-Post HSCT (6–8 weeks) | - EXP: n = 52, (21 female), 47.6 years (18–70) - CT: n = 53, (13 female), 50 years (20–71) | AA, ALL, AML, CLL, CML, Lymphoma, MDS, MM | Type: AT (N/R), ST (elastic bands) Duration: 8 weeks. Frequency: AT: T1 (3 times a week), T2 (5 times a week), T3 (3 times a week). ST: T1, T2, and T3 (twice a week). Intensity and volume: Not specified Supervised: yes Setting: home/hospital | T1-T3: EXfit: - ↓ Knee extensión (∆-31.3%) - ↓ Hip flexion (∆-16.4%) - ↓ Elbow extensión (∆-21.2%) - ↓ Elbow flexion (∆-22.1%) - ↓ 6MWT (∆-4.3%) T1-T3: Exunfit: - ↓ Knee extensión (∆-8.6%) - ↑ Hip flexion (∆10.3%) - ↑ Elbow extensión (∆3.4%) - ↓ Elbow flexion - ↑ 6MWT (∆10.4%) - ↔ Immune system |
| (Baumann et al., 2010) [23] | RCT T1: Pre HSCT (A) T2: Post HSCT (D) | - EXP: n = 32, (11 female), 44.9 ± 12.4 b years - CT: n = 32, (18 female), 44.1 ± 14.2 b years | ALL, AML, CLL, CML, LHN, MDS, MM, Solid tumour, immuno-deficiency | Type: AT (stationary bicycle), ADL Duration: 7 weeks Volume: AT twice a week (80% HRmax), ADL 5 times a week (5 × 20 steps with 1 min break RPE ‘slightly strenuous’ to ‘strenuous’. CT 5 times a week Cadence: AT (increase 25 W/2 min) Supervised: yes Setting: hospital | T1-T2: - Relative endurance: ↑ EXP/↓ CT (∆16.7%; (∆-16.7%) - Plts: ↓ EXP/↓ CT - Hb: ↓ EXP/↓CT - Leucocytes: ↓ CT |
| (Jarden et al., 2007) [31] | RCT T1: Pre HSCT (A) T2:Post HSCT (±1 day D) | - EXP: n = 6 (2 female), 34 years (18–58) - CT: n = 8 (4 female) 37 years (18–53) | AA, ALL, AML, CML, hemoglobinuria, LHN, MF, MM, PNH | Type: AT (stationary bicycle), ST (hand and ankle weights), stretching, relaxation Duration: 6 weeks Intensity and volume: AT 5 times a week (Low to moderate 50–75% HR max and RPE 10–13/20), ST 3 times a week (Low to moderate 1–2 sets of 10–12 reps of 1RM at RPE 10–13/20), stretching 5 times a week (Dynamic: 1–2 sets of 10–12 reps Static: 1 set, hold for 15–30 s), relaxation 2 times a week (Low RPE 6–9/20), Psychoeducation 5 times a week Cadence: 30–70 cycles since 50 W Supervised: yes Setting: hospital | T1-T2: - Chest press:↓ CT (∆-14.9%) - Leg ext: ↑ EXP/↓ CT (∆6.1%; ∆-16.3%) - Right knee flex: ↑ EXP/↓ CT (∆0.2%; ∆-14.5%) - ↔ Immune system |
| (Mello et al., 2003) [46] | RCT T1: Pre HSCT (A)-Post HSCT (D) T2: Post HSCT (6 weeks) | - EXP: n = 9, (4 female), 27.9 years (18–39) - CT: n = 9, (6 female), 30.2 years (18–44) | AML, CML, LHN, MDS, SAA | Type:AT (walking), stretching, mobilization Duration: 6 weeks Volume: AT, range of motion and stretching (5 sets of 3 min comfortable walk to 2 sets of 10–20 min at 70% HR max speed walk in the sixth week) Rest: 3 min Supervised: yes Setting: hospital | T1-T2: - Knee DM-NDM Flexors: ↓ EXP/↓ CT - Shoulder:DM–NDM: ↓ CT - Elbow DM flexors/NDM: ↓ CT - Ankle DM/NDM Flexors: ↓ CT - ↔ Immune system |
| (Wiskemann et al., 2015) [47] | Multicenter RCT T1: Pre HSCT (A) T2: Post HSCT (D) | - EXP: n = 50, (21 female), 48.2 ± 14.5 b years - CT: n = 53, (13 female), 50 ± 12.4 b years | AA, ALL, AML, CLL, CML, Lymphoma, MDS, MM | Type: AT (walking, stationary bicycle), ST (elastic bands) Duration: 15–18 weeks Volume and Intensity: AT 3–5 times a week (RPE 12–14/20), ST twice a week (RPE 12–14/20) Supervised: yes Setting: home/hospital | T1-T2: - No changes |
| (Peters et al., 2018) [48] | RCT T1: Pre HSCT (H) T2: Post HSCT (D) T3: Post HSCT (6 weeks) | n = 70, 53.1 ± 13.5 years - EXP: n = 37 (15 female) - CT: n = 33 (13 female) | ALL, AML, CLL, CML, HL, LHN, MDS, MM | Type: ST (elastic bands), range of motion Duration: 6 weeks Intensity: ST T2-T3 (RPE 13–14/20) Intensity and volume: ST and range of motion: T2-T3 three times a week for 16 weeks with 18 sessions (1–2 sets of increase reps with bands) Supervised: not T1-T2 and yes T2-T3 Setting: hospital/home | - No changes |
| (Pahl et al., 2018) [49] | RCT pilot study T1: Pre HSCT (Admission) T2: Post HSCT (D) | - EXP: n = 6 (1 female), 47 years (19–62) - CT: n = 5 (2 female), 56 years (32–63) | ALL, AML, APL, HL, LHN, MM, MW, PMF | Type: AT stationary bicycle (CT), and ST with vibration (EXP) Duration: 27 days Intensity: AT and ST (RPE 14–16/20) Intensity and Volume: AT (CT) (20 min with/without rest), ST (EXP) 3times a week (3 sets, 30–60 sg) Rest: ST: 30–60 sg (between exercises), 60–120 sg (between sets) Supervised: yes Setting: Hospital | T1-T2: - ↑ Jumping height (∆12.4%) - ↓ TUG (∆-19.4%) ↑ STEO/↑ STEC sway path (∆5.5%, (∆7.7%)) |
| (Pahl et al., 2020) [54] | RCT T1: Pre HSCT (Admission) T2: Post HSCT (D) T3: PostHSCT (180 days D) | - EXP: n = 18 (7 female), 55 years (50–63) - CT: n = 26 (7 female), 56 years (32–63) | ALL, AML, CLL, CML, Lymphoma, MDS, MF, MM, SAA, Septic granulomatosis, | Type: ST with vibration (EXP), mobilization of the spine and stretching (CT) Duration: N/R Intensity: N/R Volume: WBV/ST (EXP) 5times a week (20 min), mobilization and stretching (CT) 5times a week (20 min) Supervised: yes Setting: Hospital | T1-T3: - VO2: ↑ EXP/↓ CT (∆5.3%; (∆-11.8%) - P max: ↑ EXP(∆16.3%) - Knee flexors/extensors: ↓ CT (∆-23.1%; ∆-3.9%) - JH: ↓ CT (∆-3.3%) - BMI: ↓ EXP/↓ CT (∆-3.1%; (∆-12.4%) |
| (Almeida et al., 2020) [55] | RCT T1: Pre HSCT (Admission) T2: Post HSCT (D) | - EXP: n = 15 (7 female), 46.6 years (35.1–52) - CT: n = 16 (6 female), years 37.5 (39.5–53.6) | AML, Amyloidosis, HL, LHN, MM, SAA | Type: IMT (EXP) and AT (stationary bicycle), ADL, stretching, coordination, and balance (EXP/CT) Duration: N/R Intensity: IMT (40% MIP) Volume: IMT (EXP) 5 times a week (10–20 min, 12–16 diaphragmatic breathing per min), AT (EXP/CT) 5 times a week (10–20 min at 50–70% HR max), ADL weekends (EXP/CT), stretching (EXP) (CT) 5 times a week (10–20 min) Supervised: yes Setting: Hospital | T1-T2: - MIP: ↑ EXP (∆19.3%) |
| Study | Study Design | Sample Size by Group (Sex), Age (Mean ± SD; Range) | Primary Cancer | Intervention | Main Results in Physical Related Variables |
|---|---|---|---|---|---|
| (Shelton et al., 2009) [34] | RCT T1: Pre HSCT (A) T2:Post HSCT (4 weeks) | - Supervised: n = 26, (9 female), 43.65 ± 13.18 a years - Self-directed: n = 27, (11 female), 93 ± 11.66 a years | ALL, AML, CLL, CML, HD, Lymphoma, LHN | Type: AT (stationary bicycle, treadmill), ST (weight machines) Duration: 4 weeks Volume and intensity: AT: 3 days a week (20–30 min 60–75% HR max and BFI: 0–10), ST: 3 days a week EXP supervised (1–3 sets of 10 reps), EXP self-directed (1–3 sets of 10–15 reps). The AT and ST increased every third visit; if extreme fatigue, resistance was reduced to the previous level. Supervised: yes Setting: hospital/home | T1-T2: Supervised= - ↓ 50 FWT (∆-13.7%) Self-directed = - ↑ 6MWT (∆12.0%) - ↔ Immune system |
| (Barğı et al., 2016) [35] | RCT T1: Pre HSCT (A) T2: Post HSCT (6 weeks) | - EXP: n = 20, (8 female), 34.10 ± 12.65 a years - CT: n = 18, (6 female), 39.11 ± 12.57 a years | AA, ALL, AML, CML, Fanconi anemia, MDS, MM, LHN, PNH | Type: Respiratory muscle Duration: 6 weeks Volume and intensity: AT: 7 days at week (speed progressively increased at 1 min intervals walking at 12 stages/30 min rest between 2 tests with FIS (1–4). Diaphragmatic breaths: 7 days at week (EXP) (15 sg/25–30 breaths/5–10 resting IMT at 40% of MIP), (CT) (received sham IMT at fixed workload, 5% of baseline MIP with MMRC (0–4)) Supervised: yes Setting: hospital/home | T1-T2: - ↑ MISWT (∆8.0%) - ↑ 6MWT (∆5.8%) - ↑ MIP (∆36.6%) - MEP:↑ EXP/↑ CT (∆15.3%) - FEV1/FVC: ↓ CT (∆-1.1) - ↓ MMRC (∆-37.5%) - ↔ Immune system |
| (KIM & KIM, 2006) [41] | RCT T1: Pre HSCT (A) T2: Post HSCT (6 weeks) | - EXP: n = 18 (10 female), 32.9 ± 7.0 a years - CT: n = 17 (8 female), 34.3 ± 7.8 a years | AA, ALL, AML | Type: bed exercise intervention: Stretching, mobility, relaxation breathing Duration: 6 weeks Volume and intensity: Stretching and mobility bed exercise intervention: 7 days a week, 3 × 10 min: preliminary exercise. Relaxation breathing and finish exercise. Supervised: yes Setting: hospital | T1-T2: Lymphocytes: ↓ CT |
| (Persoon et al., 2017) [50] | RCT T1: Post HSCT (A) T2: Post HSCT (18 weeks) | - EXP: n = 54 (22 female), 53.5 years (20–67) - CT: n = 55 (18 female), 56 years (19–67) | HL, MM | Type: AT (stationary bicycle), ST (weight machines) Duration: 18 weeks Intensity and volume: AT 1–8 week twice a week (blocks of 30 sg at 65% MSEC alternated with blocks of 60 s at 30% MSEC), from 9–18 weeks (blocks of 30 s at 65% MSEC alternated with blocks of 30 sg at 30% MSEC), ST 1–12 weeks twice a week (2 sets/10 reps 60–80% 1 RM, from 13–18 weeks once a week (1 set/20 reps 35–40% 1RM). Supervised: Yes Setting: local physiotherapy | T1-T2: - No changes |
| (Bird et al., 2010) [51] | RCT T1: Post HSCT (A) T2: Post HSCT (6 months) | - EXP: n = 29 (13 female), 57 years (44–53.5) - CT: n = 29 (7 female), 52 years (42.5–63) | Leukaemia, Lymphoma, Myeloma | Type: AT, relaxation Duration: 10 weeks Intensity and volume: AT CEXP) 1–10 weeks (a series of circuit training exercise), relaxation (guided imagery). AT (CT) 1–10 weeks 3 times/week (home-based exercise program) Supervised: Yes Setting: Hospital/Home | T1-T2: - No changes |
| (Oechsle et al., 2014) [52] | RCT T1: Post HSCT (A) T2: Post HSCT (After intervention) | - EXP: n = 17 (7 female), years 51.7 ± 13.3 c - CT: n = 17 (7 female), years 52.9 ± 15.4 c | AML, LHN, MM, Germ cell tumor | Type: AT (stationary bicycle), ST (elastic bands, bodyweight) Duration: 21 days Intensity and volume: AT 5 times a week (10–20 min), ST 5 times a week (20 min, 2 sets of 16–25 reps at 40–60% of 1 RM) Rest: AT (regular pauses until recuperated to 66.6%) Supervised: Yes Setting: Hospital | T1-T2: - CT: ↓ VO2 (∆-26.0%) - EXP: ↑ VO2, VE and strength upper limbs (∆11.3%; (∆21.8%; (∆35.7%) |
| (Hacker et al., 2011) [37] | RCT T1: Pre HSCT-Post-HSCT (After 8° day) T2: H-Post-HSCT (1–6 week) | - EXP: n = 9 - CT: n = 10 n = 19, (5 female) 46.26 years (16.23)c | AML, Lymphoma | Type: ST (elastic bands, bodyweight) Duration: 6 weeks Volume and intensity: ST 1–6 weeks 3 times a week (1–2 sets of 8–10 reps of RPE (13/20) Supervised: yes Setting: hospital/home | T2: - ↑ 30CST: EXP/CT (∆-12.7%; ∆-12.0%) - ↓ TNSU: EXP/CT (∆-18.9%; ∆-20.3%) - ↔ Immune system |
| (Knols et al., 2011) [43] | RCT T1: Pre HSCT (A)-Post HSCT (D) T2: Post HSCT (D)-Post HSCT (3 months) | - EXP: n = 64 (26 female), 46.7 ± 13.7 years (18–75) a - CT: n = 67 (28 female), 46.6 ± 12 years (20–67) a | ALL, AML, Amyloidosis, CLL, HL, LHN, Lymphoma, MM, osteomyelofibrosis, testicular cancer | Type: AT (stationary bicycle), ST (dumbbell) Frequency: 2 days/week Duration: 12 weeks Intensity and volume: AT twice a time (50–70% to 80% HRmax) Supervised: yes Setting: fitness center/physiotherapy practise | T1-T2: - Knee extensión: ↑ EXP/↑ CT (∆26.2%) - Walk speed: ↓ EXP/↓ CT (∆-11.9%; ∆-2.4%) - 6MWT: ↑ EXP/↑ CT (∆17.7%; ∆9.8%) - ↔ Immune system |
| (Schumacher et al., 2018) [44] | RCT T1: Pre HSCT (A)-Post HSCT (14 days) T2: Pre HSCT (A)-Post HSCT (30 days) | - EXP: n = 19 (3 female), 56 years (21–65) b - CT: n = 23 (14 female), 56.5 years (23–69) b | AML, CLL, CML, LHN, MDS, MM, Teratoma | Type: AT (walking, step), ST (elastic bands, bodyweight), Stretching, Wii sports, Wii fit program, Wii balance Duration:100 days Intensity: N/R Frequency: 5 days/week Supervised: yes Setting: hospital | T1-T2: - 2MWT: ↓ EXP/↓ CT (∆-1.7%; ∆-4.9%) - Treadmill: ↓ EXP/↓ CT (∆-13.2%; ∆-3.8%) - L HGS: ↓ EXP/↓ CT (∆-9.3%; ∆-8.1%) - ↔ Immune system |
| (Van Dongen et al., 2019) [53] | Multicenter RCT T1: Post HSCT (Baseline) T2: Post HSCT (After exersice or similar time point in the CT) T3: Post HSCT (12 months later) | - EXP: n = 54 (22 female), 52 ± 11 c years - CT: n = 55 (2 female), 53 ± 12 c years | HL, MM | Type: AT (stationary bicycle), ST (weight machines) Duration: 18 weeks Intensity and volume: AT 1–8 weeks twice a week (2 × 8 min, alternating 30 sg at 65% and 60 sg at 30% MSEC), 9–12 weeks twice a week (2 × 8 min, alternating 30 sg at 65% and 30 sg at 30% MSEC), 13–18 weeks once a week (2 × 8 min, alternating 30 s at 65% and 30 sg at 30% MSEC), ST: 1–12 weeks twice a week (2 sets of 10 reps at 65–80% of 1-RM), 13–18 weeks once a week (2 sets of 20 reps at 35–40% of 1-RM) Supervised: Yes Setting: Hospital | T1-T3: - No changes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales-Rodriguez, E.; Pérez-Bilbao, T.; San Juan, A.F.; Calvo, J.L. Effects of Exercise Programs on Physical Factors and Safety in Adult Patients with Cancer and Haematopoietic Stem Cell Transplantation: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 1288. https://doi.org/10.3390/ijerph19031288
Morales-Rodriguez E, Pérez-Bilbao T, San Juan AF, Calvo JL. Effects of Exercise Programs on Physical Factors and Safety in Adult Patients with Cancer and Haematopoietic Stem Cell Transplantation: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(3):1288. https://doi.org/10.3390/ijerph19031288
Chicago/Turabian StyleMorales-Rodriguez, Erica, Txomin Pérez-Bilbao, Alejandro F. San Juan, and Jorge Lorenzo Calvo. 2022. "Effects of Exercise Programs on Physical Factors and Safety in Adult Patients with Cancer and Haematopoietic Stem Cell Transplantation: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 3: 1288. https://doi.org/10.3390/ijerph19031288
APA StyleMorales-Rodriguez, E., Pérez-Bilbao, T., San Juan, A. F., & Calvo, J. L. (2022). Effects of Exercise Programs on Physical Factors and Safety in Adult Patients with Cancer and Haematopoietic Stem Cell Transplantation: A Systematic Review. International Journal of Environmental Research and Public Health, 19(3), 1288. https://doi.org/10.3390/ijerph19031288