Abstract
Increasingly popular, ultra-endurance participation exposes athletes to extremely high levels of functional and structural damage. Ultra-endurance athletes commonly develop acute kidney injury (AKI) and other pathologies harmful to kidney health. There is strong evidence that non-steroidal anti-inflammatory drugs, common amongst ultra-athletes, is linked to increased risk and severity of AKI and potentially ischaemic renal injury, i.e., acute tubular necrosis. Ultra-endurance participation also increases the risk of exertional rhabdomyolysis, exercise-associated hyponatremia, and gastrointestinal symptoms, interlinked pathologies all with potential to increase the risk of AKI. Hydration and fuelling both also play a role with the development of multiple pathologies and ultimately AKI, highlighting the need for individualised nutritional and hydration plans to promote athlete health. Faster athletes, supplementing nitrates, and being female also increase the risk of developing AKI in this setting. Serum creatinine criteria do not provide the best indicator for AKI for ultra-athletes therefore further investigations are needed to assess the practicality and accuracy of new renal biomarkers such as neutrophil gelatinase-associated lipocalin (NGAL). The potential of recurring episodes of AKI provide need for further research to assess the longitudinal renal health impact of ultra-participation to provide appropriate advice to athletes, coaches, medical staff, and event organisers.
1. Introduction
Since the turn of the millennium ultra-endurance events, defined by distance (>42.195 km for running), duration (>6 h or multiple days/stages), and environment (mountain, desert) [1,2] have increased in popularity [3,4]. As regular exercise including endurance and/or resistance is recommended to promote health benefits and prolong life [5], ultra-endurance athletes are considered to be healthy due to their increased cardiovascular fitness, commitment to high-volume training, and increased energy expenditure [6]. Preliminary evidence suggests repeated extremely strenuous exercise can promote increased mortality and reductions in health benefits in relation to increasing training dose endorsing a J- or U- shaped relationship [7,8]. Of interest to this review is the common development of acute kidney injury (AKI) post-ultra-endurance participation [1,4,7,9]. Although a consensus has not been reached regarding the true incidence of AKI for these athletes due to the multiple and inconsistent methods used [1,3,7].
Ultra-athletes are at increased risk of AKI, especially those participating in high volume and intensity ultra-running events, are exposed to high levels of functional and structural damage [2,4,7], increased serum creatinine (SCr) levels [8] and increasing renal filtration requirements [10]. The ingestion of non-steroidal anti-inflammatory drugs (NSAIDs), which is common in sports medicine [11,12,13] with up to 75% of ultra-athletes reporting NSAIDs use [14,15,16,17] is also a concern. NSAIDs are a contributing factor to ultra-endurance event completion success [16] as they assist in mitigating muscle inflammation, postpone fatigue, and improve pain tolerances [18,19,20]. High doses, equalling the maximal over-the-counter doses, can compromise training adaptations, reduce performance [12,21], increase the risk of AKI and accelerate progression of AKI to chronic kidney disease (CKD) [22]. Additionally, being of female sex, dehydration status [23,24], experiencing significant weight loss during races [25,26] and running faster over shorter durations [14,25] are associated with increased AKI risk for ultra-athletes.
Ultra-endurance events require prolonged extremely strenuous exercise while self-managing nutritional and hydrational status to facilitate optimal physical and mental performance [27]. Sub-optimal nutritional status in ultra-athletes is common and often requires participant withdrawal and/or medical intervention [27]. Conventionally, ultra-athletes do not prioritise protein [28] where nutrition and fuelling mainly focuses on carbohydrates [28,29]. In times of limited energy availability or insufficient protein ultra-events can incite muscle breakdown via inducing a catabolic state [30,31,32], which although uncommon can result in exertional rhabdomyolysis (ER) [4] which can induce kidney tubule damage and AKI [4,33]. Over-hydrating and intolerable fuelling regimes can result in exercise-associated hyponatremia (EAH) [34,35], gastro-intestinal symptoms (GIS) and endotoxemia [36,37] all of which can lead to kidney tubule damage and impaired kidney function.
AKI can be described as a sudden decrease in renal function which if prolonged can result in structural damage to renal tissues and impairment [38] but is mostly asymptomatic and reversible [39]. Increased blood levels of nitrogen waste products are characteristic of AKI [8] and changes SCr, blood urea, and cystatin-C (Cyst-C) levels are indicators of kidney function [40,41]. More novel and less used biomarkers reflecting renal tissue injury are neutrophil gelatinase-associated lipocalin (NGAL) and kidney injury molecule 1 (KIM-1) [33]. However, clinical AKI criteria, such as Risk, Injury, Failure, Loss, End-stage (RIFLE) and Kidney Disease Improving Global Guidelines (KDIGO) for AKI, are founded on changes observed to SCr levels and urine volume (Figure 1) [41,42]. Other structural and subclinical measures have been suggested but their use lacks consensus [43,44] while no established range of values exists for sport participation [4].

Figure 1.
Outline of 2 different criteria for acute kidney injury (AKI); Risk, Injury, Failure, Loss, End-stage (RIFLE) classification (left) and the clinical practice guidelines published by Kidney Disease Improving Global Guidelines (KDIGO) for acute kidney injury (right).
2. Materials and Methods
An online literature search was conducted utilising three online electronic databases, Google Scholar, PubMed, and ScienceDirect. The design of this review was narrative however, the search strategy and parameters closely followed the PRISMA statement guidelines [45]. The key search terms included, ‘kidney injury’, ‘acute kidney injury’, ‘kidney dysfunction’, ‘impaired kidney function’, and ‘ultra-endurance’, combined to produce search phrases such as, ‘acute kidney injury and ultra-endurance’. To promote a current and relevant review, papers were not included if published prior to 2000, non-peer-reviewed, or written in a language other than English. Those that were reviewed met the following inclusion criteria; ultra-endurance athlete population and included estimates or measures of renal function. Relevant articles published prior to 2000 found in reference lists of reviewed articles were also included or discussed throughout this review.
This search identified 22 articles, briefly outlined in Table 1 (full table of review, Table S1, Supplementary Material), 17 were prospective observational cohort studies [23,25,26,39,40,43,46,47,48,49,50,51,52,53,54,55,56], the remainder comprised of 3 retrospective cases series [34,35,57], and 2 individual case reports [3,58]. This resulted in 445 ultra-athletes meeting the at-risk AKI criteria and 281 meeting the injury AKI criteria. One case of acute tubular necrosis (ATN) was reported. Other conditions were reported alongside renal dysfunction including 43 cases of exertional rhabdomyolysis (ER) in six studies, 30 occurred alongside AKI diagnosis. 21 cases of exercise-associated hyponatremia (EAH) were reported in three studies, 7 occurred alongside AKI diagnosis while another 8 occurred concurrently with both ER and AKI.

Table 1.
Overview of studies examining the occurrence of AKI, Exertional rhabdomyolysis, and Exercise-associated Hyponatremia in ultra-endurance athletes.
3. Acute Kidney Injury and Ultra-Endurance Events
Acute kidney injury (AKI) in ultra-endurance events has been frequently reported [1], however, the prevalence of AKI in ultra-endurance athletes has not reached a consensus ranging from 0% [47,59] up to 85% [26]. Differing and inconsistent methodologies relying on changes to serum creatinine (SCr) levels, in addition to observing different modalities of ultra-events for measuring the impact on kidney function during ultra-endurance likely explains variances [3,56]. Recently 96.2% of AKI cases that also occurred in conjunction with exertional rhabdomyolysis (ER) were linked to ultra-running events [2]. The majority of studies in this review (Table 1) pertained to ultra-running events however 3 studies included ultra-cycling participants [53,54,56]. The serum creatinine (SCr) levels for all the participants observed by Chlibkova et al. (2015) in both ultra-mountain bike and ultra-running races increased, however there was a significant increase in post-race SCr for 24 h ultra-running athletes compared to those competing in 24 h mountain biking events (p < 0.01). It should be noted that very few ultra-athletes seek or need medical intervention in the presence of an AKI diagnosis [56,60].
Multiple factors effect SCr levels as seen in Figure 2. Endogenous creatine production occurs within the liver and kidneys (Figure 2) from glycine, methionine, and arginine which is subsequently transported to skeletal, cardiac muscles and other tissues [61] where the non-enzymatic anhydration of creatine results in creatinine [62,63]. High protein diets including cooked meats provide an additional creatine source (Figure 2). Renal elimination of serum creatine occurs via glomerular filtration and low, yet unpredictable levels of tubular secretion, which is affected by multiple drugs, while small gastrointestinal losses also occur [62,63] (Figure 2).
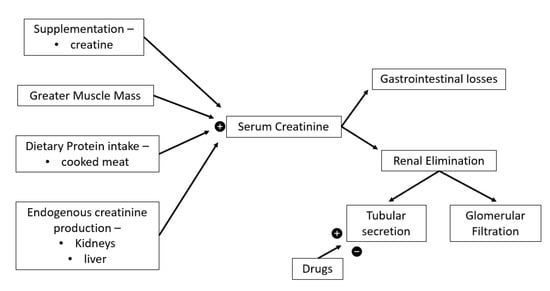
Figure 2.
Serum creatinine determinants. = increase,
= increase,  = decrease.
= decrease.
= increase, = decrease.
Creatinine clearance is a useful indicator of GFR though overestimates it by around 10% compared the gold standard inulin clearance [62]. Measuring creatinine clearance requires prolonged and impractical urine collection in addition to blood sampling [62], in clinical practice GFR is usually estimated using equations based on SCr modified by sex, age and ethnicity to provide some degree of correction for differences in creatinine generation [64]. SCr GFR equations were generated using the general population or hospitalised patients [65,66] and assume creatinine generation is steady state, not always true (Figure 2), especially during or after extreme exercise [62,64], as significant increases in SCr levels are common post ultra-events (Table 1). Severe muscle damage is common during ultra-endurance events [4] therefore increases in SCr levels can reflect muscle damage rather than reductions in GFR [8,52]. Using SCr as an indicator of renal function produces inaccurate reflections of the impact of exercise on kidney function [67] and may lead to overdiagnosis of AKI in ultra-athletes. Poussel et al. (2020) found using creatinine produced an overestimation of AKI prevalence compared to use the cystatin C. Additionally, the normal GFR for ultra-endurance athletes is unknown due to a lack of baseline data [68] and back-calculating estimates of baseline SCr for ultra-athletes has been shown to be inaccurate [43,68]. Hence, avoiding SCr in settings of extreme exercise has been recommended [8]. This highlights the importance of pre-race testing, participant screening, and the need for a more accurate and valid method for monitoring renal function for this population.
More accurate biomarkers of renal dysfunction are required which can identify abnormal kidney function and discriminate between intrinsic renal disease and prerenal azotaemia which is often induced by strenuous exercise [8]. As there are 3 groups of AKI biomarkers: indicators of renal function (low molecular weight proteins such as Cystatin C) [69], indicators of tubular damage (urinary neutrophil gelatinase-associated lipocalin (NGAL) and urinary kidney injury molecule-1 (KIM-1)) [8] and renal inflammatory mediators (leukocytes and prostaglandins) [70]. Cystatin C (Cyst-C) has less non-GFR determinants, being unrelated to muscle mass or diet, compared to SCr [69,71,72] and has been recommended in populations with increased muscle mass or extreme diets [73]. Over the marathon distance, the rise in Cyst-C was equal to half that of the increase in SCr, supporting that Cyst-C is less affected by sport related renal blood flow changes or muscle damage [74]. Mccullough et al., (2011) found that there was a comparable rise and normalisation for both SCr and Cyst-C after marathon running. Additionally, this study found a 5-fold increase in NGAL and a lesser increase in KIM-1 measures supporting a real decrease in renal function due to renal tissue injury [33]. As an 25 kDa acute phase protein, NGAL is mainly produced in the kidney tubules [8,47,48], is a key indicator of early ischemic damage to the kidneys [75,76,77,78] and early detection of AKI and predicting renal disease progression [48,59,75,76]. NGAL levels have been shown to significantly increase during then returned to baseline within 24 h [8] or continued to increase post ultra-race [33] indicating that tubular injury was present independent of changes to SCr. The minimal increase in urinary neutrophil gelatinase-associated lipocalin (NGAL) and urinary kidney injury molecule-1 (KIM-1) levels in another study also argues against the diagnosis of AKI using criteria based on increased SCr [47]. Therefore, future studies should compare the sensitivity of available biomarkers while also meetings the practical needs of medical professionals present at ultra-endurance events.
4. Non-Steroidal Anti-Inflammatory Drugs
Five studies reported AKI alongside positive use of NSAIDs for ultra-athletes (Table 1). In only one study was use of NSAIDs denied by ultra-athletes [46], whilst the remaining 16 studies did not specify whether there was use of NSAIDs by their participants. NSAIDs inhibits cyclo-oxygenase production thus preventing the synthesis of prostaglandins resulting in increased renal vasodilation and decreasing homeostasis [25,77] (Figure 3). Exercise reduces renal blood flow, however renal perfusion is augmented, and homeostasis maintained via vasodilatory prostaglandins [78]. The absence of prostaglandins and the subsequent reduced renal perfusion results in reduced GFR contributing to mild increases in renal function markers and ultimately, occasionally, kidney failure [67,79]. For healthy individuals, prostaglandin stimulated vasodilation is unnecessary for maintenance of renal function [78], while those with renal disease requires prostaglandin driven vasodilation of renal vascular beds to maintain renal perfusion [80] and avoid renal ischemic injury [78].

Figure 3.
Multiple pathologies and mechanisms promoting acute kidney injury (AKI) in ultra-endurance athletes. Non-steroidal anti-inflammortory drugs (NSAIDs), glomerular filtration rate (GFR), exertional rhabdomyolysis (ER), myoglobin (MB), serum creatine kinase (S-CK), arginine vasopressin (AVP), exercise-associated hyponatremia (EAH),  = increase,
= increase,  = decrease.
= decrease.
= increase, = decrease.
Compared to marathon (42 km) and trail runners (67 km), ultramarathon runners (112 km) had the highest per-event NSAIDs intake indicating that the duration of the event plays a role in the quantity and chronological consumption of NSAIDS in ultra-events [17]. Although NSAIDs have been found to be a significant risk factor for AKI after endurance events, some debate exists regarding whether NSAIDs induce a reduced renal function in ultra-athletes. Wharam et al., (2006) found that NSAIDs significantly increase SCr compared to non-NSAIDs users. More recently, Lipman et al., (2014) showed a 18% increase in overall AKI incidence and severity for NSAIDs users, as 12% more ultra-athletes met the AKI at-risk criteria and 6% more met the injury criteria (Figure 1) [14]. Poussel and colleagues found that observing only non-NSAIDs user ultra-athletes reduced the incidence of AKI compared to other ultra-athlete studies [59]. However, contrary evidence exists as both Dumke et al. (2007) and Page et al. (2007) found no significant difference in SCr levels between NSAID using and non-using ultra-runners, though both sample sizes were small, the NSAIDs doses subtherapeutic, and the studies were unblinded.
In the 11 case reports systematically reviewed by Hodgson et al. (2017) investigating the concern of severe AKI after various marathon and ultramarathon events, 22 of 27 cases of severe AKI in ultra-athletes required hospitalisation, 18 (67%) reported NSAIDs use. In the studies discussed in this review (Table 1) no renal biopsies were completed, although 1 case of acute tubular necrosis (ATN) was made from urinalysis, serology, and ultrasound results [58]. However, in studies reviewed by Hodgson et al., (2015), 4 kidney biopsies were completed, all revealing ATN for both marathon and ultramarathon distance events, suggesting an ischaemic aetiological link in developing AKI and ATN for endurance athletes using NSAIDs [8]. NSAIDs have also been linked to the development of EAH and ER in ultra-athletes which may also contribute to subsequent AKI and hospitalisation [34,60]. Ultra-athletes should approach the consumption of NSAIDs with caution and pay closer attention the potential negative health outcome, especially the development of AKI and ATN rather than performance benefits.
5. Hydration
Ultra-endurance events occur across the world and expose athletes to a multitude of different and fluctuating environmental conditions including hot, humid, tropical conditions [4,26,34,35,81]. Physical exertion in these ambient conditions often promotes kidney damage and ultra-athletes often experience inadequate hydration status [39,81,82]. Altered kidney function is promoted due to combinations of dehydration, high internal and external metabolic loads, and heat strain [24,83]. Severe dehydration is widely recognized as a contributor to AKI after endurance exercise and other life-threatening consequences [23,24]. Increased loss of electrolytes and water via increased sweating can also cause hyponatremia [34,56]. While adequate hydration status maintenance does not prevent ER in ultra-athletes [26], dehydration induced reduction of renal blood flow and renal ischemia resulting in an accumulation of muscle proteins within a reduced total blood volume can increase the risk AKI [84,85] and ER [86,87] for ultra-athletes (Figure 3).
Loss of body mass does not directly translate into an absolute measure of dehydration however it is a simple method of assessing hydration status during exercise [88]. Previous studies have found that limiting the body exercise induced weight loss to ~2–3% is necessary to avoid dehydration while maintaining or improving performance [89,90,91]. The average body weight loss for ultra-marathon runners was ~5%, reaching >11% of body weight in some cases [26,92]. Water can be produced during exercise via a combination of the utilisation of endogenous and exogenous substrates and the release of glycogen bound water through glycogenolysis [91] assisting in alleviating dehydration [93]. Therefore, maintaining euhydration requires at least ~2–5% reduction in body mass during ultra-events [91], which seems to be tolerated by ultra-athletes [94]. Belli et al., (2018) found that athletes who presented with body mass reductions >5% (−5.2 to −10.4%) also presented with >25% (−27.1 to −44.4%) reduced GFR from 84 km to the completion of the 200 km event. Similarly, a greater reduction in body mass from 120 km was linked to greater renal dysfunction for ultra-athletes during multi-stage 250 km desert races [25]. Hence, complying with typical hydration guidelines and avoiding a 2% mass loss [30,95], can result in hyperhydration of ultra-athletes [82], increases the risk of developing symptomatic EAH [96], and increased levels of cytokinemia and bacterial endotoxemia and subsequent increased AKI risk [97]. Dehydration is most likely to occur during the early stages of ultra-events as the first 4 h showed the maximum slope of weight loss [25,26,46]. However, an increased total percentage body mass loss resulted in a higher proportion of subjects meeting RIFLE criteria for AKI compared to those with less mass loss [39,57] and therefore needs further investigation.
6. Exertional Rhabdomyolysis
Exertional rhabdomyolysis (ER) is a pathophysiological condition described by damage to or necrosis of the striated muscle tissues during strenuous exercise leading muscle cell disintegration enabling the release of myoglobin (Mb) into the bloodstream and extracellular space [98]. Additionally, sarcoplasmic proteins such as S-CK, serum lactate dehydrogenase (S-LDH), aspartate transaminase (AST) and electrolytes are released [99]. In extreme cases of muscle necrosis, ER symptoms can present as weakness, oedema, myalgia, and reddish-brown or tea coloured urine, without haematuria [34]. Six papers were found discussing exertional rhabdomyolysis in ultra-endurance events resulting in 43 cases (Table 1). Of these, 30 cases of AKI occurred either alongside or potentially due to exertional rhabdomyolysis (ER).
Serum Mb can potentially result in kidney failure via 3 mechanisms: tubular obstruction, toxic reaction, and decreased oxygen supply due to vasoconstriction of renal tissues [60,87] (Figure 3). Mb is quickly eliminated from the bloodstream, so S-CK is the preferred marker for ER identification [23] which shows a peak 24–36 h post-exercise with recovery to baseline values at 48–72 h post-exercise [100,101,102]. In ER, Mb and S-CK, can rise ≥4–5 times and sometimes much greater, above normal values, while S-LDH and AST generally only double [103]. A recent systematic review recommended that S-CK > 1000 UI/L as an essential criterion for the diagnosis of ER diagnosis [104].
With an incidence of ~29.9 per 100,000 patient years, ER is relatively uncommon [105] however the concurrent complication of AKI which is significantly more common is a concern for ultra-athletes [86]. Hodgson et al. (2017) reported 27 cases of AKI across varying endurance disciplines (six in ultra-endurance athletes), with concurrent rhabdomyolysis in 23 cases (85%). Not surprisingly ER can lead to several other serious conditions, hyperkalaemia, hypernatremia, acidosis kidney tubule damage and the development of acute and chronic renal injuries [4]. ER due to heat stress and AKI has been reported, indicating that dehydration, hyperthermia, and eccentric muscle loads can promote and contribute to the development of ER + AKI [23,39]. As ultra-endurance events are often held in areas with hot and humid conditions for example the tropics, these conditions can increase the risk of ER [26,34,87]. It has been shown that increasingly prolonged exercise under these thermally challenging conditions can induce increased severity of both ER and AKI [4].
7. Exercise-Associated Hyponatremia
Exercise-associated hyponatremia (EAH) was initially reported in ultra-endurance athletes and is a potentially serious condition [106,107]. Symptomatic EAH is caused by fluid overload from continued over-drinking [77,108]. Previous and outdated recommendations to drink as much as possible during exercise [109] resulted in increased occurrences of EAH within athletes [110,111,112]. Blood testing is needed to identify asymptomatic EAH [77], however EAH can present with symptoms such as, vomiting, dyspnoea, changes to consciousness, and convulsions related to hyponatraemic encephalopathy [112]. Hyponatraemic death has been reported post ultra-endurance events [77,107]. Three studies were found to discuss EAH in the presence of AKI for ultra-endurance athletes. A total of 21 cases of EAH were found, 7 of which occurred alongside AKI while 8 cases occurred concurrently with both AKI and ER (Table 1).
Asymptomatic and symptomatic EAH is identified by a low blood sodium concentration (Na+ < 135 mmol/L) during or immediately post exercise [107]. Severe hyponatraemia produces water influx into the cells leading to cellular swelling, muscle cell membranes destabilisation, and ultimately traumatic cell rupture during exercise [35,113]. Increased muscle cell fragility can promote the breakdown of muscle tissues, ER, and the subsequent AKI [35,113] (Figure 3). Muscle cell lysis due to strenuous exercise [113,114] or increased thermal strain [115] can result in the third spacing of fluids which in turn can stimulate the secretion of arginine vasopressin (AVP) which facilitates the development of EAH [34]. AVP can be stimulated by pain, emotion, exercise, nausea, heat stress, hypoglycaemia, medications (NSAIDs) [107,116,117], and elevated inflammatory cytokines all of which have been found in ultra-athletes [118]. Over-drinking beyond the feelings of thirst in conjunction with non-osmotic AVP secretion induced by protracted endurance exercise results in fluid retention and EAH [119].
The impact of increased sodium loss via increased sweating on the development of EAH is still controversial [107]. Endurance athletes compared to the general population have reduced levels of sweat sodium, however sweat sodium loss is extremely variable for individuals [120]. An increase in serum sodium would be expected through loss of hypotonic sweat in opposition to EAH, although sweat loss may lead to EAH via fluid loss induced volume depletion stimulating AVP and increased water retention or the ingestion of greatly more hypotonic fluids compared to fluid loss, potentially promoting a net weight loss [107,121]. The link between EAH and ER may be casual or independent [34,103]. Renal function fluctuations can also play a part in the development of EAH, as prolonged oliguria and anuria can result in dilutional hyponatremia and further increase renal compromise [122]. It has been reported that hyponatraemic athletes are more likely to develop ER compared to normonatraemic athletes [123]. ER and EAH may be aetiological factors for the development of either condition [107]. However, each condition requires opposing treatments [34,107], mild EAH requires water restriction protocols while severe EAH need intravenous concentrated bolus of hypertonic saline [107]. ER requires aggressive intravenous isotonic fluids to limit the myoglobin build-up within the renal tissues and AKI [113]. Highlighting the importance of individualised hydration strategies to alleviate risk of EAH and increased awareness of the different treatments needed for opposing conditions.
8. Gastrointestinal Dysfunction
Ultra-endurance events require prolonged extremely strenuous exercise while also self-managing nutritional and hydrational status to facilitate optimal physical and mental performance [27]. Sub-optimal nutritional status in ultra-athletes is common and often requires participant withdrawal and/or medical intervention [27]. Gastrointestinal symptoms (GIS) are common in ultra-endurance events with an incidence of 60–93% for both severe upper and lower GIS plus acute abdominal pain, dizziness, and nausea [124,125,126,127]. GIS are linked with hindered capability to meet nutritional and energy demands, poor performance and withdrawal [16,124]. This highlights the need for effective fuelling, hydration, and nutritional strategies for optimal ultra- performance and athlete safety [27]. Ingestion of carbohydrate (CHO) during ultra-endurance events improves performance [128,129]. Indeed, ultra-athlete’s nutrition and fuelling strategies during events mainly focuses on carbohydrates (CHO) [28]. CHO account for ≥70% total daily energy intake equating to >10 gCHO/kg/day [130,131]. However, during extended strenuous exercise, to avoid malabsorption and GIS, fuelling needs to account for the total CHO oxidative capabilities of muscles in the context of individual gastrointestinal tolerance [132].
Blood redistribution away from central organs (gut, liver, and kidneys) to active muscles (oxygen and substrate supply) and skin (heat dissipation) occurs during extended strenuous exercise [31,125]. Depending on exercise intensity, the renal blood flow can be reduced to ~25% of resting values while GFR is maintained [133] and splanchnic blood flow is reduced to ~20% of resting values [134]. Severe gut under perfusion can cause shock-induced mucosal damage, releasing Gram-negative intestinal bacteria and/or endotoxins like lipo-polysaccharides (LPS) which can leak into central circulation if portal clearance is overwhelmed [36,37,135] resulting in endotoxemia [15,31,125,135]. Impaired renal function is commonly reported due endotoxemia [136]. Symptoms such as fever, shivering, dizziness, nausea may occur along with GIS including vomiting and diarrhoea, and finally sepsis [31,135,137]. In vivo, LPS are key activation molecules for the host immune response by inciting the cytokine network during exercise [15,125]. Endotoxins can enter the circulation post-ultra-endurance participation via increased gastrointestinal permeability resulting from splanchnic ischemia, which worsens in the presence of hyperthermia and muscle damage [15,31,125]. Intense exercise can result in immune suppression allowing increasing LPS concentrations exceeding systemic inflammatory response thresholds [138]. Ultimately, disseminated intravascular coagulation, multi-organ failure, and central nervous system disturbances may occur in heat stroke victims [37]. Significantly, endotoxemia has been reported mainly when intense exercise was performed in warm not cool conditions [37,139]. Individual exercise-induced increases in cytokine levels vary considerably and are further increased by NSAIDs consumption [15]. Physiological responses to endotoxins require LPS binding proteins, which can induce a pro-inflammatory response increasing tubular apoptosis and renal function impairment [36,37]. Avoiding GIS via establishing individual gastrointestinal tolerances and fuelling strategies could reduce the risk of developing sub-nutritional status and potentially reduce the risk of AKI for ultra-athletes.
9. Beetroot/Nitrates
Medically, dietary nitrates are used to treat conditions such as hypertension and cardiovascular disease [140]. The findings of a pivotal study [141] showing that increased dietary nitrates was associated with a decrease in oxygen cost during submaximal exercise. This significantly increased the popularity of nitrates in endurance athletes [28]. Beetroots and beetroot juice, exemplify several vegetables that provide high levels of inorganic nitrate (NO3-) [28] which is ultimately converted to nitric oxide (NO) within the gut [142,143]. Numerous body systems important for endurance exercise performance are affected by NO consumption for example, oxygen regulation in working muscles, blood flow, vasodilation, mitochondrial respiration and biogenesis, overall muscle contractions and relaxation, and glucose uptake [140,142,144]. Cumulatively, this results in improved endurance performance [145].
Nitrate clearance within humans is relatively unknown however it does pass easily through the glomerulus and is mostly reabsorbed at the proximal tubules [143]. Ingestion of 3.5 mmol nitrate was completely removed within 48 h in humans, of which 60% was excreted via the urine [146]. The rate of excretion of urinary nitrates has been used to monitor endogenous NO synthesis in several diseases [147,148,149]. Although this assumes that altered renal function has no effect on renal nitrate excretion or other non-renal pathways, although evidence suggests that fractional excretion of nitrates falls as renal function declines [143]. NO is a gaseous signalling molecule and conditional on its concentration, release location and period of action, has several functions within the kidney [150]. Reductions or absence of a specific isoform of NO synthase production can indicate renal endothelial damage post ischemia-reperfusion [150,151], which is the most common cause of acute tubular necrosis AKI [149].
Although nitrates are fairly non-toxic, high doses of their metabolites (e.g., nitrite, nitric oxide, and N-nitroso compounds) pose an increased concern over potentially promoting carcinogenesis [152]. An increased risk of kidney cell carcinoma has been reported when exposed to excessive amounts of nitrate and nitric oxide [153,154,155]. Dietary nitrate converted into nitrite has the potential to interreact with dietary amines, forming carcinogenic nitrosamines [156]. Nitrate supplementation during resting and submaximal endurance elicited normal kidney function responses to exercise compared to placebo [157]. Post-exercise recovery (60 min) was slightly reduced in the nitrate supplementation group, where the glomerular membrane permeability remained increased compared to the placebo, no longer term effect was reported [157]. It remains those ultra-athletes should be cautious when considering or using uncontrolled quantities of nitrate supplements [156].
10. Females
Female athletes are often excluded in studies due to menstrual cycle phases which may confuse physiological results [1]. Female gender is underrepresented compared to males in studies in Table 1 though this is a known risk factor for developing AKI in ultra-athletes [25]. Female athletes are up to 4 times more likely to develop AKI than males, which is similar to and may in part be due to the increased risk of developing EAH in females [158,159]. Bruso et al. (2010) speculated that the lack of women reported who developed EAH and rhabdomyolysis and the subsequent AKI in this paper was due to the numbers of female finishers, ratio (1:5) of females to males, respectively. Nevertheless, EAH and ER have been reported in women [160]. The true mechanisms for this increased risk and association of EAH and AKI in females needs further study [25]. A study including ~50% female participants, suggested that females were unable to rehydrate during endurance exercise as well as males [161].
Female ultra-athletes also struggle meeting the increased daily caloric requirements of ultra-training and competition due to the interaction of sex-hormones and energy availability [1]. High training volumes and/or periods of calorie intake restriction can occur in ultra-athletes causing impairment of physiological functions, known as the syndrome of relative energy deficiency in sport (RED-S) [162]. Both male and female athletes can experience the detrimental effects of a low energy availability, however female athletes feel the effects more rapidly and to a greater extent due to the Female Triad a relationship between menstrual cycle fluctuations and bone health [163]. Additionally, the high training mileage and low bone density associated with oestrogen deficiency can increase the risk of bone fractures for females [1]. The incorporation of females and the increased risk of AKI may potentially skew results or overestimate the true prevalence/risk of AKI for the whole ultra-endurance population, in which males make up the majority of participants [77].
11. Hormones
Ultra-endurance participation promotes stress indicated by changes in the hypothalamic-pituitary-testicular (HPT) axis shown by decreased testosterone, luteinizing hormone, and sex hormone-binding globulin levels, while increased cortisol levels and reductions in testosterone: cortisol ratio indicates a catabolic state [84,98,164]. Ultra-marathon running activates both the coagulation and fibrinolytic systems in male and female runners which significantly increases stress on kidney function [165].
Increased cortisol levels immediately post ultra-endurance events is a key marker of stress experienced by athletes [84,98,166]. Kupchak et al. (2014) showed greater cortisol concentrations increase (4.3-fold) after a 161 km trail run than in previous reports over marathon running [167,168], Ironman triathlon [166], and ultramarathon finishers [169]. Multiple factors could be the cause for this greater increase in cortisol such as the increased duration [170], quantity of time in eccentric downhill running and changes in altitude [46], variable temperature conditions [170,171] and experience of energy deficiency [172]. The intensity of ultra-marathon performance has also been linked to higher cortisol levels corresponding with athletes with higher running speeds [173]. Cortisol provides an immunosuppressive effect, assists in increasing blood glucose levels and the metabolism of fats and proteins [98] and increased serum cortisol level is protective against injury [174]. The increased levels of cortisol could provide a protective factor against renal injury during ultra-endurance events.
12. Ultra-Endurance Performance
Within non-athletes, the occurrence of AKI is an indicator of increased susceptibility to future AKI events and the development of CKD [57]. Mild AKI insults are common in ultra-endurance athletes, therefore the suggestion that recurring participation could result in an increased risk of developing future AKI and/or increasing the severity of the subsequent insult [57,84]. Although, assessing AKI via clinical criteria suggests that up to 82% of ultra-endurance athletes may be affected, these characteristics tend to resolve within 24 h post finish [6,14,23,33]. Renal chemistries observed post 56 km ultra-marathon showed a full recovery overnight [52], while kidney function often recovers to baseline between stages of multi-stage ultra-events [39]. Experiencing reduced renal function during an ultra-endurance event or due to participation in multiple events currently shows no negative cumulative effects and does not lead to any apparent future renal function restrictions [39,51,57]. However, clinical AKI criteria have been established during resting conditions of clinical populations, utilising this for ultra-endurance populations may lead to an overestimation of AKI and an inappropriate method for ultra-endurance athletes [41].
Ultra-athletes should be aware that shorter and faster ultra-marathons have greater likelihood of causing reductions in kidney function than longer and slower events [14,23,25,40,57,84]. Originally, an increased AKI incidence was reported for marathons runners, up to 84% of participants meeting AKI criteria [6,10,33], where the main differences between marathon and ultra-marathons runners are that the latter run at much slower speeds and have increased training hours and kilometres [85,175]. Within an ultra-endurance cohort, the slowest finishers were found to be less likely to develop AKI [14,25], compared to the top 10 fastest finishers, the AKI risk was decreased up to 82% in slower finishers [25]. A greater percentage of those with increased blood measures indicating AKI were among the faster finishers [57]. Faster finishers are also at increased risk of increased severity of AKI with more athletes meeting stage 2 criteria (Figure 1) than slower finishers [23]. Several factors could contribute to this increased risk, such as when assessing the speed variability during 100 km ultra-marathon suggested that glycogen depletion related fatigue at 40th–50th km when running ~65% VO2max may play a part in increasing AKI risk [40]. Additionally, the longer exposure time of slower athletes provides more hydration opportunities potentially attenuating the risk of renal injury due to dehydration [25]. Lower myoglobin levels have also been reported for slower finishers, which suggests a reduced renal damage due to myoglobinemia [176], however this was not reflected in a previous study [177]. Ultra-athletes should consider the health risk of competing in shorter, faster paced events, while more research is needed to provide a clearer understanding if repeated participation imparts increased risk of recurrent AKI, increased severity and/or the progression to CKD.
13. Future Considerations
Ultra-endurance events expose athletes to various extreme weather conditions due to remote locations and large distances covered by athletes, which hinders the accuracy of athlete health and safety monitoring by event and medical staff [1]. Using modern technologies, GPS tracking, or heart rate monitors can provide continued participant monitoring (training and competitive intensities, volumes, and recovery) and earlier identification of potentially serious adverse events [7]. Mandatory pre-event screening using an agreed, accurate, and appropriate method of measuring renal function for ultra-athletes should be conducted identify those at increased risk of renal dysfunction [8].
The use of new and more accurate biomarkers of renal function, Cyst-C, NGAL and/or KIM-1, can provide athlete teams, event organisers, medical staff, and researchers with increased quality and accuracy of data reflecting real race settings and longitudinal observational opportunities [1,4,8]. However, the remote nature of ultra-events means that practicality of medical assessment tools is vital. Of interest, Hoffman et al. (2013) collected post-race blood and urine samples were collected for 150 ultra-athletes where the urine dipstick tests showed a trace of protein in 76%, 3+ haemolysed blood in 62%, and measurable ketones were found in 39% of results. This study found that urine dipstick results inclusive of at least 1+ protein, 3+ blood, and specific gravity ≤ 1.025 identified participants meeting AKI ‘injury’ criteria with a sensitivity of 1.0 and specificity of 0.76. Blood creatine kinase concentrations in those meeting AKI criteria was higher than those at AKI risk and creatine kinase levels > 20,000 U/L was deemed an acceptable threshold to provide treatment preventing kidney failure due to rhabdomyolysis [60]. These finding suggest that simple dipstick urinalysis may offer a rapid and inexpensive method to evaluate susceptibility for AKI post ultra-endurance event. For medical support this information is key, as ultra-athletes are exposed to various combinations of dehydration, exertional rhabdomyolysis, and exercise-associated hyponatremia (EAH) some of which require rapid potentially opposing treatment protocols [34,107,113].
14. Conclusions
There is strong evidence that NSAIDs use is linked with increased risk of AKI and the progression of renal impairment to CKD for the general population, the common practise of NSAIDs consumption for ultra-endurance athletes is concerning and more research is needed to identify the longitudinal impact on ultra-athlete’s kidney health. Ultra-endurance athletes are also at increased risk of developing multiple different and interlinked pathologies such as ER, EAH, and GIS, which all have the potential to increase risk of developing AKI. Hydration and fuelling seem to play a role in the development of multiple pathologies as well as AKI, therefore individualised nutritional and hydration plans are key for athlete health. Further research is required to assess the longitudinal renal health impact of ultra-participation and to identify the most appropriate and accurate biomarkers and method of measuring renal function for ultra-athletes to enable the provision of suitable advice to athletes, coaches, event organisers, and medical staff.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph192416887/s1, Table S1: Overview of studies examining the occurrence of AKI, Exertional rhabdomyolysis, and Exercise-associated Hyponatremia in ultra-endurance athletes.
Author Contributions
Conceptualization, V.T., J.B., L.B., D.M., T.D., J.H., S.S. and K.F.; writing—original draft preparation V.T.; writing—review editing V.T., J.B., L.B., D.M., T.D., J.H., S.S. and K.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Scheer, V.; Tiller, N.B.; Doutreleau, S.; Khodaee, M.; Knechtle, B.; Pasternak, A.; Rojas-Valverde, D. Potential Long-Term Health Problems Associated with Ultra-Endurance Running: A Narrative Review. Sport Med. 2021, 52, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Rubio-arias, J.Á.; Ávila-Gandía, V.; López-román, F.J.; Soto-méndez, F.; Alcaraz, P.E.; Ramos-campo, D.J. Muscle damage and inflammation biomarkers after two ultra-endurance mountain races of different distances: 54 km vs 111 km. Physiol. Behav. 2019, 205, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Lecina, M.; López, I.; Castellar, C.; Pradas, F. Extreme ultra-trail race induces muscular damage, risk for acute kidney injury and hyponatremia: A case report. Int. J. Environ. Res. Public Health 2021, 18, 11323. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Valverde, D.; Sánchez-Ureña, B.; Crowe, J.; Timón, R.; Olcina, G.J. Exertional rhabdomyolysis and acute kidney injury in endurance sports: A systematic review. Eur. J. Sport Sci. 2021, 21, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Riebe, D.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.; Pescatello, L.S. Updating ACSM’s recommendations for exercise preparticipation health screening. Med. Sci. Sport. Exerc. 2015, 47, 2473–2479. [Google Scholar] [CrossRef] [PubMed]
- Mansour, S.; Verma, G.; Pata, R.; Martin, T.; Perazella, M.; Parikh, C. Kidney Injury and Repair Biomarkers in Marathon Runners. Am. J. Kidney Dis. 2017, 70, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Scheer, V.; Rojas-Valverde, D. Long-term health issues in ultraendurance runners: Should we be concerned? BMJ Open Sport Exerc. Med. 2021, 7, e001131. [Google Scholar] [CrossRef]
- Hodgson, L.E.; Walter, E.; Venn, R.M.; Galloway, R.; Pitsiladis, Y.; Sardat, F.; Forni, L.G. Acute kidney injury associated with endurance events—Is it a cause for concern? A systematic review. BMJ Open Sport Exerc. Med. 2017, 3, e000093. [Google Scholar] [CrossRef]
- Rojas-Valverde, D.; Olcina, G.; Sánchez-Ureña, B.; Pino-Ortega, J.; Martínez-Guardado, I.; Timón, R. Proteinuria and bilirubinuria as potential risk indicators of acute kidney injury during running in outpatient settings. Medicina 2020, 56, 562. [Google Scholar] [CrossRef]
- Hewing, B.; Schattke, S.; Spethmann, S.; Sanad, W.; Schroeckh, S.; Schimke, I.; Halleck, F.; Peters, H.; Brechtel, L.; Lock, J.; et al. Cardiac and renal function in a large cohort of amateur marathon runners. Cardiovasc. Ultrasound 2015, 13, 13. [Google Scholar] [CrossRef][Green Version]
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.A.; Lilja, M.; Mandić, M.; Gustafsson, T.; Larsen, F.J.; Lundberg, T.R. Resistance training with co-ingestion of anti-inflammatory drugs attenuates mitochondrial function. Front. Physiol. 2017, 8, 1074. [Google Scholar] [CrossRef] [PubMed]
- Omeragic, E.; Marjanovic, A.; Djedjibegovic, J.; Turalic, A.; Dedic, M.; Niksic, H.; Lugusic, A.; Sober, M. Prevalence of use of permitted pharmacological substances for recovery among athletes. Pharmacia 2021, 68, 35–42. [Google Scholar] [CrossRef]
- Lipman, G.S.; Shea, K.; Christensen, M.; Phillips, C.; Burns, P.; Higbee, R.; Koskenoja, V.; Eifling, K.; Krabak, B.J. Ibuprofen versus placebo effect on acute kidney injury in ultramarathons: A randomised controlled trial. Emerg. Med. J. 2017, 34, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C.; Henson, D.A.; Dumke, C.L.; Oley, K.; McAnulty, S.R.; Davis, J.M.; Murphy, E.A.; Utter, A.C.; Lind, R.H.; McAnulty, L.S.; et al. Ibuprofen use, endotoxemia, inflammation, and plasma cytokines during ultramarathon competition. Brain Behav. Immun. 2006, 20, 578–584. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Fogard, K. Factors related to successful completion of a 161-km ultramarathon. Int. J. Sports Physiol. Perform. 2011, 6, 25–37. [Google Scholar] [CrossRef]
- Martínez, S.; Aguiló, A.; Moreno, C.; Lozano, L.; Tauler, P. Use of non-steroidal anti-inflammatory drugs among participants in a mountain ultramarathon event. Sports 2017, 5, 11. [Google Scholar] [CrossRef]
- Gorski, T.; Cadore, E.L.; Pinto, S.S.; da Silva, E.M.; Correa, C.S.; Beltrami, F.G.; Kruel, L.M. Use of NSAIDs in triathletes: Prevalence, level of awareness and reasons for use. Br. J. Sports Med. 2011, 45, 85–90. [Google Scholar] [CrossRef]
- Steckling, F.M.; Lima, F.D.; Farinha, J.B.; Rosa, P.C.; Royes, L.F.F.; Cuevas, M.J.; Bresciani, G.; Soares, F.A.; González-Gallego, J.; Barcelos, R.P. Diclofenac attenuates inflammation through TLR4 pathway and improves exercise performance after exhaustive swimming. Scand. J. Med. Sci. Sports 2020, 30, 264–271. [Google Scholar] [CrossRef]
- Lundberg, T.R.; Howatson, G. Analgesic and anti-inflammatory drugs in sports: Implications for exercise performance and training adaptations. Scand. J. Med. Sci. Sports 2018, 28, 2252–2262. [Google Scholar] [CrossRef]
- Lilja, M.; Mandić, M.; Apró, W.; Melin, M.; Olsson, K.; Rosenborg, S.; Gustafsson, T.; Lundberg, T.R. High doses of anti-inflammatory drugs compromise muscle strength and hypertrophic adaptations to resistance training in young adults. Acta Physiol. 2018, 222, e12948. [Google Scholar] [CrossRef] [PubMed]
- Nderitu, P.; Doos, L.; Jones, P.W.; Davies, S.J.; Kadam, U.T. Non-steroidal anti-inflammatory drugs and chronic kidney disease progression: A systematic review. Fam. Pract. 2013, 30, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.K.; Chiu, Y.H.; Tsai, Y.F.; Tai, L.C.; Hou, P.C.; How, C.K.; Yang, C.C.; Kao, W.F. Clinical impact of speed variability to identify ultramarathon runners at risk for acute kidney injury. PLoS ONE 2015, 10, e0133146. [Google Scholar] [CrossRef] [PubMed]
- Bongers, C.C.; Alsady, M.; Nijenhuis, T.; Tulp, A.D.; Eijsvogels, T.M.; Deen, P.M.; Hopman, M.T. Impact of acute versus prolonged exercise and dehydration on kidney function and injury. Physiol. Rep. 2018, 6, e13734. [Google Scholar] [CrossRef]
- Lipman, G.S.; Krabak, B.J.; Rundell, S.D.; Shea, K.M.; Badowski, N.; Little, C. Incidence and prevalence of acute kidney injury during multistage ultramarathons. Clin. J. Sport Med. 2016, 26, 314–319. [Google Scholar] [CrossRef]
- Kao, W.F.; Hou, S.K.; Chiu, Y.H.; Chou, S.L.; Kuo, F.C.; Wang, S.H.; Chen, J.J. Effects of 100-km ultramarathon on acute kidney injury. Clin. J. Sport Med. 2015, 25, 49–54. [Google Scholar] [CrossRef]
- Costa, R.J.S.; Hoffman, M.D.; Stellingwerff, T. Research in Sports Medicine Considerations for ultra-endurance activities: Part 1- nutrition. Res. Sport Med. 2019, 27, 166–181. [Google Scholar] [CrossRef]
- Vitale, K.; Getzin, A. Nutrition and supplement update for the endurance athlete: Review and recommendations. Nutrients 2019, 11, 1289. [Google Scholar] [CrossRef]
- Nikolaidis, P.T.; Veniamakis, E.; Rosemann, T.; Knechtle, B. Nutrition in ultra-endurance: State of the art. Nutrients 2018, 10, 1995. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Jentjens, R.L.P.G.; Moseley, L. Nutritional considerations in triathlon. Sport Med. 2005, 35, 163–181. [Google Scholar] [CrossRef] [PubMed]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International society of sports nutrition position stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A.; Chinnaiyan, K.M.; Gallagher, M.J.; Colar, J.M.; Geddes, T.; Gold, J.M.; Trivax, J.E. Changes in renal markers and acute kidney injury after marathon running. Nephrology 2011, 16, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Bruso, J.R.; Hoffman, M.D.; Rogers, I.R.; Lee, L.; Towle, G.; Hew-butler, T. Rhabdomyolysis and hyponatremia: A cluster of five cases at the 161-km 2009 Western States Endurance Run. Wilderness Environ. Med. 2010, 21, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Boulter, J.; Noakes, T.D.; Hew-Butler, T. Acute renal failure in four Comrades Marathon runners ingesting the same electrolyte supplement: Coincidence or causation? S. Afr. Med. J. 2011, 101, 876–878. [Google Scholar]
- Stasi, A.; Intini, A.; Divella, C.; Franzin, R.; Montemurno, E.; Grandaliano, G.; Ronco, C.; Fiaccadori, E.; Pertosa, G.B.; Gesualdo, L.; et al. Emerging role of Lipopolysaccharide binding protein in sepsis-induced acute kidney injury. Nephrol. Dial. Transplant. 2017, 32, 24–31. [Google Scholar] [CrossRef]
- Lim, C.L.; Suzuki, K. Systemic inflammation mediates the effects of endotoxemia in the mechanisms of heat stroke. Biol. Med. 2016, 9, 1. [Google Scholar] [CrossRef]
- Makris, K.; Spanou, L. Acute kidney injury: Definition, pathophysiology and clinical phenotypes. Clin. Biochem. Rev. 2016, 37, 85–98. [Google Scholar]
- Lipman, G.S.; Krabak, B.J.; Waite, B.L.; Logan, S.B.; Menon, A.; Chan, G.K. A prospective cohort study of acute kidney injury in multi-day ultramarathon runners. Wilderness Environ. Med. 2014, 22, 358. [Google Scholar] [CrossRef]
- Shin, K.; Park, K.D.; Ahn, J.; Park, Y.; Kim, Y.-J. Comparison of changes in biochemical markers for skeletal muscles, hepatic metabolism, and renal function after three types of long-distance running: Observational study. Medicine 2016, 95, e3657. [Google Scholar] [CrossRef]
- Lopes, J.A.; Jorge, S. The RIFLE and AKIN classifications for acute kidney injury: A critical and comprehensive review. Clin. Kidney J. 2013, 6, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron. Clin. Pract. 2012, 120, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Khodaee, M.; Irion, B.; Spittler, J.; Saeedi, A.; Hoffman, M.D. Characteristics of runners meeting acute kidney injury criteria following a 161-km ultramarathon. Transl. Sport Med. 2021, 4, 733–740. [Google Scholar] [CrossRef]
- Rojas-Valverde, D.; Martínez-Guardado, I.; Sánchez-Ureña, B.; Timón, R.; Scheer, V.; Pino-Ortega, J.; Olcina, G. Outpatient assessment of mechanical load, heat strain and dehydration as causes of transitional acute kidney injury in endurance trail runners. Int. J. Environ. Res. Public Health 2021, 18, 10217. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Belli, T.; Macedo, D.V.; De Araujo, G.G.; Dos Reis, I.G.M.; Scariot, P.P.M.; Lazarim, F.L.; Nunes, L.A.S.; Brenzikofer, R.; Gobatto, C.A. Mountain ultramarathon induces early increases of muscle damage, inflammation, and risk for acute renal injury. Front. Physiol. 2018, 9, 1368. [Google Scholar] [CrossRef]
- Jouffroy, R.; Lebreton, X.; Mansencal, N.; Anglicheau, D. Acute kidney injury during an ultra-distance race. PLoS ONE 2019, 14, e0222544. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-gomar, F.; Salvagno, G.L.; Aloe, R.; Schena, F.; Guidi, G.C. Variation of serum and urinary neutrophil gelatinase associated lipocalin (NGAL) after strenuous physical exercise. Clin. Chem. Lab. Med. 2012, 50, 1585–1589. [Google Scholar] [CrossRef]
- Noakes, T.D.; Carter, J. Biochemical parameters in athletes before and after having run 160 kilometres. S. Afr. Med. J. 1976, 50, 1562–1566. [Google Scholar]
- Irving, R.A.; Noakes, T.D.; Smit, R.V.Z. Metabolic and renal changes in two athletes during a world 24 hour relay record performance. Br. J. Sports Med. 1989, 23, 227–232. [Google Scholar] [CrossRef]
- Irving, R.A.; Noakes, T.D.; Raine, R.I.; Van Zyl Smit, R. Transient oliguria with renal tubular dysfunction after a 90 km running race. Med. Sci. Sports Exerc. 1990, 22, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Irving, R.A.; Noakes, T.D.; Burger, S.C.; Myburgh, K.H.; Querido, D.; van Zyl Smit, R. Plasma volume and renal function during and after ultramarathon running. Med. Sci. Sports Exerc. 1990, 22, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Neumayr, G.; Pfister, R.; Hoertnagl, H.; Mitterbauer, G.; Getzner, W.; Ulmer, H.; Gaenzer, H.; Joannidis, M. The effect of marathon cycling on renal function. Int. J. Sports Med. 2003, 24, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Neumayr, G.; Pfister, R.; Hoertnagl, H.; Mitterbauer, G.; Prokop, W.; Joannidis, M. Renal function and plasma volume following ultramarathon cycling. Int. J. Sports Med. 2005, 26, 2–8. [Google Scholar] [CrossRef]
- Christensen, D.L.; Espino, D.; Infante-Ramírez, R.; Brage, S.; Terzic, D.; Goetze, J.P.; Kjaergaard, J. Normalization of elevated cardiac, kidney, and hemolysis plasma markers within 48 h in Mexican Tarahumara runners following a 78 km race at moderate altitude. Am. J. Hum. Biol. 2014, 26, 836–843. [Google Scholar] [CrossRef]
- Chlíbková, D.; Knechtle, B.; Rosemann, T.; Tomášková, I.; Novotný, J.; Žákovská, A.; Uher, T. Rhabdomyolysis and exercise-associated hyponatremia in ultra-bikers and ultra-runners. J. Int. Soc. Sports Nutr. 2015, 12, 29. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Weiss, R.H. Does acute kidney injury from an ultramarathon increase the risk for greater subsequent injury? Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2016, 26, 417–422. [Google Scholar] [CrossRef]
- Zyl-smit RVan Mills, P.; Vogelpoel, L. Unrecognised acute renal failure following the comrades marathon. S. Afr. Med. J. 2000, 90, 39–40. [Google Scholar]
- Poussel, M.; Touzé, C.; Allado, E.; Frimat, L.; Hily, O.; Thilly, N.; Rousseau, H.; Vauthier, J.C.; Chenuel, B. Ultramarathon and renal function: Does exercise-induced acute kidney injury really exist in common conditions? Front. Sport Act Living 2020, 1, 71. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Stuempfle, K.J.; Fogard, K.; Hew-butler, T.; Winger, J.; Weiss, R.H. Urine dipstick analysis for identification of runners susceptible to acute kidney injury following an ultramarathon. J. Sports Sci. 2013, 31, 20–31. [Google Scholar] [CrossRef]
- Andres, S.; Ziegenhagen, R.; Trefflich, I.; Pevny, S.; Schultrich, K.; Braun, H.; Schänzer, W.; Hirsch-Ernst, K.I.; Schäfer, B.; Lampen, A. Creatine and creatine forms intended for sports nutrition. Mol. Nutr. Food Res. 2017, 61, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Kashani, K.; Rosner, M.H.; Ostermann, M. Creatinine: From physiology to clinical application. Eur. J. Int. Med. 2020, 72, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Delanaye, P.; Cavalier, E.; Pottel, H. Serum creatinine: Not so simple! Nephron 2017, 136, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Inker, L.A. Assessment of glomerular filtration rate in health and disease: A state of the art review. Clin. Pharmacol. Ther. 2017, 102, 405–419. [Google Scholar] [CrossRef]
- Botev, R.; Mallié, J.P.; Wetzels, J.F.; Couchoud, C.; Schück, O. The clinician and estimation of glomerular filtration rate by creatinine-based formulas: Current limitations and quo vadis. Clin. J. Am. Soc. Nephrol. 2011, 6, 937–950. [Google Scholar] [CrossRef]
- Kork, F.; Balzer, F.; Krannich, A.; Bernardi, M.H.; Eltzschig, H.K.; Jankowski, J.; Spies, C. Back-calculating baseline creatinine overestimates prevalence of acute kidney injury with poor sensitivity. Acta Physiol. 2017, 219, 615–626. [Google Scholar] [CrossRef]
- Poortmans, J.R.; Gulbis, B.; De Bruyn, E.; Baudry, S.; Carpentier, A. Limitations of serum values to estimate glomerular filtration rate during exercise. Br. J. Sports Med. 2013, 47, 1166–1170. [Google Scholar] [CrossRef]
- Little, C.E.; Lipman, G.S.; Migliaccio, D.; Young, D.S.; Krabak, B.J. Accuracy of estimated creatinine in multistage ultramarathon runners. Wilderness Environ. Med. 2019, 30, 129–133. [Google Scholar] [CrossRef]
- Dharnidharka, V.R.; Kwon, C.; Stevens, G. Serum cystatin C is superior to serum creatinine as a marker of kidney function: A meta-analysis. Am. J. Kidney Dis. 2002, 40, 221–226. [Google Scholar] [CrossRef]
- Rabb, H.; Griffin, M.D.; McKay, D.B.; Swaminathan, S.; Pickkers, P.; Rosner, M.H.; Kellum, J.A.; Ronco, C. Inflammation in AKI: Current understanding, key questions, and knowledge gaps. J. Am. Soc. Nephrol. 2016, 27, 371–379. [Google Scholar] [CrossRef]
- Tangri, N.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Beck, G.J.; Greene, T.; Coresh, J.; Levey, A.S. Changes in dietary protein intake has no effect on serum cystatin C levels independent of the glomerular filtration rate. Kidney Int. 2011, 79, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2022, 313, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Mingels, A.; Jacobs, L.; Kleijnen, V.; Wodzig, W.; van Dieijen-Visser, M. Cystatin C a marker for renal function after exercise. Int. J. Sports Med. 2009, 30, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.R.; Parikh, C.R. Biomarkers of acute and chronic kidney disease. Annu. Rev. Physiol. 2019, 81, 309–333. [Google Scholar] [CrossRef]
- Mishra, J.; Dent, C.; Tarabishi, R.; Mitsnefes, M.M.; Ma, Q.; Kelly, C.; Ruff, S.M.; Zahedi, K.; Shao, M.; Bean, J.; et al. Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. Lancet 2005, 365, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Wharam, P.C.; Speedy, D.B.; Noakes, T.D.; Thompson, J.M.D.; Reid, S.A.; Holtzhausen, L.-M. NSAID use increases the risk of developing hyponatremia during an Ironman triathlon. Med. Sci. Sports Exerc. 2006, 38, 618–622. [Google Scholar] [CrossRef]
- Whelton, A. Nephrotoxicity of nonsteroidal anti-inflammatory drugs: Physiologic foundations and clinical implications. Am. J. Med. 1999, 106, 13S–24S. [Google Scholar] [CrossRef]
- Murray, M.D.; Brater, D.C. Renal toxicity of the nonsteroidal anti-inflammatory drugs. Annu. Rev. Pharmacol. Toxicol. 1993, 33, 435–465. [Google Scholar] [CrossRef]
- Miller, S.B. Prostaglandins in health and disease: An overview. In Seminars in Arthritis and Rheumatism; WB Saunders: Philadelphia, PA, USA, 2006; Volume 36, pp. 37–49. [Google Scholar] [CrossRef]
- Shimizu, Y.; Takaori, K.; Maeda, S. Exercise-induced acute renal failure in a trainee cyclist without hypouricemia: Successful athletic career post-treatment. J. Gen. Fam. Med. 2017, 18, 432–435. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Stellingwerff, T.; Costa, R.J. Considerations for ultra-endurance activities: Part 2—Hydration. Res. Sport Med. 2019, 27, 182–194. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Valverde, D.; Sánchez-Ureña, B.; Pino-Ortega, J.; Gómez-Carmona, C.; Gutiérrez-Vargas, R.; Timón, R.; Olcina, G. External workload indicators of muscle and kidney mechanical injury in endurance trail running. Int. J. Environ. Res. Public Health 2019, 16, 3909. [Google Scholar] [CrossRef] [PubMed]
- Knechtle, B.; Nikolaidis, P.T. Physiology and pathophysiology in ultra-marathon running. Front. Physiol. 2018, 9, 634. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, P.M. Exertional rhabdomyolysis and acute renal failure in marathon runners. Sport Med. 2007, 37, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, J.; Kim, S.; Young, H.; Suk, K. Exercise-induced rhabdomyolysis mechanisms and prevention: A literature review. J. Sport Health Sci. 2016, 5, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Asserraji, M.; Benameur, I.; Maoujoud, O.; El Kharras, A.; Hajbi, H.; Filali, K. Late care in marathon runs leading to exertional heat stroke with multiple organ failure. Asian J. Sports Med. 2014, 5, 136–138. [Google Scholar]
- Armstrong, L.E. Assessing hydration status: The elusive gold standard. J. Am. Coll. Nutr. 2007, 26, 575–584. [Google Scholar] [CrossRef]
- Goulet, E.D.B. Dehydration and endurance performance in competitive athletes. Nutr. Rev. 2012, 70, S132–S136. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Carter, R.; Sawka, M.N. Fluid balance and endurance exercise performance. Curr. Sports Med. Rep. 2003, 2, 202–208. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Goulet, E.D.; Maughan, R.J. Considerations in the use of body mass change to estimate change in hydration status during a 161-kilometer ultramarathon running competition. Sport Med. 2018, 48, 243–250. [Google Scholar] [CrossRef]
- Kao, W.F.; Shyu, C.L.; Yang, X.W.; Hsu, T.F.; Chen, J.J.; Kao, W.C.; Huang, Y.J.; Kuo, F.C.; Huang, C.I.; Lee, C.H. Athletic performance and serial weight changes during 12-and 24-hour ultra-marathons. Clin. J. Sport Med. 2008, 18, 155–158. [Google Scholar] [CrossRef] [PubMed]
- King, R.F.G.J.; Jones, B.; Hara, J.P.O. The availability of water associated with glycogen during dehydration: A reservoir or raindrop? Eur. J. Appl. Physiol. 2018, 118, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.D.; Pasternak, A.; Rogers, I.R.; Khodaee, M.; Hill, J.C.; Townes, D.A.; Scheer, B.V.; Krabak, B.J.; Basset, P.; Lipman, G.S. Medical services at ultra-endurance foot races in remote environments: Medical issues and consensus guidelines. Sport Med. 2014, 44, 1055–1069. [Google Scholar] [CrossRef] [PubMed]
- McDermott, B.P.; Anderson, S.A.; Armstrong, L.E.; Casa, D.J.; Cheuvront, S.N.; Cooper, L.; Kenney, W.L.; O’Connor, F.G.; Roberts, W.O. National athletic trainers’ association position statement: Fluid replacement for the physically active. J. Athl. Train. 2017, 52, 877–895. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.D.; Stuempfle, K.J.; Sullivan, K.; Weiss, R.H. Exercise-associated hyponatremia with exertional rhabdomyolysis: Importance of proper treatment. Clin. Nephrol. 2015, 83, 235–242. [Google Scholar] [CrossRef]
- Gill, S.K.; Hankey, J.; Wright, A.; Marczak, S.; Hemming, K.; Allerton, D.M.; Ansley-Robson, P.; Costa, R.J.S. The impact of a 24-h ultra-marathon on circulatory endotoxin and cytokine profile. Int. J. Sports Med. 2015, 36, 688–695. [Google Scholar] [CrossRef]
- Kupchak, B.R.; Kraemer, W.J.; Hoffman, M.D.; Phinney, S.D.; Volek, J.S. The impact of an ultramarathon on hormonal and biochemical parameters in men. Wilderness Environ. Med. 2014, 25, 278–288. [Google Scholar] [CrossRef]
- Mcvane, B.A.; Andreae, M.C.; Fernando, D.B.; Strayer, R.J. Exertional rhabdomyolysis in a long-distance migrant. J. Emerg. Med. 2019, 56, 551–553. [Google Scholar] [CrossRef]
- Atias-Varon, D.; Sherman, H.; Yanovich, R.; Heled, Y. Rhabdomyolysis after crawling military training. Mil. Med. 2017, 182, e1948–e1952. [Google Scholar] [CrossRef]
- Kim, D.; Ko, E.J.; Cho, H.; Park, S.H.; Lee, S.H.; Cho, N.G.; Lee, S.Y.; Jeong, H.Y.; Yang, D.H. Spinning-induced rhabdomyolysis: Eleven case reports and review of the literature. Electrolytes Blood Press. 2015, 13, 58–61. [Google Scholar] [CrossRef][Green Version]
- Oh, R.C.; Arter, J.L.; Tiglao, S.M.; Larson, S.L. Exertional rhabdomyolysis: A case series of 30 hospitalized patients. Mil. Med. 2015, 180, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical markers of muscular damage. Clin. Chem. Lab. Med. 2010, 48, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Stahl, K.; Rastelli, E.; Schoser, B. A systematic review on the definition of rhabdomyolysis. J. Neurol. 2020, 267, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Tietze, D.C.; Borchers, J. Exertional rhabdomyolysis in the athlete: A clinical review. Sports Health 2014, 6, 336–339. [Google Scholar] [CrossRef] [PubMed]
- Noakes, T.D.; Goodwin, N.; Rayner, B.L.; Branken, T.; Taylor, R.K. Water Intoxication: A possible complication during endurance exercise. Wilderness Environ. Med. 2005, 16, 221–227. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Loi, V.; Pani, A.; Rosner, M.H. Exercise-associated hyponatremia: 2017 update. Front. Med. 2017, 4, 21. [Google Scholar] [CrossRef]
- Noakes, T. Hyponatremia in distance runners: Fluid and sodium balance during exercise. Curr. Sports Med. Rep. 2002, 1, 197–207. [Google Scholar] [CrossRef]
- Convertino, V.A.; Armstrong, L.E.; Coyle, E.F.; Mack, G.W.; Sawka, M.N.; Senay Jr, L.C.; Sherman, W.M. American College of Sports Medicine. Position Stand. Exercise and fluid replacement. Med. Sci. Sports Exerc. 1996, 28, i–ix. [Google Scholar] [CrossRef]
- Noakes, T.D.; Sharwood, K.; Collins, M.; Perkins, D.R. The dipsomania of great distance: Water intoxication in an Ironman triathlete. Br. J. Sports Med. 2004, 38, e16. [Google Scholar] [CrossRef]
- Sharwood, K.A.; Collins, M.; Goedecke, J.H.; Wilson, G.; Noakes, T.D. Weight changes, medical complications, and performance during an Ironman triathlon. Br. J. Sports Med. 2004, 38, 718–724. [Google Scholar] [CrossRef]
- Speedy, D.B.; Rogers, I.; Safih, S.; Foley, B. Hyponatremia and seizures in an ultradistance triathlete. J. Emerg. Med. 2000, 18, 41–44. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Ayus, J.C.; Kipps, C.; Maughan, R.J.; Mettler, S.; Meeuwisse, W.H.; Page, A.J.; Reid, S.A.; Rehrer, N.J.; Roberts, W.O.; et al. Statement of the second international exercise-associated hyponatremia consensus development conference, New Zealand, 2007. Clin. J. Sport Med. 2008, 18, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, P.M.; Kearns, A.K.; Rouzier, P.; Rubin, R.; Thompson, P.D. Serum creatine kinase levels and renal function measures in exertional muscle damage. Med. Sci. Sports Exerc. 2006, 38, 623. [Google Scholar] [CrossRef] [PubMed]
- Chorley, J.; Cianca, J.; Divine, J. Risk factors for exercise-associated hyponatremia in non-elite marathon runners. Clin. J. Sport Med. 2007, 17, 471–477. [Google Scholar] [CrossRef]
- Freund, B.J.; Shizuru, E.M.; Hashiro, G.M.; Claybaugh, J.R. Hormonal, electrolyte, and renal responses to exercise are intensity dependent. J. Appl. Physiol. 1991, 70, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Takamata, A.K.I.R.A.; Mack, G.W.; Stachenfeld, N.S.; Nadel, E.R. Body temperature modification of osmotically induced vasopressin secretion and thirst in humans. Am. J. Physiol. Integr. Comp. Physiol. 1995, 269, R874–R880. [Google Scholar] [CrossRef]
- Cairns, R.S.; Hew-Butler, T. Incidence of exercise-associated hyponatremia and its association with nonosmotic stimuli of arginine vasopressin in the GNW100s ultra-endurance marathon. Clin. J. Sport Med. 2015, 25, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Hew-Butler, T.; Rosner, M.H.; Fowkes-Godek, S.; Dugas, J.P.; Hoffman, M.D.; Lewis, D.P.; Maughan, R.J.; Miller, K.C.; Montain, S.J.; Rehrer, N.J.; et al. Statement of the third international exercise-associated hyponatremia consensus development conference, Carlsbad, California, 2015. Clin. J. Sport Med. 2015, 25, 303–320. [Google Scholar] [CrossRef] [PubMed]
- Buono, M.J.; Sjoholm, N.T. Effect of physical training on peripheral sweat production. J. Appl. Physiol. 1988, 65, 811–814. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Jordaan, E.; Stuempfle, K.J.; Speedy, D.B.; Siegel, A.J.; Noakes, T.D.; Soldin, S.J.; Verbalis, J.G. Osmotic and nonosmotic regulation of arginine vasopressin during prolonged endurance exercise. J. Clin. Endocrinol. Metab. 2008, 93, 2072–2078. [Google Scholar] [CrossRef]
- Verbalis, J.G.; Goldsmith, S.R.; Greenberg, A.; Schrier, R.W.; Sterns, R.H. Hyponatremia treatment guidelines 2007: Expert panel recommendations. Am. J. Med. 2007, 120, S1–S21. [Google Scholar] [CrossRef] [PubMed]
- Chlíbková, D.; Rosemann, T.; Posch, L.; Matoušek, R.; Knechtle, B. Pre-and post-race hydration status in hyponatremic and non-hyponatremic ultra-endurance athletes. Chin. J. Physiol. 2016, 59, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.J.S.; Snipe, R.; Camões-Costa, V.; Scheer, V.; Murray, A. The impact of gastrointestinal symptoms and dermatological injuries on nutritional intake and hydration status during ultramarathon events. Sport Med. Open 2016, 2, 16. [Google Scholar] [CrossRef] [PubMed]
- Jeukendrup, A.E.; Vet-Joop, K.; Sturk, A.; Stegen, J.H.J.C.; Senden, J.; Saris, W.H.M.; Wagenmakers, A.J.M. Relationship between gastro-intestinal complaints and endotoxaemia, cytokine release and the acute-phase reaction during and after a long-distance triathlon in highly trained men. Clin. Sci. 2000, 98, 47–55. [Google Scholar] [CrossRef]
- Stuempfle, K.J.; Hoffman, M.D. Gastrointestinal distress is common during a 161-km ultramarathon. J. Sports Sci. 2015, 33, 1814–1821. [Google Scholar] [CrossRef] [PubMed]
- Stuempfle, K.J.; Hoffman, M.D.; Hew-Butler, T. Association of gastrointestinal distress in ultramarathoners with race diet. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 103–109. [Google Scholar] [CrossRef]
- Jeukendrup, A.E. Nutrition for endurance sports: Marathon, triathlon, and road cycling. J. Sports Sci. 2011, 29, 91–99. [Google Scholar] [CrossRef]
- Stellingwerff, T.; Cox, G.R. Systematic review: Carbohydrate supplementation on exercise performance or capacity of varying durations. Appl. Physiol. Nutr. Metab. 2014, 39, 998–1011. [Google Scholar] [CrossRef]
- Fudge, B.W.; Westerterp, K.R.; Kiplamai, F.K.; Onywera, V.O.; Boit, M.K.; Kayser, B.; Pitsiladis, Y.P. Evidence of negative energy balance using doubly labelled water in elite Kenyan endurance runners prior to competition. Br. J. Nutr. 2006, 95, 59–66. [Google Scholar] [CrossRef]
- Onywera, V.O.; Kiplamai, F.K.; Tuitoek, P.J.; Boit, M.K.; Pitsiladis, Y.P. Food and macronutrient intake of elite Kenyan distance runners. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 709–719. [Google Scholar] [CrossRef]
- Costa, R.J.; Miall, A.; Khoo, A.; Rauch, C.; Snipe, R.; Camões-Costa, V.; Gibson, P. Gut-training: The impact of two weeks repetitive gut-challenge during exercise on gastrointestinal status, glucose availability, fuel kinetics, and running performance. Appl. Physiol. Nutr. Metab. 2017, 42, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Poortmans, J.R. Exercise and renal function. Exerc. Sport Sci. Rev. 1977, 5, 255–294. [Google Scholar] [CrossRef] [PubMed]
- Clausen, J.P. Effect of physical training on cardiovascular adjustments to exercise in man. Physiol. Rev. 1977, 57, 779–815. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Yeh, W.; Ohashi, P.S. LPS/TLR4 signal transduction pathway. Cytokine 2008, 42, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Anders, H.J.; Banas, B.; Schlöndorff, D. Signaling danger: Toll-like receptors and their potential roles in kidney disease. J. Am. Soc. Nephrol. 2004, 15, 854–867. [Google Scholar] [CrossRef] [PubMed]
- Dauphinee, S.M.; Karsan, A. Lipopolysaccharide signaling in endothelial cells. Lab. Investig. 2006, 86, 9–22. [Google Scholar] [CrossRef]
- Lim, C.L.; Mackinnon, L.T. The roles of exercise-induced immune system disturbances in the pathology of heat stroke—The dual pathway model of heat stroke. Sport Med. 2006, 36, 39–64. [Google Scholar] [CrossRef]
- Selkirk, G.A.; Mclellan, T.M.; Wright, H.E.; Rhind, S.G. Mild endotoxemia, NF-κB translocation, and cytokine increase during exertional heat stress in trained and untrained individuals. Am. J. Physiol. Integr. Comp. Physiol. 2008, 295, 611–623. [Google Scholar] [CrossRef]
- Shaltout, H.A.; Eggebeen, J.; Marsh, A.P.; Brubaker, P.H.; Laurienti, P.J.; Burdette, J.H.; Basu, S.; Morgan, A.; Dos Santos, P.C.; Norris, J.L.; et al. Effects of supervised exercise and dietary nitrate in older adults with controlled hypertension and/or heart failure with preserved ejection fraction. Nitric. Oxide 2017, 69, 78–90. [Google Scholar] [CrossRef]
- Larsen, F.J.; Weitzberg, E.; Lundberg, J.O.; Ekblom, B. Effects of dietary nitrate on oxygen cost during exercise. Acta Physiol. 2007, 191, 59–66. [Google Scholar] [CrossRef]
- Domínguez, R.; Cuenca, E.; Maté-Muñoz, J.L.; García-Fernández, P.; Serra-Paya, N.; Estevan, M.C.L.; Herreros, P.V.; Garnacho-Castaño, M.V. Effects of beetroot juice supplementation on cardiorespiratory endurance in athletes. A systematic review. Nutrients 2017, 9, 43. [Google Scholar] [CrossRef]
- Williams, J.K.; Smallwood, M.J.; Benjamin, N.; D’Souza, R.J.; Shore, A.C.; Winyard, P.G.; Gilchrist, M. Renal nitrate clearance in chronic kidney disease. Nitric. Oxide 2020, 97, 16–19. [Google Scholar] [CrossRef]
- McMahon, N.F.; Leveritt, M.D.; Pavey, T.G. The effect of dietary nitrate supplementation on endurance exercise performance in healthy adults: A systematic review and meta-analysis. Sport Med. 2017, 47, 735–756. [Google Scholar] [CrossRef]
- Ravindra, P.V.; Janhavi, P.; Divyashree, S.; Muthukumar, S.P. Nutritional interventions for improving the endurance performance in athletes. Arch. Physiol. Biochem. 2020, 128, 851–858. [Google Scholar] [CrossRef]
- Wagner, D.A.; Schultz, D.S.; Deen, W.M.; Young, V.R.; Tannenbaum, S.R. Metabolic fate of an oral dose of 15N-labeled nitrate in humans: Effect of diet supplementation with ascorbic acid. Cancer Res. 1983, 43, 1921–1925. [Google Scholar] [PubMed]
- Sagnella, G.A.; Markandu, N.D.; Onipinla, A.K.; Chelliah, R.; Singer, D.R.J.; Macgregor, G.A. Plasma and urinary nitrate in essential hypertension. J. Hum. Hypertens. 1997, 11, 587–588. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dykhuizen, R.S.; Copland, M.; Smith, C.C.; Douglas, G.; Benjamin, N. Plasma nitrate concentration and urinary nitrate excretion in patients with gastroenteritis. J. Infect. 1995, 31, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Mian, A.I.; Du, Y.; Garg, H.K.; Caviness, A.C.; Goldstein, S.L.; Bryan, N.S. Urinary nitrate might be an early biomarker for pediatric acute kidney injury in the emergency department. Pediatr. Res. 2011, 70, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Goligorsky, M.S.; Brodsky, S.V.; Noiri, E. Nitric oxide in acute renal failure: NOS versus NOS. Kidney Int. 2002, 61, 855–861. [Google Scholar] [CrossRef]
- Kwon, O.; Hong, S.; Ramesh, G. Diminished NO generation by injured endothelium and loss of macula densa nNOS may contribute to sustained acute kidney injury after ischemia-reperfusion. Am. J. Physiol. Physiol. 2009, 296, 25–33. [Google Scholar] [CrossRef]
- Poortmans, J.R.; Gualano, B.; Carpentier, A. Nitrate supplementation and human exercise performance: Too much of a good thing? Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 599–604. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Nitrate in vegetables-Scientific Opinion of the Panel on Contaminants in the Food chain. EFSA J. 2008, 6, 689. [Google Scholar] [CrossRef]
- Calvert, J.W.; Lefer, D.J. Role of β-adrenergic receptors and nitric oxide signaling in exercise-mediated cardioprotection. Physiology 2013, 28, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.H.; Rusiecki, J.A.; Lynch, C.F.; Cantor, K.P. Nitrate in public water supplies and the risk of renal cell carcinoma. Cancer Causes Control 2007, 18, 1141–1151. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, J.O.; Larsen, F.J.; Weitzberg, E. Supplementation with nitrate and nitrite salts in exercise: A word of caution. J. Appl. Physiol. 2011, 111, 616–617. [Google Scholar] [CrossRef]
- Carpentier, A.; Stragier, S.; Bréjeon, C.; Poortmans, J.R. Nitrate supplementation, exercise, and kidney function: Are there detrimental effects? Med. Sci. Sports Exerc. 2015, 47, 1519–1522. [Google Scholar] [CrossRef]
- Zouhal, H.; Groussard, C.; Minter, G.; Vincent, S.; Cretual, A.; Gratas-Delamarche, A.; Delamarche, P.; Noakes, T.D. Inverse relationship between percentage body weight change and finishing time in 643 forty-two-kilometre marathon runners. Br. J. Sports Med. 2011, 45, 1101–1105. [Google Scholar] [CrossRef]
- Chlíbková, D.; Knechtle, B.; Rosemann, T.; Žákovská, A.; Tomášková, I.; Shortall, M.; Tomášková, I. Changes in foot volume, body composition, and hydration status in male and female 24-hour ultra-mountain bikers. J. Int. Soc. Sports Nutr. 2014, 11, 18–21. [Google Scholar] [CrossRef]
- Glace, A.B.; Murphy, C. Severe hyponatremia develops in a runner following a half-marathon. J. Am. Acad PAs. 2008, 21, 27–29. [Google Scholar] [CrossRef]
- Atkins, W.C.; Butts, C.L.; Kelly, M.R.; Troyanos, C.; Laursen, R.M.; Duckett, A.; Emerson, D.M.; Rosa-Caldwell, M.E.; McDermott, B.P. Acute Kidney Injury Biomarkers and Hydration Outcomes at the Boston Marathon. Front. Physiol. 2022, 12, 2402. [Google Scholar] [CrossRef]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.; Meyer, N.; et al. International Olympic Committee (IOC) consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 316–331. [Google Scholar] [CrossRef] [PubMed]
- Beals, K.A.; Meyer, N.L. Female athlete triad update. Clin. Sports Med. 2007, 26, 69–89. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Fragala, M.S.; Watson, G.; Volek, J.S.; Rubin, M.R.; French, D.N.; Maresh, C.M.; Vingren, J.L.; Hatfield, D.L.; Spiering, B.A.; et al. Hormonal responses to a 160-km race across frozen Alaska. Br. J. Sports Med. 2008, 42, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Kupchak, B.R.; Volk, B.M.; Kunces, L.J.; Kraemer, W.J.; Hoffman, M.D.; Phinney, S.D.; Volek, J.S. Alterations in coagulatory and fibrinolytic systems following an ultra-marathon. Eur. J. Appl. Physiol. 2013, 113, 2705–2712. [Google Scholar] [CrossRef]
- Neubauer, O.; König, D.; Wagner, K.H. Recovery after an Ironman triathlon: Sustained inflammatory responses and muscular stress. Eur. J. Appl. Physiol. 2008, 104, 417–426. [Google Scholar] [CrossRef]
- Karkoulias, K.; Habeos, I.; Charokopos, N.; Tsiamita, M.; Mazarakis, A.; Pouli, A.; Spiropoulos, K. Hormonal responses to marathon running in non-elite athletes. Eur. J. Int. Med. 2008, 19, 598–601. [Google Scholar] [CrossRef]
- Semple, C.G.; Thomson, J.A.; Beastall, G.H. Endocrine responses to marathon running. Br. J. Sports Med. 1985, 19, 148–151. [Google Scholar] [CrossRef]
- Roupas, N.D.; Mamali, I.; Maragkos, S.; Leonidou, L.; Armeni, A.K.; Markantes, G.K.; Tsekouras, A.; Sakellaropoulos, G.C.; Markou, K.B.; Georgopoulos, N.A. The effect of prolonged aerobic exercise on serum adipokine levels during an ultra-marathon endurance race. Hormones 2013, 12, 275–282. [Google Scholar] [CrossRef]
- Hartley, L.H.; Mason, J.W.; Hogan, R.P.; Jones, L.G.; Kotchen, T.A.; Mougey, E.H.; Wherry, F.E.; Pennington, L.L.; Ricketts, P.T. Multiple hormonal responses to prolonged exercise in relation to physical training. J. Appl. Physiol. 1972, 33, 607–610. [Google Scholar] [CrossRef]
- Collins, K.J.; Weiner, J.S. Endocrinological aspects of exposure to high environmental temperatures. Physiol. Rev. 1968, 48, 785–839. [Google Scholar] [CrossRef]
- Friedl, K.E.; Moore, R.J.; Hoyt, R.W.; Marchitelli, L.J.; Martinez-lopez, L.E.; Askew, E.W. Endocrine markers of semistarvation in healthy lean men in a multistressor environment. J. Appl. Physiol. 2000, 88, 1820–1830. [Google Scholar] [CrossRef] [PubMed]
- Tauler, P.; Martinez, S.; Moreno, C.; Martínez, P.; Aguilo, A. Changes in salivary hormones, immunoglobulin A, and C-reactive protein in response to ultra-endurance exercises. Appl. Physiol. Nutr. Metab. 2014, 39, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Yousef, E.A.; El-kannishy, S.; Arfa, L.F.; Mahmoud, R. Plasma cortisol level and its relation to in-hospital mortality in acute kidney injury patients. J. Egypt Soc. Nephrol. Trans. 2021, 21, 91–97. [Google Scholar] [CrossRef]
- Rüst, C.A.; Knechtle, B.; Knechtle, P.; Rosemann, T. Similarities and differences in anthropometry and training between recreational male 100-km ultra-marathoners and marathoners. J. Sports Sci. 2012, 30, 1249–1257. [Google Scholar] [CrossRef]
- Reid, S.A.; Speedy, D.B.; Thompson, J.M.; Noakes, T.D.; Mulligan, G.; Page, T.; Campbell, R.G.; Milne, C. Study of hematological and biochemical parameters in runners completing a standard marathon. Clin. J. Sport Med. 2004, 14, 344–353. [Google Scholar] [CrossRef]
- Sinert, R.; Kohl, L.; Rainone, T.; Scalea, T. Exercise-induced rhabdomyolysis. Ann. Emerg. Med. 1994, 23, 1301–1306. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).