
The Short-Term Effect of Dynamic Tape versus the Low-Dye Taping Technique in Plantar Fasciitis: A Randomized Clinical Trial

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Method
2.1. Design
2.2. Participants
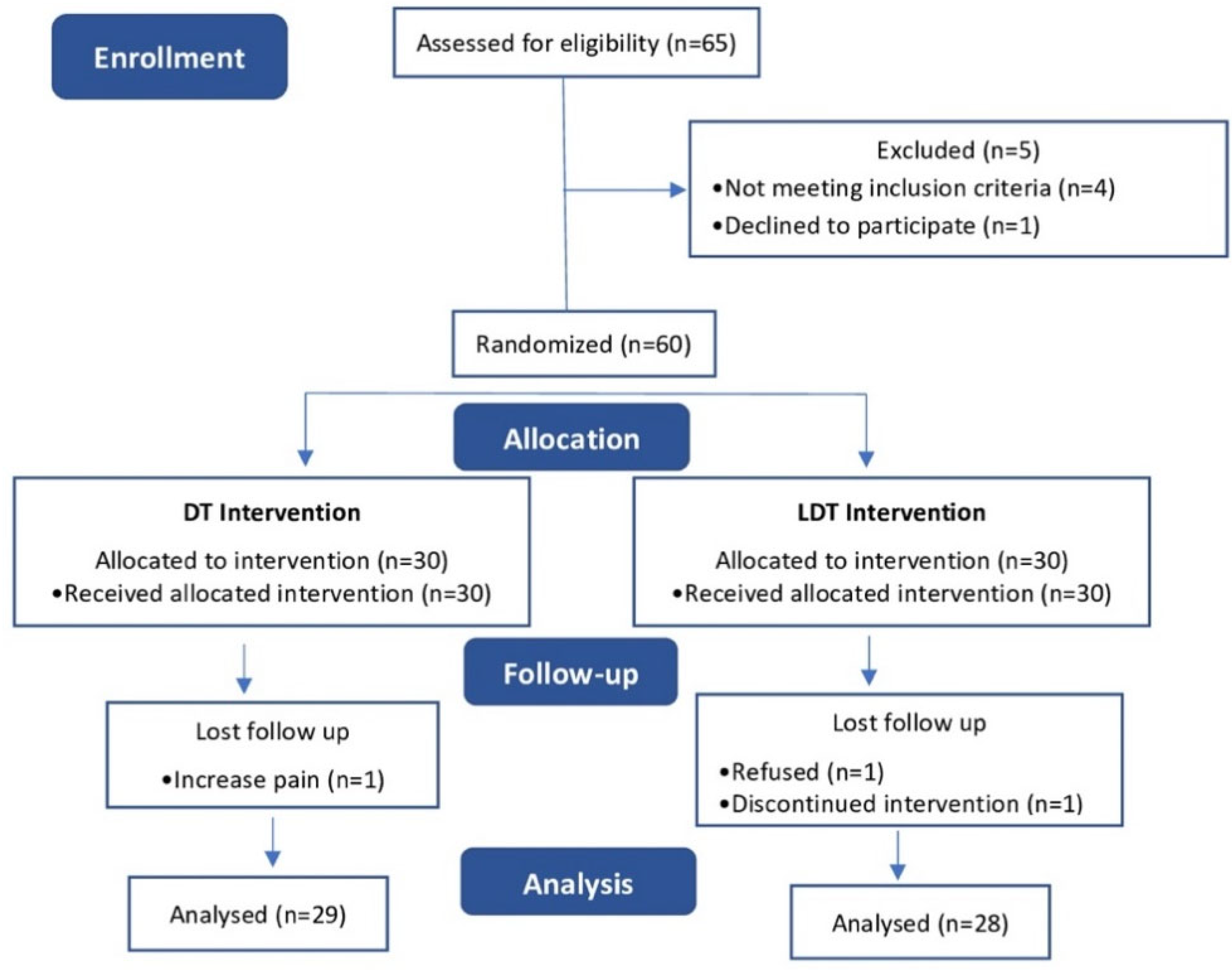
2.3. Randomization and Blinding
2.4. Measurements
2.5. Study Protocol
- -
- Windlass mechanism assessment.
- -
- Characteristic pain in the proximal medial calcaneal region.
- -
- Increased pain intensity after rest or exercise.
- -
- Test negative for tarsal tunnel syndrome.
- -
- FPI alteration.
- -
- Increase in BMI.
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trojian, T.; Tucker, A.K. Plantar Fasciitis. Am. Fam. Physician 2019, 99, 744–750. [Google Scholar] [PubMed]
- Salvioli, S.; Guidi, M.; Marcotulli, G. The Effectiveness of Conservative, Non-Pharmacological Treatment, of Plantar Heel Pain: A Systematic Review with Meta-Analysis. Foot 2017, 33, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, S.K.; Cerrato, R. Plantar Fasciitis: Evaluation and Treatment. J. Am. Acad. Orthop. Surg. 2008, 16, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Nie, D.; Rocha, J.L.; Hogan, M.V.; Wang, J.H.-C. Characterization of the Structure, Cells, and Cellular Mechanobiological Response of Human Plantar Fascia. J. Tissue Eng. 2018, 9, 204173141880110. [Google Scholar] [CrossRef] [PubMed]
- Latt, L.D.; Jaffe, D.E.; Tang, Y.; Taljanovic, M.S. Evaluation and Treatment of Chronic Plantar Fasciitis. Foot Ankle Orthop. 2020, 5, 2473011419896763. [Google Scholar] [CrossRef]
- Martin, R.L.; Davenport, T.E.; Reischl, S.F.; McPoil, T.G.; Matheson, J.W.; Wukich, D.K.; McDonough, C.M.; Altman, R.D.; Beattie, P.; Cornwall, M.; et al. Heel Pain—Plantar Fasciitis: Revision 2014. J. Orthop. Sport. Phys. Ther. 2014, 44, A1–A33. [Google Scholar] [CrossRef]
- Podolsky, R.; Kalichman, L. Taping for Plantar Fasciitis. J. Back Musculoskelet. Rehabil. 2015, 28, 1–6. [Google Scholar] [CrossRef]
- Verbruggen, L.A.; Thompson, M.M.; Durall, C.J. The Effectiveness of Low-Dye Taping in Reducing Pain Associated with Plantar Fasciitis. J. Sport Rehabil. 2018, 27, 94–98. [Google Scholar] [CrossRef]
- Van Tonder, T.; Allison, G.T.; Hopper, D.; Grisbrook, T.L. Multidimensional Impact of Low-Dye Taping on Low-Load Hopping in Individuals with and without Plantar Fasciitis. Phys. Ther. Sport 2018, 29, 43–49. [Google Scholar] [CrossRef]
- Chen, T.L.W.; Wong, D.W.C.; Peng, Y.; Zhang, M. Prediction on the Plantar Fascia Strain Offload upon Fascia Taping and Low-Dye Taping during Running. J. Orthop. Transl. 2020, 7, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Radford, J.A.; Burns, J.; Buchbinder, R.; Landorf, K.B.; Cook, C. The Effect of Low-Dye Taping on Kinematic, Kinetic, and Electromyographic Variables: A Systematic Review. J. Orthop. Sport. Phys. Ther. 2006, 36, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Osborne, H.R. Treatment of Plantar Fasciitis by LowDye Taping and Iontophoresis: Short Term Results of a Double Blinded, Randomised, Placebo Controlled Clinical Trial of Dexamethasone and Acetic Acid * Commentary. Br. J. Sport. Med. 2006, 40, 545–549. [Google Scholar] [CrossRef] [PubMed]
- McNeill, W.; Pedersen, C. Dynamic Tape. Is It All about Controlling Load? J. Bodyw. Mov. Ther. 2016, 20, 179–188. [Google Scholar] [CrossRef] [PubMed]
- de la Cruz Torres, B.; Albornoz Cabello, M.; Espejo Antúnez, L. Efecto Inmediato Del Vendaje Dynamic Tape® Sobre La Torsión Tibial Externa Con Dolor En Un Futbolista. Rev. Andal. Med. Deporte 2016, 9, 50–53. [Google Scholar] [CrossRef]
- Stecco, C.; Corradin, M.; Macchi, V.; Morra, A.; Porzionato, A.; Biz, C.; De Caro, R. Plantar Fascia Anatomy and Its Relationship with Achilles Tendon and Paratenon. J. Anat. 2013, 223, 665–676. [Google Scholar] [CrossRef]
- Bittencourt, N.; Leite, M.; Zuin, A.; Pereira, M.; Gonçalves, G.; Signoretti, S. Dynamic taping and high frontal plane knee projection angle in female volleyball athletes. Br. J. Sport. Med. 2017, 51, 297–298. [Google Scholar] [CrossRef]
- Lazaar, N.; Hernandez, B. Dynamic Tape®. Le Tape Nouvelle Génération. Rev. Podol. 2017, 13, 24–27. [Google Scholar] [CrossRef]
- McNeill, W.; Silvester, M. Plantar Heel Pain. J. Bodyw. Mov. Ther. 2017, 21, 205–211. [Google Scholar] [CrossRef]
- Cantín, M. Declaración de Helsinki de La Asociación Médica Mundial: Principios Éticos Para Las Investigaciones Médicas En Seres Humanos. Int. J. Med. Surg. Sci. 2014, 1, 339–346. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE Guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef]
- Martin, R.; PT, P.; Davenport, T.; Reischl, S.; Mcpoil, T.; Mathenson, J.; Wukich, D.; Mcdonough, C. Heel Pain-Plantar Fasciitis: Revision 2014: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2014, 44, A1–A33. [Google Scholar] [CrossRef]
- Al-Boloushi, Z.; Gómez-Trullén, E.M.; Bellosta-López, P.; López-Royo, M.P.; Fernández, D.; Herrero, P. Comparing Two Dry Needling Interventions for Plantar Heel Pain: A Protocol for a Randomized Controlled Trial. J. Orthop. Surg. Res. 2019, 14, 31. [Google Scholar] [CrossRef]
- Saghaei, M. Random Allocation Software for Parallel Group Randomized Trials. BMC Med. Res. Methodol. 2004, 4, 26. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the Visual Analog Scale for Measurement of Acute Pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef]
- Redmond, A.C.; Crane, Y.Z.; Menz, H.B. Normative Values for the Foot Posture Index. J. Foot Ankle Res. 2008, 1, 6. [Google Scholar] [CrossRef] [PubMed]
- Labovitz, J.M.; Yu, J.; Kim, C. The Role of Hamstring Tightness in Plantar Fasciitis. Foot Ankle Spec. 2011, 4, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Newell, T.; Simon, J.; Docherty, C.L. Arch-Taping Techniques for Altering Navicular Height and Plantar Pressures During Activity. J. Athl. Train. 2015, 50, 825–832. [Google Scholar] [CrossRef]
- Madruga Armada, Ó.; Molines Barroso, R.J.; Orejana García, Á.M. Efectos Del Vendaje Low-Dye Sobre El Pie. Revisión Narrativa. Rev. Española Podol. 2019, 30, 38–52. [Google Scholar] [CrossRef]
- Bolgla, L.A.; Malone, T.R. Plantar Fasciitis and the Windlass Mechanism: A Biomechanical Link to Clinical Practice. J. Athl. Train. 2004, 39, 77–82. [Google Scholar]
- Bagheri, R.; Pourahmadi, M.R.; Sarmadi, A.R.; Takamjani, I.E.; Torkaman, G.; Fazeli, S.H. What Is the Effect and Mechanism of Kinesiology Tape on Muscle Activity? J. Bodyw. Mov. Ther. 2018, 22, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Robinson, N.A.; Spratford, W.; Welvaert, M.; Gaida, J.; Fearon, A.M. Does Dynamic Tape Change the Walking Biomechanics of Women with Greater Trochanteric Pain Syndrome? A Blinded Randomised Controlled Crossover Trial. Gait Posture 2019, 70, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.; Riveiro, V.; Silva, R.; Zuin, A. Dynamic Tape in Elite Wolleyballers with Instability Post Lateral Ankle Sprain. Movimenta 2017, 4, 895. [Google Scholar]
- Kirmizigil, B.; Chauchat, J.R.; Yalciner, O.; Iyigun, G.; Angin, E.; Baltaci, G. The Effectiveness of Kinesio Taping in Recovering from Delayed Onset Muscle Soreness: A Crossover Study. J. Sport Rehabil. 2020, 29, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Evans, L. An Investigation Into the Effects of Dynamic Tape on Stabilisation, Foot Length, Foot Width and Navicular Drop in Athletes. Ph.D. Thesis, University of the West of England, Bristol, UK, 2018. [Google Scholar]



{kind=link}
{kind=link}
| DT Group (n = 29) | LDT Group (n = 28) | |
|---|---|---|
| Age | 39.59 ± 9.55 | 44.43 ± 7.06 |
| Gender male | 15 (51.7%) | 14 (50.0%) |
| Gender female | 14 (48.3%) | 14 (50%) |
| Weight | 75.21 ± 15.23 | 75.71 ± 6.97 |
| Height | 169.28 ± 10.65 | 165.29 ± 4.52 |
| IMC | 26.11 ± 4.07 | 24.38 ± 3.64 |
| Mean SD | 95 IC | pa | ||
|---|---|---|---|---|
| VAS | PRE | |||
| DT group | 7.55 ± 1.38 | 7.03–8.08 | ||
| LDT group | 6.64 ± 2.87 | 5.53–7.76 | 0.20 | |
| POST | ||||
| DT group | 5.35 ± 1.15 | 5.11–5.99 | ||
| LDT group | 5.54 ± 3.30 | 4.26–6.81 | ||
| DF_EXT | PRE | |||
| DT group | 7.50 ± 5.05 | 5.06–9.43 | ||
| LDT group | 8.32 ± 1.65 | 7.67–8.96 | 0.73 | |
| POST | ||||
| DT group | 8.45 ± 4.90 | 6.57–10.32 | ||
| LDT group | 8.56 ± 1.60 | 7.91–9.15 | ||
| DF_FLEX | PRE | |||
| DT group | 15.17 ± 6.31 | 12.77–17.57 | ||
| LDT group | 15.42 ± 4.57 | 13.65–17.20 | 0.78 | |
| POST | ||||
| DT group | 15.69 ± 6.20 | 13.32–18.05 | ||
| LDT group | 16.36 ± 4.50 | 14.61–18.10 | ||
| FPI | PRE | |||
| DT group | 2.90 ± 3.68 | 1.60–4.30 | ||
| LDT group | 3.96 ± 3.70 | 2.53–5.40 | 0.19 | |
| POST | ||||
| DT group | 2.93 ± 3.67 | 1.53–4.33 | ||
| LDT group | 3.50 ± 3.99 | 1.95–5.05 |
| Changes (POST-PRE Values) | Group | Mean SD | 95 IC | p b | η2 | F |
|---|---|---|---|---|---|---|
| VAS | DT | −2.05 ± 0.96 | (−2.37)–(−1.63) | 0.015 * | 0.10 | 6.33 |
| LDT | −1.10 ± 1.64 | (−1.74)–(−0.47) | ||||
| DF_EXT | DT | 0.93 ± 2.17 | 0.10–1.7 | 0.09 | 0.05 | 2.86 |
| LDT | 0.21 ± 0.56 | (<−0.01)–0.43 | ||||
| DF_FLEX | DT | 0.52 ± 2.89 | (−0.58)–1.6 | 0.47 | 0.01 | 0.51 |
| LDT | 0.93 ± 0.94 | 0.56–1.2 | ||||
| FPI | DT | 0.034 ± 0.32 | (−0.08)–0.15 | <0.001 * | 0.20 | 14 |
| LDT | −0.47 ± 0.64 | (−0.71)–(−0.22) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Méndez, A.; Palomo-Toucedo, I.C.; Pabón-Carrasco, M.; Ortiz-Romero, M.; Fernández-Seguín, L.M. The Short-Term Effect of Dynamic Tape versus the Low-Dye Taping Technique in Plantar Fasciitis: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 16536. https://doi.org/10.3390/ijerph192416536
Castro-Méndez A, Palomo-Toucedo IC, Pabón-Carrasco M, Ortiz-Romero M, Fernández-Seguín LM. The Short-Term Effect of Dynamic Tape versus the Low-Dye Taping Technique in Plantar Fasciitis: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2022; 19(24):16536. https://doi.org/10.3390/ijerph192416536
Chicago/Turabian StyleCastro-Méndez, Aurora, Inmaculada C. Palomo-Toucedo, Manuel Pabón-Carrasco, Mercedes Ortiz-Romero, and Lourdes Mª Fernández-Seguín. 2022. "The Short-Term Effect of Dynamic Tape versus the Low-Dye Taping Technique in Plantar Fasciitis: A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 19, no. 24: 16536. https://doi.org/10.3390/ijerph192416536
APA StyleCastro-Méndez, A., Palomo-Toucedo, I. C., Pabón-Carrasco, M., Ortiz-Romero, M., & Fernández-Seguín, L. M. (2022). The Short-Term Effect of Dynamic Tape versus the Low-Dye Taping Technique in Plantar Fasciitis: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health, 19(24), 16536. https://doi.org/10.3390/ijerph192416536