

Tobacco Use and Cessation Counseling among Dental Professionals in Saudi Arabia


Abstract
1. Introduction
2. Materials and Methods
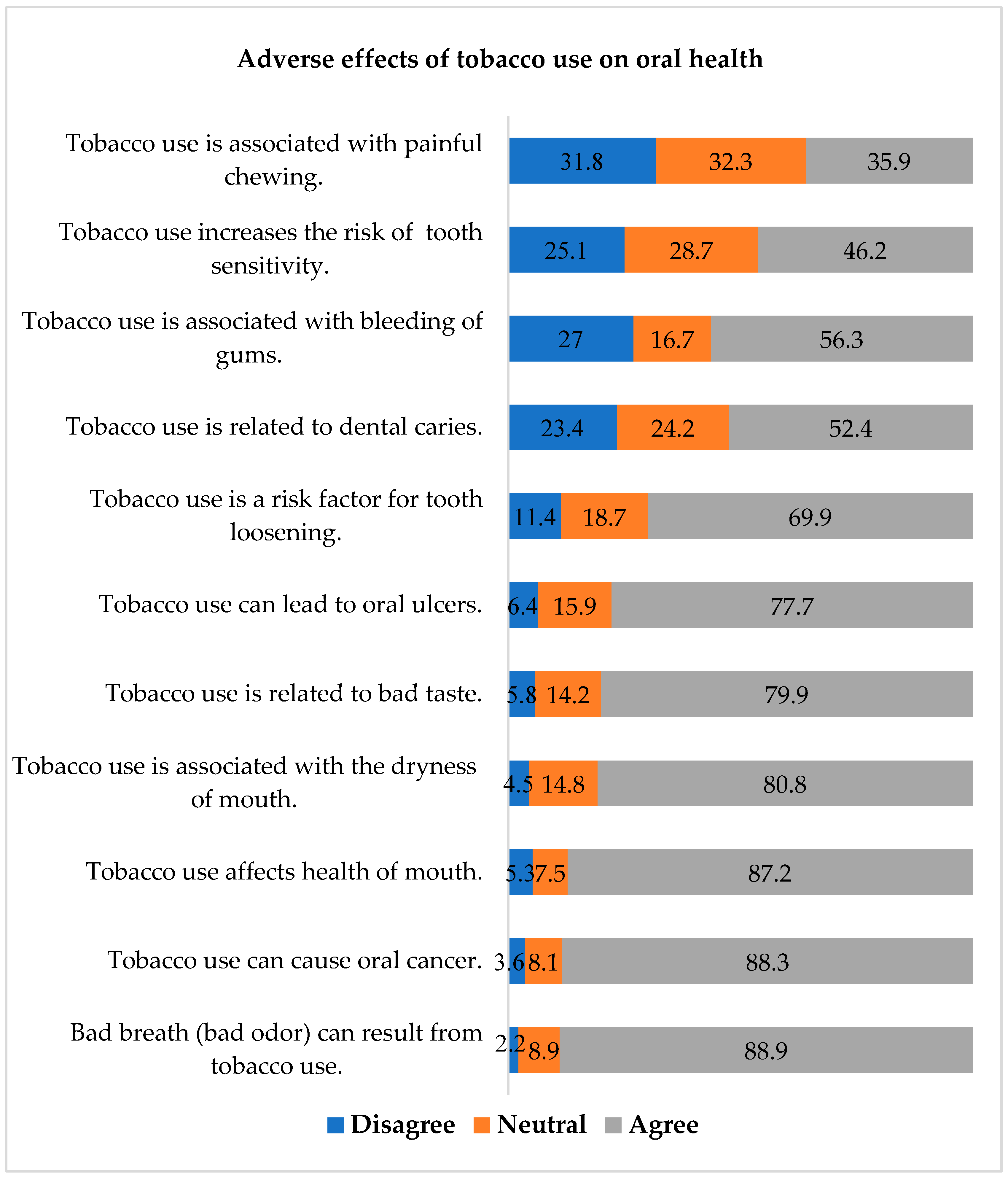
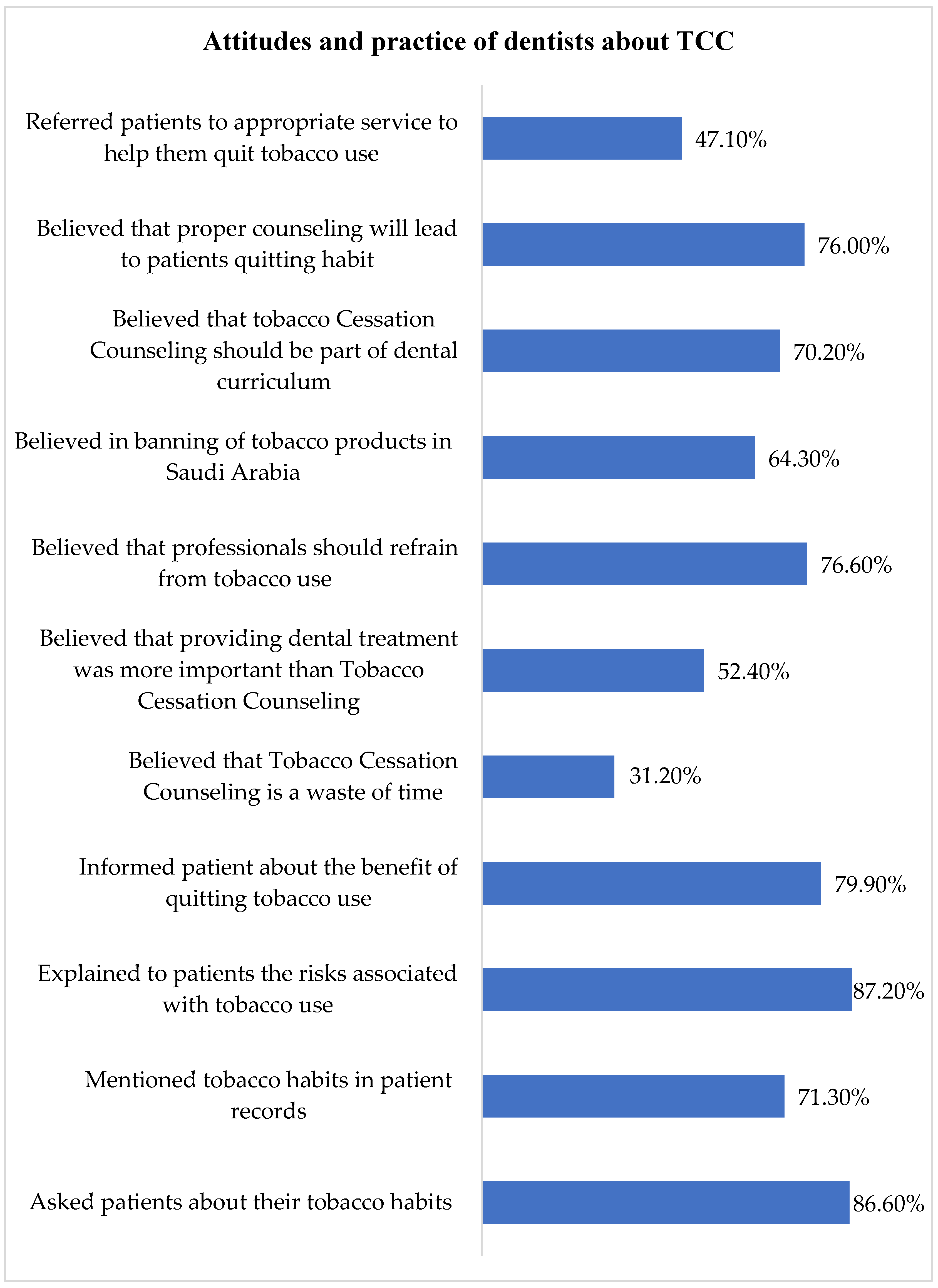
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health. Statistics of Smoking in Saudi Arabia. 2019. Available online: https://www.moh.gov.sa/HealthAwareness/EducationalContent/Anti-Smoking/Pages/default.aspx (accessed on 5 January 2022).
- World Health Organization. WHO Launches New Report on Global Tobacco Use Trends. Available online: https://www.who.int/news-room/detail/19-12-2019-who-launches-new-report-on-global-tobacco-use-trends (accessed on 5 January 2022).
- World Health Organization. Tobacco Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 5 January 2022).
- Centers for Disease Control and Prevention. Health Effects of Cigarette Smoking. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm (accessed on 5 January 2022).
- Wagnew, F.; Eshetie, S.; Alebel, A.; Dessie, G.; Tesema, C.; Abajobir, A.A. Meta-analysis of the prevalence of tuberculosis in diabetic patients and its association with cigarette smoking in African and Asian countries. BMC Res. Notes 2018, 11, 298. [Google Scholar] [CrossRef]
- Alexandridi, F.; Tsantila, S.; Pepelassi, E. Smoking cessation and response to periodontal treatment. Aust. Dent. J. 2018, 63, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Vellappally, S.; Fiala, Z.; Smejkalová, J.; Jacob, V.; Somanathan, R. Smoking related systemic and oral diseases. Acta Med.-Hradec Kral. 2007, 50, 161. [Google Scholar] [CrossRef]
- Omana-Cepeda, C.; Jane-Salas, E.; Estrugo-Devesa, A.; Chimenos-Kustner, E.; Lopez-Lopez, J. Effectiveness of dentist’s intervention in smoking cessation: A review. J. Clin. Exp. Dent. 2016, 8, e78–e83. [Google Scholar] [CrossRef]
- Nazir, M.A.; Almas, K. Awareness about the effects of tobacco consumption on oral health and the possibility of smoking behavior among male Saudi schoolchildren. Eur. J. Dent. 2017, 11, 29–35. [Google Scholar]
- Johnson, N.W.; Lowe, J.C.; Warnakulasuriya, K.A. Tobacco cessation activities of UK dentists in primary care: Signs of improvement. Br. Dent. J. 2006, 200, 85–89. [Google Scholar] [CrossRef]
- Babayan, A.; Dubray, J.; Haji, F.; Schwartz, R. Provision of Smoking Cessation by Ontario Dental Health Professionals; Ontario Tobacco Research Unit: Toronto, ON, Canada, 2012. [Google Scholar]
- Bhat, N.; Jyothirmai-Reddy, J.; Gohil, M.; Khatri, M.; Ladha, M.; Sharma, M. Attitudes, practices and perceived barriers in smoking cessation among dentists of Udaipur city, Rajasthan, India. Addict. Health 2014, 6, 73. [Google Scholar]
- Dean, A.; Sullivan, K.; Soe, M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version 2.3.1. 2010. Available online: https://www.scienceopen.com/book?vid=61cdd360-9883-4330-8c18-3f0341b0f715 (accessed on 5 November 2022).
- Maheswaran, T.; Mohanapriya, S.; Ganapathy, N.; Ilayaraja, V.; Dineshshankar, J.; Yoithapprabhunath, T.R.; Yamunadevi, A.M. Attitudes, practices, and perceived barriers in smoking cessation among the dental surgeons: A pilot study. J. Indian Acad. Dent. Spec. Res. 2017, 4, 38–41. [Google Scholar] [CrossRef]
- Bangera, D.; Takana, M.; Muttappallymyalil, J. Tobacco cessation: Attitude and practice of dentists in Northern United Arab Emirates. East Mediterr. Health J. 2018, 24, 419–426. [Google Scholar] [CrossRef]
- Al-Maweri, S.A.; Al-Soneidar, W.A.; Al Maqtari, A.; Hunaish, A.; Al-Sufyani, G.; Halboub, E. Tobacco Cessation Counseling: Attitudes and Practices among Yemeni Dental Professionals. J. Cancer Educ. 2018, 33, 1088–1093. [Google Scholar] [CrossRef] [PubMed]
- Parakh, A.; Megalamanegowdru, J.; Agrawal, R.; Hathiwala, S.; Chandrakar, M.; Tiwari, R.; Veeranna, T. Dental practitioners self reported performance of tobacco cessation counseling interventions: A cross sectional study. Asian Pac. J. Cancer Prev. 2013, 14, 6141–6145. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Alblowi, J.A. Perception of Tobacco Counseling and Cessation among Dental Practitioners. J. Smok. Cessat. 2021, 2021, 6692525. [Google Scholar] [CrossRef] [PubMed]
- Alajmi, B.; Abu-Hammad, O.; Al-Sharrad, A.; Dar-Odeh, N. Tobacco cessation support among dentists: A cross-sectional survey in Saudi Arabia and Kuwait. Tob. Prev. Cessat. 2017, 3, 121. [Google Scholar] [CrossRef] [PubMed]
- Ojima, M.; Hanioka, T.; Tanaka, H. Necessity and readiness for smoking cessation intervention in dental clinics in Japan. J. Epidemiol. 2012, 22, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Keogan, S.; Burns, A.; Babineau, K.; Clancy, L. Dental practitioners and smoking cessation in Ireland. Tob. Prev. Cessat. 2015, 1, 5. [Google Scholar] [CrossRef][Green Version]
- Lund, M.; Lund, K.E.; Rise, J. Preventing tobacco use in Norwegian dental practice. Commun. Dent. Oral Epidemiol. 2004, 32, 385–394. [Google Scholar] [CrossRef]
- Smith, D.R.; Leggat, P.A. Tobacco smoking prevalence among a cross-section of dentists in Queensland, Australia. Kurume Med. J. 2005, 52, 147–151. [Google Scholar] [CrossRef][Green Version]
- Patrick, D.L.; Cheadle, A.; Thompson, D.C.; Diehr, P.; Koepsell, T.; Kinne, S. The validity of self-reported smoking: A review and meta-analysis. Am. J. Public Health 1994, 84, 1086–1093. [Google Scholar] [CrossRef]
- Ray, C.S.; Pednekar, M.S.; Gupta, P.C.; Bansal-Travers, M.; Quah, A.C.; Fong, G.T. Social impacts on adult use of tobacco: Findings from the International Tobacco Control Project India, Wave 1 Survey. WHO South East Asia J. Public Health 2016, 5, 123–132. [Google Scholar] [CrossRef]
- Komar, K.; Glavina, A.; Boras, V.V.; Verzak, Ž.; Brailo, V. Impact of Smoking on Oral Health: Knowledge and Attitudes of Croatian Dentists and Dental Students. Acta Stomatol. Croat. 2018, 52, 148–155. [Google Scholar] [CrossRef]
- World Health Organization. WHO Monograph on Tobacco Cessation and Oral Health Integration. 2017. Available online: https://www.who.int/publications/i/item/who-monograph-on-tobacco-cessation-and-oral-health-integration (accessed on 14 May 2022).
- Dedeke, A.A.; Popoola, O.A.; Adebiyi, A.O.; Asuzu, M.C. Tobacco cessation services and related challenges among dentists in southwest Nigeria. Ann. Ib. Postgrad. Med. 2018, 16, 125–130. [Google Scholar] [PubMed]
- Wyne, A.H.; Chohan, A.N.; Al-Moneef, M.M.; Al-Saad, A.S. Attitudes of general dentists about smoking cessation and prevention in child and adolescent patients in Riyadh, Saudi Arabia. J. Contemp. Dent. Pract. 2006, 7, 35–43. [Google Scholar] [PubMed]
- Al-Jdani, S.; Mashabi, S.; Alsaywid, B.; Zahrani, A. Smoking cessation counseling: Knowledge, attitude and practices of primary healthcare providers at National Guard Primary Healthcare Centers, Western Region, Saudi Arabia. J. Fam. Commun. Med. 2018, 25, 175–182. [Google Scholar]
- Khalaf, M. Smoking cessation practices in Kuwaiti general dental clinics. Med. Princ. Pract. 2013, 22, 576–582. [Google Scholar] [CrossRef]
- Alhussain, A.A.; Alsaif, R.F.; Alahmari, J.M.; Aleheideb, A.A. Perceptions of smoking cessation counseling among dental students in Riyadh, Saudi Arabia: A cross-sectional study. Imam J. Appl. Sci. 2019, 4, 21. [Google Scholar]
- Preet, R.; Khan, N.; Blomstedt, Y.; Nilsson, M.; Stewart Williams, J. Assessing dental professionals’ understanding of tobacco prevention and control: A qualitative study in Västerbotten County, Sweden. BDJ Open 2016, 2, 16009. [Google Scholar] [CrossRef][Green Version]
- Uti, O.G.; Sofola, O.O. Smoking cessation counseling in dentistry: Attitudes of Nigerian dentists and dental students. J. Dent. Educ. 2011, 75, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Gaidhankar, S.; Sowmya, N.K.; Preeti, K.B.; Mehta, D.S. Knowledge, attitude, and implementation of nicotine replacement therapy by dental and medical interns in Davangere city: A cross-sectional survey. J. Indian Soc. Periodontol. 2020, 24, 567–571. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Study Variables | N (%) |
|---|---|
| Gender | |
| Male | 185 (51.5) |
| Female | 174 (48.5) |
| Nationality | |
| Saudi | 184 (51.3) |
| Non-Saudi | 175 (48.7) |
| Place of work | |
| Government sector | 114 (31.8) |
| Private sector | 245 (68.2) |
| Qualifications | |
| General Dentist | 238 (66.3) |
| Specialist/Consultant | 121 (33.7) |
| Income (Saudi Riyal) | |
| <10,000 per month | 142 (39.6) |
| ≥10,000 per month | 217 (60.4) |
| Marital Status | |
| Single | 129 (35.9) |
| Married | 230 (64.1) |
| Years in dental practice | |
| <10 years | 196 (54.6) |
| ≥10 years | 163 (45.4) |
| Current tobacco user | |
| Cigarette | 57 (15.9) |
| Cigars | 25 (7) |
| Smokeless tobacco | 7 (1.9) |
| Electronic Cigarettes | 10 (2.8) |
| Waterpipe (Hishah) | 15 (4.2) |
| Had a tobacco user at home/workplace (exposed to SHS) | 181 (50.4) |
| Variables | Unadjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Gender | 6.42 (3.04,13.56) | <0.001 * |
| Male | ||
| Female (Reference category) | ||
| Nationality | 1.16 (0.66, 2.05) | 0.606 |
| Saudi | ||
| Non-Saudi (Reference category) | ||
| Place of work | 0.73 (0.39, 1.38) | 0.336 |
| Government sector | ||
| Private sector (Reference category) | ||
| Qualifications | 1.24 (0.67, 2.29) | 0.499 |
| General Dentist | ||
| Specialist/Consultant (Reference category) | ||
| Income (Saudi Riyal) | 0.73 (0.40, 1.32) | 0.295 |
| <10,000 per month | ||
| ≥10,000 per month (Reference category) | ||
| Marital Status | 1.36 (0.77, 2.43) | 0.290 |
| Single | ||
| Married (Reference category) | ||
| Years in dental practice | 0.84 (0.47, 1.48) | 0.539 |
| <10 years | ||
| ≥10 years (Reference category) | ||
| Had a tobacco user at home/workplace (exposed to SHS) | 2.96 (1.59, 5.51) | <0.001 * |
| Yes | ||
| No (Reference category) | ||
| Believed that TCC is a waste of time. | 1.93 (1.08, 3.45) | 0.024 * |
| Yes | ||
| No (Reference category) | ||
| Believed that providing dental treatment was more important than TCC. | 2.45 (1.33, 4.51) | 0.003 * |
| Yes | ||
| No (Reference category) | ||
| Believed that dental professionals should refrain from tobacco use | 0.26 (0.14, 0.47) | <0.001 * |
| Yes | ||
| No (Reference category) | ||
| Favored banning of tobacco products in Saudi Arabia. | 0.19 (0.11, 0.35) | <0.001 * |
| Yes | ||
| No (Reference category) | ||
| Believed that proper TCC will lead patients to quit tobacco. | 0.52 (0.28, 0.95) | 0.032 * |
| Yes | ||
| No (Reference category) |
| Variables | β | S.E | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Gender | 1.705 | 0.407 | 5.50 (2.48, 12.23) | <0.001 |
| Male | ||||
| Female (Reference category) | ||||
| Had a tobacco user at home/workplace (exposed to SHS) | 1.156 | 0.361 | 3.18 (1.57, 6.45) | 0.001 |
| Yes | ||||
| No (Reference category) | ||||
| Believed that TCC is a waste of time | 0.843 | 0.366 | 2.32 (1.13, 4.76) | 0.021 |
| Yes | ||||
| No (Reference category) | ||||
| Believed that providing dental treatment was more important than TCC | 0.927 | 0.369 | 2.53 (1.23, 5.21) | 0.012 |
| Yes | ||||
| No (Reference category) | ||||
| Believed in banning of tobacco products in Saudi Arabia | −1.881 | 0.363 | 0.15 (0.07, 0.31) | <0.001 |
| Yes | ||||
| No (Reference category) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljubran, H.; Alkoudemi, M.; Althunayan, M.; Aljeraisy, A.; Asiri, A.; Nazir, M. Tobacco Use and Cessation Counseling among Dental Professionals in Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 16306. https://doi.org/10.3390/ijerph192316306
Aljubran H, Alkoudemi M, Althunayan M, Aljeraisy A, Asiri A, Nazir M. Tobacco Use and Cessation Counseling among Dental Professionals in Saudi Arabia. International Journal of Environmental Research and Public Health. 2022; 19(23):16306. https://doi.org/10.3390/ijerph192316306
Chicago/Turabian StyleAljubran, Hussain, Mohammed Alkoudemi, Mustafa Althunayan, Abdulrahman Aljeraisy, Amal Asiri, and Muhammad Nazir. 2022. "Tobacco Use and Cessation Counseling among Dental Professionals in Saudi Arabia" International Journal of Environmental Research and Public Health 19, no. 23: 16306. https://doi.org/10.3390/ijerph192316306
APA StyleAljubran, H., Alkoudemi, M., Althunayan, M., Aljeraisy, A., Asiri, A., & Nazir, M. (2022). Tobacco Use and Cessation Counseling among Dental Professionals in Saudi Arabia. International Journal of Environmental Research and Public Health, 19(23), 16306. https://doi.org/10.3390/ijerph192316306