
The Influence of Therapeutic Exercise on Survival and the Quality of Life in Survivorship of Women with Ovarian Cancer


 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection of Studies
2.4. Data Extraction
2.5. Methodological Quality
3. Results
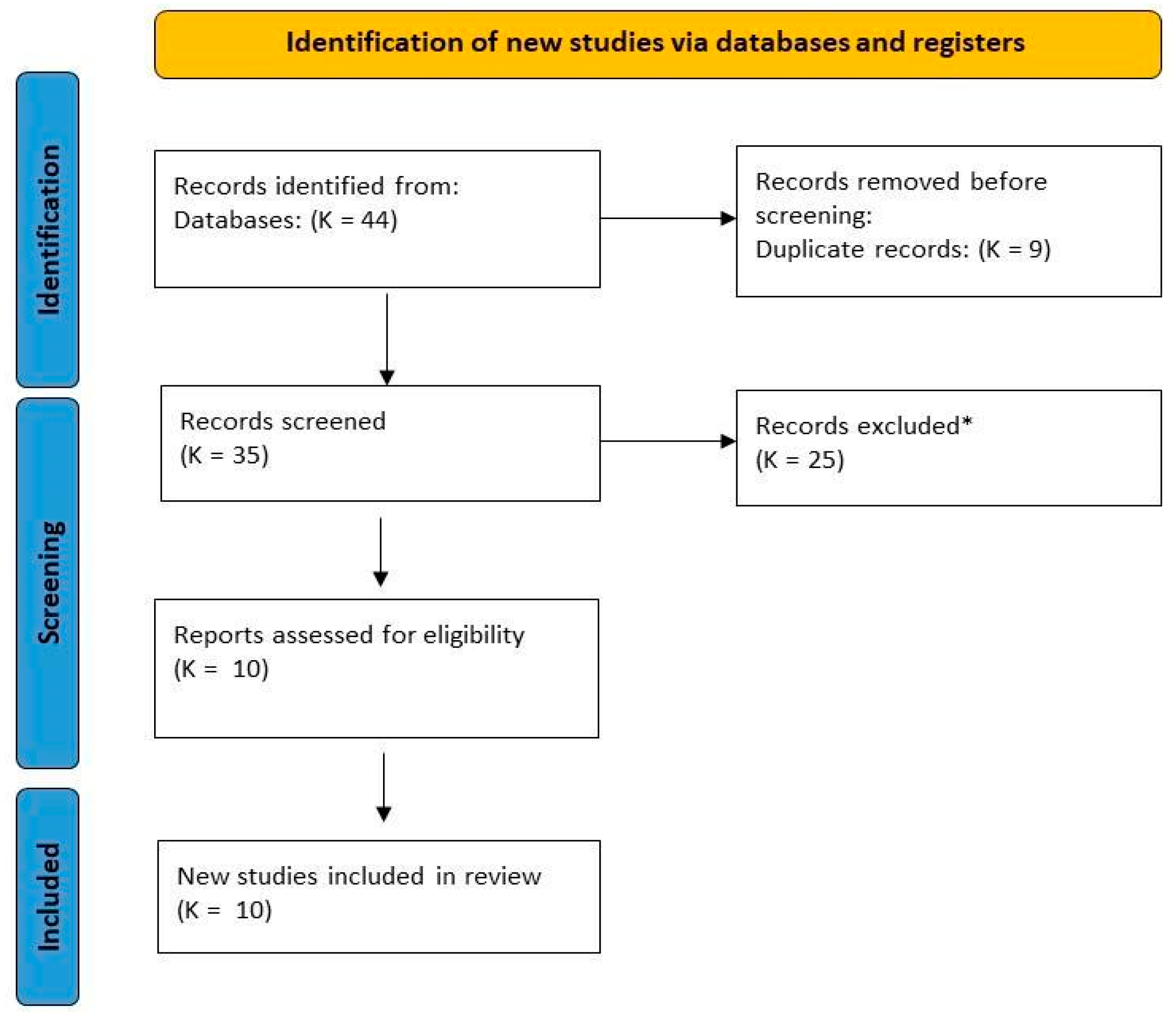
3.1. Selection of Studies
3.2. Main Characteristics of the Studies
3.3. Methodological Quality
4. Discussion
4.1. Synthesis of the Discussion in Terms of Selected Articles
4.2. Synthesis of the Discussion in Terms of Non-Selected Articles
4.3. Discussion of the Evolution of the Characteristics of the Studies. Development Standards, Objectivity, Conclusions and Specific Justifications
4.4. Strengths and Limitations of Our Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Stewart, C.; Ralyea, C.; Lockwood, S. Ovarian Cancer: An Integrated Review. Semin. Oncol. Nurs. 2019, 35, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Slatnik, C.L.P.; Duff, E. Ensuring Early Diagnosis. Nurse Pract. 2015, 40, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Kossaï, M.; Leary, A.; Scoazec, J.Y.; Genestie, C. Ovarian Cancer: A Heterogeneous Disease. Pathobiology 2018, 85, 41–49. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services Cancer Stat Facts: Ovarian Cancer. Available online: https://seer.cancer.gov/statfacts/html/ovary.html (accessed on 21 July 2022).
- Society, A.C. Special Section: Ovarian Cancer. Cancers Facts Fig. 2018, 45, 28–43. [Google Scholar]
- McGrath, D.; O’halloran, P.; Prue, G.; Brown, M.; Millar, J.; O’donnell, A.; McWilliams, L.; Murphy, C.; Hinds, G.; Reid, J. Exercise Interventions for Women with Ovarian Cancer: A Realist Review. Healthcare 2022, 10, 720. [Google Scholar] [CrossRef]
- Stout, N.L.; Baima, J.; Swisher, A.K.; Winters-Stone, K.M.; Welsh, J. A Systematic Review of Exercise Systematic Reviews in the Cancer Literature (2005–2017). PM R 2017, 9, S347–S384. [Google Scholar] [CrossRef] [PubMed]
- Rojas Avendaño, F.A.; Sepúlveda Arenas, N.; González Victoria, A.F.; Carvajal Tello, N. Prescription of Exercise in Cancer Patients. Systematic Review. Fisioterapia 2021, 43, 218–229. [Google Scholar] [CrossRef]
- Arroyo Morales, M.; Fernández de las Peñas, C. Fisioterapia y Cáncer: Cruce de Caminos. Fisioterapia 2014, 36, 151–152. [Google Scholar] [CrossRef]
- Dovnik, A.; Dovnik, N.F. Vitamin D and Ovarian Cancer: Systematic Review of the Literature with a Focus on Molecular Mechanisms. Cells 2020, 9, 335. [Google Scholar] [CrossRef]
- Antoniak, A.E.; Greig, C.A. The Effect of Combined Resistance Exercise Training and Vitamin D 3 Supplementation on Musculoskeletal Health and Function in Older Adults: A Systematic Review and Meta-Analysis. BMJ Open 2017, 7, e014619. [Google Scholar] [CrossRef] [PubMed]
- Willems, H.M.E.; van den Heuvel, E.G.H.M.; Schoemaker, R.J.W.; Klein-Nulend, J.; Bakker, A.D. Diet and Exercise: A Match Made in Bone. Curr. Osteoporos. Rep. 2017, 15, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Beck, B.R.; Daly, R.M.; Singh, M.A.F.; Taaffe, D.R. Exercise and Sports Science Australia (ESSA) Position Statement on Exercise Prescription for the Prevention and Management of Osteoporosis. J. Sci. Med. Sport 2017, 20, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Gruber, F.O.; Sagaster, P. Generalrehabilitation in Der Onkologie. Oncol. Res. Treat. 1979, 2, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Cannioto, R.A.; Moysich, K.B. Epithelial Ovarian Cancer and Recreational Physical Activity: A Review of the Epidemiological Literature and Implications for Exercise Prescription. Gynecol. Oncol. 2015, 137, 559–573. [Google Scholar] [CrossRef]
- Jones, T.L.; Sandler, C.X.; Spence, R.R.; Hayes, S.C. Physical Activity and Exercise in Women with Ovarian Cancer: A Systematic Review. Gynecol. Oncol. 2020, 158, 803–811. [Google Scholar] [CrossRef]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a Knowledge Representation for Clinical Questions. AMIA Annu. Symp. Proc. 2006, 2006, 359–363. [Google Scholar] [PubMed]
- Health Sciences Descriptors: DeCS. 2017 ed. São Paulo (SP): BIREME/PAHO/WHO. 2017. Available online: http://decs.bvsalud.org/I/homepagei.htm (accessed on 25 July 2022).
- National Library of Medicine MeSH (Medical Subject Headings). Available online: https://www.ncbi.nlm.nih.gov/mesh/ (accessed on 25 July 2022).
- Donnelly, C.M.; Blaney, J.M.; Lowe-Strong, A.; Rankin, J.P.; Campbell, A.; McCrum-Gardner, E.; Gracey, J.H. A Randomised Controlled Trial Testing the Feasibility and Efficacy of a Physical Activity Behavioural Change Intervention in Managing Fatigue with Gynaecological Cancer Survivors. Gynecol. Oncol. 2011, 122, 618–624. [Google Scholar] [CrossRef]
- Mizrahi, D.; Broderick, C.; Friedlander, M.; Ryan, M.; Harrison, M.; Pumpa, K.; Naumann, F. An Exercise Intervention during Chemotherapy for Women with Recurrent Ovarian Cancer: A Feasibility Study. Int. J. Gynecol. Cancer 2015, 25, 985–992. [Google Scholar] [CrossRef]
- Zhou, Y.; Cartmel, B.; Gottlieb, L.; Ercolano, E.A.; Li, F.; Harrigan, M.; McCorkle, R.; Ligibel, J.A.; von Gruenigen, V.E.; Gogoi, R.; et al. Randomized Trial of Exercise on Quality of Life in Women with Ovarian Cancer: Women’s Activity and Lifestyle Study in Connecticut (WALC). J. Natl. Cancer Inst. 2017, 109, djx072. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, F.; Zhang, H.; Yu, X.; Cong, Y. Effects of Nurse-Led Home-Based Exercise & Cognitive Behavioral Therapy on Reducing Cancer-Related Fatigue in Patients with Ovarian Cancer during and after Chemotherapy: A Randomized Controlled Trial. Int. J. Nurs. Stud. 2018, 78, 52–60. [Google Scholar] [CrossRef]
- Iyer, N.S.; Cartmel, B.; Friedman, L.; Li, F.; Zhou, Y.; Ercolano, E.; Harrigan, M.; Gottlieb, L.; McCorkle, R.; Schwartz, P.E.; et al. Lymphedema in Ovarian Cancer Survivors: Assessing Diagnostic Methods and the Effects of Physical Activity. Cancer 2018, 124, 1929–1937. [Google Scholar] [CrossRef] [PubMed]
- Schofield, C.; Newton, R.U.; Galvão, D.A.; Cohen, P.A.; Peddle-McIntyre, C.J. A Physiological Profile of Ovarian Cancer Survivors to Inform Tailored Exercise Interventions and the Development of Exercise Oncology Guidelines. Int. J. Gynecol. Cancer 2017, 27, 1560–1567. [Google Scholar] [CrossRef]
- Newton, M.J.; Hayes, S.C.; Janda, M.; Webb, P.M.; Obermair, A.; Eakin, E.G.; Wyld, D.; Gordon, L.G.; Beesley, V.L. Safety, Feasibility and Effects of an Individualised Walking Intervention for Women Undergoing Chemotherapy for Ovarian Cancer: A Pilot Study. BMC Cancer 2011, 11, 389. [Google Scholar] [CrossRef]
- Zhang, X.; McClean, D.; Ko, E.; Morgan, M.A.; Schmitz, K.H. Exercise among Women with Ovarian Cancer: A Feasibility and Pre-/Post-Test Exploratory Pilot Study. Oncol. Nurs. Forum 2017, 44, 366–374. [Google Scholar] [CrossRef]
- Czerwińska-Ledwig, O.; Vesole, D.H.; Piotrowska, A.; Gradek, J.; Pilch, W.; Jurczyszyn, A. Effect of a 6-Week Cycle of Nordic Walking Training on Vitamin 25(OH)D3, Calcium-Phosphate Metabolism and Muscle Damage in Multiple Myeloma Patients–Randomized Controlled Trial. J. Clin. Med. 2022, 11, 6534. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services Cancer Stat Facts: Female Breast Cancer. Available online: https://seer.cancer.gov/statfacts/html/breast.html (accessed on 10 July 2022).
- Schwartz, A.L. Physical Activity after a Cancer Diagnosis: Psychosocial Outcomes. Cancer Investig. 2004, 22, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Mock, V.; Pickett, M.; Ropka, M.E.; Lin, E.M.; Stewart, K.J.; Rhodes, V.A.; McDaniel, R.; Grimm, P.M.; Krumm, S.; McCorkle, R.; et al. Fatigue and Quality of Life Outcomes of Exercise during Cancer Treatment. Cancer Pract. 2001, 9, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; Friedenreich, C.M.; Sela, R.A.; Quinney, H.A.; Rhodes, R.E.; Handman, M. The Group Psychotherapy and Home-Based Physical Exercise (GROUP-HOPE) Trial in Cancer Survivors: Physical Fitness and Quality of Life Outcomes. Psychooncology 2003, 12, 357–374. [Google Scholar] [CrossRef] [PubMed]
- Beesley, V.L.; Price, M.A.; Butow, P.N.; Green, A.C.; Olsen, C.M.; Webb, P.M. Beesley (2011): PA/QOL in OVCA. Psychooncology 2011, 20, 1161–1169. [Google Scholar] [CrossRef]
- Anderson, R.T.; Peres, L.C.; Camacho, F.; Bandera, E.V.; Funkhouser, E.; Moorman, P.G.; Paddock, L.E.; Peters, E.S.; Abbott, S.E.; Alberg, A.J.; et al. Individual, Social, and Societal Correlates of Health-Related Quality of Life among African American Survivors of Ovarian Cancer: Results from the African American Cancer Epidemiology Study. J. Womens Health 2019, 28, 284–293. [Google Scholar] [CrossRef]
- Lowe, K.; Andersen, M.; Sweet, E.; Standish, L.; Drescher, C.; Goff, B. The Effect of Regular Exercise and Yoga on Health-Related Quality of Life Among Ovarian Cancer Survivors. J. Evid. Based Complement. Altern. 2012, 17, 155–160. [Google Scholar] [CrossRef]
- Smits, A.; Smits, E.; Lopes, A.; Das, N.; Hughes, G.; Talaat, A.; Pollard, A.; Bouwman, F.; Massuger, L.; Bekkers, R.; et al. Bodymass Index, Physical Activity and Quality of Life of Ovarian Cancer Survivors: Time to Get Moving? Gynecol. Oncol. 2015, 139, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Stevinson, C.; Faught, W.; Steed, H.; Tonkin, K.; Ladha, A.B.; Vallance, J.K.; Capstick, V.; Schepansky, A.; Courneya, K.S. Associations between Physical Activity and Quality of Life in Ovarian Cancer Survivors. Gynecol. Oncol. 2007, 106, 244–250. [Google Scholar] [CrossRef]
- Webber, K.; Carolus, E.; Mileshkin, L.; Sommeijer, D.; McAlpine, J.; Bladgen, S.; Coleman, R.L.; Herzog, T.J.; Sehouli, J.; Nasser, S.; et al. OVQUEST—Life after the Diagnosis and Treatment of Ovarian Cancer—An International Survey of Symptoms and Concerns in Ovarian Cancer Survivors. Gynecol. Oncol. 2019, 155, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Schofield, C.; Newton, R.U.; Cohen, P.A.; Galvão, D.A.; McVeigh, J.A.; Mohan, G.R.; Tan, J.; Salfinger, S.G.; Straker, L.M.; Peddle-McIntyre, C.J. Health-Related Quality of Life and Pelvic Floor Dysfunction in Advanced-Stage Ovarian Cancer Survivors: Associations with Objective Activity Behaviors and Physiological Characteristics. Support. Care Cancer 2018, 26, 2239–2246. [Google Scholar] [CrossRef]
- Joly, F.; Ahmed-Lecheheb, D.; Kalbacher, E.; Heutte, N.; Clarisse, B.; Grellard, J.M.; Gernier, F.; Berton-Rigaud, D.; Tredan, O.; Fabbro, M.; et al. Long-Term Fatigue and Quality of Life among Epithelial Ovarian Cancer Survivors: A GINECO Case/Control VIVROVAIRE i Study. Ann. Oncol. 2019, 30, 845–852. [Google Scholar] [CrossRef]
- Liavaag, A.H.; Dørum, A.; Fosså, S.D.; Tropé, C.; Dahl, A.A. Controlled Study of Fatigue, Quality of Life, and Somatic and Mental Morbidity in Epithelial Ovarian Cancer Survivors: How Lucky Are the Lucky Ones? J. Clin. Oncol. 2007, 25, 2049–2056. [Google Scholar] [CrossRef]
- Stevinson, C.; Steed, H.; Faught, W.; Tonkin, K.; Vallance, J.; Ladha, A.; Schepansky, A.; Capstick, V.; Courneya, K. Physical Activity in Ovarian Cancer Survivors: Associations with Fatigue, Sleep, and Psychosocial Functioning. Int. J. Gynecol Cancer 2009, 19, 73–78. [Google Scholar] [CrossRef]
- von Gruenigen, V.E.; Frasure, H.E.; Jenison, E.L.; Hopkins, M.P.; Gil, K.M. Longitudinal Assessment of Quality of Life and Lifestyle in Newly Diagnosed Ovarian Cancer Patients: The Roles of Surgery and Chemotherapy. Gynecol. Oncol. 2006, 103, 120–126. [Google Scholar] [CrossRef]
- Cannioto, R.A.; LaMonte, M.J.; Kelemen, L.E.; Risch, H.A.; Eng, K.H.; Minlikeeva, A.N.; Hong, C.C.; Szender, J.B.; Sucheston-Campbell, L.; Joseph, J.M.; et al. Recreational Physical Inactivity and Mortality in Women with Invasive Epithelial Ovarian Cancer: Evidence from the Ovarian Cancer Association Consortium. Br. J. Cancer 2016, 115, 95–101. [Google Scholar] [CrossRef]
- Minlikeeva, A.N.; Cannioto, R.; Jensen, A.; Kjaer, S.K.; Jordan, S.J.; Diergaarde, B.; Szender, J.B.; Odunsi, K.; Almohanna, H.; Mayor, P.; et al. Joint Exposure to Smoking, Excessive Weight, and Physical Inactivity and Survival of Ovarian Cancer Patients, Evidence from the Ovarian Cancer Association Consortium. Cancer Causes Control 2019, 30, 537–547. [Google Scholar] [CrossRef] [PubMed]
- De Groef, A.; Geraerts, I.; Demeyer, H.; Van der Gucht, E.; Dams, L.; de Kinkelder, C.; Dukers-van Althuis, S.; Van Kampen, M.; Devoogdt, N. Physical Activity Levels after Treatment for Breast Cancer: Two-Year Follow-Up. Breast 2018, 40, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Fassier, P.; Zelek, L.; Partula, V.; Srour, B.; Bachmann, P.; Touillaud, M.; Druesne-Pecollo, N.; Galan, P.; Cohen, P.; Hoarau, H.; et al. Variations of Physical Activity and Sedentary Behavior between before and after Cancer Diagnosis: Results from the Prospective Population-Based NutriNet-Santé Cohort. Medicine 2016, 95, e4629. [Google Scholar] [CrossRef]
- Lin, K.Y.; Edbrooke, L.; Granger, C.L.; Denehy, L.; Frawley, H.C. The Impact of Gynaecological Cancer Treatment on Physical Activity Levels: A Systematic Review of Observational Studies. Braz. J. Phys. Ther. 2019, 23, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.A.; Crane, T.E.; Miller, A.; Garcia, D.O.; Basen-Engquist, K.; Alberts, D.S. A Randomized Trial of Diet and Physical Activity in Women Treated for Stage II–IV Ovarian Cancer: Rationale and Design of the Lifestyle Intervention for Ovarian Cancer Enhanced Survival (LIVES): An NRG Oncology/Gynecologic Oncology Group (GOG-225) Study. Contemp. Clin. Trials 2016, 49, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Stelten, S.; Hoedjes, M.; Kenter, G.G.; Kampman, E.; Huijsmans, R.J.; Van Lonkhuijzen, L.R.C.W.; Buffart, L.M. Rationale and Study Protocol of the Physical Activity and Dietary Intervention in Women with OVArian Cancer (PADOVA) Study: A Randomised Controlled Trial to Evaluate Effectiveness of a Tailored Exercise and Dietary Intervention on Body Composition, Physic. BMJ Open 2020, 10, e036854. [Google Scholar] [CrossRef]
- Campbell, K.; Winters-Stone, K.; Wiskemann, J.; May, A.; Schwartz, A.; Courneya, K.; Zucker, D.; Matthews, C.; Ligibel, J.; Gerber, L.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sport. Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- El-Sherif, A.; El-Sherif, S.; Taylor, A.; Ayakannu, T. Ovarian Cancer: Lifestyle, Diet. Nutr. Nutr. Cancer 2020, 74, 1092–1107. [Google Scholar]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvão, D.A. The Exercise and Sports Science Australia Position Statement: Exercise Medicine in Cancer Management. J. Sci. Med. Sport 2019, 22, 1175–1199. [Google Scholar] [CrossRef]
- Shinde, S.; Wanger, T.; Novotny, P.; Grudem, M.; Jatoi, A. Disease-Free Ovarian Cancer Patients Report Severe Pain and Fatigue over Time: Prospective Quality of Life Assessment in a Consecutive Series. Eur. J. Gynaecol. Oncol. 2015, 36, 155–160. [Google Scholar]
- Kurnit, K.C.; Fleming, G.F. Updates and New Options in Advanced Epithelial Ovarian Cancer Treatment. Obstet. Gynecol. 2021, 137, 108–121. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search Equations | Database |
|---|---|
| (exercise therapy[MeSH Terms]) AND (ovarian neoplasms[MeSH Terms]) (exercise therapy[MeSH Terms]) AND (cancer, ovarian[MeSH Terms]) | PubMed 1 |
| ovarian neoplasms exercise therapy ovarian cancer exercise therapy | PEDro 2 |
| “exercise therapy” AND (“ovarian cancer” OR “ovarian neoplasms”) | Scopus 3 |
| Study | Year | Type of Study | Sample (n = ) Groups | Interventions | Scales/ Instruments | Conclusions | JBI Evidence Synthesis |
|---|---|---|---|---|---|---|---|
| Donnelly et al. [19] | 2011 | Randomised clinical trial | 1 n = 33 2 EG: n = 16 3 CG: n = 17 | 2 EG: home-based physical activity for 12 weeks. -Frequency: individualised according to the duration of chemotherapy. -Intensity: moderate (Borg RPE 12–13). -Type: walking and strengthening exercises. -Time: individualised (e.g., 10 min at the beginning and then increase). Supervision: 1 initial individual face-to-face session with a physiotherapist + 1 phone call/week for 10 weeks + final face-to-face consultation at week 12 and 2 months of follow-up phone calls. 3 CG: standard care. Same phone calls as 2 EG. No advice on how to change their physical activity levels during the study period. | 5 MFSI-SF 6 FACIT-F 7 FACT-G 8 BDI-II 9 PANAS 10 BMI 11 12MWT 12 Borg RPE 13 PSQI 14 7 Day PAR | A physical activity intervention for gynaecological cancer survivors demonstrates improvements in fatigue, but confirmation in the form of a larger, more powered randomised clinical trial is warranted. | 11/13 |
| Mizrahi et al. [20] | 2015 | Single group clinical trial (pre/post) | 4 GP/P: n = 30 | 4 GP/P: physical exercise carried out at home. -Frequency: 3–4 times/week for 12 weeks. -Intensity: Low-Moderate (Borg RPE 11–14). -Resistance: 3 sets per exercise of 10 repetitions. -Type: Combination of aerobic (walking, cycling, swimming), resistance (resistance band, body weight exercises), core stability (floor, stability ball exercises) and balance exercises. -Time: 10–40 min/session, 90 min/wk. - Supervision: 1 face-to-face session + 1 telephone session/week. | 15 IPAQ 13 PSQI 16 SPHERE 17 SF-36 18 FACT-O 19 FACT-Ntx 12 Borg RPE | The results indicate that two-thirds of women with recurrent ovarian cancer were able to complete a low-to-moderate aerobic exercise programme of 90 min per week, with no adverse events reported. Randomised control studies are required to confirm the benefits of exercise reported in this study. | 8/9 |
| Zhou et al. [21] | 2017 | Randomised clinical trial | 1 n = 144 2 GE: n = 74 3 GC: n = 70 | 2 EG: physical exercise performed at home. -Frequency: 26 weeks. -Intensity: Moderate (target heart rate range based on the Karvonen method for moderate to vigorous intensity. The study provided heart rate monitors). -Type: Aerobic (mainly brisk walking) -Time: 150 min/week. -Supervision: 1 phone session/week with a 20ACSM-certified cancer exercise coach. 3 CG: 26 weeks, information related to ovarian cancer survivorship. -Supervision: 1 phone session/week with a 21WALC staff member. 21 WALC staff member. | 22 HRQOL 23 FACT-F 17 SF-36 24 MCS 25 PCS | A six-month, home-based, telephone-delivered exercise intervention, consisting primarily of brisk walking, was shown to be associated with improved physical health-related quality of life in women with ovarian cancer. For this reason, health professionals should recommend and refer women diagnosed with ovarian cancer for physical exercise programmes in the clinic or in the community. | 9/13 |
| Zhang et al. [26] | 2018 | Randomised clinical trial | 1 n = 72 2 EG: n = 36 3 CG: n = 36 | 2 GE: physical exercise performed at home + 26 TCC. -Frequency: 3–5 times/week. -Intensity: 40–75% of 27 FCM. Type: warm-up, aerobic, muscle strength, resistance training and stretching, deep relaxation and cool down. -Time: 25–60 min/session. -Supervision: 1 telephone session/week conducted by experienced nurses. 26 CBT: via internet. 1x/week for 12 consecutive weeks. Duration: 1 h/session. 3 CG: no special care. Only medication education, balanced diet recommendations and health education on ovarian cancer chemotherapy. | 28 PFS 29 SDS 13 PSQI 30 ANOVA | The results indicate that exercise plus nurse-delivered home-based 26 CBT has measurable benefits in helping women with ovarian cancer decrease cancer-related fatigue and depressive symptoms and improve their sleep quality. | 11/13 |
| Iyer et al. [23] | 2018 | Part of a randomised controlled trial. | 1 n = 95 2 EG: n = 50 3 CG: n = 45 | 2 EG: physical exercise performed at home. -Frequency: 26 weeks. -Intensity: moderate (target heart rate range based on the Karvonen method for moderate to vigorous intensity. The study provided heart rate monitors). -Type: Aerobic (mainly brisk walking). Time: 150 min/week. -Supervision: 1 telephone session/week with a 20 ACSM certified cancer exercise trainer. 3 CG: 26 weeks, information related to ovarian cancer survivorship. -Supervision: 1 phone session/week with a 21 WALC staff member. | Self-Report questionnaire. Electronic periometer. Assessment by a physiotherapist specialising in lymphoedema. | With a potential prevalence of lower limb lymphoedema (LLL) of up to 40%, further evaluation of diagnostic methods is required to better characterise this side effect of ovarian cancer treatment. No adverse effects of exercise on LLL were found. Further research is needed to evaluate predictors of LLL and the effects of exercise on LLL to develop effective physical activity recommendations for women with ovarian cancer. | 10/13 |
| Cannioto et al. [14] | 2015 | Systematic Review | Number of studys: 26 | A comprehensive literature search was conducted through PubMed for epidemiological investigations focusing on the association between 31 RPA and epithelial ovarian cancer risk and survival. | Total number of hours or 32 MET hours of activity performed/week. 10 BMI | Due to the limitations found in the research, emphasis should be placed on the larger body of scientific literature, which has shown that leading a physically active lifestyle results in a wide range of benefits. | 6/11 |
| Schofield et al. [24] | 2017 | Narrative Review | Number of studys: not specified | A review was conducted of the current literature in PubMed, MEDLINE, CINAHL and SPORTDiscus databases of English-language articles published between January 1970 and December 2016 on the physiological status of ovarian cancer survivors. | Physiological status such as treatment-related adverse effects, comorbidities, body weight and composition, physical fitness and function, and participation in physical activity were defined. 10 BMI | Ovarian cancer survivors may benefit from physical activity and exercise interventions aimed at addressing the harms and changes in patients’ physiological status due to disease and treatment. However, gaps in knowledge regarding physiological characteristics across the survivorship spectrum currently remain and challenge the development of tailored exercise intervention studies and exercise oncology guidelines. | 6/11 |
| Jones et al. [15] | 2020 | Systematic Review | Number of studys: 34 | A systematic literature search was conducted using different databases such as PubMed, EMBASE, Scopus and CINAHL until 31 December 2019, to find out the possible benefits of physical activity and exercise in women with ovarian cancer. | 6 FACIT-F 7 FACT-G 13 PSQI 17 SF-36 18 FACT-O 33 EORTC QLQ-30 30 s sit-to-stand 34 6 MWT 35 MSAS-PHYS | The results obtained suggest that physical activity is relevant to the health of women with ovarian cancer, providing benefits and improvements in their lives. Furthermore, future work is needed to evaluate specific exercise interventions to ensure that the results obtained in this review can be translated into improved ovarian cancer care. | 10/11 |
| Newton et al. [25] | 2011 | Pilot study | 4 GP/P: 1 n = 17 | 4 GP/P: exercise performed at home. -Frequency: individualised according to the length of chemotherapy. Mostly 4 days/week. -Intensity: individualised (e.g., low at first, then increasing). -Type: Aerobic (walking). -Time: individualised. Mostly 30 min/session. - Supervision: 1 session/week with a specialist (face-to-face or by phone). (in person or by telephone). | 18 FACT-O 34 6 MWT 35 MSAS-PHYS 36 HADS Likert Scale | Significant improvements in physical functioning, symptoms, physical well-being and quality of life were found, suggesting that a walking intervention for women receiving chemotherapy for ovarian cancer is safe, feasible and acceptable and could be used to develop future studies. | 8/9 |
| Zhang et al. [22] | 2017 | Pilot study | 4 GP/P: 1 n = 10 | 4GP/P: home exercise. -Frequency: 26 weeks. -Intensity: moderate (Borg RPE 12–15). -Type: Aerobic (mainly walking, although cycling and cardiovascular training equipment were allowed). -Time: 225 min/week. -Supervision: - Week 1–6: face-to-face session/week with a certified trainer. - Week 7–26: face-to-face session/month with a certified trainer. | 10 BMI 12 Borg RPE Triaxial accelerometer ActiGraph GT3X Fitbit Zip | The results suggest that prescribing an exercise programme of 225 min per week to women with advanced ovarian cancer is feasible, safe and acceptable, although the need for a definitive clinical trial to evaluate the potential therapeutic effects of exercise on disease-related symptoms and endpoints among women with ovarian cancer is highlighted. | 9/9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sicardo Jiménez, S.; Vinolo-Gil, M.J.; Carmona-Barrientos, I.; Martin-Vega, F.J.; García-Muñoz, C.; Guillén Vargas, A.R.; Gonzalez-Medina, G. The Influence of Therapeutic Exercise on Survival and the Quality of Life in Survivorship of Women with Ovarian Cancer. Int. J. Environ. Res. Public Health 2022, 19, 16196. https://doi.org/10.3390/ijerph192316196
Sicardo Jiménez S, Vinolo-Gil MJ, Carmona-Barrientos I, Martin-Vega FJ, García-Muñoz C, Guillén Vargas AR, Gonzalez-Medina G. The Influence of Therapeutic Exercise on Survival and the Quality of Life in Survivorship of Women with Ovarian Cancer. International Journal of Environmental Research and Public Health. 2022; 19(23):16196. https://doi.org/10.3390/ijerph192316196
Chicago/Turabian StyleSicardo Jiménez, Sebastián, Maria Jesus Vinolo-Gil, Ines Carmona-Barrientos, Francisco Javier Martin-Vega, Cristina García-Muñoz, Antonio Rodrigo Guillén Vargas, and Gloria Gonzalez-Medina. 2022. "The Influence of Therapeutic Exercise on Survival and the Quality of Life in Survivorship of Women with Ovarian Cancer" International Journal of Environmental Research and Public Health 19, no. 23: 16196. https://doi.org/10.3390/ijerph192316196
APA StyleSicardo Jiménez, S., Vinolo-Gil, M. J., Carmona-Barrientos, I., Martin-Vega, F. J., García-Muñoz, C., Guillén Vargas, A. R., & Gonzalez-Medina, G. (2022). The Influence of Therapeutic Exercise on Survival and the Quality of Life in Survivorship of Women with Ovarian Cancer. International Journal of Environmental Research and Public Health, 19(23), 16196. https://doi.org/10.3390/ijerph192316196