
Comparison of Long COVID-19 Caused by Different SARS-CoV-2 Strains: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Methods
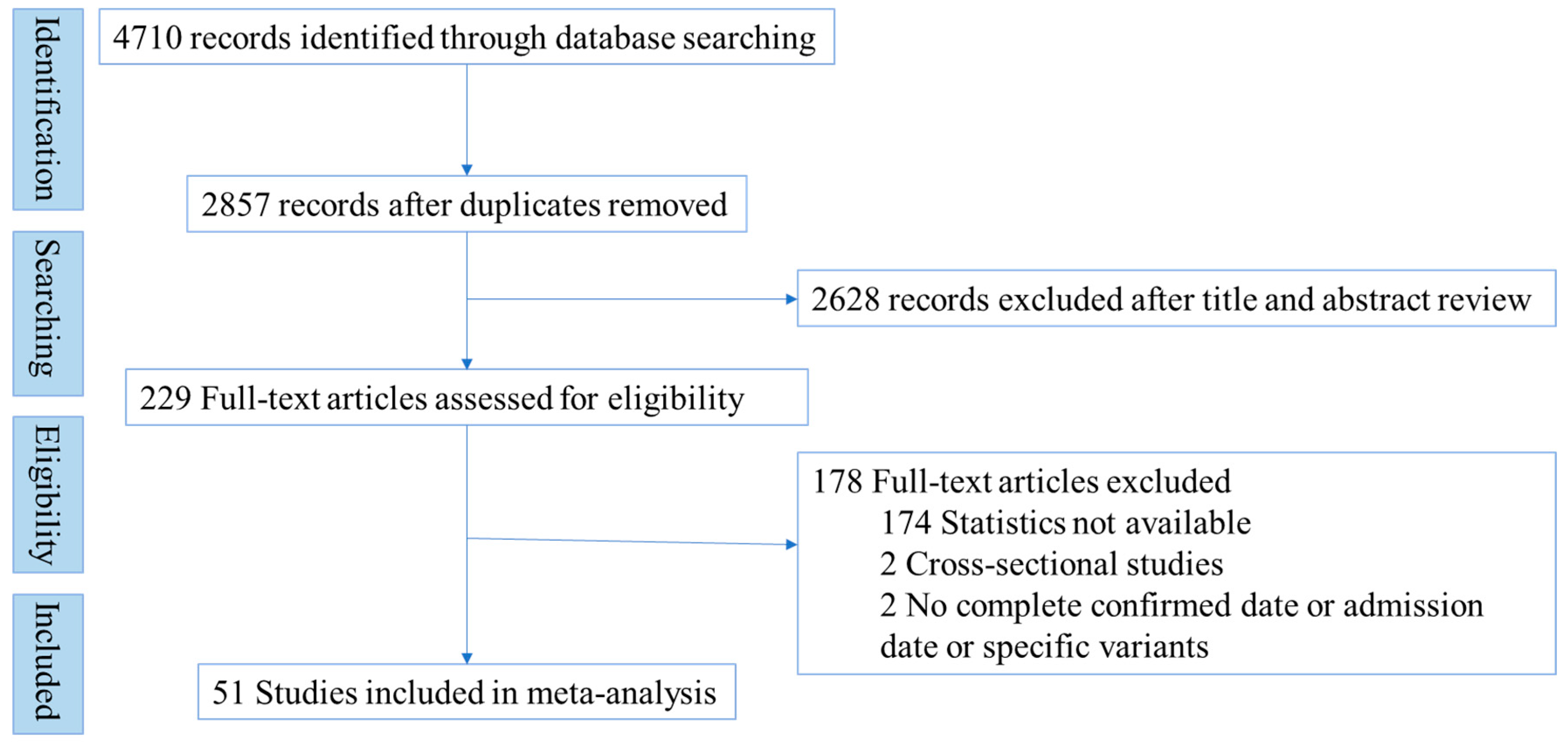
2.1. Search Strategy and Selection Criteria
- (P)
- Participants: the long COVID-19 patients;
- (I)
- Intervention: the different SARS-CoV-2 strains;
- (C)
- Comparison: not applicable;
- (O)
- Outcome measures: the long COVID-19 effects and related issues, including clinical features (general symptoms, respiratory symptoms, cardiovascular symptoms, gastrointestinal symptoms, neurological, and psychiatric symptoms), pulmonary functional test (PFT), chest computerized tomography (CT]), and quality of life.
2.2. Inclusion and Exclusion Criteria
2.3. Variants Identification and Data Extraction
2.4. Quality Assessment and Risk of Bias
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics
3.2. Pooled Estimates of Long COVID-19
3.3. Pooled Estimates of Long COVID-19 by Different Strains
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| WHO | World Health Organization |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| GISAID | Global Initiative of Sharing All Influenza Data |
| PRISMA | Preferred reporting items for systematic reviews and meta-analyses |
| PFT | Pulmonary functional test |
| CT | Computerized tomography |
| EQ-5D-5L | European Quality of Life Five-Dimension Five-Level Scale |
| PP | Pooled prevalence |
| CI | Confidence interval |
| DLCO | Carbon monoxide diffusing capacity |
| mMRC | Modified medical research council dyspnea scale |
| ICU | Intensive care unit |
References
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 18 May 2022).
- The, L. Facing up to long COVID. Lancet (Lond. Engl.) 2020, 396, 1861. [Google Scholar] [CrossRef]
- De Sire, A.; Moggio, L.; Marotta, N.; Agostini, F.; Tasselli, A.; Drago Ferrante, V.; Curci, C.; Calafiore, D.; Ferraro, F.; Bernetti, A.; et al. Impact of Rehabilitation on Fatigue in Post-COVID-19 Patients: A Systematic Review and Meta-Analysis. Appl. Sci. 2022, 12, 8593. [Google Scholar] [CrossRef]
- A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus, 6 October 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 22 April 2022).
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Sigfrid, L.; Drake, T.M.; Pauley, E.; Jesudason, E.C.; Olliaro, P.; Lim, W.S.; Gillesen, A.; Berry, C.; Lowe, D.J.; McPeake, J.; et al. Long Covid in adults discharged from UK hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO Clinical Characterisation Protocol. Lancet Reg. Health—Eur. 2021, 8, 100186. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Li, X.; Gu, X.; Zhang, H.; Ren, L.; Guo, L.; Liu, M.; Wang, Y.; Cui, D.; Wang, Y.; et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: A longitudinal cohort study. Lancet. Respir. Med. 2022, 10, 863–876. [Google Scholar] [CrossRef]
- Cohen, K.; Ren, S.; Heath, K.; Dasmariñas, M.C.; Jubilo, K.G.; Guo, Y.; Lipsitch, M.; Daugherty, S.E. Risk of persistent and new clinical sequelae among adults aged 65 years and older during the post-acute phase of SARS-CoV-2 infection: Retrospective cohort study. BMJ 2022, 376, e068414. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Long-Term Consequences of COVID-19 at 6 Months and Above: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6865. [Google Scholar] [CrossRef]
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 17 April 2022).
- US Centers for Disease Control and Prevention. SARS-CoV-2 Variant Classifications and Definitions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants (accessed on 27 November 2022).
- Duong, B.V.; Larpruenrudee, P.; Fang, T.; Hossain, S.I.; Saha, S.C.; Gu, Y.; Islam, M.S. Is the SARS CoV-2 Omicron Variant Deadlier and More Transmissible Than Delta Variant? Int. J. Environ. Res. Public Health 2022, 19, 4586. [Google Scholar] [CrossRef]
- Yu, W.; Guo, Y.; Zhang, S.; Kong, Y.; Shen, Z.; Zhang, J. Proportion of asymptomatic infection and nonsevere disease caused by SARS-CoV-2 Omicron variant: A systematic review and analysis. J. Med. Virol. 2022, 94, 5790–5801. [Google Scholar] [CrossRef]
- Emecen, A.N.; Keskin, S.; Turunc, O.; Suner, A.F.; Siyve, N.; Basoglu Sensoy, E.; Dinc, F.; Kilinc, O.; Avkan Oguz, V.; Bayrak, S.; et al. The presence of symptoms within 6 months after COVID-19: A single-center longitudinal study. Ir. J. Med. Sci. 2022, 10.1007/s11845-022-03072-0. [Google Scholar] [CrossRef] [PubMed]
- Peter, R.S.; Nieters, A.; Kräusslich, H.G.; Brockmann, S.O.; Göpel, S.; Kindle, G.; Merle, U.; Steinacker, J.M.; Rothenbacher, D.; Kern, W.V.; et al. Prevalence, determinants, and impact on general health and working capacity of post-acute sequelae of COVID-19 six to 12 months after infection: A population-based retrospective cohort study from southern Germany. medRxiv 2022. [Google Scholar] [CrossRef]
- Global Initiative of Sharing All Influenza Data (GISAID) Platform. Genomic Epidemiology of SARS-CoV-2 with Subsampling Focused Globally over the Past 6 Months. Available online: https://gisaid.org/phylodynamics/global/nextstrain/ (accessed on 10 September 2022).
- Todt, B.C.; Szlejf, C.; Duim, E.; Linhares, A.O.M.; Kogiso, D.; Varela, G.; Campos, B.A.; Baghelli Fonseca, C.M.; Polesso, L.E.; Bordon, I.N.S.; et al. Clinical outcomes and quality of life of COVID-19 survivors: A follow-up of 3 months post hospital discharge. Respir. Med. 2021, 184, 106453. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ (Clin. Res. Ed.) 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Och, A.; Tylicki, P.; Polewska, K.; Puchalska-Reglińska, E.; Parczewska, A.; Szabat, K.; Biedunkiewicz, B.; Dębska-ślizień, A.; Tylicki, L. Persistent post-covid-19 syndrome in hemodialyzed patients—A longitudinal cohort study from the North of Poland. J. Clin. Med. 2021, 10, 4451. [Google Scholar] [CrossRef]
- Lindahl, A.; Aro, M.; Reijula, J.; Mäkelä, M.J.; Ollgren, J.; Puolanne, M.; Järvinen, A.; Vasankari, T. Women report more symptoms and impaired quality of life: A survey of Finnish COVID-19 survivors. Infect. Dis. 2022, 54, 53–62. [Google Scholar] [CrossRef]
- Becker, C.; Beck, K.; Zumbrunn, S.; Memma, V.; Herzog, N.; Bissmann, B.; Gross, S.; Loretz, N.; Mueller, J.; Amacher, S.A.; et al. Long COVID 1 year after hospitalisation for COVID-19: A prospective bicentric cohort study. Swiss Med. Wkly. 2021, 151, w30091. [Google Scholar] [CrossRef]
- Dai, S.; Zhao, B.; Liu, D.; Zhou, Y.; Liu, Y.; Lan, L.; Li, Y.; Luo, W.; Zeng, Y.; Li, W. Follow-up study of the cardiopulmonary and psychological outcomes of covid-19 survivors six months after discharge in sichuan, china. Int. J. Gen. Med. 2021, 14, 7207–7217. [Google Scholar] [CrossRef]
- Caruso, D.; Guido, G.; Zerunian, M.; Polidori, T.; Lucertini, E.; Pucciarelli, F.; Polici, M.; Rucci, C.; Bracci, B.; Nicolai, M.; et al. Post-acute sequelae of COVID-19 pneumonia: Six-month chest CT follow-up. Radiology 2021, 301, E36–E405. [Google Scholar] [CrossRef]
- Bretas, D.C.; Leite, A.S.; Mancuzo, E.V.; Prata, T.A.; Andrade, B.H.; Oliveira, J.D.G.F.; Batista, A.P.; Machado-Coelho, G.L.L.; Augusto, V.M.; Marinho, C.C. Lung function six months after severe COVID-19: Does time, in fact, heal all wounds? Braz. J. Infect. Dis. 2022, 26, 102352. [Google Scholar] [CrossRef] [PubMed]
- Noviello, D.; Costantino, A.; Muscatello, A.; Bandera, A.; Consonni, D.; Vecchi, M.; Basilisco, G. Functional Gastrointestinal And Somatoform Symptoms Five Months After SARS-CoV-2 Infection: A Controlled Cohort Study. Dig. Liver Dis. 2021, 53, S119–S120. [Google Scholar] [CrossRef]
- Buonsenso, D.; Munblit, D.; Pazukhina, E.; Ricchiuto, A.; Sinatti, D.; Zona, M.; De Matteis, A.; D’Ilario, F.; Gentili, C.; Lanni, R.; et al. Post-COVID Condition in Adults and Children Living in the Same Household in Italy: A Prospective Cohort Study Using the ISARIC Global Follow-Up Protocol. Front. Pediatr. 2022, 10, 834875. [Google Scholar] [CrossRef] [PubMed]
- Zuschlag, D.; Grandt, D.; Custodis, F.; Braun, C.; Häuser, W. Spontaneously reported persistent symptoms related to coronavirus disease 2019 one year after hospital discharge: A retrospective cohort single-center study. Schmerz 2022, 36, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Menges, D.; Ballouz, T.; Anagnostopoulos, A.; Aschmann, H.E.; Domenghino, A.; Fehr, J.S.; Puhan, M.A. Burden of post-COVID-19 syndrome and implications for healthcare service planning: A population-based cohort study. PLoS ONE 2021, 16, e0254523. [Google Scholar] [CrossRef]
- Tessitore, E.; Handgraaf, S.; Poncet, A.; Achard, M.; Höfer, S.; Carballo, S.; Marti, C.; Follonier, C.; Girardin, F.; Mach, F.; et al. Symptoms and quality of life at 1-year follow up of patients discharged after an acute COVID-19 episode. Swiss Med. Wkly. 2021, 151, W30093. [Google Scholar] [CrossRef]
- Zhou, F.; Tao, M.; Shang, L.; Liu, Y.; Pan, G.; Jin, Y.; Wang, L.; Hu, S.; Li, J.; Zhang, M.; et al. Assessment of Sequelae of COVID-19 Nearly 1 Year After Diagnosis. Front. Med. 2021, 8, 717194. [Google Scholar] [CrossRef]
- Desgranges, F.; Tadini, E.; Munting, A.; Regina, J.; Filippidis, P.; Viala, B.; Karachalias, E.; Suttels, V.; Haefliger, D.; Kampouri, E.; et al. Post-COVID-19 Syndrome in Outpatients: A Cohort Study. J. Gen. Intern. Med. 2022, 37, 1943–1952. [Google Scholar] [CrossRef]
- Förster, C.; Colombo, M.G.; Wetzel, A.J.; Martus, P.; Joos, S. Persisting Symptoms after COVID-19: Prevalence and Risk Factors in a Population-Based Cohort. Dtsch. Arztebl. Int. 2022, 119, 167–174. [Google Scholar] [CrossRef]
- Nesan, G.S.C.Q.; Keerthana, D.; Yamini, R.; Jain, T.; Kumar, D.; Eashwer, A.; Maiya, G.R. 3-Month Symptom-Based Ambidirectional Follow-up Study Among Recovered COVID-19 Patients from a Tertiary Care Hospital Using Telehealth in Chennai, India. Inq. A J. Med. Care Organ. Provis. Financ. 2021, 58, 469580211060165. [Google Scholar] [CrossRef]
- Prestes, G.D.S.; Simon, C.S.; Walz, R.; Ritter, C.; Dal-Pizzol, F. Respiratory Outcomes After 6 Months of Hospital Discharge in Patients Affected by COVID-19: A Prospective Cohort. Front. Med. 2022, 9, 795074. [Google Scholar] [CrossRef]
- Calcaianu, G.; Degoul, S.; Michau, B.; Payen, T.; Gschwend, A.; Fore, M.; Iamandi, C.; Morel, H.; Oster, J.-P.; Bizieux, A.; et al. Mid-term pulmonary sequelae after hospitalisation for COVID-19: The French SISCOVID cohort. Respir. Med. Res. 2022, 82, 100933. [Google Scholar] [CrossRef] [PubMed]
- Vargas Centanaro, G.; Calle Rubio, M.; Álvarez-Sala Walther, J.L.; Martinez-Sagasti, F.; Albuja Hidalgo, A.; Herranz Hernández, R.; Rodríguez Hermosa, J.L. Long-term Outcomes and Recovery of Patients who Survived COVID-19: LUNG INJURY COVID-19 Study. Open Forum Infect. Dis. 2022, 9, ofac098. [Google Scholar] [CrossRef] [PubMed]
- Labarca, G.; Henríquez-Beltrán, M.; Lastra, J.; Enos, D.; Llerena, F.; Cigarroa, I.; Lamperti, L.; Ormazabal, V.; Ramirez, C.; Espejo, E.; et al. Analysis of clinical symptoms, radiological changes and pulmonary function data 4 months after COVID-19. Clin. Respir. J. 2021, 15, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- Klein, H.; Asseo, K.; Karni, N.; Benjamini, Y.; Nir-Paz, R.; Muszkat, M.; Israel, S.; Niv, M.Y. Onset, duration and unresolved symptoms, including smell and taste changes, in mild COVID-19 infection: A cohort study in Israeli patients. Clin. Microbiol. Infect. 2021, 27, 769–774. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; Motos, A.; Menéndez, R.; Gabarrús, A.; González, J.; Fernández-Barat, L.; Ceccato, A.; Pérez-Arnal, R.; García-Gasulla, D.; Ferrer, R.; et al. ICU-Acquired Pneumonia Is Associated with Poor Health Post-COVID-19 Syndrome. J. Clin. Med. 2022, 11, 224. [Google Scholar] [CrossRef]
- González, J.; Benítez, I.D.; Carmona, P.; Santisteve, S.; Monge, A.; Moncusí-Moix, A.; Gort-Paniello, C.; Pinilla, L.; Carratalá, A.; Zuil, M.; et al. Pulmonary Function and Radiologic Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort. Chest 2021, 160, 187–198. [Google Scholar] [CrossRef]
- Aranda, J.; Oriol, I.; Martín, M.; Feria, L.; Vázquez, N.; Rhyman, N.; Vall-Llosera, E.; Pallarés, N.; Coloma, A.; Pestaña, M.; et al. Long-term impact of COVID-19 associated acute respiratory distress syndrome. J. Infect. 2021, 83, 581–588. [Google Scholar] [CrossRef]
- Zhang, J.; Shu, T.; Zhu, R.; Yang, F.; Zhang, B.; Lai, X. The Long-Term Effect of COVID-19 Disease Severity on Risk of Diabetes Incidence and the Near 1-Year Follow-Up Outcomes among Postdischarge Patients in Wuhan. J. Clin. Med. 2022, 11, 3094. [Google Scholar] [CrossRef]
- Kingery, J.R.; Safford, M.M.; Martin, P.; Lau, J.D.; Rajan, M.; Wehmeyer, G.T.; Li, H.A.; Alshak, M.N.; Jabri, A.; Kofman, A.; et al. Health Status, Persistent Symptoms, and Effort Intolerance One Year After Acute COVID-19 Infection. J. Gen. Intern. Med. 2022, 37, 1218–1225. [Google Scholar] [CrossRef]
- Zhan, K.; Zhang, X.; Wang, B.; Jiang, Z.; Fang, X.; Yang, S.; Jia, H.; Li, L.; Cao, G.; Zhang, K.; et al. Short-and long-term prognosis of glycemic control in COVID-19 patients with type 2 diabetes. QJM 2022, 115, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Miskowiak, K.W.; Fugledalen, L.; Jespersen, A.E.; Sattler, S.M.; Podlekareva, D.; Rungby, J.; Porsberg, C.M.; Johnsen, S. Trajectory of cognitive impairments over 1 year after COVID-19 hospitalisation: Pattern, severity, and functional implications. Eur. Neuropsychopharmacol. 2022, 59, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Peghin, M.; Palese, A.; Venturini, M.; De Martino, M.; Gerussi, V.; Graziano, E.; Bontempo, G.; Marrella, F.; Tommasini, A.; Fabris, M.; et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin. Microbiol. Infect. 2021, 27, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Colizzi, M.; Peghin, M.; De Martino, M.; Bontempo, G.; Gerussi, V.; Palese, A.; Isola, M.; Tascini, C.; Balestrieri, M. Mental health symptoms one year after acute COVID-19 infection: Prevalence and risk factors. Rev. Psiquiatr. Salud Ment. 2022. [Google Scholar] [CrossRef] [PubMed]
- Vejen, M.; Hansen, E.F.; Al-Jarah, B.N.I.; Jensen, C.; Thaning, P.; Jeschke, K.N.; Ulrik, C.S. Hospital admission for COVID-19 pneumonitis—Long-term impairment in quality of life and lung function. Eur. Clin. Respir. J. 2022, 9, 2024735. [Google Scholar] [CrossRef] [PubMed]
- Aiello, M.; Marchi, L.; Calzetta, L.; Speroni, S.; Frizzelli, A.; Ghirardini, M.; Celiberti, V.; Sverzellati, N.; Majori, M.; Mori, P.A.; et al. Coronavirus Disease 2019: COSeSco—A Risk Assessment Score to Predict the Risk of Pulmonary Sequelae in COVID-19 Patients. Respiration 2021, 101, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Izquierdo, M.; Láinez-Ramos-Bossini, A.J.; de Alba, I.G.; Ortiz-González-Serna, R.; Serrano-Ortiz, Á.; Fernández-Martínez, N.F.; Ruiz-Montero, R.; Cervilla, J.A. Long COVID 12 months after discharge: Persistent symptoms in patients hospitalised due to COVID-19 and patients hospitalised due to other causes-a multicentre cohort study. BMC Med. 2022, 20, 92. [Google Scholar] [CrossRef]
- Rigoni, M.; Torri, E.; Nollo, G.; Donne, L.D.; Rizzardo, S.; Lenzi, L.; Falzone, A.; Cozzio, S. "Long COVID" results after hospitalization for SARS-CoV-2 infection. Sci. Rep. 2022, 12, 9581. [Google Scholar] [CrossRef]
- Mølhave, M.; Leth, S.; Gunst, J.D.; Jensen-Fangel, S.; Østergaard, L.; Wejse, C.; Agergaard, J. Long-term symptoms among hospitalized COVID-19 patients 48 weeks after discharge—A prospective cohort study. J. Clin. Med. 2021, 10, 5298. [Google Scholar] [CrossRef]
- Porto, M.H.; Delgado, T.; Aguirre-Jaime, A.; Ramos, M.J.; Campos, S.; Acosta, O.; Llanos, A.B.; Lecuona, M. Patients at risk of pulmonary fibrosis Post COVID-19: Epidemiology, pulmonary sequelaes and humoral response. medRxiv 2022. [Google Scholar] [CrossRef]
- Attauabi, M.; Dahlerup, J.F.; Poulsen, A.; Hansen, M.R.; Vester-Andersen, M.K.; Eraslan, S.; Prahm, A.P.; Pedersen, N.; Larsen, L.; Jess, T.; et al. Outcomes and Long-Term Effects of COVID-19 in Patients with Inflammatory Bowel Diseases—A Danish Prospective Population-Based Cohort Study with Individual-Level Data. J. Crohn’s Colitis 2022, 16, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.A.; Hossain, K.M.A.; Saunders, K.; Uddin, Z.; Walton, L.M.; Raigangar, V.; Sakel, M.; Shafin, R.; Hossain, M.S.; Kabir, M.F.; et al. Prevalence of Long COVID symptoms in Bangladesh: A prospective Inception Cohort Study of COVID-19 survivors. BMJ Glob. Health 2021, 6, 006838. [Google Scholar] [CrossRef]
- Eloy, P.; Tardivon, C.; Martin-Blondel, G.; Isnard, M.; Turnier, P.L.; Marechal, M.L.; CabiÉ, A.; Launay, O.; Tattevin, P.; Senneville, E.; et al. Severity of self-reported symptoms and psychological burden 6-months after hospital admission for COVID-19: A prospective cohort study. Int. J. Infect. Dis. 2021, 112, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Duggal, P.; Penson, T.; Manley, H.N.; Vergara, C.; Munday, R.M.; Duchen, D.; Linton, E.A.; Zurn, A.; Keruly, J.C.; Mehta, S.H.; et al. Post-sequelae symptoms and comorbidities after COVID-19. J. Med. Virol. 2022, 94, 2060–2066. [Google Scholar] [CrossRef] [PubMed]
- Mónica, R.-S.; Maribel, Q.-F.; Javier, J.; Isabel, L.-M.; Rocío, T.; Rocío, A.; Javier, G.-P.F. Cardiac complications in a geriatric population hospitalized with COVID-19: The OCTA-COVID cohort. Rev. Española Geriatría Gerontol. 2022, 57, 63–70. [Google Scholar] [CrossRef]
- Robey, R.C.; Kemp, K.; Hayton, P.; Mudawi, D.; Wang, R.; Greaves, M.; Yioe, V.; Rivera-Ortega, P.; Avram, C.; Chaudhuri, N. Pulmonary Sequelae at 4 Months After COVID-19 Infection: A Single-Centre Experience of a COVID Follow-Up Service. Adv. Ther. 2021, 38, 4505–4519. [Google Scholar] [CrossRef]
- Titze-de-Almeida, R.; da Cunha, T.R.; dos Santos Silva, L.D.; Ferreira, C.S.; Silva, C.P.; Ribeiro, A.P.; de Castro Moreira Santos Júnior, A.; de Paula Brandão, P.R.; Silva, A.P.B.; da Rocha, M.C.O.; et al. Persistent, new-onset symptoms and mental health complaints in Long COVID in a Brazilian cohort of non-hospitalized patients. BMC Infect. Dis. 2022, 22, 133. [Google Scholar] [CrossRef]
- Zayet, S.; Zahra, H.; Royer, P.Y.; Tipirdamaz, C.; Mercier, J.; Gendrin, V.; Lepiller, Q.; Marty-Quinternet, S.; Osman, M.; Belfeki, N.; et al. Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comté Hospital, France. Microorganisms 2021, 9, 1719. [Google Scholar] [CrossRef]
- Liao, X.; Li, D.; Liu, Z.; Ma, Z.; Zhang, L.; Dong, J.; Shi, Y.; Gu, X.; Zheng, G.; Huang, L.; et al. Pulmonary Sequelae in Patients After Recovery From Coronavirus Disease 2019: A Follow-Up Study With Chest CT. Front. Med. 2021, 8, 686878. [Google Scholar] [CrossRef]
- Li, Y.; Han, X.; Huang, J.; Alwalid, O.; Jia, X.; Yuan, M.; Cao, Y.; Shao, G.; Cui, Y.; Liu, J.; et al. Follow-up study of pulmonary sequelae in discharged COVID-19 patients with diabetes or secondary hyperglycemia. Eur. J. Radiol. 2021, 144, 109997. [Google Scholar] [CrossRef]
- Aparisi, Á.; Ybarra-Falcón, C.; García-Gómez, M.; Tobar, J.; Iglesias-Echeverría, C.; Jaurrieta-Largo, S.; Ladrón, R.; Uribarri, A.; Catalá, P.; Hinojosa, W.; et al. Exercise Ventilatory Inefficiency in Post-COVID-19 Syndrome: Insights from a Prospective Evaluation. J. Clin. Med. 2021, 10, 2591. [Google Scholar] [CrossRef]
- Romero-Duarte, Á.; Rivera-Izquierdo, M.; Guerrero-Fernández de Alba, I.; Pérez-Contreras, M.; Fernández-Martínez, N.F.; Ruiz-Montero, R.; Serrano-Ortiz, Á.; González-Serna, R.O.; Salcedo-Leal, I.; Jiménez-Mejías, E.; et al. Sequelae, persistent symptomatology and outcomes after COVID-19 hospitalization: The ANCOHVID multicentre 6-month follow-up study. BMC Med. 2021, 19, 129. [Google Scholar] [CrossRef] [PubMed]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, 28568. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.L.; Lely, A.T.; Navis, G.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (Lond. Engl.) 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet (Lond. Engl.) 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 24 September 2022).
- Kow, C.S.; Ramachandram, D.S.; Hasan, S.S. The effectiveness of mRNA-1273 vaccine against COVID-19 caused by Delta variant: A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 2269–2274. [Google Scholar] [CrossRef]
- Külper-Schiek, W.; Piechotta, V.; Pilic, A.; Batke, M.; Dreveton, L.S.; Geurts, B.; Koch, J.; Köppe, S.; Treskova, M.; Vygen-Bonnet, S.; et al. Facing the Omicron variant-how well do vaccines protect against mild and severe COVID-19? Third interim analysis of a living systematic review. Front. Immunol. 2022, 13, 940562. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef]
- Peghin, M.; De Martino, M.; Palese, A.; Gerussi, V.; Bontempo, G.; Graziano, E.; Visintini, E.; D’Elia, D.; Dellai, F.; Marrella, F.; et al. Post-COVID-19 syndrome and humoral response association after 1 year in vaccinated and unvaccinated patients. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2022, 28, 1140–1148. [Google Scholar] [CrossRef]
- Wu, Y.; Kang, L.; Guo, Z.; Liu, J.; Liu, M.; Liang, W. Incubation Period of COVID-19 Caused by Unique SARS-CoV-2 Strains: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2228008. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Consequences | Number of Studies | Patients n/N | PP (95% CI, %) | p-Value | I2 |
|---|---|---|---|---|---|
| General Symptoms | |||||
| ≥1 symptoms | |||||
| Alpha | 3 | 475/779 | 65.8 (47.7, 83.9) | <0.05 | 96.8% |
| Delta | 1 | 56/162 | 34.6 (27.2, 41.9) | <0.05 | - |
| Omicron | 2 | 931/4860 | 28.4 (7.9, 49.0) | <0.05 | 97.5% |
| Wild-type | 18 | 3659/7069 | 52.1 (44.0, 60.1) | <0.05 | 98.0% |
| Fever or Feverishness | |||||
| Alpha | 1 | 10/324 | 3.1 (1.2, 5.0) | <0.05 | - |
| Omicron | 3 | 178/11,535 | 8.0 (−1.7, 17.7) | >0.05 | 95.2% |
| Wild-type | 9 | 101/3681 | 2.6 (1.3, 3.8) | <0.05 | 90.9% |
| Fatigue | |||||
| Alpha | 3 | 494/760 | 66.1 (42.2, 89.9) | <0.05 | 98.1% |
| Beta | 1 | 295/2198 | 13.4 (12.0, 14.8) | <0.05 | - |
| Delta | 1 | 40/162 | 24.7 (18.1, 31.3) | <0.05 | - |
| Omicron | 2 | 3457/15,848 | 18.1 (0.4, 35.8) | <0.05 | 99.9% |
| Wild-type | 19 | 1234/6094 | 26.3 (20.7, 31.9) | <0.05 | 97.3% |
| Muscle weakness | |||||
| Delta | 1 | 42/1354 | 3.1 (2.2, 4.0) | <0.05 | - |
| Omicron | 1 | 30/245 | 12.2 (8.1, 16.3) | <0.05 | - |
| Wild-type | 4 | 70/1730 | 4.2 (1.5, 6.9) | <0.05 | 87.7% |
| Myalgia | |||||
| Alpha | 1 | 74/324 | 22.8 (18.3, 27.4) | <0.05 | - |
| Delta | 1 | 69/1354 | 5.1 (3.9, 6.3) | <0.05 | - |
| Omicron | 3 | 1346/11,539 | 11.7 (8.3, 15.1) | <0.05 | 64.8% |
| Wild-type | 11 | 235/2727 | 9.4 (6.3, 12.5) | <0.05 | 96.0% |
| Joint pain or arthralgia | |||||
| Alpha | 1 | 53/301 | 17.6 (13.3, 21.9) | <0.05 | - |
| Omicron | 4 | 2124/11,732 | 14.9 (8.3, 21.4) | <0.05 | 93.4% |
| Wild-type | 4 | 152/602 | 24.3 (6.6, 42.0) | <0.05 | 95.8% |
| Headache | |||||
| Alpha | 1 | 45/324 | 65.8 (47.7, 83.9) | <0.05 | - |
| Beta | 1 | 8/2198 | 34.6 (27.2, 41.9) | <0.05 | - |
| Delta | 5 | 32/1516 | 28.4 (7.9, 49.0) | <0.05 | 82.1% |
| Omicron | 5 | 3276/16,157 | 52.1 (44.0, 60.1) | <0.05 | 99.9% |
| Wild-type | 1 | 624/7604 | 10.0 (7.6, 12.4) | <0.05 | 95.8% |
| Dizziness or Vertigo | |||||
| Delta | 1 | 1/162 | 0.6 (−0.6, 1.8) | >0.05 | - |
| Omicron | 3 | 2023/6074 | 1.6 (−0.8, 4.0) | >0.05 | 90.1% |
| Wild-type | 6 | 175/3098 | 5.9 (2.7, 9.2) | <0.05 | 96.7% |
| Olfactory abnormalities | |||||
| Omicron | 4 | 2651/16,123 | 10.2 (−3.2, 23.6) | >0.05 | 99.8% |
| Wild-type | 4 | 46/773 | 7.0 (2.7, 11.4) | <0.05 | 84.7% |
| Olfactory loss | |||||
| Delta | 1 | 23/1354 | 1.7 (1.0, 2.4) | <0.05 | - |
| Omicron | 1 | 62/222 | 27.9 (22.0, 33.8) | <0.05 | - |
| Wild-type | 9 | 418/3725 | 13.1 (8.5, 17.8) | <0.05 | 95.1% |
| Taste abnormalities | |||||
| Omicron | 4 | 2030/16,090 | 8.7 (−2.3, 19.7) | >0.05 | 99.8% |
| Wild-type | 3 | 40/703 | 7.1 (1.0, 13.2) | <0.05 | 90.9% |
| Taste loss | |||||
| Alpha | 1 | 21/301 | 7.0 (4.1, 9.9) | <0.05 | - |
| Beta | 1 | 12/2198 | 0.5 (0.2, 0.9) | <0.05 | - |
| Delta | 1 | 34/1354 | 2.5 (1.7, 3.3) | <0.05 | - |
| Omicron | 1 | 50/222 | 22.5 (17.0, 28.0) | <0.05 | - |
| Wild-type | 7 | 328/3515 | 10.4 (6.1, 14.6) | <0.05 | 94.4% |
| Hair loss | |||||
| Omicron | 2 | 1572/11,019 | 18.2 (8.2, 28.2) | <0.05 | 76.6% |
| Wild-type | 7 | 209/3018 | 6.8 (3.4, 10.1) | <0.05 | 94.2% |
| Cutaneous or Skin disorders | |||||
| Wild-type | 6 | 156/3738 | 3.9 (2.1, 5.7) | <0.05 | 88.3% |
| Rash | 5 | 666/16,548 | 3.3 (0.4, 6.1) | <0.05 | 99.3% |
| Omicron | 4 | 665/16,204 | 4.2 (0.3, 8.1) | <0.05 | 99.5% |
| Wild-type | 1 | 1/344 | 0.3 (-0.3, 0.9) | >0.05 | - |
| Respiratory symptoms | |||||
| Cough | |||||
| Alpha | 2 | 87/452 | 23.7 (2.0, 45.5) | <0.05 | 95.7% |
| Delta | 1 | 3/162 | 1.9 (−0.2, 3.9) | >0.05 | - |
| Gamma | 1 | 34/156 | 21.8 (15.3, 28.3) | <0.05 | - |
| Omicron | 2 | 1470/15,768 | 6.8 (−5.1, 18.7) | >0.05 | 99.9% |
| Wild-type | 21 | 853/7691 | 13.4 (10.4, 16.5) | <0.05 | 97.4% |
| Dyspnea | |||||
| Alpha | 2 | 125/429 | 34.2 (8.3, 60.1) | <0.05 | 96.4% |
| Beta | 1 | 37/2197 | 1.7 (1.1, 2.2) | <0.05 | - |
| Delta | 1 | 14/1354 | 1.0 (0.5, 1.6) | <0.05 | - |
| Gamma | 1 | 68/158 | 43.0 (35.3, 50.8) | <0.05 | - |
| Omicron | 2 | 177/4860 | 9.2 (−3.3, 21.6) | >0.05 | 96.3% |
| Wild-type | 20 | 1684/7469 | 23.3 (16.2, 30.5) | <0.05 | 98.9% |
| Expectoration | |||||
| Wild-type | 5 | 80/998 | 7.5 (2.9, 12.1) | <0.05 | 94.8% |
| Nasal congestion | |||||
| Alpha | 1 | 52/324 | 16.0 (12.1, 20.0) | <0.05 | - |
| Omicron | 1 | 18/4638 | 0.4 (0.2, 0.6) | <0.05 | - |
| Wild-type | 5 | 35/1049 | 2.8 (0.4, 5.1) | <0.05 | 85.5% |
| Sore throat | |||||
| Alpha | 1 | 19/324 | 5.9 (3.3, 8.4) | <0.05 | - |
| Delta | 1 | 9/1354 | 0.7 (0.2, 1.1) | <0.05 | - |
| Omicron | 2 | 991/15,846 | 4.5 (−3.7, 12.7) | >0.05 | 99.9% |
| Wild-type | 3 | 26/635 | 4.3 (0.9, 7.8) | <0.05 | 73.0% |
| mMRC = 0 | |||||
| Alpha | 1 | 97/312 | 31.1 (26.0, 36.2) | <0.05 | - |
| Wild-type | 5 | 702/1005 | 54.7 (33.9, 75.5) | <0.05 | 98.3% |
| mMRC ≥ 1 | |||||
| Alpha | 1 | 215/312 | 68.9 (63.8, 74.0) | <0.05 | - |
| Omicron | 1 | 25/73 | 34.2 (23.4, 45.1) | <0.05 | - |
| Wild-type | 6 | 350/1125 | 44.1 (26.3, 62.0) | <0.05 | 97.9% |
| Cardiovascular symptoms | |||||
| Short Breath | |||||
| Alpha | 1 | 175/327 | 53.5 (48.1, 58.9) | <0.05 | - |
| Delta | 1 | 14/162 | 8.6 (4.3, 13.0) | <0.05 | - |
| Omicron | 1 | 3444/11,183 | 30.8 (29.9, 31.7) | <0.05 | - |
| Wild-type | 5 | 215/1530 | 17.6 (9.5, 25.8) | <0.05 | 96.5% |
| Palpitations | |||||
| Delta | 1 | 7/1354 | 0.5 (0.1, 0.9) | <0.05 | 96.8% |
| Omicron | 3 | 87/4956 | 5.9 (1.1, 10.7) | <0.05 | - |
| Wild-type | 9 | 191/3454 | 5.7 (3.2, 8.3) | <0.05 | 97.5% |
| Gastrointestinal symptoms | |||||
| ≥1 symptoms | |||||
| Wild-type | 5 | 35/1603 | 1.8 (0.2, 3.3) | <0.05 | 84.3% |
| Loss of appetite | |||||
| Delta | 2 | 53/1516 | 2.2 (−0.9, 5.4) | >0.05 | 93.7% |
| Omicron | 2 | 26/318 | 11.9 (−3.8, 27.6) | >0.05 | 90.6% |
| Wild-type | 4 | 28/876 | 3.0 (0.7, 5.3) | <0.05 | 74.6% |
| Nausea | |||||
| Delta | 1 | 1/162 | 0.6 (−0.6, 1.8) | >0.05 | - |
| Omicron | 2 | 505/11,353 | 15.3 (−7.3, 37.9) | >0.05 | 94.9% |
| Wild-type | 3 | 14/710 | 1.5 (−0.5, 3.5) | >0.05 | 75.9% |
| Diarrhea | |||||
| Omicron | 2 | 505/11,353 | 4.4 (−1.5, 10.2) | >0.05 | 70.8% |
| Wild-type | 8 | 14/710 | 2.5 (1.0, 3.9) | <0.05 | 92.5% |
| Abdominal pain | |||||
| Omicron | 3 | 636/16,163 | 3.2 (−1.1, 7.5) | >0.05 | 99.7% |
| Wild-type | 6 | 58/2164 | 2.0 (0.5, 3.5) | <0.05 | 87.4% |
| Constipation | |||||
| Delta | 1 | 35/1354 | 2.6 (1.7, 3.4) | <0.05 | - |
| Omicron | 1 | 26/245 | 10.6 (6.8, 14.5) | <0.05 | - |
| Wild-type | 3 | 38/1370 | 3.1 (0.4, 5.8) | <0.05 | 92.2% |
| Neurological and psychiatric symptoms | |||||
| ≥1 symptoms | |||||
| Wild-type | 8 | 371/2950 | 13.8 (8.5, 19.2) | <0.05 | 95.7% |
| Paresthesias | |||||
| Delta | 1 | 6/1354 | 0.4 (0.1, 0.8) | <0.05 | - |
| Omicron | 1 | 1337/11,236 | 11.9 (11.3, 12.5) | <0.05 | - |
| Wild-type | 7 | 161/1773 | 12.7 (7.7, 17.7) | <0.05 | 95.1% |
| Memory problem | |||||
| Omicron | 1 | 1794/11,174 | 16.1 (15.4, 16.7) | <0.05 | - |
| Wild-type | 6 | 225/1489 | 17.3 (8.7, 25.9) | <0.05 | 97.2% |
| Sleep difficulty | |||||
| Alpha | 1 | 151/327 | 46.2 (40.8, 51.6) | <0.05 | - |
| Delta | 2 | 51/1516 | 2.5 (0.2, 4.9) | <0.05 | 82.2% |
| Omicron | 4 | 3082/16,211 | 18.7 (1.0, 36.5) | <0.05 | 99.9% |
| Wild-type | 11 | 474/3067 | 24.5 (17.5, 31.5) | <0.05 | 98.5% |
| Depression | 1 | ||||
| Delta | 1 | 1/162 | 0.6 (−0.6, 1.8) | >0.05 | - |
| Omicron | 1 | 2274/11,149 | 20.4 (19.6, 21.1) | <0.05 | - |
| Wild-type | 9 | 411/3585 | 19.7 (10.1, 29.4) | <0.05 | 99.1% |
| Anxiety | |||||
| Delta | 1 | 1/162 | 0.6 (−0.6, 1.8) | >0.05 | - |
| Omicron | 1 | 1196/11,174 | 10.7 (10.1, 11.3) | <0.05 | - |
| Wild-type | 11 | 442/3134 | 15.3 (9.7, 20.8) | <0.05 | 96.8% |
| Difficulty concentrating | |||||
| Omicron | 2 | 3542/15,817 | 16.0 (−14.5, 46.4) | >0.05 | 100.0% |
| Wild-type | 6 | 370/2276 | 23.3 (14.9, 31.6) | <0.05 | 96.1% |
| PFT | |||||
| FEV1 < 80% | |||||
| Alpha | 1 | 31/123 | 25.2 (17.5, 32.9) | <0.05 | - |
| Wild-type | 4 | 39/302 | 13.4 (7.0, 19.9) | <0.05 | 62.9% |
| TLC < 80% | |||||
| Alpha | 1 | 30/111 | 27.0 (18.8, 35.3) | <0.05 | - |
| Delta | 1 | 76/121 | 62.8 (54.2, 71.4) | <0.05 | - |
| Wild-type | 4 | 98/596 | 17.2 (8.6, 25.8) | <0.05 | 87.8% |
| DLCO < 80% | |||||
| Alpha | 1 | 50/111 | 45.0 (35.8, 54.3) | <0.05 | - |
| Wild-type | 5 | 816/1302 | 59.2 (40.4, 78.1) | <0.05 | 96.7% |
| CT results | |||||
| CT abnormalities | |||||
| Wild-type | 11 | 1540/2206 | 60.5 (40.4, 80.6) | <0.05 | 99.2% |
| GGO | |||||
| Wild-type | 12 | 403/1231 | 38.9 (26.8, 51.0) | <0.05 | 95.7% |
| Consolidation | |||||
| Wild-type | 5 | 21/388 | 5.4 (0.8, 9.9) | <0.05 | 80.6% |
| Fibrosis | |||||
| Wild-type | 9 | 340/1790 | 24.4 (13.3, 35.4) | <0.05 | 96.3% |
| Bronchiectasis | |||||
| Wild-type | 7 | 195/892 | 22.2 (9.7, 34.7) | <0.05 | 96.6% |
| EQ-5D-5L | |||||
| Mobility | |||||
| Alpha | 1 | 65/128 | 50.8 (42.1, 59.4) | <0.05 | - |
| Omicron | 1 | 28/73 | 38.4 (27.2, 49.5) | <0.05 | - |
| Wild-type | 3 | 99/837 | 11.7 (9.5, 13.9) | <0.05 | 0.0% |
| Personal care | |||||
| Omicron | 1 | 28/73 | 68.5 (57.8, 79.1) | <0.05 | - |
| Wild-type | 3 | 99/837 | 2.8 (−0.3, 6.0) | >0.05 | 88.5% |
| Usual activity | |||||
| Alpha | 1 | 69/128 | 53.9 (45.3, 62.5) | <0.05 | - |
| Omicron | 1 | 37/73 | 50.7 (39.2, 62.2) | <0.05 | - |
| Wild-type | 2 | 79/595 | 15.2 (5.2, 25.1) | <0.05 | 88.2% |
| Pain or discomfort | |||||
| Alpha | 1 | 78/128 | 60.9 (52.5, 69.4) | <0.05 | - |
| Omicron | 1 | 52/73 | 71.2 (60.8, 81.6) | <0.05 | - |
| Wild-type | 3 | 300/838 | 37.2 (30.1, 44.3) | <0.05 | 76.9% |
| Anxiety and depression | |||||
| Omicron | 1 | 53/73 | 72.6 (62.4, 82.8) | <0.05 | - |
| Wild-type | 4 | 724/941 | 28.0 (7.0, 49.0) | <0.05 | 98.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, M.; Ma, Y.; Deng, J.; Liu, M.; Liu, J. Comparison of Long COVID-19 Caused by Different SARS-CoV-2 Strains: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 16010. https://doi.org/10.3390/ijerph192316010
Du M, Ma Y, Deng J, Liu M, Liu J. Comparison of Long COVID-19 Caused by Different SARS-CoV-2 Strains: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(23):16010. https://doi.org/10.3390/ijerph192316010
Chicago/Turabian StyleDu, Min, Yirui Ma, Jie Deng, Min Liu, and Jue Liu. 2022. "Comparison of Long COVID-19 Caused by Different SARS-CoV-2 Strains: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 23: 16010. https://doi.org/10.3390/ijerph192316010
APA StyleDu, M., Ma, Y., Deng, J., Liu, M., & Liu, J. (2022). Comparison of Long COVID-19 Caused by Different SARS-CoV-2 Strains: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(23), 16010. https://doi.org/10.3390/ijerph192316010