

Combined Training with Aerobic Exercise Performed Outdoors Can Promote Better Blood Pressure and Affective Responses in Individuals with Cardiovascular Risk Factors

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Recruitment and Participants
2.3. Experimental Procedures
2.4. Allocation
2.5. Evaluations
2.5.1. Sample Characterization
2.5.2. Blood Pressure Measurement
2.5.3. Training Internal Load Measurement
2.5.4. Affective Response to Training Measurement
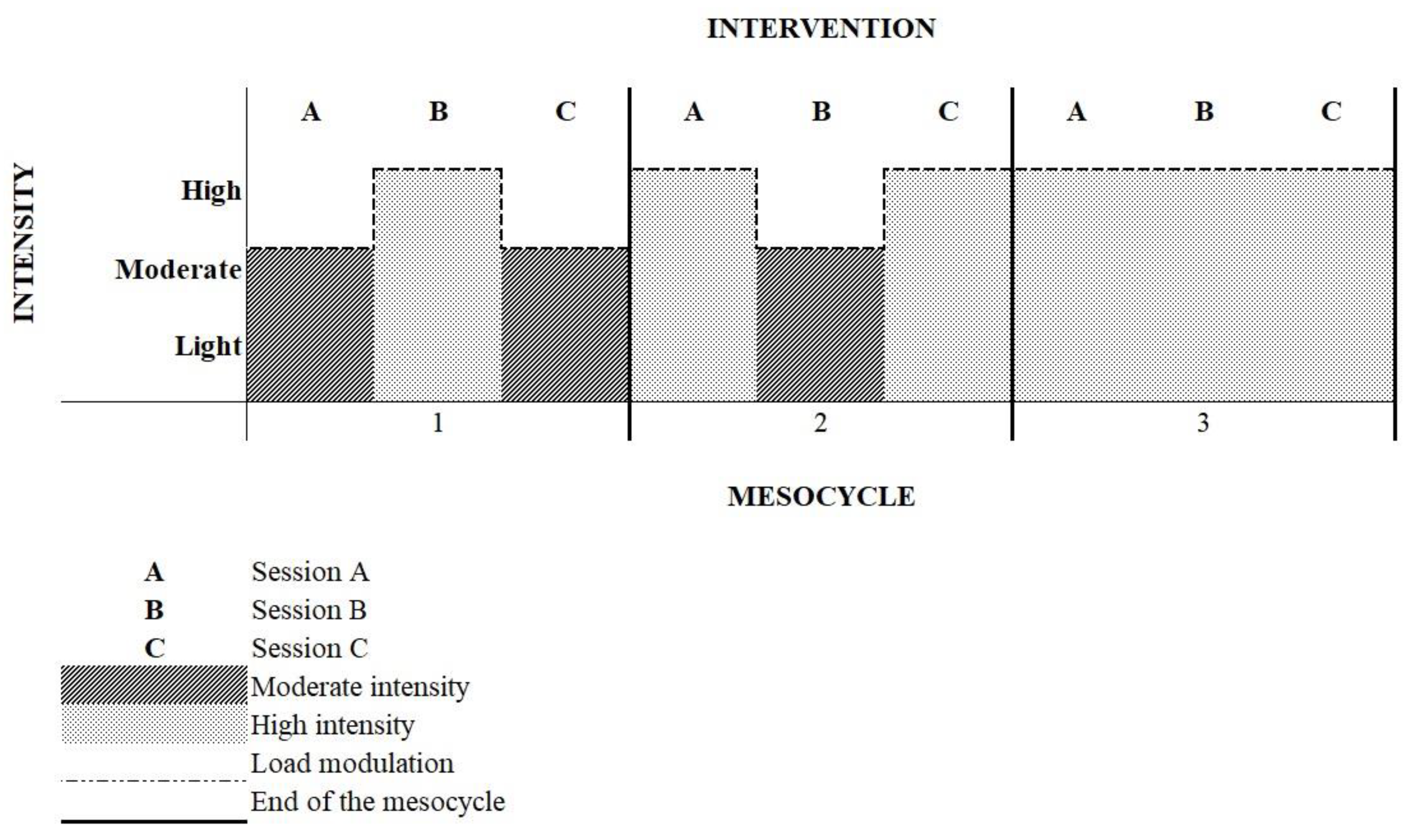
2.5.5. Intervention
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ervatti, L.; Borges, G.; Jardim, A. (Eds.) Mudança Demográfica no Brasil no Início do Século XXI. Subsídios Para as Projeções da População. IBGE. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv93322.pdf (accessed on 10 October 2022). (In Portuguese)
- Chen, C.; Zhou, M.; Ge, Y.; Wang, X. SIRT1 and aging related signaling pathways. Mech. Ageing Dev. 2020, 187, 111215. [Google Scholar] [CrossRef] [PubMed]
- Schmeer, C.; Kretz, A.; Wengerodt, D.; Stojiljkovic, M.; Witte, O.W. Dissecting Aging and Senescence—Current Concepts and Open Lessons. Cells 2019, 8, 1446. [Google Scholar] [CrossRef]
- BRASIL. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis. Vigitel Brasil 2018: Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas Por Inquérito Telefônico: Estimativas Sobre Frequência e Distribuição Sociodemográfica de Fatores de Risco e Proteção Para Doenças Crônicas Nas Capitais Dos 26 Estados Brasileiros e no Distrito Federal em 2018/Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis—Brasília: Ministério da Saúde, 2019./BRASIL. Ministério da Saúde. Available online: https://www.gov.br/saude/pt-br (accessed on 18 October 2019). (In Portuguese)
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef] [PubMed]
- Barroso, W.K.S.; Rodrigues, C.I.S.; Bortolotto, L.A.; Mota-Gomes, M.A.; Brandão, A.A.; Feitosa, A.D.D.M.; Machado, C.A.; Poli-De-Figueiredo, C.E.; Amodeo, C.; Mion, D.; et al. Diretrizes Brasileiras de Hipertensão Arterial—2020. Arq. Bras. Cardiol. 2020, 116, 516–658. (In Portuguese) [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Smart, N.A. Exercise Training for Blood Pressure: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [PubMed]
- Eddens, L.; van Someren, K.; Howatson, G. The Role of Intra-Session Exercise Sequence in the Interference Effect: A Systematic Review with Meta-Analysis. Sports Med. 2017, 48, 177–188. [Google Scholar] [CrossRef]
- Polito, M.D.; Farinatti, P.D.T.V. Comportamento da pressão arterial após exercícios contra-resistência: Uma revisão sistemática sobre variáveis determinantes e possíveis mecanismos. Rev. Bras. Med. Esporte 2006, 12, 386–392. (In Portuguese) [Google Scholar] [CrossRef][Green Version]
- Viecili, P.R.N.; Bündchen, D.C.; Richter, C.M.; Dipp, T.; Lamberti, D.B.; Pereira, A.M.R.; Barbosa, L.D.C.; Rubin, A.C.; Barbosa, E.G.; Panigas, T.F. Curva dose-resposta do exercício em hipertensos: Análise do número de sessões para efeito hipotensor. Arq. Bras. Cardiol. 2009, 92, 393–399. (In Portuguese) [Google Scholar] [CrossRef][Green Version]
- Buzzachera, C.F.; Baldari, C.; Elsangedy, H.M.; Krinski, K.; Santos, B.V.; De Campos, W.; Guidetti, L.; Da Silva, S.G. Comparação das respostas fisiológicas, perceptuais e afetivas durante caminhada em ritmo autosselecionado por mulheres adultas de três diferentes faixas etárias. Rev. Bras. Med. Esporte 2010, 16, 329–334. (In Portuguese) [Google Scholar] [CrossRef][Green Version]
- Kura, G.G.; Filho, H.T.; Paula, A.P.; Calegari, L.; Schmidt, R.; Bona, C.C. Efeitos do treinamento aeróbio versus treinamento combinado na pressão arterial de repouso em idosos. Rev. FisiSenectus 2013, 1, 3–11. (In Portuguese) [Google Scholar] [CrossRef]
- Alves, R.C.; Ferreira, S.; Benites, M.L.; Krinski, K.; Follador, L.; Da Silva, S.G. Exercícios com pesos sobre as respostas afetivas e perceptuais. Rev. Bras. Med. Esporte 2015, 21, 200–205. (In Portuguese) [Google Scholar] [CrossRef]
- Dos Reis, J.P.C.; Almeida, K.D.S.; Souza, R.A.D.S.; De Sousa, M.S.S.R. Effect of Resistance Training with Different Intensities on Blood Pressure in Hypertensive Patients. Int. J. Cardiovasc. Sci. 2015, 1, 25–34. [Google Scholar] [CrossRef]
- Calogiuri, G.; Evensen, K.; Weydahl, A.; Andersson, K.; Patil, G.; Ihlebæk, C.; Raanaas, R.K. Green exercise as a workplace intervention to reduce job stress. Results from a pilot study. Work 2015, 53, 99–111. [Google Scholar] [CrossRef]
- Lacharité-Lemieux, M.; Dionne, I.J. Physiological Responses to Indoor Versus Outdoor Training in Postmenopausal Women. J. Aging Phys. Act. 2016, 24, 275–283. [Google Scholar] [CrossRef]
- Krinski, K.; Machado, D.G.S.; Lirani, L.S.; DaSilva, S.G.; Costa, E.C.; Hardcastle, S.J.; Elsangedy, H.M. Let’s Walk Outdoors! Self-Paced Walking Outdoors Improves Future Intention to Exercise in Women with Obesity. J. Sport Exerc. Psychol. 2017, 39, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Matsouka, O.; Kabitsis, C.; Harahousou, Y.; Trigonis, I. Mood alterations following an indoor and outdoor exercise pro-gram in healthy elderly women. Percept. Mot. Ski. 2005, 100, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Fuegen, K.; Breitenbecher, K.H. Walking and Being Outdoors in Nature Increase Positive Affect and Energy. Ecopsychology 2018, 10, 14–25. [Google Scholar] [CrossRef]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does Participating in Physical Activity in Outdoor Natural Environments Have a Greater Effect on Physical and Mental Wellbeing than Physical Activity Indoors? A Systematic Review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Alves, H.D.N.; Fridich, G.A.; De Souza, T.S.P.; López, L.C.S.; De Lucena, R.F.P. Exercício físico outdoor e indoor, bem-estar subjetivo e conexão com a Natureza: Uma revisão sistemática. Rev. Bras. Gestão Ambient. Sustentabilidade 2019, 6, 515–529. (In Portuguese) [Google Scholar] [CrossRef]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The Effects of Green Exercise on Physical and Mental Wellbeing: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1352. [Google Scholar] [CrossRef]
- Malachias, M.V.B. 7th Brazilian Guideline of Arterial Hypertension: Presentation. Arq. Bras. Cardiol. 2016, 107, 1–104. [Google Scholar] [PubMed]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, A.C. A New Approach to Monitoring Exercise Training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar] [PubMed]
- Hardy, C.J.; Rejeski, W.J. Not What, but How One Feels: The Measurement of Affect during Exercise. J. Sport Exerc. Psychol. 1989, 11, 304–317. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Lima, L.G.; Bonardi, J.T.M.; Campos, G.O.; Bertani, R.F.; Scher, L.M.L.; Moriguti, J.C.; Ferriolli, E.; Lima, N.K.C. Combined Aerobic and Resistance Training: Are There Additional Benefits for Older Hypertensive Adults? Clinics 2017, 72, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, I.C.; de Sousa Araújo Santos, Z.M.; Mont’Alverne, D.G.B.; Martins, A.B.T.; de Araujo Magalhães, C.B. Exercícios e outras estratégias não farmacológicas para reduzir a pressão arterial em idosos: Uma revisão sistemática e meta-análise. Rev. Bras. Geriatr. Gerontol. 2018, 12, 248–267. (In Portuguese) [Google Scholar] [CrossRef]
- de Oliveira, S.N.; Moro, A.R.P.; Domingues, W.J.R.; Bezerra, E.D.S. Effects of concurrent training with self-selected intensity on the physical fitness of hypertensive individuals. Acta Sci. Health Sci. 2018, 40, 35739. [Google Scholar] [CrossRef]
- Feng-Bin, L. Effects of integrated exercise on blood pressure in elderly Mongolian hypertensive patients. Acta Med. Mediterr. 2020, 36, 653–659. [Google Scholar] [CrossRef]
- Machado Cda, S.; Venancio, V.P.; Aissa, A.F.; Hernandes, L.C.; de Mello, M.B.; Del Lama, J.E.; Marzocchi-Machado, C.M.; Bianchi, M.L.; Antunes, L.M. Vitamin D3 deficiency increases DNA damage and the oxidative burst of neutrophils in a hypertensive rat model. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2016, 798, 19–26. [Google Scholar] [CrossRef]
- Martins, D.; Wolf, M.; Pan, D.; Zadshir, A.; Tareen, N.; Thadhani, R.; Felsenfeld, A.; Levine, B.; Mehrotra, R.; Norris, K. Prevalence of cardiovascular risk factors and the serum levels of 25-hydroxyvitamin D in the United States: Data from the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2007, 167, 1159–1165. [Google Scholar] [CrossRef]
- Flint, A.C.; Conell, C.; Ren, X.; Banki, N.M.; Chan, S.L.; Rao, V.A.; Melles, R.B.; Bhatt, D.L. Effect of Systolic and Diastolic Blood Pressure on Cardiovascular Outcomes. N. Engl. J. Med. 2019, 381, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Lacharité-Lemieux, M.; Brunelle, J.-P.; Dionne, I.J. Adherence to Exercise and Affective Responses: Comparison between Outdoor and Indoor Training. Menopause 2015, 22, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, A.; Veloso, S. Outdoor Exercise, Well-Being and Connectedness to Nature. Psico 2014, 45, 299–304. [Google Scholar] [CrossRef]
- Johnson, M.N.; Maher, J.P.; Meadows, C.C.; Bittel, K.M.; Hevel, D.J.; Drollette, E.S. Positive affect moderates inhibitory control and positive affect following a single bout of self-select aerobic exercise. Psychol. Sport Exerc. 2022, 60, 102141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | OCT (n = 12) | ICT (n = 14) | p-Value |
|---|---|---|---|
| ± sd | ± sd | ||
| Age (years) | 67.3 ± 8.2 | 65.8 ± 7.8 | 0.644 |
| Body mass (kg) | 78.1 ± 15.2 | 79.3 ± 13.9 | 0.839 |
| Height (m) | 1.68 ± 0.1 | 1.64 ± 0.1 | 0.390 |
| BMI (kg/m²) | 27.4 ± 3.0 | 29.4 ± 4.3 | 0.198 |
| n (%) | n (%) | ||
| Sex (female) | 3 (25.0) | 7 (50.0) | 0.192 |
| Hypertension | 6 (50.0) | 11 (78.6) | 0.126 |
| Dyslipidemia | 8 (66.7) | 5 (35.5) | 0.115 |
| Diabetes | 3 (25.0) | 2 (14.3) | 0.489 |
| Antihypertensive users | |||
| No medication | 7 (58.3%) | 5 (35.7) | 0.248 |
| Up to 1 medication | 3 (25.0) | 5 (35.7) | 0.555 |
| Up to 2 medications | 1 (8.3) | 4 (28.6) | 0.191 |
| Up to 3 medications | 1 (8.3) | 0 (0.0) | 0.270 |
| OCT (n = 12) | ICT (n = 14) | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Cohen’s d | Pre | Post | Cohen’s d | g | t | g*t | |
| ± sd | ± sd | ± sd | ± sd | ||||||
| SBP (mmHg) | 122.7 ± 9.1 | 118.8 ± 10.3 | 0.40 | 123.4 ± 14.0 | 128.2 ± 19.9 | −0.27 | 0.341 | 0.885 | 0.312 |
| Δ SBP | −3.9 ± 11.7 | 4.8 ± 11.1 | |||||||
| DBP (mmHg) | 69.7 ± 5.9 | 65.9 ± 6.9 † | 0.59 | 71.3 ± 6.2 | 75.0 ± 6.5 | −0.58 | 0.004 | 0.876 | 0.040 |
| Δ DBP | −3.8 ± 5.3 | 3.7 ± 6.9 | |||||||
| MBP (mmHg) | 87.4 ± 6.0 | 83.5 ± 6.8 | 0.61 | 88.6 ± 6.9 | 92.7 ± 9.6 | −0.49 | 0.015 | 0.836 | 0.065 |
| Δ MBP | −3.9 ± 7.3 | 4.1 ± 8.0 | |||||||
| HR (bpm) | 70.8 ± 12.3 | 65.9 ± 6.9 | 0.49 | 73.1 ± 8.2 | 73.9 ± 9.6 | −0.09 | 0.057 | 0.481 | 0.284 |
| Δ HR | −4.9 ± 12.7 | 0.8 ± 7.8 | |||||||
| OCT (n = 12) | ICT (n = 14) | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Cohen’s d | Pre | Post | Cohen’s d | g | t | g*t | |
| ± sd | ± sd | ± sd | ± sd | ||||||
| RPE | 4.08 ± 1.44 | 3.75 ± 1.05 | 0.26 | 3.75 ± 1.05 | 3.35 ± 1.59 | 0.30 | 0.144 | 0.202 | 0.671 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Moraes, J.A.; De Barcelos, G.T.; Coneglian, J.C.; Do Espírito Santo, B.C.d.R.; Delevatti, R.S.; Gerage, A.M. Combined Training with Aerobic Exercise Performed Outdoors Can Promote Better Blood Pressure and Affective Responses in Individuals with Cardiovascular Risk Factors. Int. J. Environ. Res. Public Health 2022, 19, 16009. https://doi.org/10.3390/ijerph192316009
De Moraes JA, De Barcelos GT, Coneglian JC, Do Espírito Santo BCdR, Delevatti RS, Gerage AM. Combined Training with Aerobic Exercise Performed Outdoors Can Promote Better Blood Pressure and Affective Responses in Individuals with Cardiovascular Risk Factors. International Journal of Environmental Research and Public Health. 2022; 19(23):16009. https://doi.org/10.3390/ijerph192316009
Chicago/Turabian StyleDe Moraes, Janara Antunes, Guilherme Tadeu De Barcelos, Juliana Cavestré Coneglian, Bárbara Carlin de Ramos Do Espírito Santo, Rodrigo Sudatti Delevatti, and Aline Mendes Gerage. 2022. "Combined Training with Aerobic Exercise Performed Outdoors Can Promote Better Blood Pressure and Affective Responses in Individuals with Cardiovascular Risk Factors" International Journal of Environmental Research and Public Health 19, no. 23: 16009. https://doi.org/10.3390/ijerph192316009
APA StyleDe Moraes, J. A., De Barcelos, G. T., Coneglian, J. C., Do Espírito Santo, B. C. d. R., Delevatti, R. S., & Gerage, A. M. (2022). Combined Training with Aerobic Exercise Performed Outdoors Can Promote Better Blood Pressure and Affective Responses in Individuals with Cardiovascular Risk Factors. International Journal of Environmental Research and Public Health, 19(23), 16009. https://doi.org/10.3390/ijerph192316009