
eHealth Platforms to Promote Autonomous Life and Active Aging: A Scoping Review

 , , , , , ,
, , , , , ,  , ,
, ,  ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
- -
- Which eHealth platforms facilitate autonomous life and promote active aging?
- -
- What are the age groups targeted by the eHealth platforms?
- -
- What are the domains of intervention of these eHealth platforms (physical, emotional, cognitive, or social)?
- -
- Which outcomes are assessed in studies that have implemented and evaluated these eHealth platforms?
2. Materials and Methods
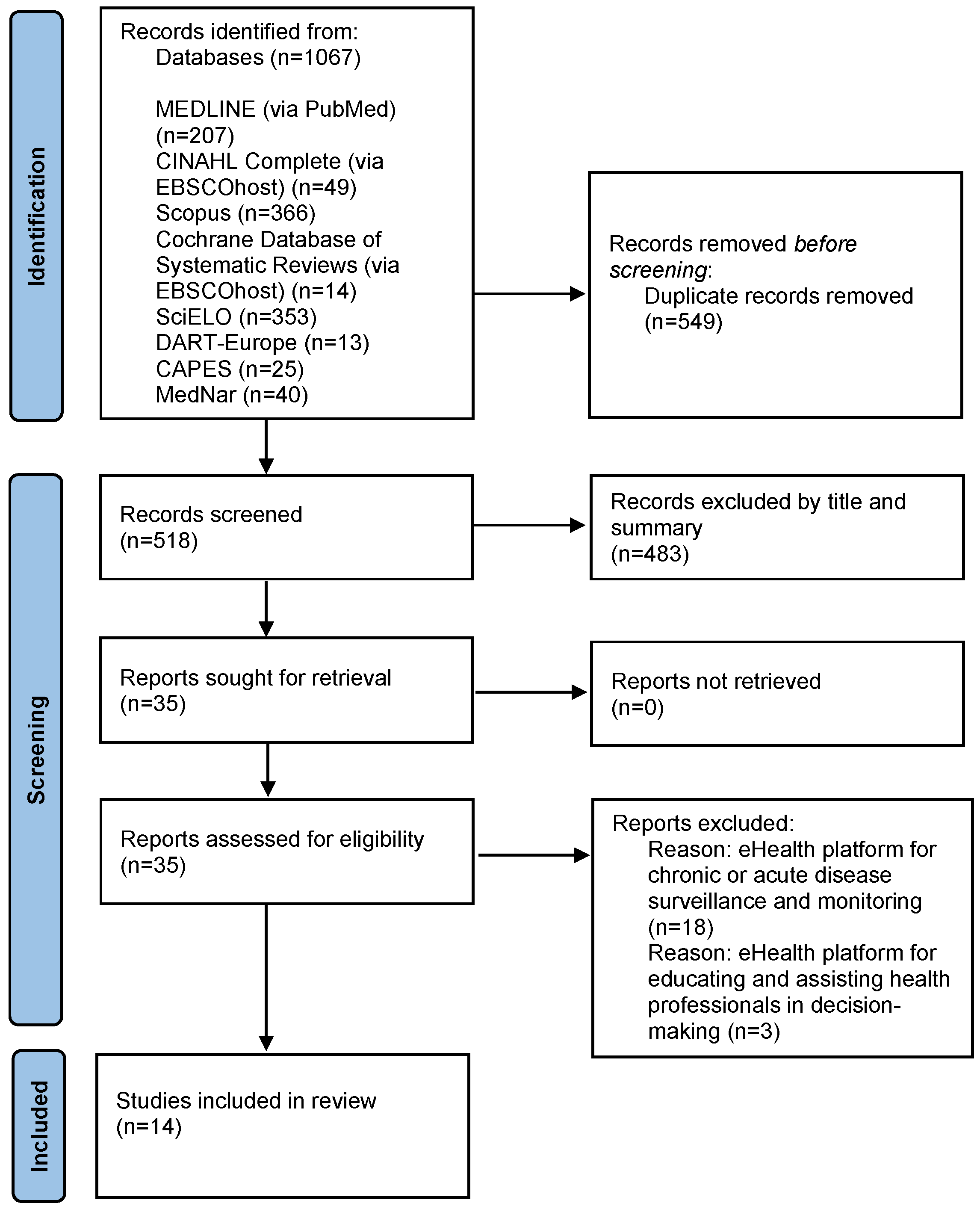
2.1. Search Strategy
2.2. Study Selection and Data Extraction
3. Results
3.1. Study Characteristics, Settings, and Samples

{kind=link}
| Author, Year, Country | Project/Platform Development | Aims/Purpose | Age Group (Years)/Sample Size | eHealth Platforms/Project |
|---|---|---|---|---|
| Palumbo et al. (2020) [37]. Consortium Italy, Switzerland, Spain, Romania | This paper describes the design of the NESTORE methodology and its IoT architecture. | To describe the design of the NESTORE methodology and its IoT architecture and describe the validation strategy to assess the effectiveness of NESTORE as a coaching platform for healthy aging. | 65–75/* | NESTORE system—coaching activities and personalized feedback to the user. |
| Reijnders et al. (2015) [38]. The Netherlands | A randomized controlled trial | To investigate the effectiveness of the eHealth intervention in terms of subjective cognitive functioning and to measure objective cognitive functioning and psychological well-being. | 40–65/n = 376 | “Keep your brain fit!” —online psychoeducational intervention. |
| Nebeker, C. and Zlatar, Z. (2021) [39]. USA | Exit Survey | To understand the motivations and perceptions of participants enrolled in studies promoting brain health and their opinions regarding the use of mHealth tools within this context. | 65–80/n = 41 | mHealth device to assist Independent Walking for Brain Health |
| Beristain et al. (2021) [40]. Consortium Spain, USA, Greece, Ireland, Italy | This paper describes the coaching aspects in CAPTAIN from different perspectives following a top-down approach. | To present a user-centered virtual coach for older adults at home to promote active and healthy aging and independent living. | Older adults/* | CAPTAIN—virtual coaching ecosystem (VCE). |
| Bilbao et al. (2016) [41]. Consortium UK, The Netherlands, Spain, Germany, Austria, France, Belgium | This paper describes the SONOPA framework and its elements, explains the deployments carried out in the course of the project execution and the evaluation of the matchmaking algorithm and draws some conclusions and proposes further work. | To present an Ambient Assisted Living framework developed within the SONOPA project, whose objective is to promote active aging by combining a social network with information inferred using in-home sensors. | Older adults/* | SONOPA—an Ambient Assisted Living framework. |
| Konstantinidis et al. (2014) [42]. Greece | This paper presents the design, implementation, wide deployment, and evaluation of the FitForAll platform system usability, user adherence to exercise, and efficacy are explored. | To present the design, implementation, wide deployment, and evaluation of the low cost, physical exercise, and gaming (exergaming) FitForAll (FFA) platform system usability. | 67–87/n = 116 | FitForAll (FFA) platform—maintain/advance healthy physical status and well-being. |
| Irvine et al. (2013) [43]. USA | A randomized controlled trial. | To evaluate the efficacy of a 12-week Internet intervention to help sedentary older adults adopt and maintain an exercise regimen. | Over 55/n = 368 | Active After 55—participation in exercise activities on a regular basis. |
| Muellmann et al. (2019) [44]. Germany | A randomized controlled trial. | To examine the effects of two web-based interventions on physical activity in older adults compared to a delayed intervention control group. | 65–75/n = 589 | PROMOTE study—supported in web-based interventions, one including subjective physical activity monitoring and the other a combination of subjective and objective physical activity monitoring. |
| Ballesteros et al. (2014) [45]. Consortium Spain, Sweden, and Greece | A randomized controlled trial. | To investigate the potential of new Information and Communication Technology (ICT) environments to help maintain independence and well-being. | 65–85/n = 57 | AGNES is a novel ICT solution that promotes connectivity and social inclusion. |
| Compernolle et al. (2020) [46]. Belgium | A mixed methods study to evaluate engagement, acceptability, usability, and preliminary efficacy. | To evaluate engagement, acceptability, usability, and preliminary efficacy of a self-monitoring-based mHealth intervention developed to reduce sedentary behavior. | 60/n = 28 | Activator self-monitoring device of sedentary behavior. |
| O’Caoimh et al. (2018) [47]. Consortium The Netherlands and Italy | This paper describes the 25 healthcare related recommendations of PERSSILAA | To address pre-frailty and promote active and healthy aging, targeting three pre-frailty subdomains: nutrition, cognition, and physical function. | Older adults/* | PERSSILAA—ICT-supported platform to screen, assess, manage, and monitor community-dwelling older adults |
| Christophorou et al. (2016) [48]. Consortium Switzerland and The Netherlands | This paper described the Miraculous-Life project. | To identify and assess a set of services that an ICT system for Aging Well should support, in an actual end-user setting. | Older adults/1st trial–n = 7 older adults and n = 2 caregivers; 2nd trial–n = 16 older adults and n = 5 caregivers; 3rd trial–n = 15 older adults and n = 4 caregivers. | Miraculous-Life—a package of ICT services for Ageing Well that promotes ‘Positive Ageing’. |
| Taraldsen et al. (2020) [49]. Norway, Germany, and The Netherlands | A randomized controlled trial. | To assess the feasibility of delivering a lifestyle-integrated functional exercise program and evaluate the delivery of the intervention by use of digital technology (eLiFE) to prevent functional decline. | 61–70/n = 180 | eLiFE intervention—delivered to participants via the PreventIT application on a smartphone and a smartwatch through video clips, pictures, and text/verbal instructions for each activity. |
| Fornasini et al. (2020) [50]. Italy | Qualitative study to evaluate the usability of technologies and determine the user experience of participants. | To investigate the effectiveness of activities that combine geocaching and self-tracking technologies to promote active aging. | 65–82/n = 14 | The Impronte project—combines the geocaching activity, accompanied by gamification elements, with the use of fitness tracking technology in the form of a pedometer bracelet. |
3.2. Description of the eHealth Platforms
3.3. Domains of Intervention of These eHealth Platforms
3.4. Outcomes Assessed
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
| MEDLINE (via PubMed)—searched on 5 June 2022: 207 records (“environment design”[MeSH Terms] OR “digital technology”[MeSH Terms] OR “telemedicine”[MeSH Terms] OR “internet based intervention”[MeSH Terms] OR “telenursing”[MeSH Terms] OR (“ehealth”[Title/Abstract] OR “ehealth intervention”[Title/Abstract] OR “ehealth program”[Title/Abstract] OR “digital health interventions”[Title/Abstract] OR “digital health”[Title/Abstract] OR “digital healthcare”[Title/Abstract] OR “digital health technology”[Title/Abstract] OR “telehealth”[Title/Abstract] OR “environment design”[Title/Abstract] OR “digital technology”[Title/Abstract] OR “telemedicine”[Title/Abstract] OR “internet based intervention”[Title/Abstract] OR “telenursing”[Title/Abstract] OR “digital health applications”[Title/Abstract] OR “mobile health applications”[Title/Abstract] OR “mobile applications”[Title/Abstract] OR “mobile health interventions”[Title/Abstract] OR “digital health services”[Title/Abstract])) AND (“healthy aging”[MeSH Terms] OR “active aging”[Title/Abstract] OR “active ageing”[Title/Abstract] OR “healthy ageing”[Title/Abstract] OR “aging well”[Title/Abstract] OR “ageing well”[Title/Abstract] OR “healthy strategies”[Title/Abstract] OR “healthy aging”[Title/Abstract]) Filters: English, Portuguese, Spanish |
| CINAHL Complete (via EBSCOhost)—searched on 5 June 2022: 49 records ((TI “active aging” OR “active ageing” OR “healthy ageing” OR “aging well” OR “ageing well” OR “healthy strategies” OR “healthy aging” OR AB “active aging” OR “active ageing” OR “healthy ageing” OR “aging well” OR “ageing well” OR “healthy strategies” OR “healthy aging”) OR (MH “Healthy Aging”)) AND ((MH “Telenursing”) OR (MH “Telemedicine”) OR (MH “Digital Health”) OR TI (“ehealth” OR “ehealth intervention” OR “ehealth program” OR “digital health interventions” OR “digital health” OR “digital healthcare” OR “digital health technology” OR “telehealth” OR “environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “digital health applications” OR “mobile health applications” OR “mobile applications” OR “mobile health interventions” OR “digital health services”) OR AB (“ehealth” OR “ehealth intervention” OR “ehealth program” OR “digital health interventions” OR “digital health” OR “digital healthcare” OR “digital health technology” OR “telehealth” OR “environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “digital health applications” OR “mobile health applications” OR “mobile applications” OR “mobile health interventions” OR “digital health services”)) Filters: English, Portuguese, Spanish |
| SCOPUS—searched on 5 June 2022: 366 records (TITLE-ABS-KEY (“healthy aging” OR “active aging” OR “active ageing” OR “healthy ageing” OR “aging well” OR “ageing well” OR “healthy strategies”)) AND (TITLE-ABS-KEY (“environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “ehealth” OR “ehealth intervention” OR “ehealth program” OR “digital health interventions” OR “digital health” OR “digital healthcare” OR “digital health technology” OR “telehealth” OR “environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “digital health applications” OR “mobile health applications” OR “mobile applications” OR “mobile health interventions” OR “digital health services”)) Filters: English, Portuguese, Spanish |
| Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews (via EBSCOhost)—searched on 5 June 2022: 14 records ((TI “active aging” OR “active ageing” OR “healthy ageing” OR “aging well” OR “ageing well” OR “healthy strategies” OR “healthy aging” OR AB “active aging” OR “active ageing” OR “healthy ageing” OR “aging well” OR “ageing well” OR “healthy strategies” OR “healthy aging”) AND TI (“ehealth” OR “ehealth intervention” OR “ehealth program” OR “digital health interventions” OR “digital health” OR “digital healthcare” OR “digital health technology” OR “telehealth” OR “environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “digital health applications” OR “mobile health applications” OR “mobile applications” OR “mobile health interventions” OR “digital health services”) OR AB (“ehealth” OR “ehealth intervention” OR “ehealth program” OR “digital health interventions” OR “digital health” OR “digital healthcare” OR “digital health technology” OR “telehealth” OR “environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “digital health applications” OR “mobile health applications” OR “mobile applications” OR “mobile health interventions” OR “digital health services”)) Filters: English, Portuguese, Spanish |
| SciELO—searched on 5 June 2022: 353 records ((ti:(*”active aging” OR “active ageing” OR “healthy ageing” OR “aging well” OR “ageing well” OR “healthy strategies” OR “healthy aging”)) OR (ab:(“active aging” OR “active ageing” OR “healthy ageing” OR “aging well” OR “ageing well” OR “healthy strategies” OR “healthy aging”))) AND ((ti:(“ehealth” OR “ehealth intervention” OR “ehealth program” OR “digital health interventions” OR “digital health” OR “digital healthcare” OR “digital health technology” OR “telehealth” OR “environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “digital health applications” OR “mobile health applications” OR “mobile applications” OR “mobile health interventions” OR “digital health services”)) OR (ab:(“ehealth” OR “ehealth intervention” OR “ehealth program” OR “digital health interventions” OR “digital health” OR “digital healthcare” OR “digital health technology” OR “telehealth” OR “environment design” OR “digital technology” OR “telemedicine” OR “internet based intervention” OR “telenursing” OR “digital health applications” OR “mobile health applications” OR “mobile applications” OR “mobile health interventions” OR “digital health services”))) Filters: English, Portuguese, Spanish |
| DART-Europe—searched on 5 June 2022: 13 records (“active aging” OR healthy aging”) AND (ehealth OR digital) Filters: English, Portuguese, Spanish |
| CAPES—searched on 5 June 2022: 25 records Ehealth Filters: English, Portuguese, Spanish |
| MedNar—searched on 5 June 2022: 40 records ageing AND ehealth Filters: English, Portuguese, Spanish |
Appendix B. Description of Domain(s) of Intervention
| eHealth Platforms/Project | Domain(s) of intervention of eHealth platforms |
| NESTORE [37] | Physical, nutrition, cognition, and social:
|
| Keep your brain fit [38] | Lifestyle, memory, and effective work:
|
| Independent Walking for Brain Health [39] | Cognitive and physical:
|
| CAPTAIN [40] | Cognitive, physical, social, and nutritional: The general idea of this virtual coaching system from the participant’s point of view (i.e., older adult) is to become a lifelong learning (i.e., coaching), motivational and supportive platform to promote healthy habits through individual behavior change. Each SMART goal is composed of a weekly plan with coaching actions provided by digital intervention tools such as recommendation systems, quizzes, coaches, and games. All of them are focused on supporting the process of behavior change.
|
| SONOPA [41] | Social:
|
| FitForAll (FFA) [42] | Physical:
|
| Active After 55 [43] | Physical:
|
| PROMOTE [44] | Physical:
|
| AGNES [45] | Social:
|
| Activator [46] | Physical:
|
| PERSSILAA [47] | Nutritional, physical, cognitive, and social:
|
| Miraculous Projet [48] | Social and physical:
|
| eLiFE [49] | Physical:
|
| Impronte Project [50] | Physical and social:
|
References
- European Commission. Directorate General for Economic and Financial Affairs. The 2021 Ageing Report: Economic & Budgetary Projections for the EU Member States (2019–2070); Publications Office: Brussels, Belgium, 2021.
- Musich, S.; Wang, S.; Hawkins, K.; Klemes, A. The Impact of Personalized Preventive Care on Health Care Quality, Utilization, and Expenditures. Popul. Health Manag. 2016, 19, 389–397. [Google Scholar] [CrossRef]
- Seah, B.; Wang, W. SHAPE: A Healthy Aging Community Project Designed Based on the Salutogenic Theory. In Health Promotion in Health Care—Vital Theories and Research [Internet]; Haugan, G., Eriksson, M., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 329–347. [Google Scholar]
- United Nations. General Assembly Resolution A/RES/70/1. Transforming Our World, the 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Ayala, A.; Rodríguez-Blázquez, C.; Calderón-Larrañaga, A.; Beridze, G.; Teixeira, L.; Araújo, L.; Rojo-Pérez, F.; Fernández-Mayoralas, G.; Rodríguez-Rodríguez, V.; Quirós-González, V.; et al. Influence of Active and Healthy Ageing on Quality of Life Changes: Insights from the Comparison of Three European Countries. Int. J. Environ. Res. Public Health 2021, 18, 4152. [Google Scholar] [CrossRef]
- Robbins, T.D.; Lim Choi Keung, S.N.; Arvanitis, T.N. E-health for active ageing; A systematic review. Maturitas 2018, 114, 34–40. [Google Scholar] [CrossRef]
- World Report on Aging and Health—Executive Summary. Psychol. Sci. 2015, 25, 1682–1690.
- Dos Varela, V.S.; Mendes, J.M.; Abreu, D.P.G.; Piexak, D.R.; do Martins, K.P.; de Bandeira, E.O. Health promotion and disease prevention from the perspective of active aging. Res. Soc. Dev. 2020, 9, e65491110096. [Google Scholar] [CrossRef]
- Liu, L.; Wu, F.; Tong, H.; Hao, C.; Xie, T. The Digital Divide and Active Aging in China. Int. J. Environ. Res. Public Health 2021, 18, 12675. [Google Scholar] [CrossRef]
- De Luca, V.; Lazic, V.; Birov, S.; Piesche, K.; Beyhan, O.; Pengo, M.F.; Melgara, M.; Sherman, M.H.; Lilja, M.; Balenovic, A.; et al. Digitally Enabled Health Service for the Integrated Management of Hypertension: A Participatory User-Centred Design Process. Int. J. Environ. Res. Public Health 2021, 18, 12442. [Google Scholar] [CrossRef]
- Sülz, S.; van Elten, H.J.; Askari, M.; Weggelaar-Jansen, A.M.; Huijsman, R. eHealth Applications to Support Independent Living of Older Persons: Scoping Review of Costs and Benefits Identified in Economic Evaluations. J. Med. Internet Res. 2021, 23, e24363. [Google Scholar] [CrossRef]
- Francis, J.; Rikard, R.V.; Cotten, S.R.; Kadylak, T. Does ICT Use matter? How information and communication technology use affects perceived mattering among a predominantly female sample of older adults residing in retirement communities. Inf. Commun. Soc. 2019, 22, 1281–1294. [Google Scholar] [CrossRef]
- Peterson, C.B.; Hamilton, C.; Hasvold, P. From Innovation to Implementation: eHealth in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2016.
- International Telecommunication Union. Ageing in a Digital World—From Vulnerable to Valuable. 2020. Available online: https://docslib.org/doc/5844293/ageing-in-a-digital-world-from-vulnerable-to-valuable (accessed on 17 May 2022).
- Benis, A.; Tamburis, O.; Chronaki, C.; Moen, A. One Digital Health: A Unified Framework for Future Health Ecosystems. J. Med. Internet Res. 2021, 23, e22189. [Google Scholar] [CrossRef]
- Buyl, R.; Beogo, I.; Fobelets, M.; Deletroz, C.; Van Landuyt, P.; Dequanter, S.; Gorus, E.; Bourbonnais, A.; Giguère, A.; Lechasseur, K.; et al. e-Health interventions for healthy aging: A systematic review. Syst. Rev. 2020, 9, 128. [Google Scholar] [CrossRef]
- Mazeas, A.; Duclos, M.; Pereira, B.; Chalabaev, A. Evaluating the Effectiveness of Gamification on Physical Activity: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2022, 24, e26779. [Google Scholar] [CrossRef]
- Moerenhout, T.; Devisch, I.; Cornelis, G.C. E-health beyond technology: Analyzing the paradigm shift that lies beneath. Med. Health Care Philos. 2018, 21, 31–41. [Google Scholar] [CrossRef]
- Organisation for Economic Co-Operation and Development. ICT Access and Usage by Households and Individuals Database 2018. Available online: http://www.oecd.org/sti/broadband/broadband-statistics (accessed on 1 May 2022).
- Shapira, S.; Yeshua-Katz, D.; Goren, G.; Aharonson-Daniel, L.; Clarfield, A.M.; Sarid, O. Evaluation of a Short-Term Digital Group Intervention to Relieve Mental Distress and Promote Well-Being Among Community-Dwelling Older Individuals During the COVID-19 Outbreak: A Study Protocol. Front. Public Health 2021, 9, 577079. [Google Scholar] [CrossRef]
- Shapira, S.; Cohn-Schwartz, E.; Yeshua-Katz, D.; Aharonson-Daniel, L.; Clarfield, A.M.; Sarid, O. Teaching and Practicing Cognitive-Behavioral and Mindfulness Skills in a Web-Based Platform among Older Adults through the COVID-19 Pandemic: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 10563. [Google Scholar] [CrossRef]
- Billis, A.S.; Papageorgiou, E.I.; Frantzidis, C.A.; Tsatali, M.S.; Tsolaki, A.C.; Bamidis, P.D. A decision-support framework for promoting independent living and ageing well. IEEE J. Biomed Health Inform. 2015, 19, 199–209. [Google Scholar] [CrossRef]
- Hoffman, G.J.; Webster, N.J.; Bynum, J.P.W. A Framework for Aging-Friendly Services and Supports in the Age of COVID-19. J. Aging Soc. Policy 2020, 32, 450–459. [Google Scholar] [CrossRef]
- Scase, M.; Kreiner, K.; Ascolese, A. Development and Evaluation of Cognitive Games to Promote Health and Wellbeing in Elderly People with Mild Cognitive Impairment. Stud. Health Technol. Inform. 2018, 248, 255–262. [Google Scholar]
- Stara, V.; Santini, S.; Kropf, J.; D’Amen, B. Digital Health Coaching Programs Among Older Employees in Transition to Retirement: Systematic Literature Review. J. Med. Internet Res. 2020, 22, e17809. [Google Scholar] [CrossRef]
- World Health Organization. E-Health. 2016. Available online: https://www.who.int/ehealth/en (accessed on 20 June 2022).
- Bousquet, J.; Anto, J.M.; Haahtela, T.; Jousilahti, P.; Erhola, M.; Basagaña, X.; Czarlewski, W.; Odemyr, M.; Palkonen, S.; Sofiev, M.; et al. Digital transformation of health and care to sustain Planetary Health: The MASK proof-of-concept for airway diseases-POLLAR symposium under the auspices of Finland’s Presidency of the EU, 2019 and MACVIA-France, Global Alliance against Chronic Respiratory Diseases (GARD, WHO) demonstration project, Reference Site Collaborative Network of the European Innovation Partnership on Active and Healthy Ageing. Clin. Transl. Allergy 2020, 10, 24. [Google Scholar]
- Sánchez-González, D.; Rojo-Pérez, F.; Rodríguez-Rodríguez, V.; Fernández-Mayoralas, G. Environmental and Psychosocial Interventions in Age-Friendly Communities and Active Ageing: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8305. [Google Scholar] [CrossRef] [PubMed]
- Simmons, L.A.; Wolever, R.Q.; Bechard, E.M.; Snyderman, R. Patient engagement as a risk factor in personalized health care: A systematic review of the literature on chronic disease. Genome Med. 2014, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Czaja, S.J.; Boot, W.R.; Charness, N.; Rogers, W.A.; Sharit, J. Improving Social Support for Older Adults Through Technology: Findings from the PRISM Randomized Controlled Trial. Gerontologist 2018, 58, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Henriquez-Camacho, C.; Losa, J.; Miranda, J.J.; Cheyne, N.E. Addressing healthy aging populations in developing countries: Unlocking the opportunity of eHealth and mHealth. Emerg. Themes Epidemiol. 2014, 11, 136. [Google Scholar] [CrossRef] [PubMed]
- Schlomann, A.; Seifert, A.; Zank, S.; Woopen, C.; Rietz, C. Use of Information and Communication Technology (ICT) Devices Among the Oldest-Old: Loneliness, Anomie, and Autonomy. Innov. Aging 2020, 4, igz050. [Google Scholar] [CrossRef]
- Dantas, C.; van Staalduinen, W.; Jegundo, A.; Ganzarain, J.; Van der Mark, M.; Rodrigues, F.; Illario, M.; De Luca, V. Smart Healthy Age-Friendly Environments—Policy Recommendations of the Thematic Network SHAFE. Transl. Med. Unisa 2019, 19, 103–108. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Apóstolo, J.; Bernardo, J.; Loureiro, R.; Santana, E.; Duque, F.M.; Dantas, C.; Ventura, F.; Silva, R. eHealth platforms for promoting active living: A scoping review protocol. Res. Soc. Dev. 2022, 11, e236111132184. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Palumbo, F.; Crivello, A.; Furfari, F.; Girolami, M.; Mastropietro, A.; Manferdelli, G.; Röcke, C.; Guye, S.; Casanovas, A.S.; Caon, M.; et al. «Hi This Is NESTORE, Your Personal Assistant»: Design of an Integrated IoT System for a Personalized Coach for Healthy Aging. Front. Digit. Health 2020, 2, 545949. [Google Scholar] [CrossRef]
- Reijnders, J.S.A.M.; Geusgens, C.A.V.; Ponds, R.W.H.M.; van Boxtel, M.P.J. «Keep your brain fit!» Effectiveness of a psychoeducational intervention on cognitive functioning in healthy adults: A randomised controlled trial. Neuropsychol. Rehabil. 2017, 27, 455–471. [Google Scholar] [CrossRef] [PubMed]
- Nebeker, C.; Zlatar, Z.Z. Learning from Older Adults to Promote Independent Physical Activity Using Mobile Health (mHealth). Front. Public Health 2021, 9, 703910. [Google Scholar] [CrossRef] [PubMed]
- Beristain Iraola, A.; Álvarez Sánchez, R.; Hors-Fraile, S.; Petsani, D.; Timoleon, M.; Díaz-Orueta, U.; Carroll, J.; Hopper, L.; Epelde, G.; Kerexeta, J.; et al. User Centered Virtual Coaching for Older Adults at Home Using SMART Goal Plans and I-Change Model. Int. J. Environ. Res. Public Health 2021, 18, 6868. [Google Scholar] [CrossRef] [PubMed]
- Bilbao, A.; Almeida, A.; López-de-Ipiña, D. Promotion of active ageing combining sensor and social network data. J. Biomed. Inform. 2016, 64, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, E.I.; Billis, A.S.; Mouzakidis, C.A.; Zilidou, V.I.; Antoniou, P.E.; Bamidis, P.D. Design, Implementation, and Wide Pilot Deployment of FitForAll: An Easy to use Exergaming Platform Improving Physical Fitness and Life Quality of Senior Citizens. IEEE J. Biomed. Health Inform. 2016, 20, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Irvine, A.B.; Gelatt, V.A.; Seeley, J.R.; Macfarlane, P.; Gau, J.M. Web-based intervention to promote physical activity by sedentary older adults: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e19. [Google Scholar] [CrossRef]
- Muellmann, S.; Buck, C.; Voelcker-Rehage, C.; Bragina, I.; Lippke, S.; Meyer, J.; Peters, M.; Pischke, C.R. Effects of two web-based interventions promoting physical activity among older adults compared to a delayed intervention control group in Northwestern Germany: Results of the PROMOTE community-based intervention trial. Prev. Med. Rep. 2019, 15, 100958. [Google Scholar] [CrossRef]
- Ballesteros, S.; Toril, P.; Mayas, J.; Reales, J.M.; Waterworth, J.A. An ICT-mediated social network in support of successful ageing. Gerontechnology 2014, 13, 39–48. [Google Scholar] [CrossRef]
- Compernolle, S.; Cardon, G.; van der Ploeg, H.P.; Van Nassau, F.; De Bourdeaudhuij, I.; Jelsma, J.J.; Brondeel, R.; Van Dyck, D. Engagement, Acceptability, Usability, and Preliminary Efficacy of a Self-Monitoring Mobile Health Intervention to Reduce Sedentary Behavior in Belgian Older Adults: Mixed Methods Study. JMIR mHealth uHealth 2020, 8, e18653. [Google Scholar] [CrossRef]
- O’Caoimh, R.; Molloy, D.W.; Fitzgerald, C.; Van Velsen, L.; Cabrita, M.; Nassabi, M.H.; de Vette, F.; van Weering, M.D.; Jansen-Kosterink, S.; Frazer, S.; et al. Healthcare Recommendations from the Personalised ICT Supported Service for Independent Living and Active Ageing (PERSSILAA) Study. In Proceedings of the 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health [Internet], Porto, Portugal, 28–29 April 2017; SCITEPRESS—Science and Technology Publications: Porto, Portugal, 2017; pp. 91–103. [Google Scholar]
- Christophorou, C.; Kleanthous, S.; Georgiadis, D.; Cereghetti, D.M.; Andreou, P.; Wings, C.; Christodoulou, E.; Samaras, G. ICT services for active ageing and independent living: Identification and assessment. Health Technol. Lett. 2016, 3, 159–164. [Google Scholar] [CrossRef]
- Taraldsen, K.; Mikolaizak, A.S.; Maier, A.B.; Mellone, S.; Boulton, E.; Aminian, K.; Becker, C.; Chiari, L.; Follestad, T.; Gannon, B.; et al. Digital Technology to Deliver a Lifestyle-Integrated Exercise Intervention in Young Seniors—The PreventIT Feasibility Randomized Controlled Trial. Front. Digit. Health 2020, 2, 10. [Google Scholar] [CrossRef] [PubMed]
- Fornasini, S.; Dianti, M.; Bacchiega, A.; Forti, S.; Conforti, D. Using Geocaching to Promote Active Aging: Qualitative Study. J. Med. Internet Res. 2020, 22, e15339. [Google Scholar] [CrossRef] [PubMed]
- Mannheim, I.; Schwartz, E.; Xi, W.; Buttigieg, S.C.; McDonnell-Naughton, M.; Wouters, E.J.M.; van Zaalen, Y. Inclusion of Older Adults in the Research and Design of Digital Technology. Int. J. Environ. Res. Public Health 2019, 16, 3718. [Google Scholar] [CrossRef]
- Muellmann, S.; Bragina, I.; Voelcker-Rehage, C.; Rost, E.; Lippke, S.; Meyer, J.; Schnauber, J.; Wasmann, M.; Toborg, M.; Koppelin, F.; et al. Development and evaluation of two web-based interventions for the promotion of physical activity in older adults: Study protocol for a community-based controlled intervention trial. BMC Public Health 2017, 17, 512. [Google Scholar] [CrossRef] [PubMed]
- Astasio-Picado, Á.; Cobos-Moreno, P.; Gómez-Martín, B.; Verdú-Garcés, L.; Zabala-Baños, M.D.C. Efficacy of Interventions Based on the Use of Information and Communication Technologies for the Promotion of Active Aging. Int. J. Environ. Res. Public Health 2022, 19, 1534. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, e20. [Google Scholar] [CrossRef]
- Yerrakalva, D.; Hajna, S.; Griffin, S. Effects of Mobile Health App Interventions on Sedentary Time, Physical Activity, and Fitness in Older Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e14343. [Google Scholar] [CrossRef]
- Dekker-van Weering, M.; Jansen-Kosterink, S.; Frazer, S.; Vollenbroek-Hutten, M. User Experience, Actual Use, and Effectiveness of an Information Communication Technology-Supported Home Exercise Program for Pre-Frail Older Adults. Front. Med. 2017, 4, 208. [Google Scholar] [CrossRef]
- Jaschinski, C.; Ben Allouch, S.; Peters, O.; Cachucho, R.; van Dijk, J.A.G.M. Acceptance of Technologies for Aging in Place: A Conceptual Model. J. Med. Internet Res. 2021, 23, e22613. [Google Scholar] [CrossRef]
- Ienca, M.; Schneble, C.; Kressig, R.W.; Wangmo, T. Digital health interventions for healthy ageing: A qualitative user evaluation and ethical assessment. BMC Geriatr. 2021, 21, 412. [Google Scholar] [CrossRef]
- Aung, M.N.; Koyanagi, Y.; Nagamine, Y.; Nam, E.W.; Mulati, N.; Kyaw, M.Y.; Moolphate, S.; Shirayama, Y.; Nonaka, K.; Field, M.; et al. Digitally Inclusive, Healthy Aging Communities (DIHAC): A Cross-Cultural Study in Japan, Republic of Korea, Singapore, and Thailand. Int. J. Environ. Res. Public Health 2022, 19, 6976. [Google Scholar] [CrossRef] [PubMed]
- Compernolle, S.; Van Dyck, D.; Cardon, G.; Brondeel, R. Exploring Breaks in Sedentary Behavior of Older Adults Immediately After Receiving Personalized Haptic Feedback: Intervention Study. JMIR mHealth uHealth 2021, 9, e26387. [Google Scholar] [CrossRef] [PubMed]

| Domain(s) of Intervention of eHealth Platforms | eHealth Platforms/Project |
|---|---|
| Physical | NESTORE [37] |
| Independent Walking for Brain Health [39] | |
| CAPTAIN [40] | |
| FitForAll (FFA) [42] | |
| Active After 55 [43] | |
| PROMOTE [44] | |
| Activator [46] | |
| PERSSILAA [47] | |
| Miraculous Projet [48] | |
| eLiFE [49] | |
| Impronte Project [50] | |
| Nutrition | NESTORE [37] |
| CAPTAIN [40] | |
| PERSSILAA [47] | |
| Cognition | NESTORE [37] |
| Keep your brain fit [38] | |
| Independent Walking for Brain Health [39] | |
| CAPTAIN [40] | |
| PERSSILAA [47] | |
| Social | NESTORE [37] |
| CAPTAIN [40] | |
| SONOPA [41] | |
| AGNES [45] | |
| PERSSILAA [47] | |
| Miraculous Project [48] | |
| Impronte Project [50] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernardo, J.; Apóstolo, J.; Loureiro, R.; Santana, E.; Yaylagul, N.K.; Dantas, C.; Ventura, F.; Duque, F.M.; Jøranson, N.; Zechner, M.; et al. eHealth Platforms to Promote Autonomous Life and Active Aging: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 15940. https://doi.org/10.3390/ijerph192315940
Bernardo J, Apóstolo J, Loureiro R, Santana E, Yaylagul NK, Dantas C, Ventura F, Duque FM, Jøranson N, Zechner M, et al. eHealth Platforms to Promote Autonomous Life and Active Aging: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(23):15940. https://doi.org/10.3390/ijerph192315940
Chicago/Turabian StyleBernardo, Joana, João Apóstolo, Ricardo Loureiro, Elaine Santana, Nilufer Korkmaz Yaylagul, Carina Dantas, Filipa Ventura, Filipa Margarida Duque, Nina Jøranson, Minna Zechner, and et al. 2022. "eHealth Platforms to Promote Autonomous Life and Active Aging: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 23: 15940. https://doi.org/10.3390/ijerph192315940
APA StyleBernardo, J., Apóstolo, J., Loureiro, R., Santana, E., Yaylagul, N. K., Dantas, C., Ventura, F., Duque, F. M., Jøranson, N., Zechner, M., Staalduinen, W. v., De Luca, V., Illario, M., & Silva, R. (2022). eHealth Platforms to Promote Autonomous Life and Active Aging: A Scoping Review. International Journal of Environmental Research and Public Health, 19(23), 15940. https://doi.org/10.3390/ijerph192315940