

Hospice Care Improves Patients’ Self-Decision Making and Reduces Aggressiveness of End-of-Life Care for Advanced Cancer Patients


Abstract
1. Introduction
2. Materials and Methods
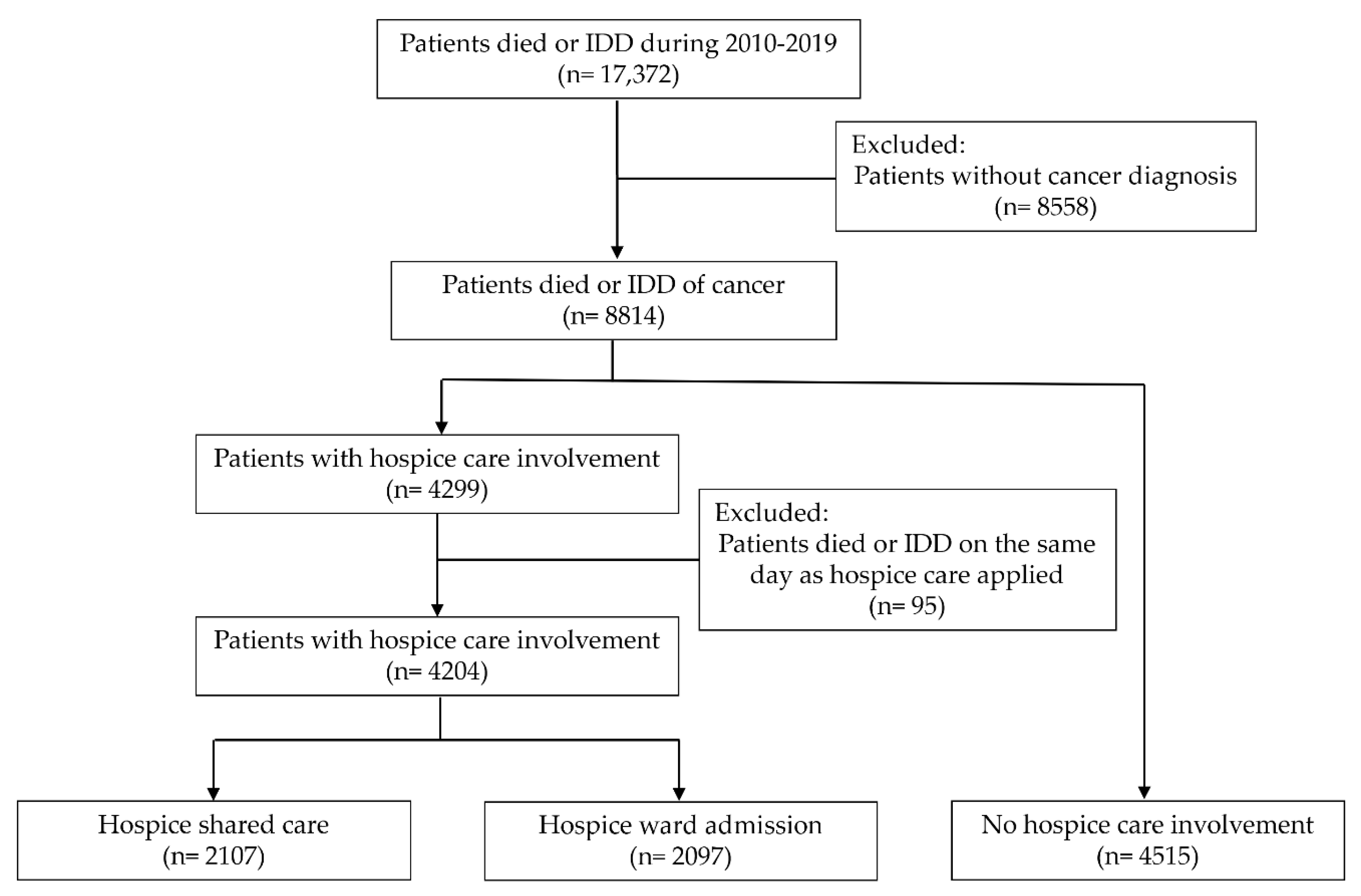
2.1. Data Source and Study Patients
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics by Status and Type of Hospice Care
3.2. Primary Outcome
3.3. Indicators of Aggressiveness of Cancer Care at the End of Life
3.4. Factors Associated with Aggressiveness of Cancer Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- 2020 Cancer Detail. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 3 February 2022).
- Ministry of Health and Welfare. 2019 Cause of Death Statistics. Available online: https://www.mohw.gov.tw/cp-4964-55572-2.html (accessed on 11 May 2021).
- Ruijs, C.D.; Kerkhof, A.J.; van der Wal, G.; Onwuteaka-Philipsen, B.D. Symptoms, unbearability and the nature of suffering in terminal cancer patients dying at home: A prospective primary care study. BMC Fam. Pract. 2013, 14, 201. [Google Scholar] [CrossRef] [PubMed]
- Tai, S.Y.; Lee, C.Y.; Wu, C.Y.; Hsieh, H.Y.; Huang, J.J.; Huang, C.T.; Chien, C.Y. Symptom severity of patients with advanced cancer in palliative care unit: Longitudinal assessments of symptoms improvement. BMC Palliat. Care 2016, 15, 32. [Google Scholar] [CrossRef] [PubMed]
- Morasso, G.; Capelli, M.; Viterbori, P.; Di Leo, S.; Alberisio, A.; Costantini, M.; Fiore, M.; Saccani, D.; Zeitler, G.; Verzolatto, N.; et al. Psychological and symptom distress in terminal cancer patients with met and unmet needs. J. Pain Symptom. Manag. 1999, 17, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Polley, M.J.; Jolliffe, R.; Boxell, E.; Zollman, C.; Jackson, S.; Seers, H. Using a whole person approach to support people with cancer: A longitudinal, mixed-methods service evaluation. Integr. Cancer Ther. 2016, 15, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Nalley, C. The calm model: Addressing the whole person in cancer care. Oncol. Times 2019, 41, 28. [Google Scholar] [CrossRef]
- Jordhøy, M.S.; Fayers, P.; Saltnes, T.; Ahlner-Elmqvist, M.; Jannert, M.; Kaasa, S. A palliative-care intervention and death at home: A cluster randomised trial. Lancet 2000, 356, 888–893. [Google Scholar] [CrossRef]
- Earle, C.C.; Park, E.R.; Lai, B.; Weeks, J.C.; Ayanian, J.Z.; Block, S. Identifying potential indicators of the quality of end-of-life cancer care from administrative data. J. Clin. Oncol. 2003, 21, 1133–1138. [Google Scholar] [CrossRef]
- Earle, C.C.; Neville, B.A.; Landrum, M.B.; Ayanian, J.Z.; Block, S.D.; Weeks, J.C. Trends in the aggressiveness of cancer care near the end of life. J. Clin. Oncol. 2004, 22, 315–321. [Google Scholar] [CrossRef]
- Earle, C.C.; Neville, B.A.; Landrum, M.B.; Souza, J.M.; Weeks, J.C.; Block, S.D.; Grunfeld, E.; Ayanian, J.Z. Evaluating claims-based indicators of the intensity of end-of-life cancer care. Int. J. Qual. Health Care 2005, 17, 505–509. [Google Scholar] [CrossRef]
- Earle, C.C.; Landrum, M.B.; Souza, J.M.; Neville, B.A.; Weeks, J.C.; Ayanian, J.Z. Aggressiveness of cancer care near the end of life: Is it a quality-of-care issue? J. Clin. Oncol. 2008, 26, 3860–3866. [Google Scholar] [CrossRef]
- Barbera, L.; Paszat, L.; Chartier, C. Indicators of poor quality end-of-life cancer care in ontario. J. Palliat. Care 2006, 22, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Colombet, I.; Bouleuc, C.; Piolot, A.; Vilfaillot, A.; Jaulmes, H.; Voisin-Saltiel, S.; Goldwasser, F.; Vinant, P. Multicentre analysis of intensity of care at the end-of-life in patients with advanced cancer, combining health administrative data with hospital records: Variations in practice call for routine quality evaluation. BMC Palliat. Care 2019, 18, 35. [Google Scholar] [CrossRef] [PubMed]
- Martins-Branco, D.; Lopes, S.; Canario, R.; Freire, J.; Feio, M.; Ferraz-Goncalves, J.; Sousa, G.; Lunet, N.; Gomes, B. Factors associated with the aggressiveness of care at the end of life for patients with cancer dying in hospital: A nationwide retrospective cohort study in mainland portugal. ESMO Open 2020, 5, e000953. [Google Scholar] [CrossRef] [PubMed]
- Luta, X.; Maessen, M.; Egger, M.; Stuck, A.E.; Goodman, D.; Clough-Gorr, K.M. Measuring intensity of end of life care: A systematic review. PLoS ONE 2015, 10, e0123764. [Google Scholar] [CrossRef]
- Wright, A.A.; Zhang, B.; Ray, A.; Mack, J.W.; Trice, E.; Balboni, T.; Mitchell, S.L.; Jackson, V.A.; Block, S.D.; Maciejewski, P.K.; et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008, 300, 1665–1673. [Google Scholar] [CrossRef]
- Loke, S.S.; Rau, K.M.; Huang, C.F. Impact of combined hospice care on terminal cancer patients. J. Palliat. Med. 2011, 14, 683–687. [Google Scholar] [CrossRef]
- Shao, Y.Y.; Hsiue, E.H.; Hsu, C.H.; Yao, C.A.; Chen, H.M.; Lai, M.S.; Cheng, A.L. National policies fostering hospice care increased hospice utilization and reduced the invasiveness of end-of-life care for cancer patients. Oncologist 2017, 22, 843–849. [Google Scholar] [CrossRef]
- Hughes, S.L.; Weaver, F.M.; Giobbie-Hurder, A.; Manheim, L.; Henderson, W.; Kubal, J.D.; Ulasevich, A.; Cummings, J. Effectiveness of team-managed home-based primary care: A randomized multicenter trial. JAMA 2000, 284, 2877–2885. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.E.; Todd, C.J.; Barclay, S.I.; Farquhar, M.C. A randomized controlled trial of a hospital at home service for the terminally ill. Palliat. Med. 2000, 14, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.L.; Wales, J.; Bernstein, L.; Leibowitz, A.; Kaplan, S. A randomised controlled trial of hospice care. Lancet 1984, 1, 890–894. [Google Scholar] [CrossRef] [PubMed]
- Rabow, M.W.; Dibble, S.L.; Pantilat, S.Z.; McPhee, S.J. The comprehensive care team: A controlled trial of outpatient palliative medicine consultation. Arch. Intern. Med. 2004, 164, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.K.; Lee, Y.C.; Kao, Y.H. Trend analysis of end-of-life care between hospice and nonhospice groups of cancer patients in taiwan for 2002-11. Medicine 2017, 96, e7825. [Google Scholar] [CrossRef]
- Lai, C.F.; Tsai, H.B.; Hsu, S.H.; Chiang, C.K.; Huang, J.W.; Huang, S.J. Withdrawal from long-term hemodialysis in patients with end-stage renal disease in taiwan. J. Formos Med. Assoc. 2013, 112, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, W.H.; Wang, C.L.; Lee, L.C.; Chien, S.P.; Hsu, C.C.; Chu, W.M. Exploring risk factors of unexpected death, using palliative care outcomes collaboration (pcoc) measures, among terminal patients receiving palliative care in taiwan. Int. J. Environ. Res. Public Health 2022, 19, 13294. [Google Scholar] [CrossRef]
- Chen, H.C.; Wu, C.Y.; Hsieh, H.Y.; He, J.S.; Hwang, S.J.; Hsieh, H.M. Predictors and assessment of hospice use for end-stage renal disease patients in taiwan. Int. J. Environ. Res. Public Health 2021, 19, 85. [Google Scholar] [CrossRef]
- Shih, T.C.; Chang, H.T.; Lin, M.H.; Chen, C.K.; Chen, T.J.; Hwang, S.J. Differences in do-not-resuscitate orders, hospice care utilization, and late referral to hospice care between cancer and non-cancer decedents in a tertiary hospital in taiwan between 2010 and 2015: A hospital-based observational study. BMC Palliat. Care 2018, 17, 18. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Chiu, T.Y.; Ho, C.T.; Davidson, L.E.; Hsu, H.S.; Liu, C.S.; Chiu, C.F.; Peng, C.T.; Chen, C.Y.; Hu, W.Y.; et al. Hospice shared-care saved medical expenditure and reduced the likelihood of intensive medical utilization among advanced cancer patients in taiwan--a nationwide survey. Support. Care Cancer 2014, 22, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- Barbera, L.; Seow, H.; Sutradhar, R.; Chu, A.; Burge, F.; Fassbender, K.; McGrail, K.; Lawson, B.; Liu, Y.; Pataky, R.; et al. Quality indicators of end-of-life care in patients with cancer: What rate is right? J. Oncol. Pract. 2015, 11, e279–e287. [Google Scholar] [CrossRef] [PubMed]
- Colombet, I.; Montheil, V.; Durand, J.P.; Gillaizeau, F.; Niarra, R.; Jaeger, C.; Alexandre, J.; Goldwasser, F.; Vinant, P. Effect of integrated palliative care on the quality of end-of-life care: Retrospective analysis of 521 cancer patients. BMJ Support. Palliat. Care 2012, 2, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.P.; Hui, D. Quality of life in palliative care. Expert Rev. Qual. Life Cancer Care 2017, 2, 293–302. [Google Scholar] [CrossRef]
- Pratheepawanit, N.; Salek, M.S.; Finlay, I.G. The applicability of quality-of-life assessment in palliative care: Comparing two quality-of-life measures. Palliat. Med. 1999, 13, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Walbert, T. Maintaining quality of life near the end of life: Hospice in neuro-oncology. Neuro Oncol. 2018, 20, 439–440. [Google Scholar] [CrossRef]
- Teno, J.M.; Clarridge, B.R.; Casey, V.; Welch, L.C.; Wetle, T.; Shield, R.; Mor, V. Family perspectives on end-of-life care at the last place of care. JAMA 2004, 291, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Ersek, M.; Miller, S.C.; Wagner, T.H.; Thorpe, J.M.; Smith, D.; Levy, C.R.; Gidwani, R.; Faricy-Anderson, K.; Lorenz, K.A.; Kinosian, B.; et al. Association between aggressive care and bereaved families’ evaluation of end-of-life care for veterans with non-small cell lung cancer who died in veterans affairs facilities. Cancer 2017, 123, 3186–3194. [Google Scholar] [CrossRef]
- Mor, V.; Kidder, D. Cost savings in hospice: Final results of the national hospice study. Health Serv. Res. 1985, 20, 407–422. [Google Scholar]
- Brooks, C.H.; Smyth-Staruch, K. Hospice home care cost savings to third-party insurers. Med. Care 1984, 22, 691–703. [Google Scholar] [CrossRef]
- Kidder, D. The effects of hospice coverage on medicare expenditures. Health Serv. Res. 1992, 27, 195–217. [Google Scholar] [PubMed]
- Smith, S.; Brick, A.; O’Hara, S.; Normand, C. Evidence on the cost and cost-effectiveness of palliative care: A literature review. Palliat. Med. 2014, 28, 130–150. [Google Scholar] [CrossRef]
- Houska, A.; Loučka, M. Patients’ autonomy at the end of life: A critical review. J. Pain Symptom. Manag. 2019, 57, 835–845. [Google Scholar] [CrossRef]
- Steinhauser, K.E.; Christakis, N.A.; Clipp, E.C.; McNeilly, M.; McIntyre, L.; Tulsky, J.A. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000, 284, 2476–2482. [Google Scholar] [CrossRef]
- Sekimoto, M.; Asai, A.; Ohnishi, M.; Nishigaki, E.; Fukui, T.; Shimbo, T.; Imanaka, Y. Patients’ preferences for involvement in treatment decision making in japan. BMC Fam. Pract. 2004, 5, 1. [Google Scholar] [CrossRef]
- Yao, C.A.; Hu, W.Y.; Lai, Y.F.; Cheng, S.Y.; Chen, C.Y.; Chiu, T.Y. Does dying at home influence the good death of terminal cancer patients? J. Pain Symptom Manag. 2007, 34, 497–504. [Google Scholar] [CrossRef]
- Tang, S.T. When death is imminent: Where terminally ill patients with cancer prefer to die and why. Cancer Nurs. 2003, 26, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Townsend, J.; Frank, A.O.; Fermont, D.; Dyer, S.; Karran, O.; Walgrove, A.; Piper, M. Terminal cancer care and patients’ preference for place of death: A prospective study. BMJ 1990, 301, 415–417. [Google Scholar] [CrossRef]
- Higginson, I.J.; Sen-Gupta, G.J. Place of care in advanced cancer: A qualitative systematic literature review of patient preferences. J. Palliat. Med. 2000, 3, 287–300. [Google Scholar] [CrossRef]
- Chiu, T.Y.; Hu, W.Y.; Cheng, S.Y.; Chen, C.Y. Ethical dilemmas in palliative care: A study in taiwan. J. Med. Ethics 2000, 26, 353–357. [Google Scholar] [CrossRef]
- Henson, L.A.; Maddocks, M.; Evans, C.; Davidson, M.; Hicks, S.; Higginson, I.J. Palliative care and the management of common distressing symptoms in advanced cancer: Pain, breathlessness, nausea and vomiting, and fatigue. J. Clin. Oncol 2020, 38, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, S.C.; Wesker, W.; Kruitwagen, C.; de Haes, H.C.; Voest, E.E.; de Graeff, A. Symptom prevalence in patients with incurable cancer: A systematic review. J. Pain Symptom. Manag. 2007, 34, 94–104. [Google Scholar] [CrossRef]
- Tsai, J.S.; Wu, C.H.; Chiu, T.Y.; Hu, W.Y.; Chen, C.Y. Symptom patterns of advanced cancer patients in a palliative care unit. Palliat. Med. 2006, 20, 617–622. [Google Scholar] [CrossRef]
- Verkissen, M.N.; Hjermstad, M.J.; Van Belle, S.; Kaasa, S.; Deliens, L.; Pardon, K. Quality of life and symptom intensity over time in people with cancer receiving palliative care: Results from the international european palliative care cancer symptom study. PLoS ONE 2019, 14, e0222988. [Google Scholar] [CrossRef] [PubMed]
- Santomassino, M.; Costantini, G.D.; McDermott, M.; Primiano, D.; Slyer, J.T.; Singleton, J.K. A systematic review on the effectiveness of continuity of care and its role in patient satisfaction and decreased hospital readmissions in the adult patient receiving home care services. JBI Libr. Syst. Rev. 2012, 10, 1214–1259. [Google Scholar] [CrossRef] [PubMed]
- Tralongo, P.; Ferraù, F.; Borsellino, N.; Verderame, F.; Caruso, M.; Giuffrida, D.; Butera, A.; Gebbia, V. Cancer patient-centered home care: A new model for health care in oncology. Ther. Clin. Risk Manag. 2011, 7, 387–392. [Google Scholar]
- Lindsay, J.; Dooley, M.; Martin, J.; Fay, M.; Kearney, A.; Barras, M. Reducing potentially inappropriate medications in palliative cancer patients: Evidence to support deprescribing approaches. Support. Care Cancer 2014, 22, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Lees, J.; Chan, A. Polypharmacy in elderly patients with cancer: Clinical implications and management. Lancet Oncol. 2011, 12, 1249–1257. [Google Scholar] [CrossRef]
- Sera, L.; McPherson, M.L.; Holmes, H.M. Commonly prescribed medications in a population of hospice patients. Am. J. Hosp. Palliat Care 2014, 31, 126–131. [Google Scholar] [CrossRef]
- Lundy, E.; McMullan, D.; McShane, P.; Williams, M.; Watson, M.; White, C. Polypharmacy and drug omissions across hospices in northern ireland. J. Palliat. Med. 2013, 16, 1446–1449. [Google Scholar] [CrossRef]
- Schenker, Y.; Park, S.Y.; Jeong, K.; Pruskowski, J.; Kavalieratos, D.; Resick, J.; Abernethy, A.; Kutner, J.S. Associations between polypharmacy, symptom burden, and quality of life in patients with advanced, life-limiting illness. J. Gen. Intern. Med. 2019, 34, 559–566. [Google Scholar] [CrossRef]
- Kutner, J.S.; Blatchford, P.J.; Taylor, D.H., Jr.; Ritchie, C.S.; Bull, J.H.; Fairclough, D.L.; Hanson, L.C.; LeBlanc, T.W.; Samsa, G.P.; Wolf, S.; et al. Safety and benefit of discontinuing statin therapy in the setting of advanced, life-limiting illness: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Pasierski, T. Modification of cardiovascular pharmacotherapy in palliative care patients with cancer: A narrative review. Pol. Arch. Intern. Med. 2017, 127, 687–693. [Google Scholar] [CrossRef]
- Lindsay, J.; Dooley, M.; Martin, J.; Fay, M.; Kearney, A.; Khatun, M.; Barras, M. The development and evaluation of an oncological palliative care deprescribing guideline: The ‘oncpal deprescribing guideline’. Support. Care Cancer 2015, 23, 71–78. [Google Scholar] [CrossRef]
- Kvalheim, S.F.; Marthinussen, I.M.C.; Berg, E.; Strand, G.V. Dry mouth in the seriously ill and dying. Tidsskr. Nor. Laegeforen. 2022, 142. [Google Scholar] [CrossRef]
- Chiu, T.Y.; Hu, W.Y.; Chuang, R.B.; Chen, C.Y. Nutrition and hydration for terminal cancer patients in taiwan. Support. Care Cancer 2002, 10, 630–636. [Google Scholar] [CrossRef]
- Mercadante, S.; Ferrera, P.; Girelli, D.; Casuccio, A. Patients’ and relatives’ perceptions about intravenous and subcutaneous hydration. J. Pain Symptom. Manag. 2005, 30, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Bruera, E.; Hui, D.; Dalal, S.; Torres-Vigil, I.; Trumble, J.; Roosth, J.; Krauter, S.; Strickland, C.; Unger, K.; Palmer, J.L.; et al. Parenteral hydration in patients with advanced cancer: A multicenter, double-blind, placebo-controlled randomized trial. J. Clin. Oncol. 2013, 31, 111–118. [Google Scholar] [CrossRef] [PubMed]
- McCann, R.M.; Hall, W.J.; Groth-Juncker, A. Comfort care for terminally ill patients. The appropriate use of nutrition and hydration. JAMA 1994, 272, 1263–1266. [Google Scholar] [CrossRef] [PubMed]
- Meier, E.A.; Gallegos, J.V.; Thomas, L.P.; Depp, C.A.; Irwin, S.A.; Jeste, D.V. Defining a good death (successful dying): Literature review and a call for research and public dialogue. Am. J. Geriatr. Psychiatry 2016, 24, 261–271. [Google Scholar] [CrossRef]
- Dawson, N.J. Need satisfaction in terminal care settings. Soc. Sci Med. 1991, 32, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.M.; Landrum, M.B.; Neville, B.A.; Ayanian, J.Z.; Weeks, J.C.; Earle, C.C. Hospice care and survival among elderly patients with lung cancer. J. Palliat. Med. 2011, 14, 929–939. [Google Scholar] [CrossRef]
- Connor, S.R.; Pyenson, B.; Fitch, K.; Spence, C.; Iwasaki, K. Comparing hospice and nonhospice patient survival among patients who die within a three-year window. J. Pain Symptom. Manag. 2007, 33, 238–246. [Google Scholar] [CrossRef]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.F.; et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Gott, M.; Morgan, T.; Williams, L. Gender and palliative care: A call to arms. Palliat. Care Soc. Pract. 2020, 14, 2632352420957997. [Google Scholar] [CrossRef]
- Miesfeldt, S.; Murray, K.; Lucas, L.; Chang, C.H.; Goodman, D.; Morden, N.E. Association of age, gender, and race with intensity of end-of-life care for medicare beneficiaries with cancer. J. Palliat. Med. 2012, 15, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Saeed, F.; Hoerger, M.; Norton, S.A.; Guancial, E.; Epstein, R.M.; Duberstein, P.R. Preference for palliative care in cancer patients: Are men and women alike? J. Pain Symptom. Manag. 2018, 56, 1–6.e1. [Google Scholar] [CrossRef] [PubMed]
- Legler, A.; Bradley, E.H.; Carlson, M.D. The effect of comorbidity burden on health care utilization for patients with cancer using hospice. J. Palliat. Med. 2011, 14, 751–756. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 8719) | Hospice Shared Care (n = 2107) | Hospice Ward Admission (n = 2097) | No Hospice Care Involvement (n = 4515) | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Age | 65.42 | ±14.21 | 64.46 | ±13.82 | 65.64 | ±14.48 | 65.76 | ±14.24 | 0.001 ** |
| Gender | 0.002 ** | ||||||||
| Female | 2952 | (33.86%) | 728 | (34.55%) | 767 | (36.58%) | 1457 | (32.27%) | |
| Male | 5767 | (66.14%) | 1379 | (65.45%) | 1330 | (63.42%) | 3058 | (67.73%) | |
| Length of last admission stay | 19.56 | ±20.11 | 23.85 | ±21.60 | 18.97 | ±19.50 | 17.82 | ±19.37 | <0.001 ** |
| Cancer diagnosis | <0.001 ** | ||||||||
| Lung | 2344 | (26.88%) | 634 | (30.09%) | 388 | (18.50%) | 1322 | (29.28%) | |
| Liver | 1661 | (19.05%) | 390 | (18.51%) | 387 | (18.45%) | 884 | (19.58%) | |
| Hematologic | 947 | (10.86%) | 203 | (9.63%) | 84 | (4.01%) | 660 | (14.62%) | |
| Colorectal | 676 | (7.75%) | 177 | (8.40%) | 212 | (10.11%) | 287 | (6.36%) | |
| Head and neck | 721 | (8.27%) | 153 | (7.26%) | 270 | (12.88%) | 298 | (6.60%) | |
| Esophageal | 399 | (4.58%) | 92 | (4.37%) | 117 | (5.58%) | 190 | (4.21%) | |
| Gastric | 350 | (4.01%) | 81 | (3.84%) | 114 | (5.44%) | 155 | (3.43%) | |
| GYN cancer | 259 | (2.97%) | 55 | (2.61%) | 88 | (4.20%) | 116 | (2.57%) | |
| Breast | 203 | (2.33%) | 40 | (1.90%) | 85 | (4.05%) | 78 | (1.73%) | |
| Prostate | 184 | (2.11%) | 31 | (1.47%) | 60 | (2.86%) | 93 | (2.06%) | |
| Bladder | 175 | (2.01%) | 26 | (1.23%) | 51 | (2.43%) | 98 | (2.17%) | |
| Pancreases | 406 | (4.66%) | 117 | (5.55%) | 138 | (6.58%) | 151 | (3.34%) | |
| Other | 394 | (4.52%) | 108 | (5.13%) | 103 | (4.91%) | 183 | (4.05%) | |
| Comorbidity | |||||||||
| Ischemic heart diseases | 1298 | (14.89%) | 296 | (14.05%) | 304 | (14.50%) | 698 | (15.46%) | 0.274 |
| Cerebral infarction | 313 | (3.59%) | 95 | (4.51%) | 76 | (3.62%) | 142 | (3.15%) | 0.021 * |
| Hypertension | 3907 | (44.81%) | 907 | (43.05%) | 958 | (45.68%) | 2042 | (45.23%) | 0.164 |
| T2DM | 2340 | (26.84%) | 559 | (26.53%) | 530 | (25.27%) | 1251 | (27.71%) | 0.108 |
| CKD | 2765 | (31.71%) | 829 | (39.35%) | 618 | (29.47%) | 1318 | (29.19%) | <0.001 ** |
| COPD | 1791 | (20.54%) | 403 | (19.13%) | 390 | (18.60%) | 998 | (22.10%) | 0.001 ** |
| Liver cirrhosis | 1717 | (19.69%) | 405 | (19.22%) | 367 | (17.50%) | 945 | (20.93%) | 0.004 ** |
| Place of death | <0.001 ** | ||||||||
| Home | 3928 | (45.05%) | 1050 | (49.83%) | 402 | (19.17%) | 2476 | (54.84%) | |
| Hospital | 4791 | (54.95%) | 1057 | (50.17%) | 1695 | (80.83%) | 2039 | (45.16%) | |
| Hospice Shared Care (n = 2107) | Hospice Ward Admission (n = 2097) | No Hospice Care Involvement (n = 4515) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Healthcare resources use | |||||||
| >1 hospitalization | 391 | (18.56%) | 449 | (21%) | 960 | (21.26%) | 0.025 * |
| >14 days of hospitalization | 1382 | (65.59%) | 1126 | (54%) | 2227 | (49.32%) | <0.001 ** |
| ≥1 emergency department visit | 1230 | (58.38%) | 1305 | (62%) | 2994 | (66.31%) | <0.001 ** |
| ≥1 intensive care unit admission | 362 | (17.18%) | 51 | (2%) | 1313 | (29.08%) | <0.001 ** |
| Aggressive medication administration | |||||||
| antineoplastic drug administration | 243 | (11.53%) | 44 | (2%) | 553 | (12.25%) | <0.001 ** |
| excessive numbers of medication administration | 1198 | (56.86%) | 580 | (28%) | 2430 | (53.82%) | <0.001 ** |
| Life-sustaining treatments | |||||||
| cardiopulmonary resuscitation | 18 | (0.85%) | 0 | (0%) | 278 | (6.16%) | <0.001 ** |
| insertion of endotracheal tube with mechanical ventilation | 164 | (7.78%) | 7 | (0%) | 856 | (18.96%) | <0.001 ** |
| vasopressor support | 967 | (45.89%) | 486 | (23%) | 2899 | (64.21%) | <0.001 ** |
| tracheostomy | 4 | (0.19%) | 1 | (0%) | 16 | (0.35%) | 0.052 |
| placement of nasogastric tube | 226 | (10.73%) | 165 | (8%) | 791 | (17.52%) | <0.001 ** |
| implantation of central vascular catheter | 278 | (13.19%) | 41 | (2%) | 939 | (20.80%) | <0.001 ** |
| excessive parenteral infusion of nutrition | 959 | (45.51%) | 120 | (6%) | 2171 | (48.08%) | <0.001 ** |
| the imbalance of input and output fluid | 927 | (44.00%) | 133 | (6%) | 2168 | (48.02%) | <0.001 ** |
| surgical intervention | 227 | (10.77%) | 70 | (3%) | 489 | (10.83%) | <0.001 ** |
| hemodialysis | 68 | (3.23%) | 12 | (1%) | 149 | (3.30%) | <0.001 ** |
| ACCEoL ≤ 5 (n = 6651) | ACCEoL > 5 (n = 2068) | p Value | |||
|---|---|---|---|---|---|
| Status and type of hospice care | <0.001 ** | ||||
| hospice shared care | 1622 | (24.39%) | 485 | (23.45%) | |
| hospice ward admission | 2070 | (31.12%) | 27 | (1.31%) | |
| no hospice care | 2959 | (44.49%) | 1556 | (75.24%) | |
| Age | 65.71 | ±14.18 | 64.47 | ±14.26 | 0.003 ** |
| Age | <0.001 ** | ||||
| 20–39 | 236 | (3.55%) | 111 | (5.37%) | |
| 40–59 | 2120 | (31.87%) | 653 | (31.58%) | |
| 60–79 | 3078 | (46.28%) | 980 | (47.39%) | |
| >79 | 1217 | (18.30%) | 324 | (15.67%) | |
| Gender | <0.001 ** | ||||
| Female | 2339 | (35.17%) | 613 | (29.64%) | |
| Male | 4312 | (64.83%) | 1455 | (70.36%) | |
| Cancer diagnosis | <0.001 ** | ||||
| Lung | 1878 | (28.24%) | 466 | (22.53%) | |
| Liver | 1323 | (19.89%) | 338 | (16.34%) | |
| Hematologic | 537 | (8.07%) | 410 | (19.83%) | |
| Colorectal | 490 | (7.37%) | 186 | (8.99%) | |
| Head and neck | 576 | (8.66%) | 145 | (7.01%) | |
| Esophageal | 284 | (4.27%) | 115 | (5.56%) | |
| Gastric | 290 | (4.36%) | 60 | (2.90%) | |
| GYN cancer | 208 | (3.13%) | 51 | (2.47%) | |
| Breast | 177 | (2.66%) | 26 | (1.26%) | |
| Prostate | 149 | (2.24%) | 35 | (1.69%) | |
| Bladder | 113 | (1.70%) | 62 | (3.00%) | |
| Pancreases | 346 | (5.20%) | 60 | (2.90%) | |
| Other | 280 | (4.21%) | 114 | (5.51%) | |
| Death in the hospital | 3849 | (57.87%) | 942 | (45.55%) | <0.001 ** |
| Signed DNR order | 5290 | (79.54%) | 1548 | (74.85%) | <0.001 ** |
| Type of DNR order | <0.001 ** | ||||
| Signed by the patient | 1900 | (35.92%) | 248 | (16.02%) | |
| Signed by the family or surrogate | 3390 | (64.08%) | 1300 | (83.98%) | |
| Simple Model | Multiple Model | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Status and type of hospice care | ||||||
| Hospice shared care | 0.57 | (0.51–0.64) | <0.001 ** | 0.44 | (0.37–0.51) | <0.001 ** |
| Hospice ward admission | 0.02 | (0.02–0.04) | <0.001 ** | 0.02 | (0.01–0.03) | <0.001 ** |
| No hospice care | ref. | ref. | ||||
| Gender | ||||||
| Female | ref. | ref. | ||||
| Male | 1.29 | (1.16–1.43) | <0.001 ** | 1.27 | (1.09–1.47) | 0.002 ** |
| Age | ||||||
| 18–39 | ref. | ref. | ||||
| 40–59 | 0.65 | (0.51–0.83) | 0.001 ** | 0.72 | (0.52–1.01) | 0.056 |
| 60–79 | 0.68 | (0.53–0.86) | 0.001 ** | 0.75 | (0.54–1.05) | 0.094 |
| >79 | 0.57 | (0.44–0.73) | <0.001 ** | 0.62 | (0.43–0.89) | 0.009 ** |
| p for trend | 0.001 ** | 0.005 ** | ||||
| Cancer diagnosis | ||||||
| Lung | ref. | ref. | ||||
| Liver | 1.03 | (0.88–1.20) | 0.715 | 1.11 | (0.91–1.35) | 0.307 |
| Hematologic | 3.08 | (2.61–3.62) | <0.001 ** | 2.37 | (1.93–2.92) | <0.001 ** |
| Colorectal | 1.53 | (1.26–1.86) | <0.001 ** | 2.31 | (1.79–2.99) | <0.001 ** |
| Head and neck | 1.01 | (0.82–1.25) | 0.892 | 1.71 | (1.30–2.26) | <0.001 ** |
| Esophageal | 1.63 | (1.28–2.07) | <0.001 ** | 2.42 | (1.74–3.35) | <0.001 ** |
| Gastric | 0.83 | (0.62–1.12) | 0.229 | 0.87 | (0.59–1.29) | 0.502 |
| GYN cancer | 0.99 | (0.72–1.36) | 0.942 | 1.59 | (1.03–2.47) | 0.038 * |
| Breast | 0.59 | (0.39–0.90) | 0.015 * | 0.89 | (0.50–1.55) | 0.670 |
| Prostate | 0.95 | (0.65–1.39) | 0.778 | 1.00 | (0.59–1.71) | 0.997 |
| Bladder | 2.21 | (1.60–3.06) | <0.001 ** | 2.62 | (1.63–4.21) | <0.001 ** |
| Pancreases | 0.70 | (0.52–0.94) | 0.016 * | 0.90 | (0.63–1.28) | 0.559 |
| Other | 1.64 | (1.29–2.09) | <0.001 ** | 1.65 | (1.19–2.27) | 0.002 ** |
| Comorbidity | ||||||
| Ischemic heart diseases | 1.17 | (1.03–1.34) | 0.019* | 1.25 | (1.04–1.51) | 0.020 * |
| Cerebral infarction | 0.84 | (0.63–1.11) | 0.212 | |||
| Hypertension | 0.94 | (0.85–1.04) | 0.212 | |||
| T2DM | 1.03 | (0.92–1.15) | 0.650 | |||
| CKD | 1.06 | (0.96–1.18) | 0.252 | |||
| COPD | 0.95 | (0.84–1.08) | 0.462 | |||
| Liver cirrhosis | 0.96 | (0.85–1.09) | 0.517 | |||
| Place of death | ||||||
| Home | ref. | ref. | ||||
| Hospital | 0.61 | (0.55–0.67) | <0.001 ** | 0.92 | (0.80–1.05) | 0.197 |
| Signed DNR order | ||||||
| No | 1.31 | (1.16–1.47) | <0.001 ** | 1.23 | (1.09–1.39) | 0.001 ** |
| Yes | ref. | ref. | ||||
| Type of DNR order | ||||||
| Signed by the patient | ref. | ref. | ||||
| Signed by the family or surrogate | 2.94 | (2.54–3.40) | <0.001 ** | 1.94 | (1.64–2.29) | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-L.; Lin, C.-Y.; Yang, S.-F. Hospice Care Improves Patients’ Self-Decision Making and Reduces Aggressiveness of End-of-Life Care for Advanced Cancer Patients. Int. J. Environ. Res. Public Health 2022, 19, 15593. https://doi.org/10.3390/ijerph192315593
Wang C-L, Lin C-Y, Yang S-F. Hospice Care Improves Patients’ Self-Decision Making and Reduces Aggressiveness of End-of-Life Care for Advanced Cancer Patients. International Journal of Environmental Research and Public Health. 2022; 19(23):15593. https://doi.org/10.3390/ijerph192315593
Chicago/Turabian StyleWang, Chun-Li, Chia-Yen Lin, and Shun-Fa Yang. 2022. "Hospice Care Improves Patients’ Self-Decision Making and Reduces Aggressiveness of End-of-Life Care for Advanced Cancer Patients" International Journal of Environmental Research and Public Health 19, no. 23: 15593. https://doi.org/10.3390/ijerph192315593
APA StyleWang, C.-L., Lin, C.-Y., & Yang, S.-F. (2022). Hospice Care Improves Patients’ Self-Decision Making and Reduces Aggressiveness of End-of-Life Care for Advanced Cancer Patients. International Journal of Environmental Research and Public Health, 19(23), 15593. https://doi.org/10.3390/ijerph192315593