


In Schizophrenia, the Effects of the IL-6/IL-23/Th17 Axis on Health-Related Quality of Life and Disabilities Are Partly Mediated by Generalized Cognitive Decline and the Symptomatome


 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Subjects and Methods
2.1. Participants
2.2. Clinical Assessments
2.3. Assays
2.4. Statistical Analysis
3. Results
3.1. Socio-Demographic Data
3.2. Differences in Clinical Ratings between the Three DisQoL Groups
3.3. Differences in Biomarkers between the Three DisQoL Groups
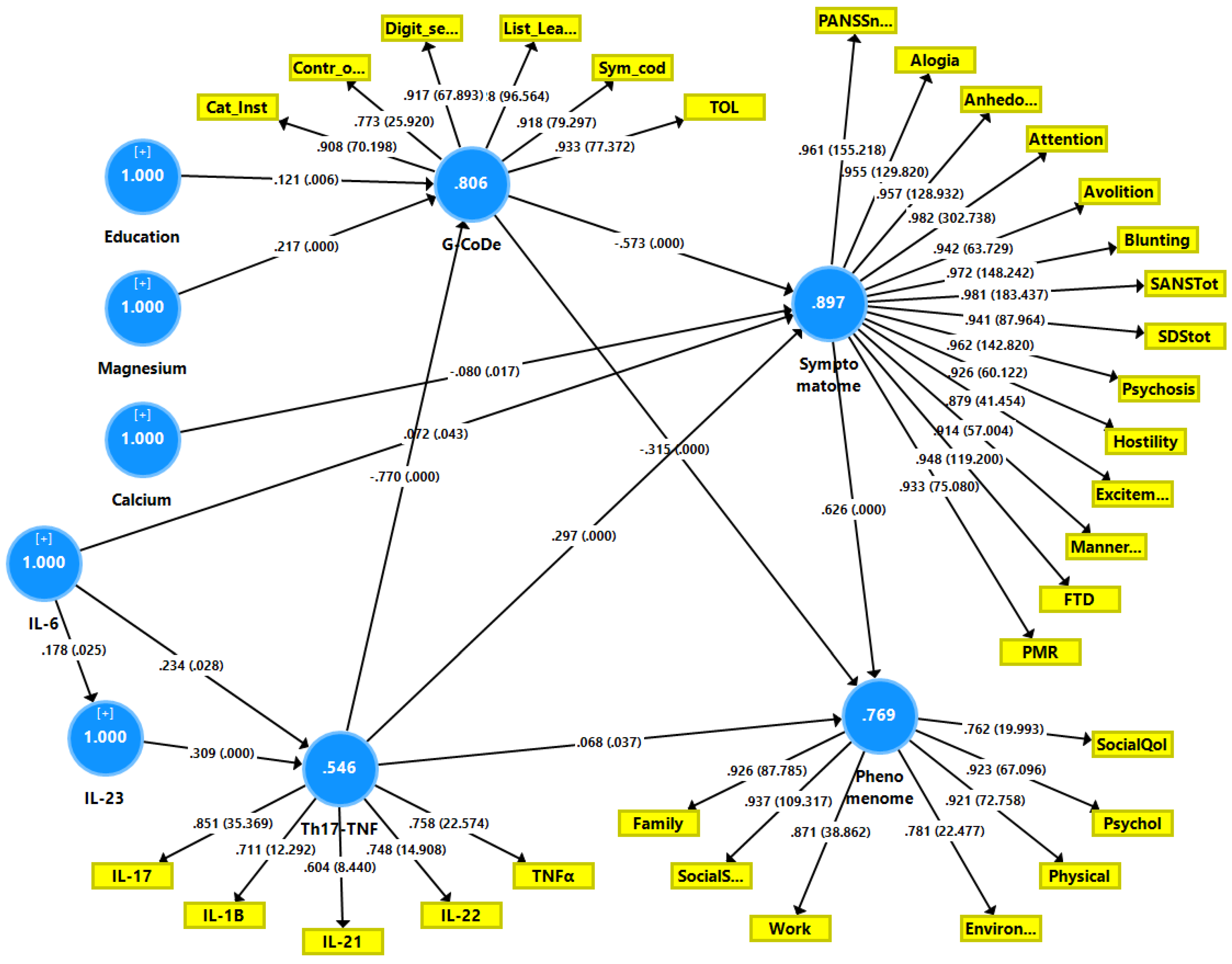
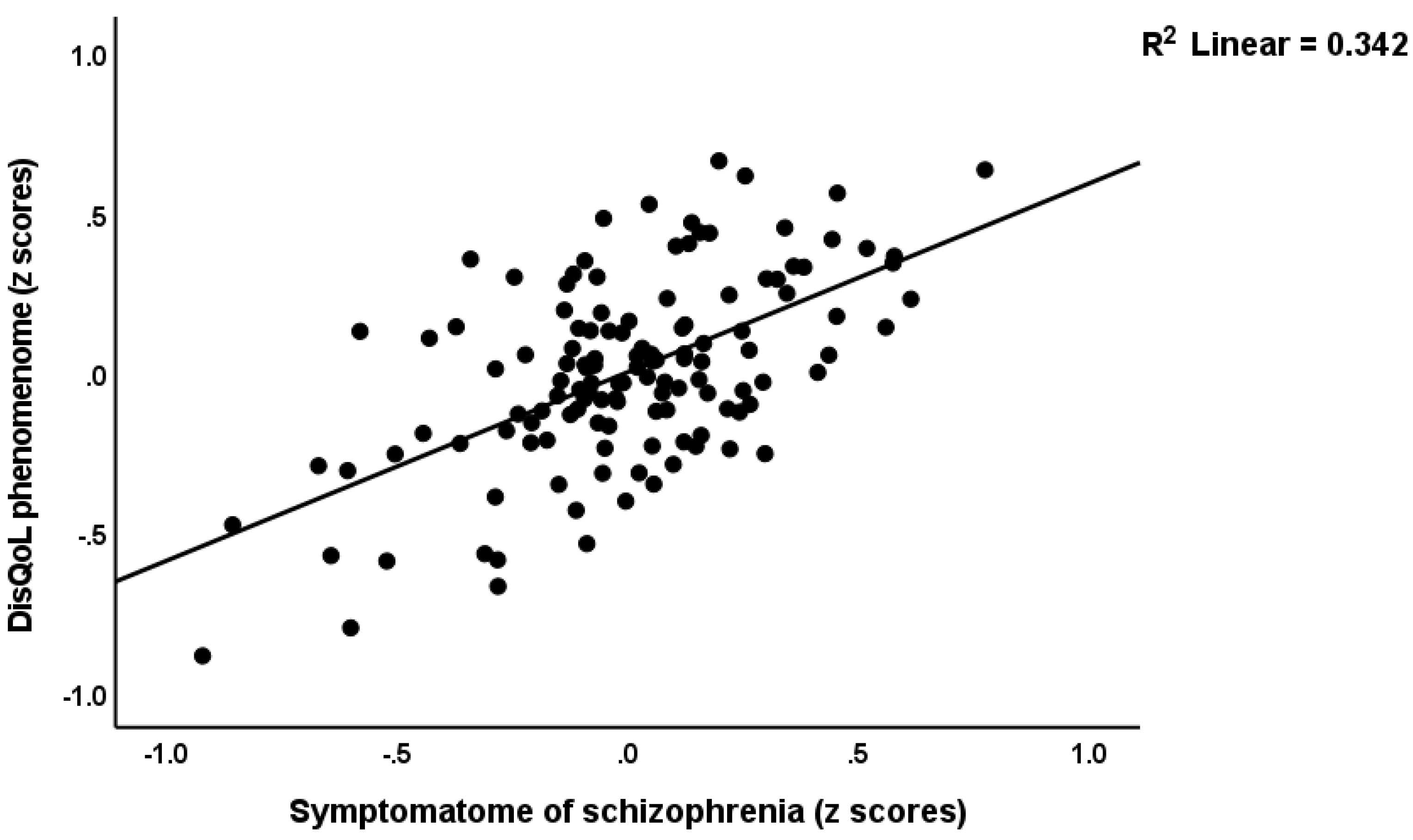
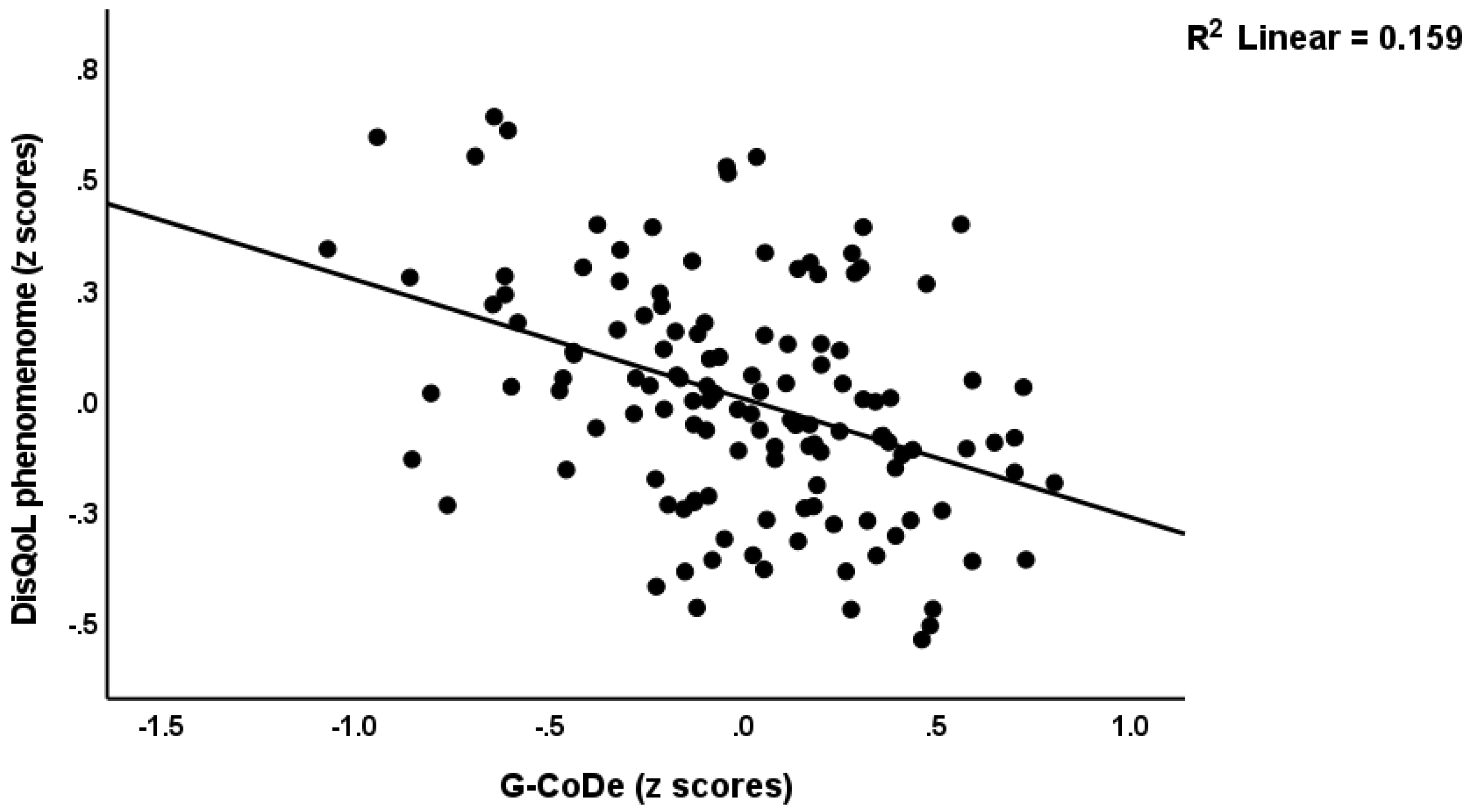
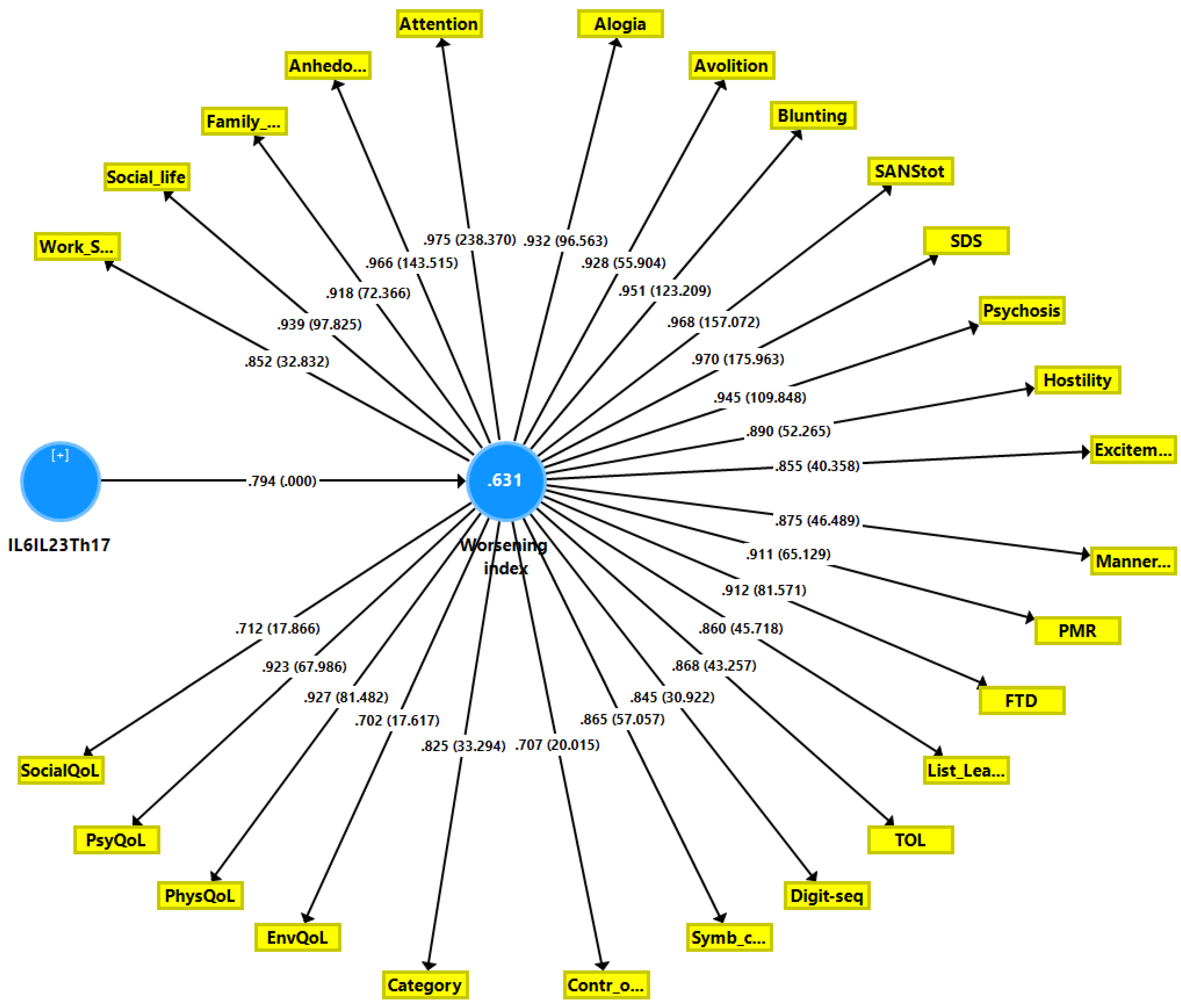
3.4. Results of PLS-SEM Path Modeling
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Schziophrenia. Available online: https://www.who.int/news-room/fact-sheets/detail/schizophrenia (accessed on 23 July 2022).
- Desalegn, D.; Girma, S.; Abdeta, T. Quality of life and its association with psychiatric symptoms and socio-demographic characteristics among people with schizophrenia: A hospital-based cross-sectional study. PLoS ONE 2020, 15, e0229514. [Google Scholar] [CrossRef]
- Kanchanatawan, B.; Sriswasdi, S.; Maes, M. Supervised machine learning to decipher the complex associations between neuro-immune biomarkers and quality of life in schizophrenia. Metab. Brain Dis. 2019, 34, 267–282. [Google Scholar] [CrossRef] [PubMed]
- Bobes, J.; Garcia-Portilla, M.P.; Bascaran, M.T.; Saiz, P.A.; Bousono, M. Quality of life in schizophrenic patients. Dialogues Clin. Neurosci. 2007, 9, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Galuppi, A.; Turola, M.C.; Nanni, M.G.; Mazzoni, P.; Grassi, L. Schizophrenia and quality of life: How important are symptoms and functioning? Int. J. Ment. Health Syst. 2010, 4, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ritsner, M.; Kurs, R.; Gibel, A.; Ratner, Y.; Endicott, J. Validity of an abbreviated quality of life enjoyment and satisfaction questionnaire (Q-LES-Q-18) for schizophrenia, schizoaffective, and mood disorder patients. Qual. Life Res. 2005, 14, 1693–1703. [Google Scholar] [CrossRef]
- Becker, T.; Leese, M.; Krumm, S.; Ruggeri, M.; Vázquez-Barquero, J.L. Needs and quality of life among patients with schizophrenia in five European centres. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, P.B.; Williams, C.L.; Corteling, N.; Filia, S.L.; Brewer, K.; Adams, A.; de Castella, A.R.; Rolfe, T.; Davey, P.; Kulkarni, J. Subject and observer-rated quality of life in schizophrenia. Acta Psychiatr. Scand. 2001, 103, 387–392. [Google Scholar] [CrossRef]
- Sim, K.; Mahendran, R.; Siris, S.G.; Heckers, S.; Chong, S.A. Subjective quality of life in first episode schizophrenia spectrum disorders with comorbid depression. Psychiatry Res. 2004, 129, 141–147. [Google Scholar] [CrossRef]
- Górna, K.; Jaracz, K.; Jaracz, J.; Kiejda, J.; Grabowska-Fudala, B.; Rybakowski, J. Social functioning and quality of life in schizophrenia patients--relationship with symptomatic remission and duration of illness. Psychiatr. Pol. 2014, 48, 277–288. [Google Scholar]
- Savill, M.; Orfanos, S.; Reininghaus, U.; Wykes, T.; Bentall, R.; Priebe, S. The relationship between experiential deficits of negative symptoms and subjective quality of life in schizophrenia. Schizophr. Res. 2016, 176, 387–391. [Google Scholar] [CrossRef]
- Maes, M.; Kanchanatawan, B. In (deficit) schizophrenia, a general cognitive decline partly mediates the effects of neuro-immune and neuro-oxidative toxicity on the symptomatome and quality of life. CNS Spectr. 2021, 27, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Sum, M.Y.; Tay, K.H.; Sengupta, S.; Sim, K. Neurocognitive functioning and quality of life in patients with and without deficit syndrome of schizophrenia. Psychiatry Res. 2018, 263, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Ueoka, Y.; Tomotake, M.; Tanaka, T.; Kaneda, Y.; Taniguchi, K.; Nakataki, M.; Numata, S.; Tayoshi, S.; Yamauchi, K.; Sumitani, S.; et al. Quality of life and cognitive dysfunction in people with schizophrenia. Prog. Neuropsychopharm. Biol. Psychiatry 2011, 35, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Alptekin, K.; Akvardar, Y.; Akdede, B.B.K.; Dumlu, K.; Işık, D.; Pirinçci, F.; Yahssin, S.; Kitiş, A. Is quality of life associated with cognitive impairment in schizophrenia? Prog. Neuropsychopharm. Biol. Psychiatry 2005, 29, 239–244. [Google Scholar] [CrossRef]
- Tolman, A.W.; Kurtz, M.M. Neurocognitive predictors of objective and subjective quality of life in individuals with schizophrenia: A meta-analytic investigation. Schizophr. Bull. 2012, 38, 304–315. [Google Scholar] [CrossRef]
- Mohamed, S.; Rosenheck, R.; Swartz, M.; Stroup, S.; Lieberman, J.A.; Keefe, R.S. Relationship of cognition and psychopathology to functional impairment in schizophrenia. Am. J. Psychiatry 2008, 165, 978–987. [Google Scholar] [CrossRef]
- Keefe, R.S.; Harvey, P.D. Cognitive impairment in schizophrenia. Handb. Exp. Pharm. 2012, 213, 11–37. [Google Scholar] [CrossRef]
- Maes, M.; Anderson, G. False Dogmas in Schizophrenia Research: Toward the Reification of Pathway Phenotypes and Pathway Classes. Front. Psychiatry 2021, 12, 663985. [Google Scholar] [CrossRef]
- Maes, M.; Vojdani, A.; Sirivichayakul, S.; Barbosa, D.S.; Kanchanatawan, B. Inflammatory and Oxidative Pathways Are New Drug Targets in Multiple Episode Schizophrenia and Leaky Gut, Klebsiella pneumoniae, and C1q Immune Complexes Are Additional Drug Targets in First Episode Schizophrenia. Mol. Neurobiol. 2021, 58, 3319–3334. [Google Scholar] [CrossRef]
- Roomruangwong, C.; Noto, C.; Kanchanatawan, B.; Anderson, G.; Kubera, M.; Carvalho, A.F.; Maes, M. The Role of Aberrations in the Immune-Inflammatory Response System (IRS) and the Compensatory Immune-Regulatory Reflex System (CIRS) in Different Phenotypes of Schizophrenia: The IRS-CIRS Theory of Schizophrenia. Mol. Neurobiol. 2020, 57, 778–797. [Google Scholar] [CrossRef]
- Maes, M.; Plaimas, K.; Suratanee, A.; Noto, C.; Kanchanatawan, B. First Episode Psychosis and Schizophrenia Are Systemic Neuro-Immune Disorders Triggered by a Biotic Stimulus in Individuals with Reduced Immune Regulation and Neuroprotection. Cells 2021, 10, 2929. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.S.; Maes, M. The macrophage-T-lymphocyte theory of schizophrenia: Additional evidence. Med. Hypotheses 1995, 45, 135–141. [Google Scholar] [CrossRef]
- Sirivichayakul, S.; Kanchanatawan, B.; Thika, S.; Carvalho, A.F.; Maes, M. A new schizophrenia model: Immune activation is associated with the induction of different neurotoxic products which together determine memory impairments and schizophrenia symptom dimensions. CNS Neurol. Disrd. Drug Targets 2019, 18, 124–140. [Google Scholar] [CrossRef] [PubMed]
- Al-Hakeim, H.K.; Alhusseini, A.F.; Al-Dujaili, A.; Debnath, M.; Maes, M. The interleukin-6/interleukin-23/Thelper-17-axis as a driver of neuro-immune toxicity in the major neurocognitive psychosis or deficit schizophrenia: A precision nomothetic psychiatry analysis. PLoS ONE 2022, 17, e0275839. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, B.; Buchanan, R.W.; McKenney, P.D.; Alphs, L.D.; Carpenter, W.T., Jr. The Schedule for the Deficit syndrome: An instrument for research in schizophrenia. Psychiatry Res. 1989, 30, 119–123. [Google Scholar] [CrossRef]
- WHOQoL-Group. Study protocol for the World Health Organization project to develop a Quality of Life assessment instrument (WHOQOL). Qual. Life Res. 1993, 2, 153–159. [Google Scholar] [CrossRef]
- Sheehan, K.H.; Sheehan, D.V. Assessing treatment effects in clinical trials with the discan metric of the Sheehan Disability Scale. Int. Clin. Psychopharm. 2008, 23, 70–83. [Google Scholar] [CrossRef]
- Andreasen, N.C. The Scale for the Assessment of Negative Symptoms (SANS): Conceptual and theoretical foundations. Br. J. Psychiat. 1989, 155, 49–52. [Google Scholar] [CrossRef]
- Overall, J.E.; Gorham, D.R. The brief psychiatric rating scale. Psychol. Rep. 1962, 10, 799–812. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Keefe, R.S.; Goldberg, T.E.; Harvey, P.D.; Gold, J.M.; Poe, M.P.; Coughenour, L. The Brief Assessment of Cognition in Schizophrenia: Reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr. Res. 2004, 68, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Ringle, C.; Da Silva, D.; Bido, D. Structural equation modeling with the SmartPLS. Brazil. J. Mark. 2015, 13, 56–73. [Google Scholar] [CrossRef]
- Norman, R.M.; Malla, A.K.; McLean, T.; Voruganti, L.P.; Cortese, L.; McIntosh, E.; Cheng, S.; Rickwood, A. The relationship of symptoms and level of functioning in schizophrenia to general wellbeing and the Quality of Life Scale. Acta Psychiatr. Scand. 2000, 102, 303–309. [Google Scholar] [CrossRef]
- Almulla, A.F.; Al-Hakeim, H.K.; Maes, M. Schizophrenia phenomenology revisited: Positive and negative symptoms are strongly related reflective manifestations of an underlying single trait indicating overall severity of schizophrenia. CNS Spectr. 2021, 26, 368–377. [Google Scholar] [CrossRef]
- Maes, M.; Vojdani, A.; Geffard, M.; Moreira, E.G.; Barbosa, D.S.; Michelin, A.P.; de Oliveira Semeão, L.; Sirivichayakul, S.; Kanchanatawan, B. Schizophrenia phenomenology comprises a bifactorial general severity and a single-group factor, which are differently associated with neurotoxic immune and immune-regulatory pathways. Biomol. Concepts 2019, 10, 209–225. [Google Scholar] [CrossRef]
- McGurk, S.R.; Mueser, K.T. Cognitive functioning and employment in severe mental illness. J. Nerv. Ment. Dis. 2003, 191, 789–798. [Google Scholar] [CrossRef]
- Orellana, G.; Slachevsky, A. Executive functioning in schizophrenia. Front. Psychiatry 2013, 4, 35. [Google Scholar] [CrossRef]
- Corlett, P.R.; Murray, G.K.; Honey, G.D.; Aitken, M.R.; Shanks, D.R.; Robbins, T.W.; Bullmore, E.T.; Dickinson, A.; Fletcher, P.C. Disrupted prediction-error signal in psychosis: Evidence for an associative account of delusions. Brain 2007, 130, 2387–2400. [Google Scholar] [CrossRef]
- Harvey, P.D.; Koren, D.; Reichenberg, A.; Bowie, C.R. Negative symptoms and cognitive deficits: What is the nature of their relationship? Schizophr. Bull. 2006, 32, 250–258. [Google Scholar] [CrossRef]
- Tamminga, C.A. The neurobiology of cognition in schizophrenia. J. Clin. Psychiatry 2006, 67, 9. [Google Scholar] [CrossRef]
- Brewer, W.J.; Francey, S.M.; Wood, S.J.; Jackson, H.J.; Pantelis, C.; Phillips, L.J.; Yung, A.R.; Anderson, V.A.; McGorry, P.D. Memory impairments identified in people at ultra-high risk for psychosis who later develop first-episode psychosis. Am. J. Psychiatry 2005, 162, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, K.; Addington, J.; Keefe, R.; Christensen, B.; Perkins, D.; Zipurksy, R.; Woods, S.; Miller, T.; Marquez, E.; Breier, A. Neuropsychological status of subjects at high risk for a first episode of psychosis. Schizophr. Res. 2004, 67, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Orellana, G.; Slachevsky, A.; Pena, M. Executive attention impairment in first-episode schizophrenia. BMC Psychiatry 2012, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Nitsch, L.; Zimmermann, J.; Krauthausen, M.; Hofer, M.J.; Saggu, R.; Petzold, G.C.; Heneka, M.T.; Getts, D.R.; Becker, A.; Campbell, I.L. CNS-specific synthesis of interleukin 23 induces a progressive cerebellar ataxia and the accumulation of both T and B cells in the brain: Characterization of a novel transgenic mouse model. Mol. Neurobiol. 2019, 56, 7977–7993. [Google Scholar] [CrossRef] [PubMed]
- Tahmasebinia, F.; Pourgholaminejad, A. The role of Th17 cells in auto-inflammatory neurological disorders. Prog. Neuropsychopharm. Biol. Psychiatry 2017, 79, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Langrish, C.L.; Chen, Y.; Blumenschein, W.M.; Mattson, J.; Basham, B.; Sedgwick, J.D.; McClanahan, T.; Kastelein, R.A.; Cua, D.J. IL-23 drives a pathogenic T cell population that induces autoimmune inflammation. J. Exp. Med. 2005, 201, 233–240. [Google Scholar] [CrossRef]
- Leavy, O. IL-21 stokes brain inflammation. Nat. Rev. Immunol. 2014, 14, 215. [Google Scholar] [CrossRef]
- Lee, D.; Jo, H.; Go, C.; Jang, Y.; Chu, N.; Bae, S.; Kang, D.; Kim, Y.; Kang, J.S. The Roles of IL-22 and Its Receptor in the Regulation of Inflammatory Responses in the Brain. Int. J. Mol. Sci. 2022, 23, 757. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.C.; Nickerson-Nutter, C.; Pittman, D.D.; Carrier, Y.; Goodwin, D.G.; Shields, K.M.; Lambert, A.J.; Schelling, S.H.; Medley, Q.G.; Ma, H.L.; et al. IL-22 induces an acute-phase response. J. Immunol. 2010, 185, 5531–5538. [Google Scholar] [CrossRef]
- Liu, Q.; Xin, W.; He, P.; Turner, D.; Yin, J.; Gan, Y.; Shi, F.D.; Wu, J. Interleukin-17 inhibits adult hippocampal neurogenesis. Sci. Rep. 2014, 4, 7554. [Google Scholar] [CrossRef]
- Bojarski, L.; Debowska, K.; Wojda, U. In vitro findings of alterations in intracellular calcium homeostasis in schizophrenia. Prog. Neuropsychopharm. Biol. Psychiatry 2010, 34, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, Y.; Li, X.; Ju, W.; Wu, G.; Yang, X.; Fu, X.; Gao, X. Association of Elements with Schizophrenia and Intervention of Selenium Supplements. Biol. Trace Elem. Res. 2018, 183, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.; Rapoport, A.; Mashiah, M.; Dolev, E. Serum and cerebrospinal levels of calcium and magnesium in acute versus remitted schizophrenic patients. Neuropsychobiology 1996, 33, 169–172. [Google Scholar] [CrossRef]
- Kirov, G.K.; Birch, N.J.; Steadman, P.; Ramsey, R.G. Plasma magnesium levels in a population of psychiatric patients: Correlations with symptoms. Neuropsychobiology 1994, 30, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Jamilian, H. Vitamin D, parathyroid hormone, serum calcium and phosphorus in patients with schizophrenia and major depression. Eur. Psychiatry 2011, 26, 1407. [Google Scholar] [CrossRef]
- Kirov, G.K.; Tsachev, K.N. Magnesium, schizophrenia and manic-depressive disease. Neuropsychobiology 1990, 23, 79–81. [Google Scholar] [CrossRef]
- Khan, A.; Tupling, D. A brief note on serum calcium levels in schizophrenics and controls. Can. J. Psychiatry 1990, 35, 74–76. [Google Scholar] [CrossRef]
- Mousa, R.F.; Smesam, H.N.; Qazmooz, H.A.; Al-Hakeim, H.K.; Maes, M. A pathway phenotype linking metabolic, immune, oxidative, and opioid pathways with comorbid depression, atherosclerosis, and unstable angina. CNS Spectr. 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Sowa-Kućma, M.; Szewczyk, B.; Sadlik, K.; Piekoszewski, W.; Trela, F.; Opoka, W.; Poleszak, E.; Pilc, A.; Nowak, G. Zinc, magnesium and NMDA receptor alterations in the hippocampus of suicide victims. J. Affect. Disord. 2013, 151, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Xin, W.-K.; Kwan, C.L.; Zhao, X.-H.; Xu, J.; Ellen, R.P.; McCulloch, C.A.; Yu, X.-M. A functional interaction of sodium and calcium in the regulation of NMDA receptor activity by remote NMDA receptors. J. Neurosci. 2005, 25, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Maes, M. Major neurocognitive psychosis: A novel schizophrenia endophenotype class that is based on machine learning and resembles Kraepelin’s and Bleuler’s conceptions. Acta Neuropsychiatr. 2022, 1–47. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Chen, D.; Xiu, M.; Li, S.; Zhang, X.Y. Serum BDNF levels, glycolipid metabolism in deficit schizophrenia: A case-control study. Asian J. Psychiatr. 2022, 69, 103003. [Google Scholar] [CrossRef]
- Mehterov, N.; Minchev, D.; Gevezova, M.; Sarafian, V.; Maes, M. Interactions Among Brain-Derived Neurotrophic Factor and Neuroimmune Pathways Are Key Components of the Major Psychiatric Disorders. Mol. Neurobiol. 2022, 59, 4926–4952. [Google Scholar] [CrossRef]
- Maes, M.; Scharpé, S.; De Meester, I.; Goossens, P.; Wauters, A.; Neels, H.; Verkerk, R.; De Meyer, F.; D’Hondt, P.; Peeters, D.; et al. Components of biological variation in prolyl endopeptidase and dipeptidyl-peptidase IV activity in plasma of healthy subjects. Clin. Chem. 1994, 40, 1686–1691. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Normal DisQoL A n = 42 | Moderate DISQoL B n = 52 | Severe DISQoL C n = 36 | F/χ2 | df | p |
|---|---|---|---|---|---|---|
| Age (years) | 36.1 ± 12.0 | 38.3 ± 12.6 | 36.9 ± 14.5 | 0.35 | 2/127 | 0.706 |
| Female/Male ratio | 21/21 | 21/31 | 15/21 | 0.97 | 2 | 0.628 |
| BMI (kg/m2) | 26.82 ± 3.49 | 27.07 ± 3.77 | 27.00 ± 4.09 | 0.05 | 2/127 | 0.950 |
| Education Year | 12.1 ± 3.2 B,C | 9.1 ± 3.7 A,C | 9.5 ± 3.3 A,B | 9.99 | 2/127 | <0.001 |
| Married/Single | 19/23 | 21/31 | 15/21 | 0.23 | 2 | 0.901 |
| Rural/Urban | 17/25 | 19/33 | 14/22 | 0.16 | 2 | 0.973 |
| TUD (No/Yes) | 26/16 | 27/25 | 24/12 | 2.10 | 2 | 0.375 |
| Employment (No/Yes) | 15/27 | 18/34 | 19/17 | 7.16 | 4 | 0.109 |
| Family history No/Yes | 41/1 | 34/18 | 17/19 | 25.02 | 2 | <0.001 |
| HC/NonDef SCZ/Def SCZ | 40/2/0 | 0/42/10 | 0/1/35 | 196.023 | 4 | <0.001 |
| Duration of Disease (years) | - | 8.4 ± 7.6 C | 13.0 ± 8.6 B | 7.01 | 1/86 | 0.010 |
| Age of onset (years) | - | 29.9 ± 9.9 C | 23.6 ± 11.9 B | 7.32 | 1/86 | 0.008 |
| Sheehan, Work-School | 1.26 ± 0.94 B,C | 5.42 ± 1.46 A,C | 7.00 ± 1.69 A,B | 184.07 | 2/127 | <0.001 |
| Sheehan, Social life | 1.00 ± 0.77 B,C | 4.54 ± 1.41 A,C | 7.92 ± 1.27 A,B | 325.45 | 2/127 | <0.001 |
| Sheehan, Family life | 1.24 ± 0.69 B,C | 4.35 ± 1.40 A,C | 7.39 ± 1.15 A,B | 281.49 | 2/127 | <0.001 |
| WHO-QoL, physical | 29.1 ± 3.3 B,C | 20.6 ± 3.3 A,C | 14.8 ± 3.4 A,B | 186.68 | 2/127 | <0.001 |
| WHO-QoL, psychological | 24.2 ± 3.0 B,C | 17.3 ± 2.2 A,C | 13.2 ± 3.3 A,B | 159.24 | 2/127 | <0.001 |
| WHO-QoL, social | 10.9 ± 1.8 B,C | 8.1 ± 1.9 A,C | 6.9 ± 2.0 A,B | 45.36 | 2/127 | <0.001 |
| WHO-QoL, environment | 30.5 ± 3.3 B,C | 24.9 ± 3.2 A,C | 22.9 ± 3.9 A,B | 52.60 | 2/127 | <0.001 |
| Benzodiazepines No/Yes | 42/0 | 43/9 | 26/10 | 1.37 * | 1 | 0.296 |
| Mood stabilizers No/Yes | 42/0 | 32/20 | 17/19 | 1.77 * | 1 | 0.199 |
| Olanzapine No/Yes | 41/1 | 11/41 | 16/20 | 5.43 * | 1 | 0.020 |
| Clozapine No/Yes | 42/0 | 48/4 | 28/8 | 3.81 * | 1 | 0.051 |
| Fluphenazine No/Yes | 42/0 | 37/15 | 24/12 | 0.20 * | 1 | 0.814 |
| Haloperidol No/Yes | 42/0 | 50/2 | 31/5 | FEPT * | - | 0.117 |
| Quetiapine No/Yes | 42/0 | 49/3 | 34/2 | FEPT * | - | 1.0 |
| Risperidone No/Yes | 42/0 | 45/7 | 27/9 | 1.90 * | 1 | 0.260 |
| Fluoxetine No/Yes | 42/0 | 50/2 | 35/1 | FEPT * | - | 1.0 |
| Variables | Normal DisQoL A n = 42 | Moderate DISQoL B n = 52 | Severe DISQoL C n = 36 |
|---|---|---|---|
| Psychosis (z scores) | −1.092 (0.149) | 0.048 (0.614) | 1.205 (0.425) |
| Hostility (z scores) | −0.960 (0.151) | 0.150 (0.707) | 1.110 (0.705) |
| Excitement (z scores) | −1.005 (0.322) | 0.101 (0.687) | 1.023 (0.752) |
| Mannerism (z scores) | −0.959 (0.160) | −0.041 (0.655) | 1.179 (0.702) |
| PMR (z scores) | −1.049 (0.124) | 0.022 (0.609) | 1.192 (0.583) |
| FTD (z scores) | −1.000 (0.255) | −0.033 (0.620) | 1.222 (0.570) |
| PANSS negative | 10.3 (3.3) | 22.3 (6.5) | 34.8 (6.1) |
| SANS blunting | 2.7 (2.8) | 15.9 (4.4) | 29.5 (7.7) |
| SANS alogia | 1.0 (0.3) | 6.9 (2.4) | 14.7 (3.6) |
| SANS avolition | 3.3 (1.7) | 9.5 (2.5) | 16.4 (3.5) |
| SANS anhedonia | 2.1 (1.6) | 11.8 (2.4) | 19.2 (3.2) |
| SANS attention | 0.6 (1.3) | 6.9 (1.9) | 11.9 (2.3) |
| Total SANS | 9.6 (7.1) | 51 (11.6) | 91.9 (18.9) |
| Total SDS | 1.4 (3.3) | 17.8 (4.4) | 28.6 (3.3) |
| BACS List learning | 50.5 (8.4) | 21.0 (8.1) | 16.8 (6.8) |
| BACS Digit sequencing | 26.9 (2.7) | 10.1 (6.7) | 7.2 (5.9) |
| BACS Category Instances | 16.5 (3.0) | 7.2 (2.6) | 5.5 (2.6) |
| BACS Controlled oral word | 8.5 (2.8) | 4.9 (2.6) | 2.6 (1.9) |
| BACS Symbol coding | 46.6 (13.7) | 15.6 (7.2) | 6.2 (2.5) |
| BACS Tower of London | 18.1 (2.7) | 6.7 (3.5) | 4.1 (0.7) |
| Biomarkers | Normal DisQol A | Moderate DisQoL B | Severe DisQol C | F (df = 2/122) | p |
|---|---|---|---|---|---|
| Total magnesium (mM) | 1.008 (0.021) C | 0.989 (0.019) C | 0.899 (0.022) A,B | 6.97 | 0.001 |
| Total calcium (mM) | 2.383 (0.042) C | 2.348 (0.037) C | 2.216 (0.045) A,B | 4.27 | 0.016 |
| IL-1β (pg/mL) | 2.46 (0.149) B,C | 3.50 (0.131) A | 3.80 (0.158) A | 21.27 | <0.001 |
| IL-6 (pg/mL) | 5.92 (0.57) C | 6.26 (0.50) C | 8.35 (0.60) A,B | 5.33 | 0.006 |
| IL-23 (pg/mL) | 14.73 (2.48) B,C | 24.63 (2.17) A | 27.02 (2.62) A | 6.61 | 0.002 |
| IL-22 (pg/mL) | 17.94 (1.19) B,C | 28.06 (1.04) A | 29.31 (1.26) A | 26.62 | <0.001 |
| IL-21 (pg/mL) | 159.88 (14.66) B,C | 232.93 (12.85) A,C | 279.40 (15.51) A,B | 15.90 | <0.001 |
| TNF-α (pg/mL) | 19.99 (2.14) B,C | 43.75 (1.88) A | 45.84 (2.26) A | 43.61 | <0.001 |
| IL-17 (pg/mL) | 17.56 (1.71) B,C | 43.28 (1.50) A,C | 47.87 (1.81) A,B | 87.67 | <0.001 |
| IL-10 (pg/mL) | 7.43 (0.63) B, C | 12.22 (0.55) A | 11.47 (0.66) A | 16.87 | <0.001 |
| Th17 pathogenic (z scores) | −0.860 (0.127) B,C | 0.215 (0.111) A,C | 0.692 (0.132) A,B | 36.47 | <0.001 |
| IL23IL16Th17 axis (z scores) | −0.973 (0.116) B,C | 0.271 (0.102) A,C | 0.744 (0.120) A,B | 54.37 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Musawi, A.F.; Al-Hakeim, H.K.; Al-Khfaji, Z.A.; Al-Haboby, I.H.; Almulla, A.F.; Stoyanov, D.S.; Maes, M. In Schizophrenia, the Effects of the IL-6/IL-23/Th17 Axis on Health-Related Quality of Life and Disabilities Are Partly Mediated by Generalized Cognitive Decline and the Symptomatome. Int. J. Environ. Res. Public Health 2022, 19, 15281. https://doi.org/10.3390/ijerph192215281
Al-Musawi AF, Al-Hakeim HK, Al-Khfaji ZA, Al-Haboby IH, Almulla AF, Stoyanov DS, Maes M. In Schizophrenia, the Effects of the IL-6/IL-23/Th17 Axis on Health-Related Quality of Life and Disabilities Are Partly Mediated by Generalized Cognitive Decline and the Symptomatome. International Journal of Environmental Research and Public Health. 2022; 19(22):15281. https://doi.org/10.3390/ijerph192215281
Chicago/Turabian StyleAl-Musawi, Ali Fattah, Hussein Kadhem Al-Hakeim, Zahraa Abdulrazaq Al-Khfaji, Inas H. Al-Haboby, Abbas F. Almulla, Drozdstoj St. Stoyanov, and Michael Maes. 2022. "In Schizophrenia, the Effects of the IL-6/IL-23/Th17 Axis on Health-Related Quality of Life and Disabilities Are Partly Mediated by Generalized Cognitive Decline and the Symptomatome" International Journal of Environmental Research and Public Health 19, no. 22: 15281. https://doi.org/10.3390/ijerph192215281
APA StyleAl-Musawi, A. F., Al-Hakeim, H. K., Al-Khfaji, Z. A., Al-Haboby, I. H., Almulla, A. F., Stoyanov, D. S., & Maes, M. (2022). In Schizophrenia, the Effects of the IL-6/IL-23/Th17 Axis on Health-Related Quality of Life and Disabilities Are Partly Mediated by Generalized Cognitive Decline and the Symptomatome. International Journal of Environmental Research and Public Health, 19(22), 15281. https://doi.org/10.3390/ijerph192215281