
Stigma Experienced by Rural Pregnant Women with Substance Use Disorder: A Scoping Review and Qualitative Synthesis

Abstract
1. Introduction
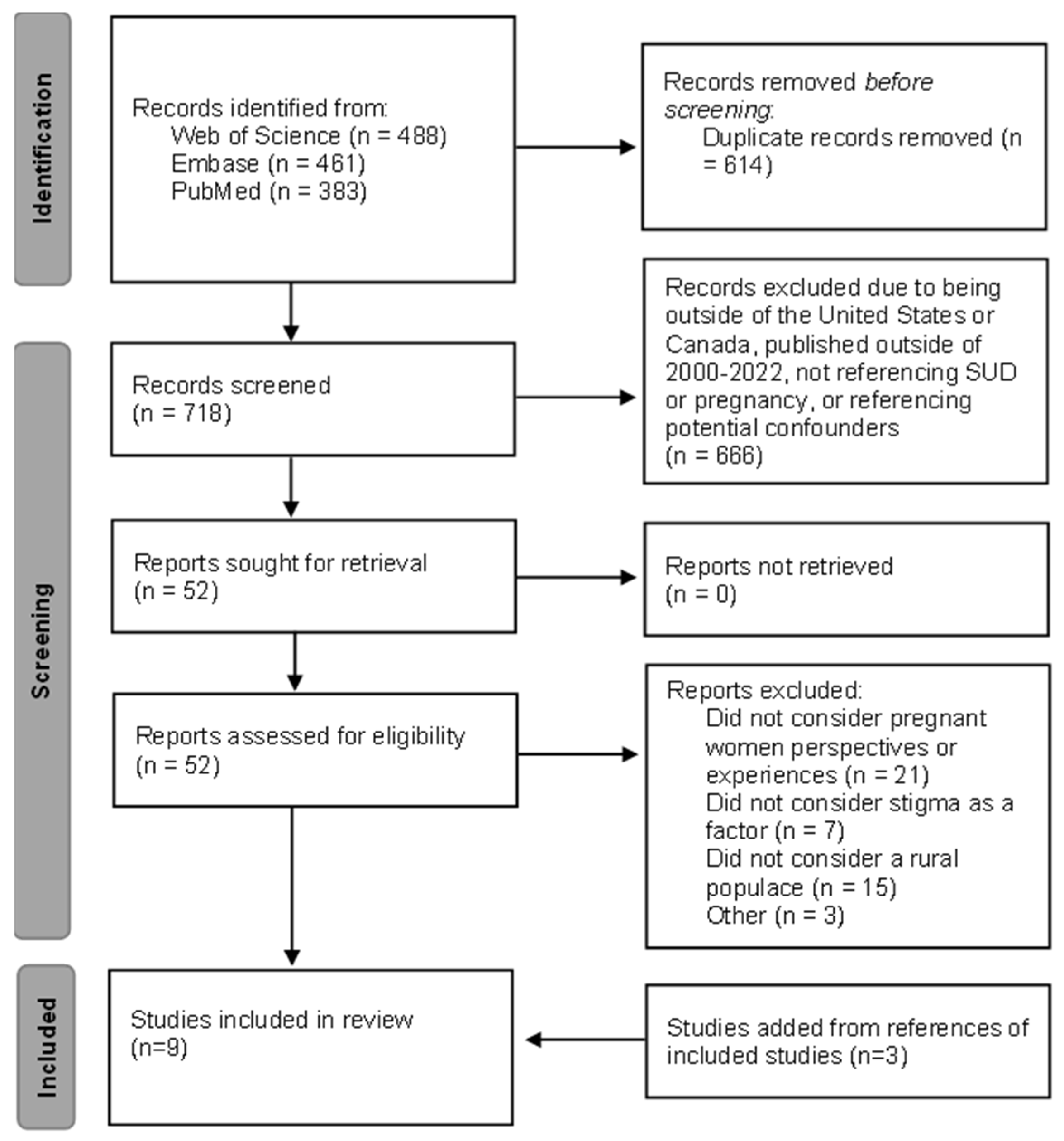
2. Materials and Methods
2.1. Study Design
2.2. Study Selection
2.3. Criteria for Inclusion
2.4. Data Extraction
3. Results

{kind=link}
| First Author (Publication Year) | Study Aim | Study Setting | Participants | Data Collection | Analysis |
|---|---|---|---|---|---|
| Blaire [8] | Characterize experiences of perinatal persons with SUD | University of Kentucky, NICU | 11 postpartum women (≥18 y.o.), with perinatal OUD and children requiring NAS observation/treatment | Semi-structured interviews | Sandelowaski’s qualitative description method |
| Burgess [9] | Learn about stigma affected seeking and maintaining treatment for opioid use disorder | MaineGeneral Health | 2 groups of postpartum women who sought treatment while pregnant (≥18 y.o.), 8 groups of non-postpartum men and women (≥18 y.o.) | Standardized interviews, recorded focus groups | Summative content analysis, conventional content analysis |
| Jackson [10] | Examine how barriers in seeking substance use treatment differ between urban and rural pregnant women | University of Kentucky Medical Center | Pregnant women (≥18 y.o.) undergoing inpatient detoxification | Face-to-face interviews, medical record review | Thematic analysis of interviews, quantitative analysis of socio-demographic variables |
| Jackson [4] | Examine barriers to entering substance use treatment experienced by rural, pregnant women | University of Kentucky Chandler Medical Center | Pregnant women (≥18 y.o.) undergoing inpatient detoxification | Face-to-face interviews, medical record review | Thematic analysis of interviews, quantitative analysis of socio-demographic variables |
| Jessup [11] | Examine extrinsic barriers to substance abuse treatment for “pregnant drug-dependent women” | Northern California | Perinatal women (24 weeks pregnant-1 year postpartum, (≥18 y.o.) undergoing residential treatment | Semi-structured interviews | Qualitative life history analysis |
| Kramlich [12] | Explore the perception of rural women with SUD during their pregnancy and infants’ hospitalization; explore how the perceptions impacted their ability to bond with their baby | Northeast United State | Perinatal women (pregnant or recently birth, (≥18 y.o.) identified as having opioid use disorder | Semi-structured interviews | Framework analysis and thematic analysis |
| Ostrach [13] | Explore ambivalence about medication-assisted treatment for OUD in the context of societal stigma | Central Appalachia | Pregnant women receiving medication-assisted treatment and prenatal care at an OB/GYN office | Observation and semi-structured interviews | Thematic analysis |
| Paterno [14] | Describe experiences of addiction in pregnancy, recovery, and a mentor/peer support role | Massachusetts | Peer mentors with a history of substance use during pregnancy | Digital storytelling workshop and semi-structured interviews | Analysis using intertextual transcripts and thematic analysis (ground theory approach) |
| Roberts [15] | Explore how drug use and factors associated with drug use became barriers to care | Northern California | Perinatal women (pregnant-2 years postpartum, (≥18 y.o.) undergoing residential treatment | Semi-structured interviews and focus groups | Thematic analysis |
3.1. Stigma within the Community
3.2. Stigma within Healthcare Settings
3.3. Importance of Comprehensive Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Health and Human Services; Substance Abuse and Mental Health Services Administration; Center for Behavioral Health Statistics and Quality. 2019 National Survey on Drug Use and Health: Women. Maryland (US): Substance Abuse and Mental Health Services. 2020. Available online: https://www.samhsa.gov/data/report/2019-nsduh-women (accessed on 15 August 2021).
- Gabrielson, S.M.B.; Carwile, J.L.; O’Connor, A.B.; Ahrens, K.A. Maternal opioid use disorder at delivery hospitalization in a rural state: Maine, 2009–2018. Public Health 2020, 181, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Racine, E.; Bell, E.; Zizzo, N.; Green, C. Public Discourse on the Biology of Alcohol Addiction: Implications for Stigma, Self-Control, Essentialism, and Coercive Policies in Pregnancy. Neuroethics 2015, 8, 177–186. [Google Scholar] [CrossRef]
- Jackson, A.; Shannon, L. Barriers to Receiving Substance Abuse Treatment Among Rural Pregnant Women in Kentucky. Matern. Child Health J. 2012, 16, 1762–1770. [Google Scholar] [CrossRef] [PubMed]
- Chipp, C.; Dewane, S.; Brems, C.; Johnson, M.E.; Warner, T.D.; Roberts, L.W. “If Only Someone Had Told Me…”: Lessons from Rural Providers. J. Rural Health 2011, 27, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Seers, K. What is a qualitative synthesis? Evid. Based Nurs. 2012, 15, 101. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Blair, L.; Ashford, K.; Gentry, L.; Bell, S.; Fallin-Bennett, A. Care Experiences of Persons with Perinatal Opioid Use a Qualitative Study. J. Perinat. Neonatal Nurs. 2021, 35, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Burgess, A.; Bauer, E.; Gallagher, S.; Karstens, B.; Lavoie, L.; Ahrens, K.; O’Connor, A. Experiences of stigma among individuals in recovery from opioid use disorder in a rural setting: A qualitative analysis. J. Subst. Abus. Treat. 2021, 130, 108488. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.; Shannon, L. Examining barriers to and motivations for substance abuse treatment among pregnant women: Does urban-rural residence matter? Women Health 2012, 52, 570–586. [Google Scholar] [CrossRef] [PubMed]
- Jessup, M.A.; Humphreys, J.C.; Brindis, C.D.; Lee, K.A. Extrinsic Barriers to Substance Abuse Treatment among Pregnant Drug Dependent Women. J. Drug Issues 2003, 33, 285–304. [Google Scholar] [CrossRef]
- Kramlich, D.; Kronk, R.; Marcellus, L.; Colbert, A.; Jakub, K. Rural Postpartum Women with Substance Use Disorders. Qual. Health Res. 2018, 28, 1449–1461. [Google Scholar] [CrossRef] [PubMed]
- Ostrach, B.; Leiner, C. “I didn’t want to be on Suboxone at first…”—Ambivalence in Perinatal Substance Use Treatment. J. Addict. Med. 2019, 13, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Paterno, M.T.; Low, M.; Gubrium, A.; Sanger, K. Mothers and Mentors: Exploring Perinatal Addiction and Recovery through Digital Storytelling. Qual. Health Res. 2019, 29, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.C.M.; Pies, C. Complex Calculations: How Drug Use during Pregnancy Becomes a Barrier to Prenatal Care. Matern. Child Health J. 2011, 15, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Logan, T.K.; Walker, R.; Nagle, L.; Lewis, J.; Wiesenhahn, D. Rural and small-town attitudes about alcohol use during pregnancy: A community and provider sample. J. Rural Health 2003, 19, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Oni, H.T.; Drake, J.A.; Dietze, P.; Higgs, P.; Islam, M.M. Barriers to women’s disclosure of and treatment for substance use during pregnancy: A qualitative study. Women Birth 2021, 35, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.M.; Nye, E.; West, K. Substance Use Disorder Treatment, Perceived Need for Treatment, and Barriers to Treatment Among Parenting Women With Substance Use Disorder in US Rural Counties. J. Rural Health 2022, 38, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Chandler, A.; Whittaker, A.; Cunningham-Burley, S.; Williams, N.; McGorm, K.; Mathews, G. Substance, structure and stigma: Parents in the UK accounting for opioid substitution therapy during the antenatal and postnatal periods. Int. J. Drug Policy 2013, 24, e35–e42. [Google Scholar] [CrossRef] [PubMed][Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bright, V.; Riddle, J.; Kerver, J. Stigma Experienced by Rural Pregnant Women with Substance Use Disorder: A Scoping Review and Qualitative Synthesis. Int. J. Environ. Res. Public Health 2022, 19, 15065. https://doi.org/10.3390/ijerph192215065
Bright V, Riddle J, Kerver J. Stigma Experienced by Rural Pregnant Women with Substance Use Disorder: A Scoping Review and Qualitative Synthesis. International Journal of Environmental Research and Public Health. 2022; 19(22):15065. https://doi.org/10.3390/ijerph192215065
Chicago/Turabian StyleBright, Victoria, Julia Riddle, and Jean Kerver. 2022. "Stigma Experienced by Rural Pregnant Women with Substance Use Disorder: A Scoping Review and Qualitative Synthesis" International Journal of Environmental Research and Public Health 19, no. 22: 15065. https://doi.org/10.3390/ijerph192215065
APA StyleBright, V., Riddle, J., & Kerver, J. (2022). Stigma Experienced by Rural Pregnant Women with Substance Use Disorder: A Scoping Review and Qualitative Synthesis. International Journal of Environmental Research and Public Health, 19(22), 15065. https://doi.org/10.3390/ijerph192215065