
Evaluation of Salivary Biomarkers of Periodontal Disease Based on Smoking Status: A Systematic Review
 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
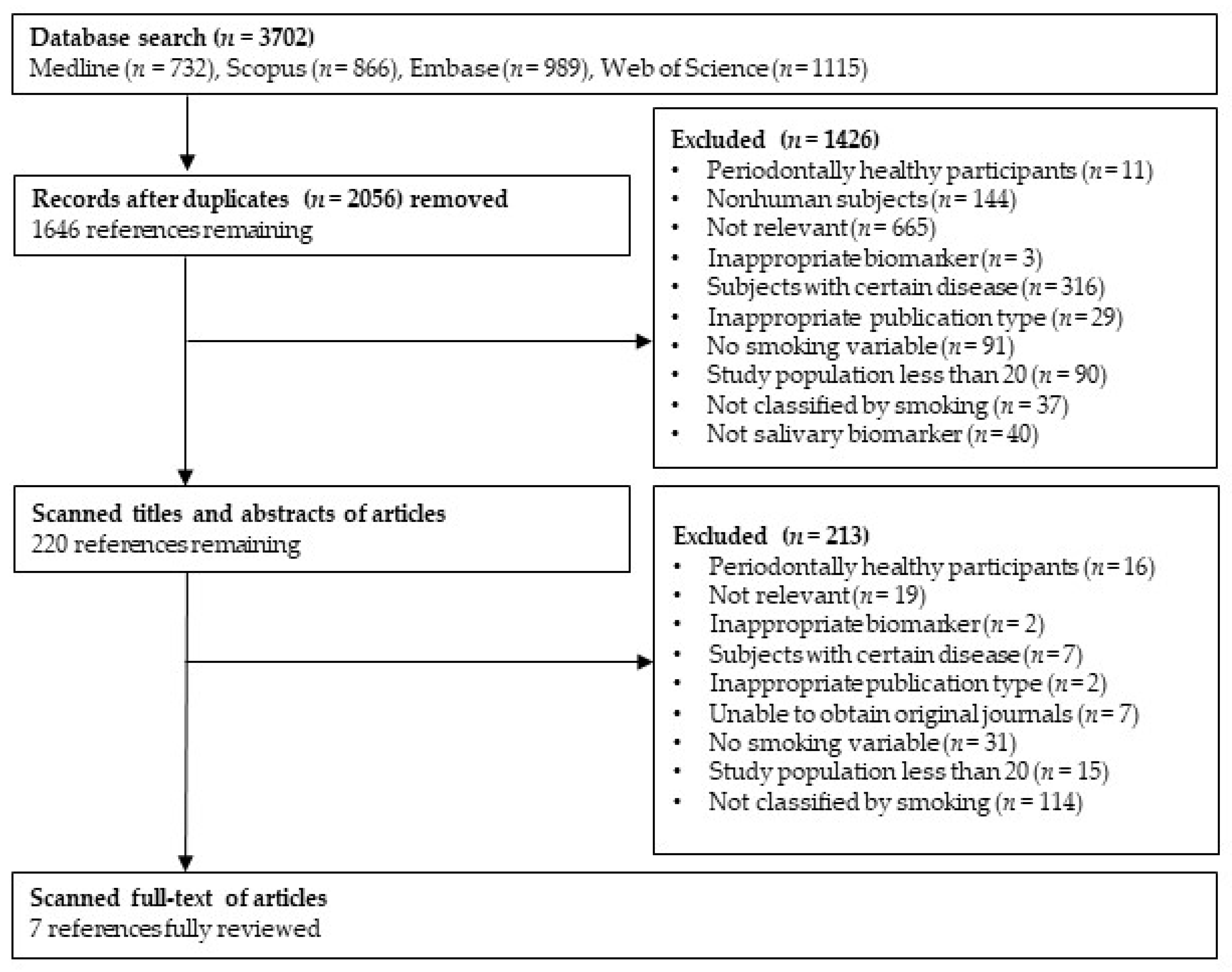
2.2. Literature Search and Selection
2.3. Study Selection and Exclusion Criteria
3. Results
3.1. Risk of Bias Assessment
3.2. Descriptive Summary of the Studies Included in the Systematic Review
3.3. Salivary Biomarker Levels Based on Smoking Status
4. Discussion
4.1. Evidence for Salivary Biomarkers Based on Smoking Status
4.2. Significance and Limitations of This Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, Y.; Zhou, X.; Cheng, L.; Li, M. The impact of smoking on subgingival microflora: From periodontal health to disease. Front. Microbiol. 2020, 11, 66. [Google Scholar] [CrossRef]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers. 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Amerio, E.; Farina, R.; Nart, J.; Ramanauskaite, A.; Renvert, S.; Roccuzzo, A.; Salvi, G.E.; Schwarz, F.; Trombelli, L.; et al. Significance of probing for monitoring peri-implant diseases. Int. J. Oral Implantol. 2021, 14, 385–399. [Google Scholar]
- Srivastava, N.; Nayak, P.A.; Rana, S. Point of care: A novel approach to periodontal diagnosis—A review. J. Clin. Diagn. Res. 2017, 11, ZE01–ZE06. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.A.; Telgi, R.L.; Tirth, A.; Tantry, I.Q.; Aleem, A. Lactate dehydrogenase and β-glucuronidase as salivary biochemical markers of periodontitis among smokers and non-smokers. Sultan Qaboos Univ. Med. J. 2018, 18, e318–e323. [Google Scholar] [CrossRef] [PubMed]
- Naresh, C.K.; Rao, S.M.; Shetty, P.R.; Ranganath, V.; Patil, A.S.; Anu, A.J. Salivary antioxidant enzymes and lipid peroxidation product malondialdehyde and sialic acid levels among smokers and nonsmokers with chronic periodontitis—A clinico-biochemical study. J. Fam. Med. Prim. Care. 2019, 8, 2960–2964. [Google Scholar] [CrossRef]
- Bawankar, P.V.; Kolte, A.P.; Kolte, R.A. Evaluation of stress, serum and salivary cortisol, and interleukin-1β levels in smokers and non-smokers with chronic periodontitis. J. Periodontol. 2018, 89, 1061–1068. [Google Scholar] [CrossRef]
- Hendek, M.K.; Erdemir, E.O.; Kisa, U.; Ozcan, G. Effect of initial periodontal therapy on oxidative stress markers in gingival crevicular fluid, saliva, and serum in smokers and non-smokers with chronic periodontitis. J. Periodontol. 2015, 86, 273–282. [Google Scholar] [CrossRef]
- Nazaryan, R.; Kryvenko, L. Salivary oxidative analysis and periodontal status in children with atopy. Interv. Med. Appl. Sci. 2017, 9, 199–203. [Google Scholar] [CrossRef]
- Chafik, A.; Essamadi, A.; Çelik, S.Y.; Solak, K.; Mavi, A. Characterization of an interesting selenium-dependent glutathione peroxidase (Se-GPx) protecting cells against environmental stress: The Camelus dromedarius erythrocytes Se-GPx. Biocatal. Agric. Biotechnol. 2019, 18, 101000. [Google Scholar] [CrossRef]
- Sardarian, A.; Andisheh Tadbir, A.; Zal, F.; Amini, F.; Jafarian, A.; Khademi, F.; Mostafavi-Pour, Z. Altered oxidativestatus and integrin expression incyclosporine A-treated oral epithelialcells. Toxicol. Mech. Methods. 2015, 25, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Kou, L.; Jiang, X.; Lin, X.; Huang, H.; Wang, J.; Yao, Q.; Chen, R. Matrix metalloproteinase inspired therapeutic strategies for bone diseases. Curr. Pharm. Biotechnol. 2021, 22, 451–467. [Google Scholar] [CrossRef] [PubMed]
- Lähteenmäki, H.; Tervahartiala, T.; Räisänen, I.T.; Pärnänen, P.; Mauramo, M.; Gupta, S.; Sampson, V.; Rathnayake, N.; Heikkinen, A.M.; Alassiri, S.; et al. Active MMP-8 point-of-care (PoC)/chairside enzyme-test as an adjunctive tool for early and real? time diagnosis of peri? implantitis. Clin. Exp. Dent. Res. 2022, 8, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Gieselmann, D.R.; Heikkinen, A.M.; Tervahartiala, T.; Sorsa, T. Salivary diagnostics—Point-of-care diagnostics of MMP-8 in dentistry and medicine. Diagnostics 2017, 7, 7. [Google Scholar] [CrossRef]
- Herrera, D.; Retamal-Valdes, B.; Alonso, B.; Feres, M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S78–S94. [Google Scholar] [CrossRef]
- Eke, P.I.; Borgnakke, W.S.; Genco, R.J. Recent epidemiologic trends in periodontitis in the USA. Periodontology 2000 2020, 82, 257–267. [Google Scholar] [CrossRef]
- Smith, M.M.; Knight, E.T.; Al-Harthi, L.; Leichter, J.W. Chronic periodontitis and implant dentistry. Periodontology 2000 2017, 74, 63–73. [Google Scholar] [CrossRef]
- Souto, M.L.S.; Rovai, E.S.; Villar, C.C.; Braga, M.M.; Pannuti, C.M. Effect of smoking cessation on tooth loss: A systematic review with meta-analysis. BMC Oral Health 2019, 19, 245. [Google Scholar] [CrossRef]
- Ramseier, C.A.; Anerud, A.; Dulac, M.; Lulic, M.; Cullinan, M.P.; Seymour, G.J.; Faddy, M.J.; Bürgin, W.; Schätzle, M.; Lang, N.P. Natural history of periodontitis: Disease progression and tooth loss over 40 years. J. Clin. Periodontol. 2017, 44, 1182–1191. [Google Scholar] [CrossRef]
- Arrejaie, A.S.; Al-Aali, K.A.; Alrabiah, M.; Vohra, F.; Mokeem, S.A.; Basunbul, G.; Alrahlah, A.; Abduljabbar, T. Proinflammatory cytokine levels and peri-implant parameters among cigarette smokers, individuals vaping electronic cigarettes, and non-smokers. J. Periodontol. 2019, 90, 367–374. [Google Scholar] [CrossRef]
- Alqahtani, F.; Alqahtani, M.; Shafqat, S.S.; Akram, Z.; Al-Kheraif, A.A.; Javed, F. Efficacy of mechanical debridement with adjunctive probiotic therapy in the treatment of peri-implant mucositis in cigarette-smokers and never-smokers. Clin. Implant Dent. Relat. Res. 2019, 21, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.; Ramesh, V.; Locasale, J.W. The evolving metabolic landscape of chromatin biology and epigenetics. Nat. Rev. Genet. 2020, 21, 737–753. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Jain, D.; Jain, S.; Jaiswal, S.; Goyal, R.K. Evaluation of salivary alkaline phosphatase levels in tobacco users to determine its role as a biomarker in oral potentially malignant disorders. Int. J. Health Sci. Res. 2022, 6, 12443–12449. [Google Scholar] [CrossRef]
- Ornelas-González, A.; Ortiz-Martínez, M.; González-González, M.; Rito-Palomares, M. Enzymatic methods for salivary biomarkers detection: Overview and current challenges. Molecules 2021, 26, 7026. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Kim, S.J.; Hong, S.; Kim, Y. Diagnosis of Alzheimer’s disease utilizing amyloid and tau as fluid biomarkers. Exp. Mol. Med. 2019, 51, 1–10. [Google Scholar] [CrossRef]
- Bostanci, N.; Mitsakakis, K.; Afacan, B.; Bao, K.; Johannsen, B.; Baumgartner, D.; Müller, L.; Kotolová, H.; Emingil, G.; Karpíšek, M. Validation and verification of predictive salivary biomarkers for oral health. Sci. Rep. 2021, 11, 6406. [Google Scholar] [CrossRef]
- Hall, M.W.; Singh, N.; Ng, K.F.; Lam, D.K.; Goldberg, M.B.; Tenenbaum, H.C.; Neufeld, J.D.; Beiko, G.R.; Senadheera, D.B. Interpersonal diversity and temporal dynamics of dental, tongue, and salivary microbiota in the healthy oral cavity. NPJ Biofilms Microbiomes 2017, 3, 1–7. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; PRISMA-DTA Group. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 89. [Google Scholar] [CrossRef]
- Riva, J.J.; Malik, K.M.; Burnie, S.J.; Endicott, A.R.; Busse, J.W. What is your research question? An introduction to the PICOT format for clinicians. J. Can. Chiropr. Assoc. 2012, 56, 167–171. [Google Scholar]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S219–S229. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Periodontol. 2018, 89 (Suppl. S1), S313–S318. [Google Scholar] [CrossRef] [PubMed]
- Arias-Bujanda, N.; Regueira-Iglesias, A.; Blanco-Pintos, T.; Alonso-Sampedro, M.; Relvas, M.; González-Peteiro, M.M.; Balsa-Castro, C.; Tomás, I. Diagnostic accuracy of IL1β in saliva: The development of predictive models for estimating the probability of the occurrence of periodontitis in non-smokers and smokers. J. Clin. Periodontol. 2020, 47, 702–714. [Google Scholar] [CrossRef]
- Chang, C.H.; Han, M.L.; Teng, N.C.; Lee, C.Y.; Huang, W.T.; Lin, C.T.; Huang, Y.K. Cigarette smoking aggravates the activity of periodontal disease by disrupting redox homeostasis-An observational study. Sci. Rep. 2018, 8, 11055. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Shakeeb, N.; Varkey, P.; Ajit, A. Human saliva as a diagnostic specimen for early detection of inflammatory biomarkers by real-time RT-PCR. Inflammation 2021, 44, 1713–1723. [Google Scholar] [CrossRef] [PubMed]
- Ghizoni, J.S.; Nichele, R.; De Oliveira, M.T.; Pamato, S.; Pereira, J.R. The utilization of saliva as an early diagnostic tool for oral cancer: microRNA as a biomarker. Clin. Transl. Oncol. 2020, 22, 804–812. [Google Scholar] [CrossRef]
- Kc, S.; Wang, X.Z.; Gallagher, J.E. Diagnostic sensitivity and specificity of host-derived salivary biomarkers in periodontal disease amongst adults: Systematic review. J. Clin. Periodontol. 2020, 47, 289–308. [Google Scholar] [CrossRef]
- Tomita, A.; Mori, M.; Hiwatari, K.; Yamaguchi, E.; Itoi, T.; Sunamura, M.; Soga, T.; Tomita, M.; Sugimoto, M. Effect of storage conditions on salivary polyamines quantified via liquid chromatography-mass spectrometry. Sci. Rep. 2018, 8, 12075. [Google Scholar] [CrossRef]
- Sharma, M.D.; Nahar, P.; Singh, M.P.; Bhuvaneshwari, S.; Goel, S.; Mathur, H. Saliva as a diagnostic tool for evaluating oxidative stress in periodontitis and its correlation with tobacco habits: A cross sectional study. J. Indian Acad. Oral Med. Radiol. 2018, 30, 361. [Google Scholar] [CrossRef]
- Gupta, N.; Gupta, N.D.; Goyal, L.; Moin, S.; Khan, S.; Gupta, A.; Garg, S. The influence of smoking on the levels of matrix metalloproteinase-8 and periodontal parameters in smoker and nonsmoker patients with chronic periodontitis: A clinicobiochemical study. J. Oral Biol. Craniofac. Res. 2016, 6, S39–S43. [Google Scholar] [CrossRef] [PubMed]
- Gursoy, U.K.; Könönen, E.; Pradhan-Palikhe, P.; Tervahartiala, T.; Pussinen, P.J.; Suominen-Taipale, L.; Sorsa, T. Salivary MMP-8, TIMP-1, and ICTP as markers of advanced periodontitis. J. Clin. Periodontol. 2010, 37, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, B.; Pan, C.; Zhang, A. To evaluate the serum cortisol, salivary cortisol, and serum interleukin-1 b level in patients of chronic periodontitis with smoking and stress and without smoking and stress. Medicine 2021, 100, e26757. [Google Scholar] [CrossRef] [PubMed]
- Lamster, I.B.; Holmes, L.G.; Gross, K.B.; Oshrain, R.L.; Cohen, D.W.; Rose, L.F.; Peters, L.M.; Pope, M.R. The relationship of beta-glucuronidase activity in crevicular fluid to clinical parameters of periodontal disease. Findings from a multicenter study. J. Clin. Periodontol. 1994, 21, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Bastos, M.F.; Tucci, M.A.; De Siqueira, A.; De Faveri, M.; Figueiredo, L.C.; Vallim, P.C.; Duarte, P.M. Diabetes may affect the expression of matrix metalloproteinases and their inhibitors more than smoking in chronic periodontitis. J. Periodont. Res. 2017, 52, 292–299. [Google Scholar] [CrossRef] [PubMed]
- de Lima, C.L.; Acevedo, A.C.; Grisi, D.C.; Taba, M., Jr.; Guerra, E.; de Luca, C.G. Hosts-derived salivary biomarkers in diagnosing periodontal disease. systematic review and meta-analysis. J. Clin. Periodontol. 2016, 43, 492–502. [Google Scholar] [CrossRef]
- Lahdentausta, L.; Paju, S.; Mäntylä, P.; Buhlin, K.; Pietiäinen, M.; Tervahartiala, T.; Nieminen, M.S.; Sinisalo, J.; Sorsa, T.; Pussinen, P.J. Smoking confounds the periodontal diagnostics using saliva biomarkers. J. Periodontol. 2019, 90, 475–483. [Google Scholar] [CrossRef]
- Lin, C.Y.; Chen, Z.; Pan, W.L.; Wang, H.L. Is History of Periodontal Disease Still a Negative Risk Indicator for Peri-implant Health under Supportive Post-implant Treatment Coverage? A Systematic Review and Meta-analysis. Int. J. Oral Maxillofac. Implants 2020, 35, 52–62. [Google Scholar] [CrossRef]
- Zhang, L.; Li, X.; Yan, H.; Huang, L. Salivary matrix metalloproteinase (MMP)-8 as a biomarker for periodontitis: A PRISMA-compliant systematic review and meta-analysis. Medicine 2018, 97, e9642. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 010502. [Google Scholar] [CrossRef]
- Willis, B.H.; Riley, R.D. Measuring the statistical validity of summary meta-analysis and meta-regression results for use in clinical practice. Stat. Med. 2017, 36, 3283–3301. [Google Scholar] [CrossRef] [PubMed]
- Ellenberg, S.S.; Keusch, G.T.; Babiker, A.G.; Edwards, K.M.; Lewis, R.J.; Lundgren, J.D.; Wells, C.D.; Wabwire-Mangen, F.; McAdam, K.P.W.J. Rigorous clinical trial design in public health emergencies is essential. Clin. Infect. Dis. 2018, 66, 1467–1469. [Google Scholar] [CrossRef] [PubMed]
- Helman, S.K.; Mummah, R.O.; Gostic, K.M.; Buhnerkempe, M.G.; Prager, K.C.; Lloyd-Smith, J.O. Estimating prevalence and test accuracy in disease ecology: How Bayesian latent class analysis can boost or bias imperfect test results. Ecol. Evol. 2020, 10, 7221–7232. [Google Scholar] [CrossRef] [PubMed]
- Kanmaz, B.; Lamont, G.; Danacı, G.; Gogeneni, H.; Buduneli, N.; Scott, D.A. Microbiological and biochemical findings in relation to clinical periodontal status in active smokers, non-smokers and passive smokers. Tob. Induc Dis. 2019, 17, 20. [Google Scholar] [CrossRef]
- Al-Nasser, L.; Lamster, I.B. Prevention and management of periodontal diseases and dental caries in the older adults. Periodontology 2020, 84, 69–83. [Google Scholar] [CrossRef]
- Armstrong, A.J.S.; Parmar, V.; Blaser, M.J. Assessing saliva microbiome collection and processing methods. NPJ Biofilms Microbiomes 2021, 7, 81. [Google Scholar] [CrossRef]
- Holliday, R.S.; Campbell, J.; Preshaw, P.M. Effect of nicotine on human gingival, periodontal ligament and oral epithelial cells. A systematic review of the literature. J. Dent. 2019, 86, 81–88. [Google Scholar] [CrossRef]


{kind=link}
| PICOT | Content |
|---|---|
| Patient | Systemically healthy participants with periodontal disease |
| Index test | Expression of biomarkers in saliva |
| Comparison | Clinical parameters (probing pocket depth and clinical attachment loss) or clinical and radiographic parameters (bone loss), irrespective of the diagnostic criteria |
| Outcome | Differences in salivary biomarker levels based on smoking status |
| Type of study | Prospective and retrospective study design |
| Authors (Year Published) | Risk of Bias | Applicability Concern | |||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
| Naresh et al. [6] | ☹ | ? | ☺ | ☺ | ☺ | ☺ | ☺ |
| Ali et al. [5] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | ☺ |
| Bawankar et al. [7] | ☹ | ? | ☺ | ☺ | ☺ | ☺ | ☺ |
| Sharma et al. [38] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | ☺ |
| Gupta et al. [39] | ☹ | ? | ☺ | ☺ | ☺ | ☺ | ☺ |
| Hendek et al. [8] | ☹ | ? | ☺ | ☺ | ☺ | ☺ | ☺ |
| Gursoy et al. [40] | ☹ | ? | ☺ | ☺ | ☺ | ☺ | ☺ |
| Authors | Country | Study Design | Cases | Age (Year) * | Definition of PD | Definition of Smoking Status | Type of Salivary Biomarkers | Main Conclusion |
|---|---|---|---|---|---|---|---|---|
| Naresh et al. [6] | India | Clinicobiochemical study | 30 smokers; 30 non-smokers | 20–60 | Chronic PD: >20 residual teeth, >1 teeth with sites of PPD ≥ 4 mm, and CAL ≥ 4 mm in all four quadrants | Non-smoker: never smoked; smoker: have smoked ≥10 cigarettes/day for ≥5 years | SOD, GPx, MDA, SA | Reduced levels of antioxidant enzymes and elevated levels of lipid peroxidation product could be used as diagnostic markers to measure oxidative stress in PD associated with risk factors such as smoking |
| Ali et al. [5] | India | Cross-sectional case-control study | 50 smokers; 50 non-smokers | 30–35 | Chronicgeneralized periodontitis: PPD ≥ 5 mm, CAL ≥ 3 mm, and moderate, severe, or generalized disease progression involving >30% of the mouth | Non-smoker: never smoked; smoker: currently smoke ≥5 times/day and have smoked for ≥5 years | Activity of LDH and BetaG | Smoking significantly altered enzymeactivity; however, LDH and BetaG were reliable salivary biomarkers of PD among smokers and non-smokers |
| Bawankar et al. [7] | India | Observational study | 25 smokers; 25 non-smokers | 30–65 | Untreated moderate to severe CP: PPD ≥ 5 mm and CAL ≥ 5 mm, ≥30% of teeth affected, and radiographic evidence of bone loss | Non-smoker: never smoked; smoker: current smoker and with history of smoking ≥10 cigarettes/day for the last 3 years | Cortisol, IL-1β | Smokers with PD exhibited a significantly higher salivary cortisol and IL-1β; thus, they may have an increased risk of PD and PD severity |
| Sharma et al. [40] | India | Cross-sectional study | 25 smokers; 25 non-smokers | Smokers: 33.32; non-smokers: 34.32 | PD: clinically diagnosed with periodontitis in accordance with Russell’s periodontal index score | Non-smoker: no tobacco-related habits; smoker: having tobacco-related habits both smoke and smokeless form | UA, ALB | Saliva can be used as a non-invasive diagnostic fluid with UA and ALB being promising biomarkers in monitoring PD |
| Gupta et al. [41] | India | Clinicobiochemical study | 20 smokers; 20 non-smokers | Smokers: 44.20 ± 7.40; non-smokers: 42.80 ± 8.02 | Moderate to severe chronic PD: ≥2 interproximal sites with CAL ≥4 mm or ≥2 interproximal sites with PPD ≥5 mm, not on the same tooth | Non-smoker: never smoked; smoker: smoked ≥1 pack/day for at least past 10 years | MMP-8 | MMP-8 is related to periodontium destruction with smoking |
| Hendek et al. [8] | Turkey | Case-control study | 24 smokers; 23 non-smokers | Smokers: 45 (12); non-smokers: 44 (15) | Chronic PD: teeth with 30% periodontal bone loss and ≥2 non-adjacent sites per quadrant with PPD ≥ 5 mm and bleeding on probing | Non-smoker: never smoked; smoker: current smoking of 10 years and ≥10 cigarettes/day | GPx | GPx enzyme activities can be used to determine the protective mechanisms against oxidative stress |
| Gursoy et al. [42] | Finland | Cross-sectional study | 44 smokers; 40 non-smokers † | Smokers: 48.6 ± 5.3; non-smokers: 50.7 ± 4.9 | Advanced periodontitis: ≥14 residual teeth with PPD ≥ 4 mm | N/A | MMP-8, MMP-14, TIMP-1, and ICTP | The combinations and ratios of salivary MMP-8, TIMP-1, and ICTP are particularly potential candidates for the detection of advanced periodontitis |
| Authors | Salivary Biomarker | Detection Method | Results * | Significance | |
|---|---|---|---|---|---|
| Non-Smoker | Smoker | ||||
| Naresh et al. [6] | SOD (U/mL) | Spectrophotometry | 50.41 ± 4.25 | 34.96 ± 4.8 | p < 0.001 |
| Naresh et al. [6] | MDA (nmol/µL) | Spectrophotometry | 0.47 ± 0.11 | 0.69 ± 0.13 | p < 0.001 |
| Naresh et al. [6] | Sialic acid (nmol/µL) | Spectrophotometry | 0.14 ± 0.02 | 0.22 ± 0.04 | p < 0.001 |
| Naresh et al. [6] | GPx (U/L) | Spectrophotometry | 124.41 ± 4.74 | 111.39 ± 6.79 | p < 0.001 |
| Hendek et al. [8] | GPx (U/µL) | ELISA | 30.59 ± 15.06 | 36.81 ± 9.16 | p = 0.003 |
| Ali et al. [5] | Activity of LDH (nmol/min/mg) | Spectrophotometry | 896.56 ± 264.14 | 682.58 ± 274.12 | N/A |
| Ali et al. [5] | Activity of BetaG (nmol/min/mg) | Spectrophotometry | 76.46 ± 10.43 | 71.27 ± 12.71 | N/A |
| Bawankar et al. [7] | Cortisol (pg/mL) | ELISA | 417.16 ± 99.67 | 563.40 ± 236.19 | p < 0.0001 |
| Bawankar et al. [7] | IL-1β (pg/mL) | ELISA | 251.35 ± 81.19 | 278.95 ± 81.40 | p < 0.0001 |
| Sharma et al. [40] | UA (mg/mL) | Spectrophotometry | 1.95 ± 0.423 | 0.94 ± 0.200 | p < 0.01 |
| Sharma et al. [40] | ALB (g/mL) | Spectrophotometry | 45.44 ± 8.032 | 47.04 ± 16.032 | p > 0.05 |
| Gupta et al. [41] | MMP-8 (ng/mL) | ELISA | 354.83 ± 29.91 | 459.16 ± 24.30 | p < 0.001 |
| Gursoy et al. [42] | MMP-8 (ng/mL) | TR-IFMA | 1075.5 (345.2–1715.9) | 703.1 (338.6–1646.7) | N/A |
| Gursoy et al. [42] | MMP-8 (ng/mL) | ELISA | 96.7 (61.8–144.7) | 83.6 (52.9–114.5) | N/A |
| Gursoy et al. [42] | TIMP-1 (ng/mL) | ELISA | 45.5 (23.3–112.3) | 73.0 (42.0–164.0) | N/A |
| Gursoy et al. [42] | ICTP (ng/mL) | EIA | 0.74 (0.56–0.96) | 0.75 (0.60–0.94) | N/A |
| Gursoy et al. [42] | MMP-14 (with APMA) (ng/mL) | ELISA | 229.3 (138.1–360.3) | 176.2 (112.7–288.3) | N/A |
| Gursoy et al. [42] | MMP-14 (without APMA) (ng/mL) | ELISA | 8.48 (2.21–11.88) | 9.31 (4.3–12.8) | N/A |
| Gursoy et al. [42] | MMP-8/TIMP-1 ratio | TR-IFMA | 15.44 ± 21.48 | 8.26 ± 11.05 | N/A |
| Gursoy et al. [42] | MMP-8/TIMP-1 ratio | ELISA | 1.30 ± 1.27 | 0.69 ± 0.72 | N/A |
| Gursoy et al. [42] | MMP-8 and ICTP combination | TR-IFMA | 0.62 ± 0.23 | 0.58 ± 0.23 | N/A |
| Gursoy et al. [42] | MMP-8 and ICTP combination | ELISA | 0.55 ± 0.12 | 0.52 ± 0.12 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noh, J.-w.; Jang, J.-H.; Yoon, H.-S.; Kim, K.-B.; Heo, M.-H.; Jang, H.-e.; Kim, Y.-J.; Lee, Y. Evaluation of Salivary Biomarkers of Periodontal Disease Based on Smoking Status: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 14619. https://doi.org/10.3390/ijerph192114619
Noh J-w, Jang J-H, Yoon H-S, Kim K-B, Heo M-H, Jang H-e, Kim Y-J, Lee Y. Evaluation of Salivary Biomarkers of Periodontal Disease Based on Smoking Status: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(21):14619. https://doi.org/10.3390/ijerph192114619
Chicago/Turabian StyleNoh, Jin-won, Jong-Hwa Jang, Hae-Soo Yoon, Kyoung-Beom Kim, Min-Hee Heo, Ha-eun Jang, Young-Jin Kim, and Yejin Lee. 2022. "Evaluation of Salivary Biomarkers of Periodontal Disease Based on Smoking Status: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 21: 14619. https://doi.org/10.3390/ijerph192114619
APA StyleNoh, J.-w., Jang, J.-H., Yoon, H.-S., Kim, K.-B., Heo, M.-H., Jang, H.-e., Kim, Y.-J., & Lee, Y. (2022). Evaluation of Salivary Biomarkers of Periodontal Disease Based on Smoking Status: A Systematic Review. International Journal of Environmental Research and Public Health, 19(21), 14619. https://doi.org/10.3390/ijerph192114619