
“Without Them, I Would Never Have Been Able to Carry on” Levers for the Sustained Employment of Patients with Chronic Inflammatory Arthritis: A French Qualitative Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
- -
- Nine participants were interviewed face-to-face in Nancy (France). On-site interviews were made possible by the geographical proximity between the researchers and the participants. This first phase of the survey allowed us to identify the majority of the job retention facilitators.
- -
- Four participants were interviewed through a focus group in Montpellier (France) in partnership with the ANDAR, a patient association. This second step of the survey provided feedback on the first results and allowed us to deepen our observations through discussions and the differences in experiences reported by the participants.
- -
- Five participants were interviewed via phone calls: two in Grenoble (France) and three in Marseille (France). This survey modality was adopted because of the geographical distance between the researchers and the participants. The non-verbal language observation was conceded, as this third phase of the survey was merely to check the accuracy of our observations. It was a way to ensure that we did not miss any important information during the previous phases of the survey. This third phase of the survey also helped to diversify the field and socio-economic contexts.
- -
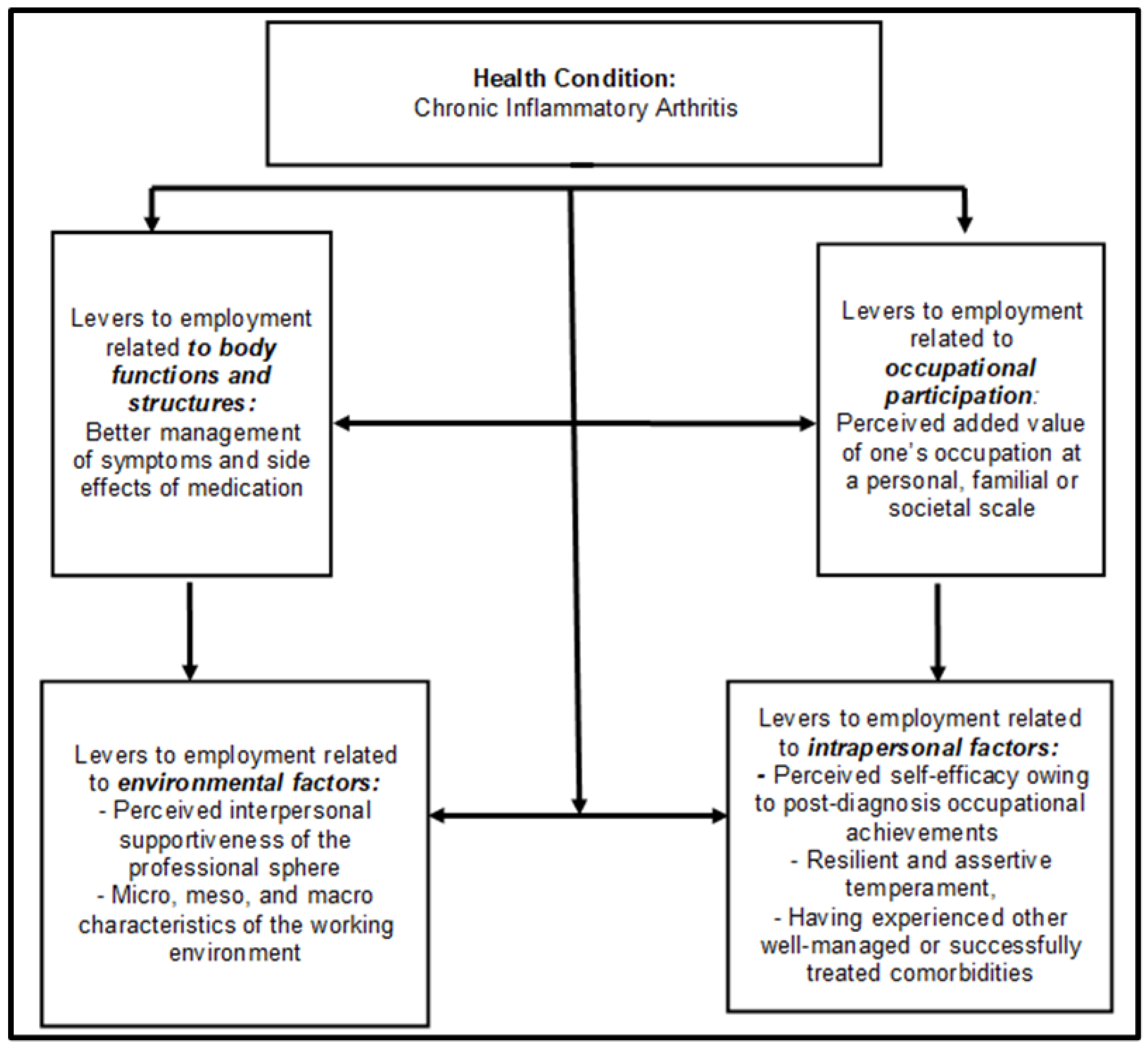
- At the micro-individual scale: ergonomic workstation design or flexible scheduling;
- -
- At the meso-professional level: inclusiveness policies implemented by one’s organization, awareness and acquaintance of one’s coworkers regarding invisible disabilities, the presence of other coworkers with disabilities or similar illnesses, and in the present case, the pathologies affecting the locomotor apparatus;
- -
- At the macro-societal scale: national legislation promoting employment retention among vulnerable workers, fiscal and other financial incentives to accommodate or reclassify such workers, and coercive sanctions against unfair or unjustified dismissals of such workers.
- -
- The perceived self-efficacy owing to post-diagnosis occupational achievements;
- -
- A resilient and assertive temperament;
- -
- Having experienced other well-managed or successfully treated comorbidities.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kleinert, S.; Bartz-Bazzanella, P.; von der Decken, C.; Knitza, J.; Witte, T.; Fekete, S.P.; Konitzny, M.; Zink, A.; Gauler, G.; Wurth, P.; et al. A Real-World Rheumatology Registry and Research Consortium: The German RheumaDatenRhePort (RHADAR) Registry. J. Med. Int. Res. 2021, 23, e28164. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, T.M.; Primdahl, J.; Antoft, R.; Hørslev-Petersen, K. Everyday Life with Rheumatoid Arthritis and Implications for Patient Education and Clinical Practice: A Focus Group Study. Musculoskelet. Care 2012, 10, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Stack, R.J.; Nightingale, P.; Jinks, C.; Shaw, K.; Herron-Marx, S.; Horne, R.; Deighton, C.; Kiely, P.; Mallen, C.; Raza, K. Delays between the Onset of Symptoms and First Rheumatology Consultation in Patients with Rheumatoid Arthritis in the UK: An Observational Study. BMJ Open 2019, 9, e024361. [Google Scholar] [CrossRef]
- Strand, V.; Thomas, V.; Jones, W.L.; Andrew, S. The impact of rheumatoid arthritis on work and predictors of overall work impairment from three therapeutic scenarios. Int. J. Clin. Rheumatol. 2015, 1758, 4272. [Google Scholar] [CrossRef]
- French Health Care System. Mapping of Conditions and Expenditures by Age, Pathology, Sex. 2020. Available online: https://assurance-maladie.ameli.fr/etudes-et-donnees/cartographie-effectif-patients-par-pathologie-age-sexe-2020 (accessed on 11 October 2022).
- Sokka, T.; Kautiainen, H.; Pincus, T.; Verstappen, S.M.; Aggarwal, A.; Alten, R.; Andersone, D.; Badsha, H.; Baecklund, E.; Belmonte, M.; et al. Work disability remains a major problem in rheumatoid arthritis in the 2000s: Data from 32 countries in the QUEST-RA study. Arthritis Res. Ther. 2010, 12, R42. [Google Scholar] [CrossRef] [PubMed]
- Barbour, K.E.; Helmick, C.G.; Theis, K.A.; Murphy, L.B.; Hootman, J.M.; Brady, T.J.; Cheng, Y.J. Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation in United States. Morb. Mortal. Wkly. Rep. 2013, 62, 869–873. [Google Scholar]
- Gignac, M.A.; Cao, X.; Tang, K.; Beaton, D.E. Examination of arthritis-related workplace activity limitations and intemittent disability over four and a half years and its relationship to job modifications and outcomes. Arthritis Care Res. 2011, 63, 953–962. [Google Scholar] [CrossRef]
- Tang, K.; Escorpizo, R.; Beaton, D.E.; Bombardier, C.; Lacaille, D.; Zhang, W.; Anis, A.H.; Boonen, A.; Verstappen, S.M.; Buchbinder, R.; et al. Measuring the impact of arthritis on worker productivity: Perspectives, methodologic issues, and contextual factors. J. Rheumatol. 2011, 38, 1776–1790. [Google Scholar] [CrossRef]
- Barnabe, C.; Wattiaux, A.; Petkovic, J.; Beaton, D.; Shea, B.; Greer-Smith, R.; Umaefulam, V. Validation Studies of Rheumatoid Arthritis Patient-Reported Outcome Measures in Populations at Risk for Inequity: A Systematic Review and Analysis Using the OMERACT Summary of Measurement Properties Equity Table. Semin. Arthritis Rheum. 2022, 55, 152029. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update Annals of the Rheumatic Diseases. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef]
- De Croon, E.M.; Sluiter, J.K.; Nijssen, T.F.; Dijkmans, B.A.; Lankhorst, G.J.; Frings-Dresen, M.H. Predictive factors of work disability in rheumatoid arthritis: A systematic literature review. Ann. Rheum. Dis. 2004, 63, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Detaille, S.I.; Heerkens, Y.F.; Engels, J.A.; van der Gulden, J.W.; van Dijk, F.J. Common prognostic factors of work disability among employees with a chronic somatic disease: A systematic review of cohort studies. Scand. J. Work Environ. Health 2009, 35, 261–281. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.; Mays, N. Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ 1995, 311, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Cardon, D. L’entretien compréhensif (Jean-Claude Kaufmann). Réseaux Commun. Technol. Soc. 1996, 14, 177–179. [Google Scholar]
- Krueger, R.A. Focus Groups: A Practical Guide for Applied Research; Sage Publications: Newbury Park, CA, USA, 2014. [Google Scholar]
- Mills, J.; Bonner, A.; Francis, K. Adopting a constructivist approach to grounded theory: Implications for research design. Int. J. Nurs. Pract. 2006, 12, 8–13, Erratum in Int. J. Nurs. Pract. 2006, 12, 119. [Google Scholar] [CrossRef]
- O’Sullivan, D.; Cambria, A.; Xiao, Y.; Chang, H. The World Health Organization’s (WHO) International Classification of Health and Functioning Framework revisited: A tool with clinical, research, and educational utility for counselors. Aust. J. Rehabil. Couns. 2019, 25, 122–137. [Google Scholar] [CrossRef]
- Kostanjsek, N. Use of The International Classification of Functioning, Disability and Health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health 2011, 31 (Suppl. 4), S3. [Google Scholar] [CrossRef]
- Purc-Stephenson, R.J.; Dostie, J.; Smith, H.J. Swimming Against the Current: A Qualitative Review of the Work Experiences and Adaptations Made by Employees with Arthritis. Arthritis Care Res. 2018, 70, 1587–1597. [Google Scholar] [CrossRef]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1992. [Google Scholar]
- Stergiou-Kita, M.; Grigorovich, A.; Tseung, V.; Milosevic, E.; Hebert, D.; Phan, S.; Jones, J. Qualitative meta synthesis of survivors’ work experiences and the development of strategies to facilitate return to work. J. Cancer Surviv. 2014, 8, 657–670. [Google Scholar] [CrossRef]
- Nikiphorou, E.; Santos, E.J.F.; Marques, A.; Böhm, P.; Bijlsma, J.W.; Daien, C.I.; Esbensen, B.A.; Ferreira, R.J.O.; Fragoulis, G.E.; Holmes, P.; et al. 2021 EULAR recommendations for the implementation of self-management strategies in patients with inflammatory arthritis. Ann. Rheum. Dis. 2021, 80, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Verstappen, S.M. Rheumatoid arthritis and work: The impact of rheumatoid arthritis on absenteeism and presenteeism. Best Pract. Res. Clin. Rheumatol. 2015, 29, 495–511. [Google Scholar] [CrossRef] [PubMed]
- Jetha, A.; Badley, E.; Beaton, D.; Fortin, P.R.; Shiff, N.J.; Gignac, M.A.M. Unpacking Early Work Experiences of Young Adults with Rheumatic Disease: An Examination of Absenteeism, Job Disruptions, and Productivity Loss. Arthritis Care Res. 2015, 67, 1246–1254. [Google Scholar] [CrossRef]
- Pinheiro, F.; Madureira, P.; Fernandes, B.; Garcia, S.; Rato, M.; Fonseca, D.; Oliveira, D.; Martins, A.; Samões, B.; Bernardes, M.; et al. Différences entre les sexes dans la spondyloarthrite-les femmes commencent-elles en étant désavantagées? Rev. Rhum. 2021, 88, A231–A232. [Google Scholar] [CrossRef]
- Yang, D.H.; Huang, J.Y.; Chiou, J.Y.; Wei, J.C. Analysis of Socioeconomic Status in the Patients with Rheumatoid Arthritis. Int. J. Environ. Res. Public Health 2018, 15, 1194. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type of IA | Socio-Professional Category (SPC) | Centers (France) | Sex Proportion (Women/Men) | Mean Age (Years) | |||||
|---|---|---|---|---|---|---|---|---|---|
| PR **** | JIA *** | RA ** | SpA * | High SPC | Medium SPC | Low SPC | |||
| 0 | 1 | 3 | 5 | 2 | 6 | 1 | 9 Nancy | 7/2 | 43.4 |
| 3 | 0 | 1 | 0 | 1 | 2 | 1 | 4 Montpellier | 1/3 | 46.2 |
| 0 | 0 | 1 | 1 | 0 | 1 | 1 | 2 Grenoble | 1/1 | 45.0 |
| 0 | 0 | 1 | 2 | 0 | 0 | 3 | 3 Marseille | 2/1 | 43.3 |
| 3 | 1 | 6 | 8 | 3 | 9 | 6 | 18 | 11/7 | 44.2 |
| Emergent Topics | Underlying Grounds | Illustrating Verbatim Records |
|---|---|---|
| 1. Levers related to improvement in disease management |
|
|
| 2. Levers related to the perceived added value of one’s occupation at a personal, familial, or societal scale. |
|
|
| 3. Levers related to the perceived interpersonal supportiveness of the professional sphere |
|
|
| 4. Levers related to the characteristics of the working environment |
|
|
| 5. Levers related to intrapersonalattributes |
|
|
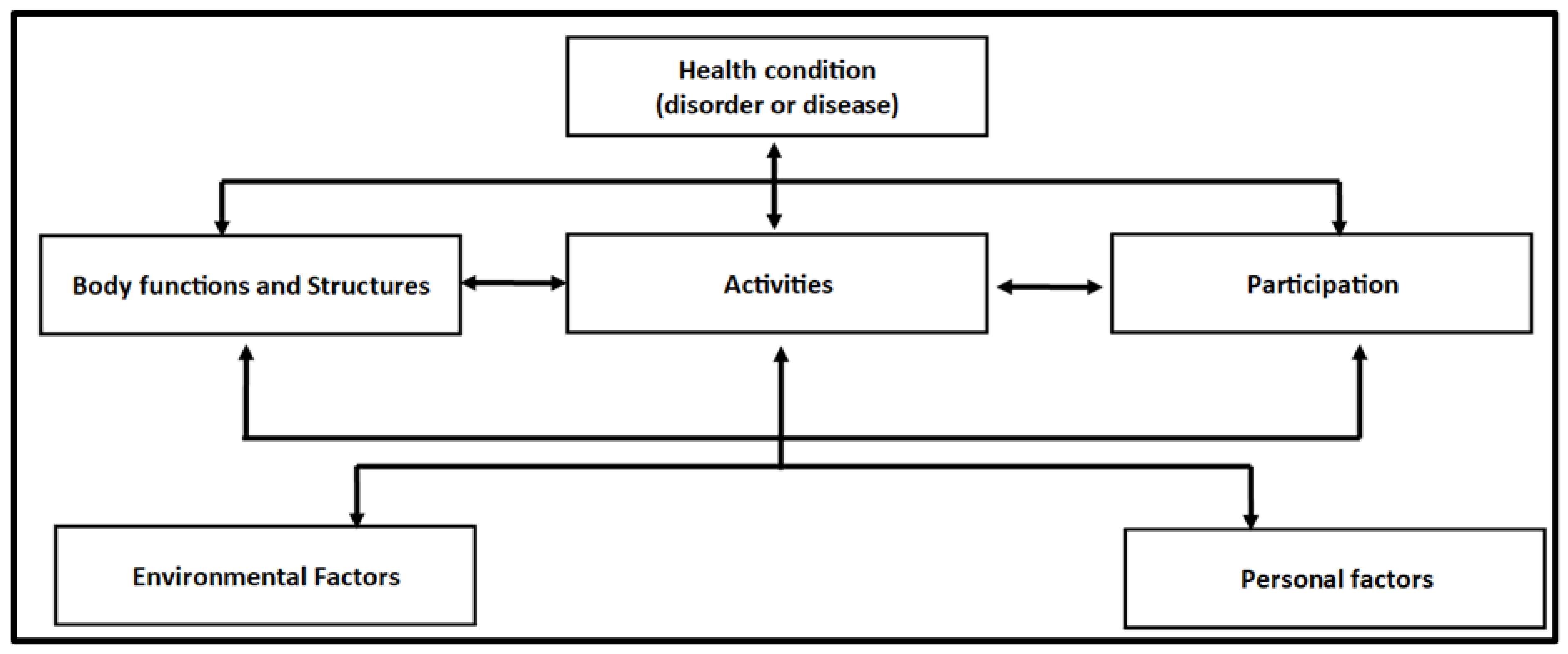
| ICF Components’ Definition | Correspondence with ICF Components | Emergent Topics from Analysis |
|---|---|---|
| It refers to impairments and problems with body functions or anatomical systems, manifested by a significant gap or loss. | Body functions and structures | 1. Levers related to the improvement in the management of the disease, its related symptoms, and medication observance |
| It refers to the ability to take part in a social, familial, or professional real-life situation. | Participation | 2. Levers related to the perceived added value of one’s occupation at a personal, familial, or societal scale |
| It refers to the physical, social, and attitudinal environments in which people live and conduct their lives. | Environmental Factors | 3. Levers related to the perceived interpersonal supportiveness of the professional sphere |
| 4. Levers related to the micro-, meso-, and macro-characteristics of the working environment | ||
| refers to the specific living environment of an individual, consisting of characteristics of the person that are not part of a health problem or condition | Personal factors | 5. Levers related to intrapersonal attributes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Louati, C.; Mouelhi, Y.; Kabuth, B.; Clément, C. “Without Them, I Would Never Have Been Able to Carry on” Levers for the Sustained Employment of Patients with Chronic Inflammatory Arthritis: A French Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 14616. https://doi.org/10.3390/ijerph192114616
Louati C, Mouelhi Y, Kabuth B, Clément C. “Without Them, I Would Never Have Been Able to Carry on” Levers for the Sustained Employment of Patients with Chronic Inflammatory Arthritis: A French Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(21):14616. https://doi.org/10.3390/ijerph192114616
Chicago/Turabian StyleLouati, Chaima, Yosra Mouelhi, Bernard Kabuth, and Céline Clément. 2022. "“Without Them, I Would Never Have Been Able to Carry on” Levers for the Sustained Employment of Patients with Chronic Inflammatory Arthritis: A French Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 21: 14616. https://doi.org/10.3390/ijerph192114616
APA StyleLouati, C., Mouelhi, Y., Kabuth, B., & Clément, C. (2022). “Without Them, I Would Never Have Been Able to Carry on” Levers for the Sustained Employment of Patients with Chronic Inflammatory Arthritis: A French Qualitative Study. International Journal of Environmental Research and Public Health, 19(21), 14616. https://doi.org/10.3390/ijerph192114616