
Efficacy of Different Types of Physical Activity Interventions on Exercise Capacity in Patients with Chronic Obstructive Pulmonary Disease (COPD): A Network Meta-Analysis

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
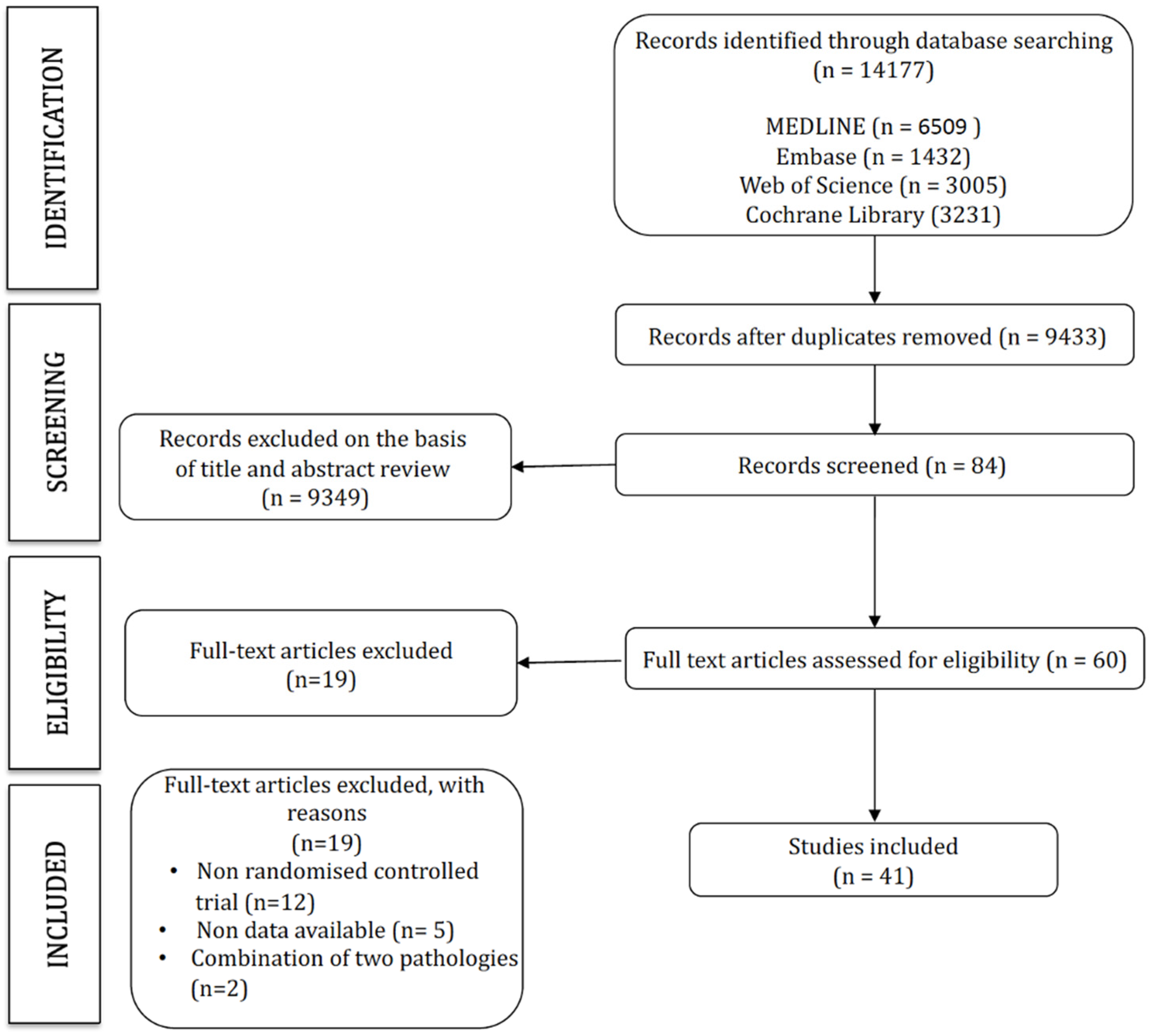
2.1. Search Strategy and Selection Criteria
2.2. Eligibility
2.3. Data Extraction
2.4. Categorization of the Interventions
2.5. Assessment of Risk of Bias
2.6. Rating of the Quality of the Evidence
2.7. Data Synthesis and Statistical Analysis
3. Results
3.1. Risk of Bias
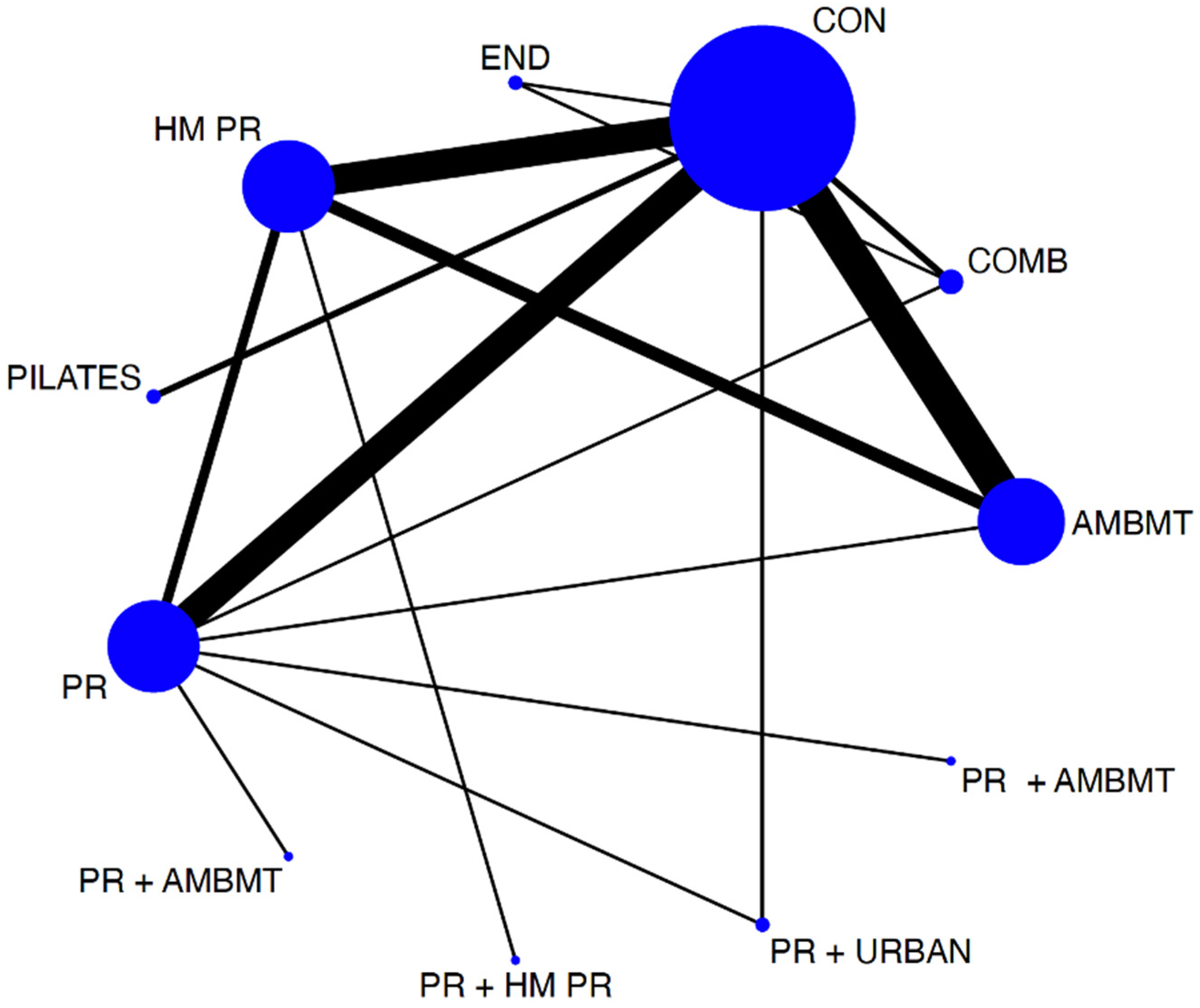
3.2. Network Analyses
3.3. Modalities of Exercise and Their Effect on Exercise Capacity
3.4. Best Treatment Probabilities
3.5. Sensitivity Analysis, Heterogeneity, and Publication Bias
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miravitlles, M.; Almagro Mena, P.; Ancochea Bermúdez, J.; Calle Rubio, M.; Carretero Díaz, M.E.; Casanova, C.; Chiner, E.; Cosío Piqueras, B.G.; Gimeno-Santos, E.; Hernández, C.; et al. Guía de Práctica Clínica para el Diagnóstico y Tratamiento de Pacientes con Enfermedad Pulmonar Obstructiva Crónica (EPOC)—Guía Española de la EPOC (GesEPOC). Arch. Bronconeumol. 2017, 53, 2–64. [Google Scholar]
- WHO. Enfermedad Pulmonar Obstructiva Crónica (EPOC). Available online: https://www.who.int/es/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (accessed on 20 May 2022).
- Vázquez, R.A.; Tarraga, M.A. Enfermedad Pulmonar Obstructiva Crónica y comorbilidad. JONNPR 2020, 5, 1195–1220. [Google Scholar] [CrossRef]
- Agusti, A.; Soriano, J.B. Copd as a systemic disease. COPD 2008, 5, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Vorrink, S.N.; Kort, H.S. Level of daily physical activity in individuals with copd compared with healthy controls. Respir. Res. 2011, 12, 33. [Google Scholar] [CrossRef]
- Alhamari, A.D.; Kowlessar, B.S. Physical activity and exercise capacity in patients with moderate COPD exacerbations. Eur. Respir. J. 2016, 48, 340–349. [Google Scholar] [CrossRef]
- Remels, A.H.; Gosker, H.R. The mechanisms of cachexia underlying muscle dysfunction in COPD. J. Appl. Physiol. 2013, 114, 1253–1262. [Google Scholar] [CrossRef]
- Ortega, F.; Valencia, B. Relación entre el grado de extensión del enfisema y alteraciones morfológicas musculares periféricas en pacientes con EPOC. Rev. Esp. Patol. Torac. 2016, 28, 198–205. [Google Scholar]
- ATS/ACCP. Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef]
- Oga, T.; Nishimura, K. Analysis of the factors related to mortality in chronic obstructive pulmonary disease: Role of exercise capacity and health status. Am. J. Respir. Crit. Care Med. 2003, 167, 544–549. [Google Scholar] [CrossRef]
- Martinez, F.J.; Foster, G. Predictors of mortality in patients with emphysema and severe airflow obstruction. Am. J. Respir. Crit. Care Med. 2006, 173, 1326–1334. [Google Scholar] [CrossRef]
- Carter, R.; Holiday, D. 6-Minute Walk Work for Assessment of Functional Capacity in Patients with COPD. Chest 2003, 123, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Gochicoa-Rangel, L.; Mora-Romero, U. Prueba de caminata de 6 minutos: Recomendaciones y procedimientos. Neumol. Cirugía Torax 2015, 74, 127–136. [Google Scholar] [CrossRef]
- Cote, C.G.; Casanova, C. Validation and comparison of reference equations for the 6-min walk distance test. Eur. Respir. J. 2008, 31, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Pitta, F.; Troosters, T. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 171, 972–977. [Google Scholar] [CrossRef]
- Martijn, A.; Spruit, M. Determinants of poor 6-min walking distance in patients with COPD: The ECLIPSE cohort. Respir. Med. 2010, 104, 849–857. [Google Scholar] [CrossRef]
- Çiftci, F.; Şen, E. A comparison of cardiopulmonary exercise test and 6-minute walking test in determination of exercise capacity in chronic obstructive pulmonary disease. Tuberk Toraks 2014, 62, 259–266. [Google Scholar] [CrossRef]
- Holland, A.E.; Cox, N.S. Defining Modern Pulmonary Rehabilitation. An Official American Thoracic Society Workshop Report. Ann. Am. Thorac. Soc. 2021, 18, 12–29. [Google Scholar] [CrossRef]
- Tarigan, A.P.; Ananda, F.R. Exercise Training and Pulmonary Rehabilitation in COPD. In Chronic Obstructive Pulmonary Disease. A Current Conspectus; Ong, K.C., Ed.; IntechOpen: London, UK, 2021. [Google Scholar]
- Hutton, B.; Catala-Lopez, F. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022; Available online: https://www.training.cochrane.org/handbook (accessed on 23 May 2022).
- McGavin, C.R.; Gupta, S.P. Physical rehabilitation for the chronic bronchitic: Results of a controlled trial of exercises in the home. Thorax 1977, 32, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Busch, A.J.; McClements, J.D. Effects of a supervised home exercise program on patients with severe chronic obstructive pulmonary disease. Phys. Ther. 1988, 68, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Salanti, G.; Ades, A. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Chaimani, A.; Higgins, J.P. Graphical tools for network meta-analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a metaanalysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Simpson, K.; Killian, K. Randomised controlled trial of weightlifting exercise in patients with chronic airflow limitation. Thorax 1992, 47, 70–75. [Google Scholar] [CrossRef]
- Bernard, S.; Whittom, F. Aerobic and strength training in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1999, 159, 896–901. [Google Scholar] [CrossRef]
- Spencer, L.M.; Alison, J.A. Maintaining benefits following pulmonary rehabilitation: A randomised controlled trial. Eur. Respir. J. 2010, 35, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.Q.; Donesky, D.A. Internet-Based dypnea self-management support for patients with chronic obstructive pulmonary disease. J. Pain Symptom Manag. 2013, 46, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Maltais, F.; Bourbeau, J. Effects of Home-Based Pulmonary Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease. Ann. Intern. Med. 2008, 149, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Oh, E. The effects of home-based pulmonary rehabilitation in patients with chronic lung disease. Int. J. Nurs. Stud. 2003, 40, 873–879. [Google Scholar] [CrossRef]
- Donesky-Cuenco, D.A.; Nguyen, H.Q. Yoga therapy decreases dypnea-related distress and improves functional performance in people with chronic obstructive pulmonary disease: A pilot study. J. Altern. Complement. Med. 2009, 15, 225–234. [Google Scholar] [CrossRef]
- Liu, X.D.; Jin, H.Z. Therapeutic Effects of Qigong in patients with COPD: A randomized controlled trial. Hong Kong J. Occup. Ther. 2012, 22, 38–46. [Google Scholar] [CrossRef]
- Yeh, G.Y.; Roberts, D.H. Tai Chi exercise for patients with chronic obstructive pulmonary disease: A pilot study. Respir. Care 2010, 55, 1475–1482. [Google Scholar]
- Niu, R.; He, R. The effect of Tai Chi on chronic obstructive pulmonary disease: A pilot randomised study of lung function, exercise capacity and diaphragm strength. Heart Lung Circ. 2014, 23, 347–352. [Google Scholar] [CrossRef]
- Gu, G.; Zhou, Y.M. Effects of shadow boxing training on exercise endurance and quality of life of patients with chronic obstructive pulmonary disease. J. Glob. 2012, 92, 952–955. [Google Scholar]
- Ng, L.; Chiang, L.K.; Tang, R.; Siu, C.; Fung, L.; Lee, A.; Tam, W. Effectiveness of incorporating Tai Chi in a pulmonary rehabilitation program for chronic obstructive pulmonary disease (COPD) in primare care. A pilot randomized controlled trial. Eur. J. Integr. Med. 2014, 6, 248–258. [Google Scholar] [CrossRef]
- Chan, A.W.K.; Lee, A. Tai chi Qigong improves lung functions and activity tolerance in COPD clients: A single blind, randomized controlled trial. Complement. Ther. Med. 2011, 19, 3–11. [Google Scholar] [CrossRef]
- Gottlieb, V.; Lyngsø, A.M. Pulmonary Rehabilitation for moderate COPD (GOLD2)—Does it have an effect? COPD 2011, 8, 380–386. [Google Scholar] [CrossRef]
- Roman, M.; Larraz, C. Efficacy of pulmonary rehabilitation in patients with moderate chronic obstructive pulmonary disease: A randomized controlled trial. BMC Fam. Pract. 2013, 14, 21. [Google Scholar] [CrossRef]
- Engström, C.P.; Persson, L.O. Long-term effects of a pulmonary rehabilitation programme in outpatients with chronic obstructive pulmonary disease: A randomized controlled study. Scand. J. Rehabil. Med. 1999, 31, 207–213. [Google Scholar] [CrossRef]
- Singh, V.; Khandelwal, D.C. Pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Indian J. Chest Dis. Allied Sci. 2003, 45, 13–17. [Google Scholar]
- Borghi-Silva, A.; Arena, R. Aerobic exercise training improves autonomic nervous control in patients with COPD. Respir. Med. 2009, 103, 1503–1510. [Google Scholar] [CrossRef]
- Fernández, A.M.; Pascual, J. Home-Based pulmonary rehabilitation in very severe COPD. Is it safe and useful? J. Cardiopulm. Rehabil. Prev. 2009, 29, 325–331. [Google Scholar] [CrossRef]
- Theander, K.; Jakobsson, P. Effects of pulmonary rehabilitation on fatigue, functional status and health perceptions in patients with chronic obstructive pulmonary disease: A randomized controlled trial. Clin. Rehabil. 2009, 23, 125–136. [Google Scholar] [CrossRef]
- Ghanem, M.; Elaal, E.A. Home-based pulmonary rehabilitation program: Effect of exercise tolerance and quality of life in chronic obstructive pulmonary disease patients. Ann. Thorac. Med. 2010, 5, 18–25. [Google Scholar] [CrossRef]
- Pleguezuelos, E.; Pérez, M.E. Improving physical activity in patients with COPD with urban walking circuits. Respir. Med. 2013, 107, 1948–1956. [Google Scholar] [CrossRef]
- De Sousa Pinto, J.; Martín-Nogueras, A.M. Clinical benefits of home-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. J. Cardiopulm. Rehabil. Prev. 2014, 34, 355–359. [Google Scholar] [CrossRef]
- Chan, A.W.K.; Lee, A. The sustaining effects of Tai chi Qigong on physiological health for COPD patients: A randomized controlled trial. Complement. Ther. Med. 2013, 21, 585–594. [Google Scholar] [CrossRef]
- Zhang, M.; Xv, G.; Luo, C.; Meng, D.J.; Ji, Y. Promotes Pulmonary Function, Physical Activity, Quality of Life and Emotion Regulation Self-Efficacy in Patients with Chronic Obstructive Pulmonary Disease: A Pilot Study. J. Altern. Complement. Med. 2016, 22, 810–817. [Google Scholar] [CrossRef]
- Ranjita, R.; Hankey, A. Yoga-based pulmonary rehabilitation for the management of dyspnea in coal miners with chronic obstructive pulmonary disease: A randomized controlled trial. J. Ayurveda Integr. Med. 2016, 7, 158–166. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, R. Pranayam for treatment of chronic obstructive pulmonary disease: Results from a randomized, controlled trial. Integr. Med. 2014, 13, 26–31. [Google Scholar]
- Xiao, C.M.; Zhuang, Y.C. Efficacy of Liuzijue Qigong in Individuals with Chronic Obstructive Pulmonary Disease in Remission. J. Am. Geriatr. Soc. 2015, 63, 1420–1425. [Google Scholar] [CrossRef]
- Ng, B.; Tsang, H. Functional and Psychosocial Effects of Health Qigong in Patients with COPD: A Randomized Controlled Trial. J. Altern. Complement. Med. 2011, 17, 243–251. [Google Scholar] [CrossRef]
- Papp, M.E.; Wändell, P.E. Effects of yogic exercises on functional capacity, lung function and quality of life in participants with obstructive pulmonary disease: A randomized controlled study. Eur. J. Phys. Rehabil. Med. 2017, 53, 447–461. [Google Scholar] [CrossRef]
- Daabis, R.; Hassan, M. Endurance and strength training in pulmonary rehabilitation for COPD patients. Egypt. J. Chest Dis. Tuberc. 2017, 66, 231–236. [Google Scholar] [CrossRef]
- Fukuoka, A.; Ueda, M. Effect of laughter yoga on pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. J. Nara Med. Assoc. 2016, 67, 11–20. [Google Scholar]
- Hansen, H.; Bieler, T. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: A randomised multicentre trial. Thorax 2020, 75, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Hagag, A.; Salem, E.Y. Pilates exercises improve postural stability, ventilatory functions and functional capacity in patients with chronic obstructive pulmonary disease. IOSR J. Nurs. Health Sci. (IOSR-JNHS) 2019, 8, 86–91. [Google Scholar] [CrossRef]
- Wen, Y.; Lian, L. Effect of a rehabilitation garden on rehabilitation efficacy in elderly patients with chronic obstructive pulmonary disease. Pak. J. Zool. 2020, 52, 2027–2426. [Google Scholar] [CrossRef]
- Kilic, B.; Cicek, H.S. Comparing the effects of self-management and hospital-based pulmonary rehabilitation programs in COPD patients. Niger. J. Clin. Pract. 2021, 24, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Kantatong, T.; Panpanich, R. Effects of tai chi qigong programme on functional capacity, and lung function in chronic obstructive pulmonary disease patients: A randomised controlled trial. J. Tradit. Complement. Med. 2020, 10, 354–359. [Google Scholar] [CrossRef]
- Smyrnova, G.S.; Babkina, T.M. Influence of Pulmonary rehabilitation on clinical characteristics in patients with chronic heart failure and chronic obstructive pulmonary disease. Int. J. Cardiovasc. Sci. 2018, 31, 499–504. [Google Scholar] [CrossRef]
- Pradella, C.O.; Belmonte, G.M. Home-based pulmonary rehabilitation for subjects with COPD: A randomized study. Respir. Care 2015, 60, 526–532. [Google Scholar] [CrossRef]
- Kraemer, K.M.; Litrownik, D. Exploring Tai Chi Exercise and Mind-Body Breathing in Patients with COPD in a Randomized Controlled Feasibility Trial. COPD 2021, 18, 288–298. [Google Scholar] [CrossRef]
- Barakat, S.; Michele, G. Outpatient pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2008, 3, 155–162. [Google Scholar] [CrossRef]
- Güell, M.R.; Díaz, S.; Rodríguez, G.; Morante, F.; San Miguel, M.; Cejudo, P. Rehabilitación respiratoria. Arch. Bronconeumol. 2014, 50, 332–344. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Qaseem, A.; Wilt, T.J. Diagnosis and management of stable chronic obstructive pulmonary disease: A clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann. Intern. Med. 2011, 155, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Isacowitz, R.; Clippinger, K. Pilates Anatomy; Human Kinetics: Windsor, ON, Canada, 2011; pp. 21–22. [Google Scholar]
- Wakde, G.; Patil, P. Effects of Pilates Breathing on Chest Expansion, Dyspnoea and Functional Capacity in COPD Patients—An Experimental Study. Int. J. Res. Rev. 2021, 8, 249–262. [Google Scholar] [CrossRef]
- Cancelliero-Gaiad, K.M.; Ike, D. Respiratory pattern of diaphragmatic breathing and Pilates breathing in COPD subjects. Braz. J. Phys. Ther. 2014, 18, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Miranda, L.B.; Morais, P.D.C. Efeitos do método pilates sobre a composicão corporal e flexibilidade [Effects of the Pilates method on the body composition and flexibility]. Rev. Bras. Prescricão Fisiol. Exerc. 2006, 3, 16–21. [Google Scholar]
- The Importance of Breathing in Pilates. Studio Pilates Internacional. Available online: https://www.studiopilates.com/the-importance-of-breathing-in-pilates (accessed on 23 May 2022).
- Kloubec, J. Pilates: How does it work and who needs it? Muscles Ligaments Tendons J. 2011, 1, 61–66. [Google Scholar]
- Chan, A.; Lee, A. Evaluation of the Sustaining Effects of Tai Chi Qigong in the Sixth Month in Promoting Psychosocial Health in COPD Patients: A Single-Blind, Randomized Controlled Trial. Sci. World J. 2013, 2013, 425082. [Google Scholar] [CrossRef]
- Tsang, H.W.H.; Mok, C.K. The effect of qigong on general and psychosocial health of elderly with chronic physical illness: A randomized clinical trial. Int. J. Geriatr. Psychiatry 2003, 18, 441–449. [Google Scholar] [CrossRef]
- Tsang, H.W.; Fung, K.M. Effect of a qigong exercise programme on elderly with depression. Int. J. Geriatr. Psychiatry 2006, 21, 890–897. [Google Scholar] [CrossRef]
- Yan, J.H.; Guo, Y. Effects of Tai Chi in patients with chronic obstructive pulmonary disease: Preliminary evidence. PLoS ONE 2013, 8, e61806. [Google Scholar] [CrossRef]
- Ries, A.L.; Kaplan, R.M. Maintenance after Pulmonary Rehabilitation in Chronic Lung Disease. A Randomized Trial. Am. J. Respir. Crit. Care Med. 2002, 167, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Allard, C.; Jones, N.L. Static peripheral skeletal muscle strength and exercise capacity in patients with chronic airflow limitation. Am. Rev. Respir. Dis. 1990, 139, A90. [Google Scholar]
- Gosselink, R.; Troosters, T. Peripheral muscle weakness contributes to exercise limitation in COPD. Am. J. Respir. Crit. Care Med. 1996, 153, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.L.; Killian, K.J. Muscle strength, symptom intensity, and exercise capacity in patients with cardiorespiratory disorders. Am. J. Respir. Crit. Care Med. 1995, 152, 2021–2031. [Google Scholar] [CrossRef] [PubMed]
- Serres, I.; Gautier, V. Impaired skeletal muscle endurance related to physical inactivity and altered lung function in COPD patients. Chest 1998, 113, 900–905. [Google Scholar] [CrossRef]
- Jakobsson, P.; Jorfeldt, L. Skeletal muscle metabolites and fibre types in patients with advanced chronic obstructive pulmonary disease (COPD), with and without chronic respiratory failure. Eur. Respir. J. 1990, 3, 192–196. [Google Scholar]
- Maltais, F.; Simard, A.A. Oxidative capacity of the skeletal muscle and lactic acid kinetics during exercise in normal subjects and in patients with COPD. Am. J. Respir. Crit. Care Med. 1996, 153, 288–293. [Google Scholar] [CrossRef]
- Wuyam, B.; Payen, J.F. Metabolism and aerobic capacity in chronic respiratory failure related to chronic obstructive pulmonary disease. Eur. Respir. J. 1992, 5, 157–162. [Google Scholar]
- Frontera, W.R.; Meredith, C.N. Strength conditioning in older men: Skeletal muscle hypertrophy and improved function. J. Appl. Physiol. 1985, 64, 1038–1044. [Google Scholar] [CrossRef]
- Killian, K.J.; Leblanc, P. Exercise capacity and ventilatory, circulatory, and symptom limitation in patients with airflow limitation. Am. Rev. Respir. Dis. 1992, 146, 935–940. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Characteristics | Population Characteristics | |||||||
|---|---|---|---|---|---|---|---|---|
| Study | Country | N | Age (y), Mean ± SD | Disease Severity | FEV1 % Pred | N Cases Failed Program | Groups by Intervention | N Intervention |
| Simpson et al., 1992 [32] | Canada | 34 | 73 ± 4.8 70 ± 5.7 | Severe COPD | 39.5 ±18.96 39.2 ± 21.39 | 3 3 | IG: COMB CG: CON | 14 14 |
| Bernard et al., 1999 [33] | Canada | 45 | 64 ± 7 67 ± 9 | Moderate to Severe | 45 ± 15 39 ± 12 | 5 4 | IG: COMB CG: PR | 21 15 |
| Spencer et al., 2010 [34] | Australia | 48 | 65 ± 8 67 ± 7 | COPD Moderate COPD | 57 ± 21 60 ± 16 | IG: PR+ HMPR CG: HMPR | 24 24 | |
| Nguyen et al., 2013 [35] | EEUU | 125 | 68.5 ± 11.0 68.2 ± 9.9 69.3 ± 8.0 | Moderate to severe COPD | 53.3 ± 20.4 50.6 ± 18.2 49.4 ± 19.8 | IG: HMPR IG: HMPR CG: CON | 43 41 41 | |
| Maltais et al., 2008 [36] | Canada | 252 | 66 ± 9 66 ± 9 | Severe COPD | 43± 13 46 ± 13 | IG: PR CG: HMPR | 126 126 | |
| Oh, 2003 [37] | Korea | 23 | 64.8 ± 7.84 66.8 ± 12.29 | Moderate to severe COPD | 42.12 ± 15.07 44.91 ± 17.75 | IG: HMPR CG: CON | 15 8 | |
| Donesky-Cuenco et al., 2009 [38] | EEUU | 29 | 72.2 ± 6.5 67.7 ± 11.5 | Moderate COPD | 72.2 ± 6.5 67.7 ± 11.5 | IG: AMBMT CG: CON | 14 15 | |
| Liu et al., 2012 [39] | China | 140 | 61.82 ± 7.69 61.34 ± 8.34 62.2 ± 6.34 | Moderate COPD | 74.43 ± 12.93 75.31 ± 12.84 75.31 ± 13.79 | IG: AMBMT IG: PR CG: CON | 51 32 35 | |
| Yeh et al., 2010 [40] | EEUU | 10 | 65 ± 6 66 ± 6 | Moderate to severe COPD | 53 ± 7 47 ± 7 | IG: AMBMT CG: CON | 5 5 | |
| Niu et al., 2014 [41] | China | 40 | 59.7 ± 2.76 61.3 ± 2.89 | Severe COPD | 41.9 ±5.50 43.7 ± 5.16 | IG: AMBMT CG: CON | 20 20 | |
| Gu et al., 2012 [42] | China | 66 | 67 ± 8 69 ± 9 | Moderate to severe COPD | 48.4 ± 18.7 51.6 ± 20.0 | 2 5 | IG: AMBMT CG: CON | 33 30 |
| Ng et al., 2014 [43] | China | 192 | 74.13 ± 6.81 74.16 ± 6.46 | Moderate to severe COPD | 64.1± 22.12 56.4 ± 23.81 | CG: PR IG: PR+AMBMT | 98 94 | |
| Chan et al., 2011 [44] | China | 206 | 71.7 ± 8.2 73.6 ± 7.5 73.6 ± 7.4 | Mild to severe COPD | 50.1 ± 21.8 56.4 ± 25.6 55.1 ± 23.3 | IG: AMBMT IG: HMPR CG: CON | 70 69 67 | |
| Gottlieb et al., 2011 [45] | Denmark | 42 | 74.1 ± 66–82 73.2 ± 67–88 | Moderate COPD | 64.27 ± 7.9 67.05 ± 8.8 | IG: PR CG: CON | 22 20 | |
| Román et al., 2013 [46] | Spain | 97 | 64.9 ± 62.1–67.7 64.1 ± 59.9–68.2 63.4 ± 60.4–66.4 | Moderate COPD | 60.9 ± 56.3–65.5 59.9 ± 54.9–64.8 60.1± 55.6–64.4 | 6 11 9 | IG: PR IG: PR CG: CON | 26 22 23 |
| Engstrom et al., 1999 [47] | Sweden | 55 (50) | 66.0 ± 5.4 66.8 ± 5.4 | Severe COPD | 30.7 ± 11.4 34.1± 10.2 | 2 3 | IG: PR CG: CON | 26 24 |
| Singh et al., 2003 [48] | India | 40 | 59.37 ± 6.4 59.37 ± 6.4 | Severe COPD | 28± 7.5 26 ± 7.1 | IG: PR CG: CON | 20 20 | |
| Borghi-Silva et al., 2009 [49] | EEUU | 34 | 67 ± 10 67 ± 10 | Severe COPD | 33± 9 35 ± 11 | IG: PR CG: CON | 20 14 | |
| Muñoz Fernández et al., 2009 [50] | Spain | 41 | 66 ± 8 70 ± 5 | Severe COPD | 33 ± 10 38 ± 12 | IG: HMPR CG: CON | 27 14 | |
| Theander et al., 2009 [51] | Sweden | 26 | 66 ± 6 64 ± 6 | Severe COPD | 35.1 ± 7.6 32.3 ± 9.5 | IG: PR CG: CON | 12 14 | |
| Ghanem et al., 2010 [52] | Egypt | 39 | 56.96 ± 11.59 56.43 ± 9.03 | Moderate to severe COPD | 29.44 ± 13.14 23.21 ± 7.70 | IG: HMPR CG: CON | 25 14 | |
| Pleguezuelos et al., 2013 [53] | Spain | 125 | 70.2 ± 2.5 70.5 ± 2.5 72.4 ± 1.7 | Severe or very severe COPD | 32.0 ± 1.2 31.8 ± 1.0 31.6 ± 0.8 | IG: PR+ URBAN IG: PR CG: CON | 34 37 54 | |
| De Sousa Pinto et al., 2014 [54] | Spain | 50 (41) | 68.9 ± 9.2 71.9 ± 7.6 | Severe or very severe COPD | 33.5 ± 7.3 34.5 ± 9.5 | 6 3 | IG: HMPR CG: CON | 23 18 |
| Chan et al. 1., 2013 [55] | China | 206 | 71.7 ± 8.2 73.6 ± 7.5 73.6 ± 7.4 | Mild to severe COPD | 50.1 ± 21.8 56.4 ± 25.6 55.1 ± 23.3 | IG: AMBMT IG: HMPR CG: CON | 70 69 67 | |
| Zhang et al., 2016 [56] | China | 130 | 64.77 ± 11.07 63.34 ± 7.86 62.35 ± 9.27 | 59.12 ± 4.13 57.39 ± 5.37 58.11 ± 4.37 | IG: AMBMT IG: HMPR CG: CON | 42 43 45 | ||
| Ranjita et al., 2016 [57] | India | 72 | 53.69 ± 5.66 54.41 ± 5.40 | Moderate COPD | 47.2–52.8 41.7–58.3 | 5 4 | IG: AMBMT CG: CON | 36 36 |
| Gupta et al., 2014 [58] | India | 50 | 52.5 ± 3.9 52 ± 4.1 | Moderate to severe COPD | 51.1 ± 8.7 49.6 ± 8.6 | IG: AMBMT CG: CON | 25 25 | |
| Xiao et al., 2015 [59] | China | 126 | 72.2 ± 1.7 70.9 ± 1.4 | Moderate to severe COPD | 41.5 ± 4.5 40.7 ± 4.0 | IG: AMBMT IG: HMPR | 63 63 | |
| Ng et al., 2011 [60] | China | 80 | 71.75 ± 1.05 73.12 ± 1.33 | Severe COPD | 37.13 ± 2.22 36.75 ± 2.11 | IG: AMBMT CG: CON | 40 40 | |
| Papp et al., 2017 [61] | Sweden | 36 | 61 ± 40–76 69 ± 43–84 | Mild to severe COPD | 67.6 ± 20.4 64.3 ± 15.4 | IG: AMBMT IG: COMB | 19 17 | |
| Daabis et al., 2016 [62] | Egypt | 45 | 58.7 ± 7 61 ± 8 60 ± 8 | Moderate COPD | 56.4 ± 8.3 53.2 ± 9.5 54.6 ± 7.1 | IG: COMB IG: END CG: CON | 15 15 15 | |
| Fukuoka et al., 2016 [63] | China | 8 | 74.6 ± 6.7 77.0 ± 7.0 | Moderate COPD | IG: PR+ AMBMT IG: PR | 5 3 | ||
| Hansen et al., 2019 [64] | Denmark | 134 | 68.4 ± 8.7 68.2 ± 9.4 | Severe COPD | 32.6 ± 10.3 33.7 ± 8.4 | IG: HMPR IG: PR | 67 67 | |
| Hagag et al., 2019 [65] | Egypt | 38 | 43.05 ± 2.07 42.09 ± 3.08 | Moderate COPD | 62.72 ± 3.34 63.59 ± 3.61 | IG: PILATES CG: CON | 19 19 | |
| Wen et al., 2020 [66] | China | 60 | 63.74 ± 3.24 64.10 ± 3.56 | IG: PR CG: CON | 30 30 | |||
| Kilic et al., 2021 [67] | Turkey | 58 | 68.4 ± 8.91 69.87 ± 10.46 | Mild to very severe COPD | 50.26 ± 19.08 57.52 ± 19.72 | IG: PR IG: HMPR | 27 31 | |
| Kantatong et al., 2019 [68] | Thailand | 50 | 69.68 ± 7.76 67.48 ± 10.17 | Mild to moderate COPD | 68.21 ± 21.63 68.37 ± 18.90 | IG: AMBMT CG: CON | 25 25 | |
| Babkina et al., 2017 [69] | Ukraine | 102 | 69.3 ± 5.6 67.2 ± 6.1 | IG: AMBMT CG: CON | 48 54 | |||
| Pradella et al., 2015 [70] | Brazil | 29 | 62.4 ± 10.7 65.3 ± 8 | Mild to very severe COPD | 62.4 ± 10.7 54 ± 26.2 | 3 3 | IG: HMPR CG: CON | 29 15 |
| Kraemer et al., 2021 [71] | EEUU | 92 | 68.6 ± 9.2 67.5 ± 7.7 | Moderate to severe COPD | 57.8 ± 14.3 59.6 ± 14.8 | IG: AMBMT CG: CON | 61 31 | |
| Barakat et al., 2008 [72] | France | 80 | 63.7 ± 11.9 65.9 ± 10.3 | Severe COPD | 41.9 ± 2.6 43.33 ± 3.6 | IG: PR CG: CON | 40 40 | |
| Study | Groups by Intervention | Intervention | Time (min)/rep | Intensity | Duration (wk) | Frequency (x/wk) |
|---|---|---|---|---|---|---|
| Simpson et al., 1992 [32] | IG: COMB | 5 min warm up of low resistance CYC + 2 min of low resistance arm exercise on AC + WLE single arm curl, single leg extension, and single leg press exercise. Normal breathing during the lifting phase of the exercise. | 3 series of 10 rep | 50% (1 week)–85% 1RM final | 8 | 3 |
| CG: CON | Usual medical care. | |||||
| Bernard et al., 1999 [33] | IG: COMB | Aerobic training + WLE: pectoralis major, elbow flexion, shoulder adduction (latissimus dorsi), leg press, and bilateral knee extension. | 30 min aerobic + 45 ST 2 series of 8/10 rep. Thereafter, it increased by more than 10 rep | Work rate 80% of peak work in incremental exercise test + 60% 1RM | 12 | 3 |
| CG: PR | Leg exercise on ergocycle + relaxation and breathing exercises. | 30 min + 45 relax and breathing | Work rate 80% of peak work in incremental exercise test | 12 | 3 | |
| Spencer et al., 2010 [34] | IG: PR+ HMPR | 1 day gym: Walk + SC + AC + LWM + AWM + UAE/HMPR: Walk + S, Sq, S/S, UAE. | 1 day gym: 20 min W + 2 min SC + 30 min AC, LWM, AWM, UAE. Total 70 min/HM PR: 30 min W + 30 min S, SQ, S/S, UAE. Total 60 min | 8 | 1 day gym + 4 HMPR | |
| CG: HMPR | HMPR: Walk + S, Sq, S/S, UAE. | HM PR: 30 min W + 30 min S, SQ, S/S, UAE. Total 60 min | 5 HMPR | |||
| Nguyen et al., 2013 [35] | IG: HMPR | Education and energy saving strategies + END (walk, CYC, swimming) + arm ST (biceps, triceps, side arm raises, and upper arm raises) program + self-monitoring of exercise and respiratory symptoms. Reinforcement emails, interactive web modules, live groups, and chat sessions. | END: 30 min + dyspnea and exercise consultation (1–1.5 h) + structured education (six 1 h sessions) | 12 months | END: 4/arm strengthening: 3 | |
| IG: HMPR | Education and energy saving strategies + END (walk, CYC, swimming) + arm ST (biceps, triceps, side arm raises, and upper arm raises) program + self-monitoring of exercise and respiratory symptoms. Reinforcement telephone calls (5–10 min), paper modules, and face-to-face groups sessions. | END: 30 min + dyspnea and exercise consultation (1–1.5 h) + structured education (six 1 h sessions) | END: 4/arm strengthening: 3 | |||
| CG: CON | Monthly face-to-face education classes (nutrition and general safety with medications). Weekly phone calls with health information. | 1 | ||||
| Maltais et al., 2008 [36] | IG: PR | END (CYC) + ST exercises. | END: 25–30 min + ST: 30 min, starting with 1 set of 10 rep e/e. Max 3 sets. Increased resistance (elastic bands, sandbags, and weight against gravity) | 80% peak work capacity during incremental exercise | 3 months (8 weeks (3 times a week) + 4 weeks education program) | 3 |
| CG: HMPR | END (CYC) + ST exercises + telephone calls to reinforce. | END: 40 min + ST: 30 min, starting with 1 set of 10 rep e/e. Max 3 sets. Increased resistance (elastic bands, sandbags, weight against gravity) | 60% max work rate achieved during a test of peak exercise capacity | 3 | ||
| Oh., 2003 [37] | IG: HMPR | Education + IMT + exercise training (stretching, walk, stair climbing, and ST of upper and lower limbs with a theraband) + psychosocial component (relaxation and telephone calls). | 5 min inspiration training each time (five times/day) + stretching 5 times/day (10 times each time) + relaxation technique (2/day) | 8 | Telephone visits: 2 | |
| CG: CON | Educational advice. | |||||
| Donesky-Cuenco et al., 2009 [38] | IG: AMBMT | Yoga asanas (stretching movements during exhalation) with breathing pranayama techniques + videotape of one yoga class to practice daily at home. | 1 h yoga sessions | 12 | 2 supervised + 7 at home | |
| CG: CON | Educational advice and were offered the yoga program at the conclusion of the 12 weeks period. | |||||
| Liu et al., 2012 [39] | IG: AMBMT | Health qigong training (selected routines). | 1 h | 6 months | 3 | |
| IG: PR | END (walk, CYC) + pursed-lip breathing + were encouraged to participate in peer-led weekly walking and ball game activities. | 1 h | 3 | |||
| CG: CON | Health education and were advised to continue exercising by themselves. | |||||
| Yeh et al., 2010 [40] | IG: AMBMT | Warm-up exercises (WLE+ arm swinging + gentle stretches of the neck, shoulders, spine, arms, and legs, visualization techniques, and traditional breathing methods) + 5 tai chi movements + 35 min instructional videotape with exercises to practice at home at least 3 times/week. | 1 h | 12 | 2 + 3 at home | |
| CG: CON | Usual medical care. | |||||
| Niu et al., 2014 [41] | IG: AMBMT | Warm-up + tai chi program + post-exercise relaxation + DVD developed for the home sessions. | 10 min warm up + 30 min tai chi + 10 min relaxation | Intensity was adjusted for each COPD patient according to her/his toleration of the program | 6 months | 4 + 3 at home |
| CG: CON | Usual medical care + lip breathing + walking daily. | 10–15 min lip breathing + 30 min walking daily | ||||
| Gu et al., 2012 [42] | IG: AMBMT | Educational sessions + simplified 24-style Taijiquan routines and their breathing method + weekly diary of physical activity measured with pedometers. | 60 min | 3 months | 3 | |
| CG: CON | Educational sessions + telephone monitoring once a month. | 2 h | ||||
| Ng et al., 2014 [43] | CG: PR | Warm-up + cooldown exercise + 2 END activities (TMW + lower limb ergometry exercise) + relaxation + HM PR exercises (warm-up + theraband exercises + aerobic exercises + cooldown + relaxation). | 5 min warm-up + 20 min each END exercise + 15 min rest between e/e + 5 min cooldown + 15 min relaxation + 1 h daily of unsupervised home exercises (5 min warm-up + 5 min of theraband exercises+ 30 min of aerobic exercises + 5 min cooldown + 15 min relaxation) | 6 | 2 (6 weeks) + after 5–7 at home | |
| IG: PR+ AMBMT | Warm-up + cooldown exercise + 2 END activities (TMW+ lower limb ergometry exercise) + tai chi (5 forms of Sun Style) + HM PR exercises (warm-up + theraband exercises + aerobic exercises + cooldown + tai chi). | 5 min warm-up + 20 min each END exercise + 15 min rest between e/e + 5 min cooldown + 15 min tai chi + 1 h daily of unsupervised home exercises (5 min warm-up + 5 min of theraband exercises + 30 min of aerobic exercises + 5 min cooldown + 15 min tai chi) | ||||
| Chan et al., 2011 [44] | IG: AMBMT | TCQ movements emphasized the elements of breathing + DVD to facilitate daily self-practice + diary for recording the frequency. | 60 min | 3-month | 2 + daily at home | |
| IG: HMPR | PLB + DB + self-paced walking + diary for recording the frequency. | daily at home | ||||
| CG: CON | Were advised to maintain routine activities. | |||||
| Gottlieb et al., 2011 [45] | IG: PR | Preliminary motivational personal interview + intensive physical training and educational phase supervised + final interview follows up. Training (END + static circuit training + walk + breathing techniques). Smoking cessation counseling + dietary intervention. | Physical training: 90 min sessions | Intensity of 16–17 Borg scale (20 point) | 7 + 6 months maintenance phase | Physical training: 2/Educational sessions: 1 |
| CG: CON | Standard community care. | |||||
| Román et al., 2013 [46] | IG: PR with maintenance group | Education program + respiratory physiotherapy (breathing + DB + exercises for the chest wall and abdominal muscle walls) + peripheral muscle training (abdominal and upper and lower limb exercises, shoulder, and full arm circling, WLE) + maintenance program. | 60 min (respiratory physiotherapy 15 min + 45 min exercises training. 8–10 rep e/e) + 45 min education session (weeks 1, 6 and 12) | Low-intensity peripheral muscle training | 3 months + 9 months maintenance phase | 3 + 1 (maintenance program) |
| IG: PR without maintenance group | Education program+ respiratory physiotherapy (breathing + DB + exercises for the chest wall and abdominal muscle walls) + peripheral muscle training (abdominal and upper and lower limb exercises, shoulder, and full arm circling, WLE) + routine care after completing the 3 months PR. | 3 months | 3 | |||
| CG: CON | Continue their routine care. | 3 months | ||||
| Engstrom et al., 1999 [47] | IG: PR with maintenance group | CYC + arm training + training in breathing techniques (PLB+ DB). | 45 min (first 15 min breathing techniques) + 30 min CYC +30 min HMPR daily: thorax and shoulder-girdle training + muscle ST (theraband) + energy saving techniques (2 sessions) + nutrition advise + educational sessions (2) | 42–85% W max at 2 min intervals after 5 min warming up at 50% of W max. These 2 min intervals (42–85%) were repeated for 25 min at most. Borg score of 15 (hard) for “effort” + 30 min HMPR | 12 months | 2 (6 weeks) + 1 (6 weeks) + once every second week (6 weeks) + 1 a month for the remaining period + HMPR daily |
| CG: CON | Usual outpatient care. | |||||
| Singh et al., 2003 [48] | IG: PR | Breathing (PLB + DB + controlled coughing + postural bronchial drainage) + lower extremity exercise (walk + PLB) + energy conservation techniques. | 30 min twice a day | Walk submaximal speed (twice a day) + PR 30 min (twice a day) | 4 | twice daily |
| CG: CON | ||||||
| Borghi-Silva et al., 2009 [49] | IG: PR | Aerobic training (ST lower and upper limbs + TMW) + stretching exercises + DB (hamstrings, quadriceps, calves, shoulders, neck, and lower back). | 30 min aerobic + 10 min stretching | Training intensity in TMW: 70% max speed achieved during the exercise test | 6 | 3 |
| CG: CON | Vibration and clapping associated with postural drainage for 10 min with supported cough. | 10 min | ||||
| Muñoz Fernández et al., 2009 [50] | IG: HMPR | Respiratory reeducation + IMT + ST upper limbs (initially isotonic exercises without weights + after WLE) + ST lower limbs (initially isotonic exercises after with resistance + walk). | 1 h (15 min respiratory reeducation) + 15 min IMT + 30 min muscular training of upper limbs + 30 min walk | IMT (70% PIM) + Walk (90% velocity reached in the 6 MWT) | 12 months | 5 |
| CG: CON | 3 respiratory education sessions. | |||||
| Theander et al., 2009 [51] | IG: PR | CYC + ST (biceps, latissimus dorsi, and quadriceps) stand-ups, toe raises, step-ups, pelvic-lifts, and sit-ups + after 1 month intervention included home program (daily walk +ST-theraband+ diet education + energy saving techniques + educational advice). | 1 h (15 min CYC + ST 10 exercises in 3 rounds per occasion) | 12 | 2 | |
| CG: CON | ||||||
| Ghanem et al., 2010 [52] | IG: HMPR | Health education + exercise training (PLB + DB) + END (CYC + Walk) + ST (upper extremity. Six to 10 upper-body and lower-body ST exercises) + stretching (hamstrings, quadriceps, calves, shoulders, neck, and lower back). | 2 months | every other day | ||
| CG: CON | Usual care. | |||||
| Pleguezuelos et al., 2013 [53] | IG: PR+ URBAN | Warm-up exercises (upper and lower limbs and spine) + END (CYC) + ST (upper limbs muscles) + stretching exercises + relax + urban walking circuits. | 10 min warm-up+ 25 min CYC + 15 min ST + 10 min stretching+ 10 relax + PR URBAN | Moderate intensity Initial intensity of training 50 W, increasing progressively with tolerance | 12 | 3 |
| IG: PR | Warm-up exercises (upper and lower limbs and spine) + END (CYC) + ST (upper limbs muscles) + stretching exercises + relax. | 10 min warm-up+ 25 min CYC + 15 min ST + 10 min stretching+ 10 relax | Moderate intensity Initial intensity of training 50 W, increasing progressively with tolerance | |||
| CG: CON | ||||||
| De Sousa Pinto et al., 2014 [54] | IG: HMPR | Breathing and stretching exercises + ST (upper and lower limbs) + END (walk, stair climbing, CYC, and TMW) + WLE. | Initially, 20–30 min, increased to 1 h. Upper and lower limbs exercises (2 sets of 10 reps e/e without weights to 2 sets of 10 reps with 2 kg weight max for both hands and legs). 3–5 min stair climbing, From 5–10 min to 30 min TMW or CYC. Patients without treadmills or bicycles, walked daily for at least 30 min | Training intensity was adjusted according to the level of dyspnea, dizziness, or leg discomfort | 3 months | First 2 weeks (2 visits per week), after twice a month and weekly telephone) |
| CG: CON | ||||||
| Chan et al., 2013 [55] | IG: AMBMT | TCQ movements emphasized the elements of breathing supervised + DVD to facilitate daily self-practice + diary for recording the frequency. | 60 min | Were allowed to adjust the position of their extremities and the exercise intensity according to their physical condition | 3-month | 2+ daily at home |
| IG: HMPR | PLB+DB+self-paced walking +diary for recording the frequency. | daily at home | ||||
| CG: CON | ||||||
| Zhang et al., 2016 [56] | IG: AMBMT | QYJJ supervised coordinate breathing with movements + DVD + pictures to facilitate individual practice + group meeting once a week to share experiences. | 60 min | 6 months | 3 group practise + 4 individual practice | |
| IG: HMPR | Self-pace Walk + DB + PLB + keep a diary to record the frequency. | 60 min | 7 | |||
| CG: CON | Were advised to maintain their routine activities without any extra recommended exercise. | |||||
| Ranjita et al., 2016 [57] | IG: AMBMT | Yoga asanas supervised + pranayamas (breathing practices). Deeply relax different muscle groups + slow breathing practices + strengthen respiratory muscles + calm mind + balance emotions + develop internal awareness. | 90 min | 12 | 6 | |
| CG: CON | Were offered the 12 weeks yoga program after the intervention period and post-testing were complete. | |||||
| Gupta et al., 2014 [58] | IG: AMBMT | Yoga asanas supervised (4 easy asanas) pranayam + usual medical care. | 30 min pranayam (5–7 min each asana) (2 x/d) | Low-intensity max heart ranges from 43% to 49% of predicted max | 3 months | 7 (twice per day) |
| CG: CON | Usual medical care. | |||||
| Xiao et al., 2015 [59] | IG: AMBMT | LQG training supervised sessions (six distinct movement routines) coordinate their breathing + audiovisual material + advised to walk daily. | 45 min. 6 routines/six times each routine. 12–15 min + 30 min walk daily | Low-intensity CYC and ST. ST. Intensity 70% 1RM + CYC (12–14 on Borg 20-scale- 50–60 rpm) | 6 months | 4 |
| IG: HMPR | PLB + coordinated breathing + walking exercise program + advised to walk daily. | 45 min training + 30 min walk daily | 4 | |||
| Ng et al., 2011 [60] | IG: AMBMT | HQG sessions supervised + package audiovisual materials (8 distint routines). | 45 min. 8 distinct movement routines repeated six times. 12–15 min | 6 months | 4 | |
| CG: CON | Breathing (PLB + coordinated breathing) + walk. Advised to keep daily walking for not less than 30 min. | 45 min | 4 | |||
| Papp et al., 2017 [61] | IG: AMBMT | Hatha yoga program supervised + DVD and paper + physical activity after the intervention. | 60–70 min | 75% of the results of 6 MWT + low-intensity resistance training with free weights. | 12 | 2 |
| IG: COMB | CYC + ST training (with gym equipment and stationary exercise bikes). | 60–70 min. ST: 2–4 sets of 10–20 rep e/e. Total 10–12 exercises+ 10–15 min CYC | Workload at 50–80% 1RM. 1RM repeated every 2 weeks to re-establish the workload | 2 | ||
| Daabis et al., 2016 [62] | IG: COMB | TMW + WLE | 60 min: 30 min TMW+ 30 min WLE + pacing for breathing | 8 | 3 | |
| IG: END | ST (weight training machines (pectoralis major, deltoids, biceps brachii, triceps and quadriceps muscles)). | 60 min: 30 min ST. 3 sets of 12 reps with a 2 min rest between sets + 30 min (15 walk + 15 at half the number of reps of low-intensity resistance training with free weights) + pacing for breathing | 3 | |||
| CG: CON | Medical only. | |||||
| Fukuoka et al., 2016 [63] | IG: PR+ AMBMT | Exercise training, educational programs (5 education sessions), lung physiotherapy, and nutrition counseling + laughter yoga (deep breathing + hand clapping + laughter activities + cool down by deep breathing. | Exercise training + 10 min laughter yoga | Low to medium intensity | 2 | |
| IG: PR | Exercise training, educational programs (5 education sessions), lung physiotherapy, and nutrition counseling. | |||||
| Hansen et al., 2019 [64] | IG: HMPR | Pulmonary telerehabilitation: supervised program (warm-up + END training + education session. | Weekly exercise volume 105 min (35 min exercise sessions + 5 min rest before beginning education session of 20 min (weekly education volume 60 min) | 10 | 2 | |
| IG: PR | Exercise training (warm-up + END + resistance training + cooldown) + education sessions. | Weekly exercise volume 120 min + Education sessions lasted 60 to 90 min | 10. In one hospital (12) | 2 | ||
| Hagag et al., 2019 [65] | IG: PILATES | Pilates exercises: Warm-up (breathing, arm circles, hip rolls) + pilates phase (5 types of exercise) + cooldown (stretching) | 7–10 min warm up + 40 min pilates (5 types of exercises, 7–8 min e/e) + 7–10 min cool-down | Warm-up: 9–11 Borg scale. Pilates phase: moderate intensity at 12–14 Borg scale + Cool down phase: 9–11 Borg scale (20) | 12 | 3 |
| CG: CON | DB. | DB: 2 sets for 5 reps with rest intervals of 5–6 tidal breaths between exercises | 12 | 3 | ||
| Wen et al., 2020 [66] | IG: PR | END (CYC) + breathing (DB, PLB, chest breathing exercise, relaxation, cough training, and resistance breath training + walk + stair training + horizontal bar training. | CYC (medium speed, rest for 1 min after every 4 min of exercise, 15 min/day) + 15 min/day breathing exercises + 500 m walk (twice daily) + 10 min (twice daily) 5-step stair + 15 min (twice daily) horizontal bar training | 4 | twice daily | |
| CG: CON | ||||||
| Kilic et al., 2021 [67] | IG: PR | Warm-up + ST upper and lower extremities + DB + stretches + cooldown + booklet and CD. | 45 min exercise + 15 min of rest in each session. 10 min warm + 20 min ST exercises (10 times e/e) + 5 min DB (10 times e/e) + stretches (10 s e/e) + 10 min cooldown | 12 | 3 | |
| IG: HMPR | ST + respiratory exercises + CD and training booklet for learning reinforcement + checked by the researcher via phone. | 45 min home exercises | 3 | |||
| Kantatong et al., 2019 [68] | IG: AMBMT | TCQ programme: 8 forms modified 3 times a week in the center-based programme led by a TCQ instructor + 2 days practise at home + poster to simplify self-practise at home. | Full breathing in supine or sitting position 4 times/day, 8–10 breaths at a time; increased the number of rounds up to 10 per day and performed it while sitting, standing, or walking | 24 (12 at center + 12 at home) | 3 at center + 2 at home | |
| CG: CON | Usual care without another intervention. | |||||
| Babkina et al., 2017 [69] | IG: AMBMT | Full yogic breathing intervention (deep, slow breathing: abdominal, thoracic, and clavicular) + diaries. | ||||
| CG: CON | Usual care. | |||||
| Pradella et al., 2015 [70] | IG: HMPR | A week at the rehabilitation center learning the exercises and received printed material (educational booklet) with exercises to be performed (warm-up, aerobic activity, stretching, and relaxation) + received a log to record their activities + weekly telephone calls. | Warm-up included five 1 min exercises with a 1 min rest interval between exercises. Walk 40 min along a corridor or a street, climbing stairs 15 min, and exercising the arms with an oil can (1 kg) using diagonal movements for 15 min | Heart rate of 60–70% of MHR | 8 | 3 |
| CG: CON | Weekly telephone calls. | |||||
| Kraemer et al., 2021 [71] | IG: AMBMT | Five core TCQ movements + four mind–body breathing techniques were integrated throughout the interventions + tai chi warm-up and cool-down exercises (1 h) + practice at home 3 times/week 30 min + 45 min DVD and audio file to encourage this home practice. | 2 times/week 1 h + 3 times/week 30 min at home | 12 + 12 | 2 + 1 s 12 weeks + 3 at home | |
| CG: CON | Four mind–body breathing techniques + mindful awareness of breath was emphasized in each of the techniques (1 h). Were also encouraged to practice at home three additional times per week for 30 min + 45-min DVD and audio files to facilitate home practice. | 2 times/week 1 h + 3 times/week 30 min at home | 12 | 2 + 3 at home | ||
| Barakat et al.,2008 [72] | IG: PR | PR: 30 min education and exercises (5 min warm-up + 10 min aerobic activity: diagonal arm raises, arm abd into elevation and reverse, arm abd, forward flexion, and reverse and straight leg rises) + 15 min cooldown) + 30 min cycling + dietary assessment and advice. | 3 times/week 1 h | 25 watts and increased the intensity by 5 watts each week until 40 watts. The aim was to reach the 80% of VO2 max of each patient | 14 | 3 |
| CG: CON | Usual medical care. |
| CONTROL | 0.59 (0.31, 0.88) | 0.54 (−0.13, 1.21) | 0.86 (0.11, 1.61) | 0.51 (0.19, 0.83) | 1.97 (1.20, 2.75) | 0.56 (0.24, 0.88) | NA | NA | 1.10 (0.64, 1.56) |
| 0.96 (0.61, 1.31) | AMBMT | −0.14 (−1.46,1.19) | NA | 0.69 (0.12, 1.27) | NA | 0.06 (−0.38, 0.50) | NA | NA | NA |
| 0.90 (0.07, 1.74) | −0.06 (−0.94, 0.82) | COMB | 0.07 (−0.65, 0.79) | NA | NA | 0.22 (−0.44, 0.89) | NA | NA | NA |
| 1.04 (−0.22, 2.29) | 0.07 (−1.22, 1.37) | 0.13 (−1.13, 1.40) | END | NA | NA | NA | NA | NA | NA |
| 0.55 (0.17, 0.92) | −0.42 (−0.86, 0.02) | −0.36 (−1.26, 0.54) | −0.49 (−1.80, 0.81) | HM PR | NA | 0.08 (−0.11, 0.26) | NA | 0.02 (−0.54, 0.59) | NA |
| 1.32 (0.18, 2.45) | 0.35 (−0.84, 1.54) | 0.41 (−1.00, 1.82) | 0.28 (−1.42, 1.97) | 0.77 (−0.43, 1.97) | PILATES | NA | NA | NA | NA |
| 0.91 (0.52, 1.31) | −0.05 (−0.55, 0.45) | 0.01 (−0.87, 0.89) | −0.12 (−1.43, 1.18) | 0.37 (−0.11, 0.85) | −0.40 (−1.61, 0.80) | PR | 0.06 (−0.22, 0.33) | NA | 0.24 (−0.23, 0.70) |
| 0.81 (−0.43, 2.06) | −0.15 (−1.43, 1.13) | −0.09 (−1.56, 1.38) | −0.22 (−1.98, 1.54) | 0.27 (−1.01, 1.55) | −0.50 (−2.19, 1.19) | −0.10 (−1.28, 1.08) | PR + AMBMT | NA | NA |
| 0.44 (−1.13, 2.01) | −0.52 (−2.11, 1.07) | −0.46 (−2.23, 1.31) | −0.59 (−2.60, 1.42) | −0.10 (−1.63, 1.42) | −0.87 (−2.81, 1.07) | −0.47 (−2.07, 1.13) | −0.37 (−2.36, 1.62) | PR + HM PR | NA |
| 1.50 (0.46, 2.55) | 0.54 (−0.55, 1.63) | 0.60 (−0.72, 1.92) | 0.47 (−1.16, 2.09) | 0.96 (−0.13, 2.05) | 0.19 (−1.36, 1.73) | 0.59 (−0.46, 1.63) | 0.69 (−0.89, 2.27) | 1.06 (−0.82, 2.94) | PR + URBAN |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priego-Jiménez, S.; Torres-Costoso, A.; Guzmán-Pavón, M.J.; Lorenzo-García, P.; Lucerón-Lucas-Torres, M.I.; Álvarez-Bueno, C. Efficacy of Different Types of Physical Activity Interventions on Exercise Capacity in Patients with Chronic Obstructive Pulmonary Disease (COPD): A Network Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14539. https://doi.org/10.3390/ijerph192114539
Priego-Jiménez S, Torres-Costoso A, Guzmán-Pavón MJ, Lorenzo-García P, Lucerón-Lucas-Torres MI, Álvarez-Bueno C. Efficacy of Different Types of Physical Activity Interventions on Exercise Capacity in Patients with Chronic Obstructive Pulmonary Disease (COPD): A Network Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(21):14539. https://doi.org/10.3390/ijerph192114539
Chicago/Turabian StylePriego-Jiménez, Susana, Ana Torres-Costoso, María José Guzmán-Pavón, Patricia Lorenzo-García, María Isabel Lucerón-Lucas-Torres, and Celia Álvarez-Bueno. 2022. "Efficacy of Different Types of Physical Activity Interventions on Exercise Capacity in Patients with Chronic Obstructive Pulmonary Disease (COPD): A Network Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 21: 14539. https://doi.org/10.3390/ijerph192114539
APA StylePriego-Jiménez, S., Torres-Costoso, A., Guzmán-Pavón, M. J., Lorenzo-García, P., Lucerón-Lucas-Torres, M. I., & Álvarez-Bueno, C. (2022). Efficacy of Different Types of Physical Activity Interventions on Exercise Capacity in Patients with Chronic Obstructive Pulmonary Disease (COPD): A Network Meta-Analysis. International Journal of Environmental Research and Public Health, 19(21), 14539. https://doi.org/10.3390/ijerph192114539