

A Depression-Risk Mental Pattern Identified by Hidden Markov Model in Undergraduates


Abstract
1. Introduction
1.1. Factors Associated with Depression
1.2. The Emergency of Depression Risk Screening
1.3. The Present Study
2. Materials and Methods
2.1. Participant
2.2. Measurement
2.2.1. Center for Epidemiological Studies Depression Scale (CES-D)
2.2.2. Subjective Well-Being Questionnaire (SWB)
2.2.3. Ways of Coping Questionnaire (WCQ)
2.2.4. Emotion Regulation Questionnaire (ERQ)
2.3. Data Analysis
2.3.1. Correlation
2.3.2. Regression
2.3.3. Pattern Recognition by Hidden Markov Model (HMM)
3. Results
3.1. Descriptive Statistics and Correlation
3.2. Regression
3.3. Pattern Recognition by HMM
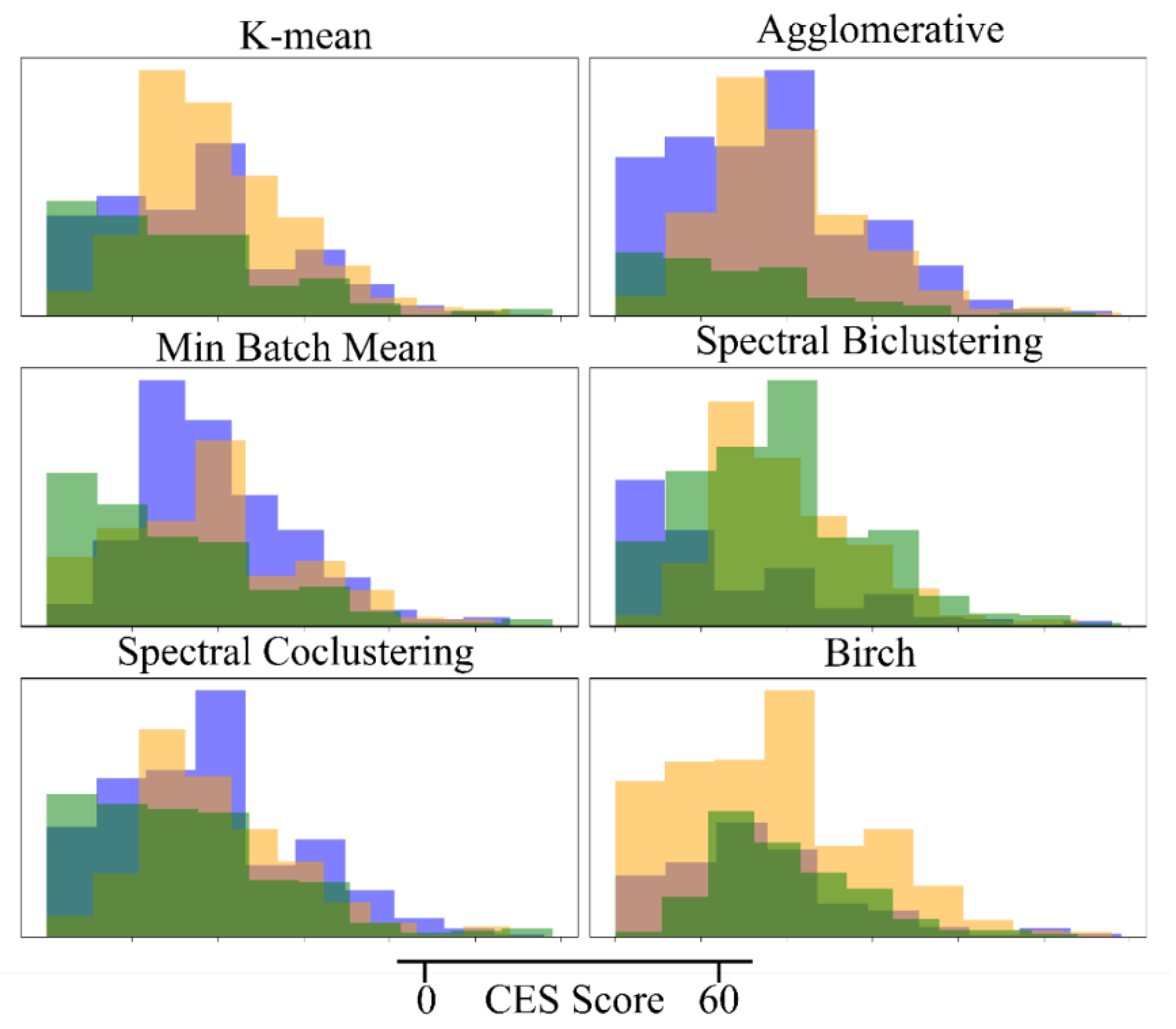
3.4. Comparison with Other Unsupervised Clustering Models
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anders, S.L.; Frazier, P.A.; Shallcross, S.L. Prevalence and Effects of Life Event Exposure among Undergraduate and Community College Students. J. Couns. Psychol. 2012, 59, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Lei, X.-Y.; Xiao, L.-M.; Liu, Y.-N.; Li, Y.-M. Prevalence of Depression among Chinese University Students: A Meta-Analysis. PLoS ONE 2016, 11, e0153454. [Google Scholar] [CrossRef] [PubMed]
- Mirza, A.A.; Baig, M.; Beyari, G.M.; Halawani, M.A.; Mirza, A.A. Depression and Anxiety Among Medical Students: A Brief Overview. AMEP 2021, 12, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Zhang, N.; Liu, J.; Zhu, B.; He, R.; Wang, X. A Systematic Review of Depression and Anxiety in Medical Students in China. BMC Med. Educ. 2019, 19, 327. [Google Scholar] [CrossRef]
- Joormann, J.; Gotlib, I.H. Emotion Regulation in Depression: Relation to Cognitive Inhibition. Cogn. Emot. 2010, 24, 281–298. [Google Scholar] [CrossRef]
- Broderick, P.C.; Korteland, C. Coping Style and Depression in Early Adolescence: Relationships to Gender, Gender Role, and Implicit Beliefs. Sex Roles 2002, 46, 201–213. [Google Scholar] [CrossRef]
- Ehring, T.; Tuschen-Caffier, B.; Schnülle, J.; Fischer, S.; Gross, J.J. Emotion Regulation and Vulnerability to Depression: Spontaneous versus Instructed Use of Emotion Suppression and Reappraisal. Emotion 2010, 10, 563–572. [Google Scholar] [CrossRef]
- Kedare, J.; Singh, D. A Study of Depression in Medically Ill Elderly Patients with Respect to Coping Strategies and Spirituality as a Way of Coping. J. Geriatr. Ment. Health 2014, 1, 83. [Google Scholar] [CrossRef]
- Oxman, T.E.; Hegel, M.T.; Hull, J.G.; Dietrich, A.J. Problem-Solving Treatment and Coping Styles in Primary Care for Minor Depression. J. Consult. Clin. Psychol. 2008, 76, 933–943. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective Well-Being: Three Decades of Progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Malone, C.; Wachholtz, A. The Relationship of Anxiety and Depression to Subjective Well-Being in a Mainland Chinese Sample. J. Relig. Health 2018, 57, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, C.W.; Hankin, B.L. Relationship Quality and Depressive Symptoms Among Adolescents: A Short-Term Multiwave Investigation of Longitudinal, Reciprocal Associations. J. Clin. Child Adolesc. Psychol. 2011, 40, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Fröjd, S.A.; Nissinen, E.S.; Pelkonen, M.U.I.; Marttunen, M.J.; Koivisto, A.-M.; Kaltiala-Heino, R. Depression and School Performance in Middle Adolescent Boys and Girls. J. Adolesc. 2008, 31, 485–498. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, C.; Batejan, K.; Kleinman, M.; Gould, M. Reasons for Attempting Suicide among a Community Sample of Adolescents. Suicide Life Threat. Behav. 2013, 43, 646–662. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.E.; Kessler, R.C.; Birnbaum, H.G.; Leong, S.A.; Lowe, S.W.; Berglund, P.A.; Corey-Lisle, P.K. The Economic Burden of Depression in the United States: How Did It Change Between 1990 and 2000? J. Clin. Psychiatry 2003, 64, 1465–1475. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.L.; Vos, T.; Whiteford, H.A. Burden of Depressive Disorders by Country, Sex, Age, and Year: Findings from the Global Burden of Disease Study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef]
- Gwynn, R.C.; McQuistion, H.L.; McVeigh, K.H.; Garg, R.K.; Frieden, T.R.; Thorpe, L.E. Prevalence, Diagnosis, and Treatment of Depression and Generalized Anxiety Disorder in a Diverse Urban Community. Psychiatr. Serv. 2008, 59, 641–647. [Google Scholar] [CrossRef]
- Yang, F.; Yang, B.X.; Stone, T.E.; Wang, X.Q.; Zhou, Y.; Zhang, J.; Jiao, S.F. Stigma towards Depression in a Community-Based Sample in China. Compr. Psychiatry 2020, 97, 152152. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, R.P. National Survey of College Counseling Centers 2013, Section One: 4-Year Directors; The International Association of Counseling Services (IACS): Alexandria, VT, USA, 2014. [Google Scholar]
- Takagaki, K.; Okamoto, Y.; Jinnin, R.; Mori, A.; Nishiyama, Y.; Yamamura, T.; Yokoyama, S.; Shiota, S.; Okamoto, Y.; Miyake, Y.; et al. Behavioral Activation for Late Adolescents with Subthreshold Depression: A Randomized Controlled Trial. Eur. Child Adolesc. Psychiatry 2016, 25, 1171–1182. [Google Scholar] [CrossRef]
- Yamamoto, A.; Tsujimoto, E.; Taketani, R.; Tsujii, N.; Shirakawa, O.; Ono, H. The Effect of Interpersonal Counseling for Subthreshold Depression in Undergraduates: An Exploratory Randomized Controlled Trial. Depress. Res. Treat. 2018, 2018, 4201897. [Google Scholar] [CrossRef]
- MacDonald, I.L.; Zucchini, W. Hidden Markov and Other Models for Discrete-Valued Time Series, 1st ed.; Monographs on statistics and applied probabilit; Chapman & Hall: London, UK; New York, NY, USA, 1997; ISBN 978-0-412-55850-4. [Google Scholar]
- Mendes, E. Introduction to Bayesian Networks. In Practitioner’s Knowledge Representation; Springer: Berlin/Heidelberg, Germany, 2014; pp. 61–71. ISBN 978-3-642-54156-8. [Google Scholar]
- Zhou, Z.H. Machine Learning; Tsinghua University Press: Beijing, China, 2016; Volume 4, ISBN 978-7-302-42328-7. [Google Scholar]
- Polani, D. Probabilistic Graphical Model. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.-H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013; p. 1748. ISBN 978-1-4419-9862-0. [Google Scholar]
- Koller, D.; Friedman, N. Probabilistic Graphical Models: Principles and Techniques; Adaptive Computation and Machine Learning; MIT Press: Cambridge, MA, USA, 2009; ISBN 978-0-262-01319-2. [Google Scholar]
- Rabiner, L.R. A Tutorial on Hidden Markov Models and Selected Applications in Speech Recognition. Proc. IEEE 1989, 77, 257–286. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, Z.Y.; Fang, G.; Li, J.; Han, B.X.; Chen, Z.Y. Development of the Chinese Age Norms of CES-D in Urban Area. Chin. Ment. Health J. 2010, 24, 139–143. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and Validation of Brief Measures of Positive and Negative Affect: The PANAS Scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Larsen, R.J.; Diener, E.; Emmons, R.A. An Evaluation of Subjective Well-Being Measures. Soc. Indic. Res. 1985, 17, 1–17. [Google Scholar] [CrossRef]
- Huang, L.; Yang, T.; Ji, Z. Applicability of the Positive and Negative Affect Scale in Chinese. Chin. Ment. Health J. 2003, 17, 54–56. [Google Scholar]
- Xiong, C.; Xu, Y. Reliability and Validity of the Chinese Version of the Life Satisfaction Scale in the Public. China J. Health Psychol. 2009, 17, 948–949. [Google Scholar]
- Folkman, S.; Lazarus, R.S. If It Changes It Must Be a Process: Study of Emotion and Coping during Three Stages of a College Examination. J. Pers. Soc. Psychol. 1985, 48, 150–170. [Google Scholar] [CrossRef]
- Xie, Y.N. A Preliminary Study of the Reliability and Validity of the Simplified Coping Style Questionnaire. Chin. J. Clin. Psychol. 1998, 6, 114–115. [Google Scholar]
- Wang, L.; Liu, H.C.; Li, Z.Q.; Du, W. Reliability and Validity of Emotion Regulation Questionnaire Chinese Revised Version. China J. Health Psychol. 2007, 15, 503–505. [Google Scholar]
- Gross, J.J.; John, O.P. Individual Differences in Two Emotion Regulation Processes: Implications for Affect, Relationships, and Well-Being. J. Pers. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Dunlap, W.P.; Kemery, E.R. Failure to Detect Moderating Effects: Is Multicollinearity the Problem? Psychol. Bull. 1987, 102, 418–420. [Google Scholar] [CrossRef]
- Kim, J.H. Multicollinearity and Misleading Statistical Results. Korean J. Anesthesiol. 2019, 72, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, F.; Farcomeni, A.; Pennoni, F. Latent Markov Models for Longitudinal Data; Chapman & Hall/CRC Statistics in the Social and Behavioral Sciences; CRC Press, Taylor & Francis Group: Boca Raton, FL, USA, 2013; ISBN 978-1-4398-1708-7. [Google Scholar]
- Vidaurre, D.; Quinn, A.J.; Baker, A.P.; Dupret, D.; Tejero-Cantero, A.; Woolrich, M.W. Spectrally Resolved Fast Transient Brain States in Electrophysiological Data. NeuroImage 2016, 126, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Vidaurre, D.; Myers, N.E.; Stokes, M.; Nobre, A.C.; Woolrich, M.W. Temporally Unconstrained Decoding Reveals Consistent but Time-Varying Stages of Stimulus Processing. Cereb. Cortex 2019, 29, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Vidaurre, D.; Abeysuriya, R.; Becker, R.; Quinn, A.J.; Alfaro-Almagro, F.; Smith, S.M.; Woolrich, M.W. Discovering Dynamic Brain Networks from Big Data in Rest and Task. NeuroImage 2018, 180, 646–656. [Google Scholar] [CrossRef]
- Vidaurre, D.; Smith, S.M.; Woolrich, M.W. Brain Network Dynamics Are Hierarchically Organized in Time. Proc. Natl. Acad. Sci. USA 2017, 114, 12827–12832. [Google Scholar] [CrossRef] [PubMed]
- Quinn, A.J.; Vidaurre, D.; Abeysuriya, R.; Becker, R.; Nobre, A.C.; Woolrich, M.W. Task-Evoked Dynamic Network Analysis Through Hidden Markov Modeling. Front. Neurosci. 2018, 12, 603. [Google Scholar] [CrossRef]
- Nelson, J.; Klumparendt, A.; Doebler, P.; Ehring, T. Everyday Emotional Dynamics in Major Depression. Emotion 2020, 20, 179–191. [Google Scholar] [CrossRef]
- Vanderlind, W.M.; Millgram, Y.; Baskin-Sommers, A.R.; Clark, M.S.; Joormann, J. Understanding Positive Emotion Deficits in Depression: From Emotion Preferences to Emotion Regulation. Clin. Psychol. Rev. 2020, 76, 101826. [Google Scholar] [CrossRef]
- Teasdale, J.D. Cognitive Vulnerability to Persistent Depression. Cogn. Emot. 1988, 2, 247–274. [Google Scholar] [CrossRef]
- Eisenberg, D.; Downs, M.F.; Golberstein, E.; Zivin, K. Stigma and Help Seeking for Mental Health Among College Students. Med. Care Res. Rev. 2009, 66, 522–541. [Google Scholar] [CrossRef] [PubMed]
- Vidourek, R.A.; King, K.A.; Nabors, L.A.; Merianos, A.L. Students’ Benefits and Barriers to Mental Health Help-Seeking. Health Psychol. Behav. Med. 2014, 2, 1009–1022. [Google Scholar] [CrossRef] [PubMed]
- Wimsatt, L.A.; Schwenk, T.L.; Sen, A. Predictors of Depression Stigma in Medical Students. Am. J. Prev. Med. 2015, 49, 703–714. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Items | n | % |
|---|---|---|---|
| Gender | Male | 480 | 42.55 |
| Female | 720 | 63.83 | |
| Age | Mean (std) = 19.86 (1.31) | ||
| Number of siblings | 0 | 670 | 59.40 |
| 1 | 281 | 24.91 | |
| 2 | 177 | 15.69 | |
| Place of residence | City | 490 | 43.44 |
| Town | 638 | 56.56 | |
| Education of Father | Primary School | 194 | 17.20 |
| Middle School | 444 | 39.36 | |
| High School | 274 | 24.29 | |
| Undergraduate | 489 | 43.35 | |
| Graduate | 27 | 2.39 | |
| Education of Mother | Primary School | 300 | 26.60 |
| Middle School | 433 | 38.39 | |
| High School | 234 | 20.74 | |
| Undergraduate | 144 | 12.77 | |
| Graduate | 17 | 1.51 |
| All | Var | M (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | CES | 18.000 (10.58) | — | |||||||
| 2 | PC | 2.943 (0.50) | −0.024 | — | ||||||
| 3 | NC | 2.270 (0.51) | −0.050 | 0.142 *** | — | |||||
| 4 | PA | 29.016 (7.60) | −0.223 *** | 0.439 *** | 0.115 *** | — | ||||
| 5 | NA | 22.879 (7.72) | −0.240 *** | −0.172 *** | 0.247 *** | 0.234 *** | — | |||
| 6 | LS | 17.211 (5.74) | 0.033 | 0.346 *** | 0.030 | 0.397 *** | −0.231 *** | — | ||
| 7 | CR | 22.188 (3.74) | 0.020 | 0.477 *** | 0.016 | 0.269 *** | −0.175 *** | 0.286 *** | — | |
| 8 | ES | 11.326 (3.07) | 0.009 | −0.181 *** | 0.087 ** | −0.126 *** | 0.111 *** | −0.095 ** | 0.010 | — |
| Low-depression-risk group | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
| 1 | CES | 4.868 (2.78) | — | |||||||
| 2 | PC | 2.99 (0.50) | −0.050 | — | ||||||
| 3 | NC | 2.339 (0.53) | −0.082 | 0.099 | — | |||||
| 4 | PA | 35.23 (7.53) | −0.112 | 0.396 **** | 0.141 * | — | ||||
| 5 | NA | 28.128 (8.76) | −0.171 ** | −0.170 ** | 0.228 *** | 0.207 ** | — | |||
| 6 | LS | 17.811 (5.61) | 0.010 | 0.342 *** | 0.073 | 0.397 *** | −0.250 *** | — | ||
| 7 | CR | 22.037 (3.88) | 0.128 * | 0.450 *** | −0.105 | 0.248 *** | −0.178 ** | 0.179 ** | — | |
| 8 | ES | 10.992 (3.22) | −0.014 | −0.178 ** | 0.189 ** | −0.047 | 0.175 ** | −0.118 | −0.098 | — |
| High-depression-risk group | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
| 1 | CES | 29.007 (7.62) | — | |||||||
| 2 | PC | 2.963 (0.49) | −0.096 | — | ||||||
| 3 | NC | 2.267 (0.49) | −0.064 | 0.238 *** | — | |||||
| 4 | PA | 28.017 (6.48) | 0.030 | 0.495 *** | 0.129 ** | — | ||||
| 5 | NA | 21.265 (6.15) | 0.092 | −0.171*** | 0.301 *** | 0.102 * | — | |||
| 6 | LS | 17.698 (5.30) | 0.004 | 0.316 *** | 0.048 | 0.443 *** | −0.173 *** | — | ||
| 7 | CR | 22.19 (3.60) | −0.048 | 0.455 *** | 0.028 | 0.320 *** | −0.191 *** | 0.322 *** | — | |
| 8 | ES | 11.35 (2.96) | −0.054 | −0.221 *** | 0.035 | −0.209 *** | 0.079 | −0.047 | 0.051 | — |
| Var | β | t | 95%CI | Multicollinearity | ||
|---|---|---|---|---|---|---|
| Lower | Upper | Tolerance | VIF | |||
| PC | 0.01 | 0.19 | −1.4 | 1.69 | 0.59 | 1.69 |
| NC | 0.01 | 0.43 | −0.96 | 1.5 | 0.89 | 1.12 |
| PA | −0.22 | −6.02 *** | −0.41 | −0.21 | 0.59 | 1.69 |
| NA | −0.17 | −4.95 *** | −0.32 | −0.14 | 0.69 | 1.44 |
| LS | 0.07 | 2.16 * | 0.01 | 0.26 | 0.72 | 1.40 |
| CR | 0.03 | 0.77 | −0.11 | 0.26 | 0.73 | 1.37 |
| ES | 0.01 | 0.23 | −0.18 | 0.22 | 0.93 | 1.08 |
| All: F (7,1119) =16.282 ***, R2 = 0.087 | ||||||
| PC | −0.13 | −1.59 | −1.57 | 0.17 | 0.64 | 1.56 |
| NC | −0.01 | −0.15 | −0.75 | 0.65 | 0.87 | 1.15 |
| PA | −0.09 | −1.07 | −0.09 | 0.03 | 0.64 | 1.57 |
| NA | −0.14 | −1.84 | −0.09 | 0.00 | 0.72 | 1.38 |
| LS | 0.02 | 0.28 | −0.06 | 0.08 | 0.71 | 1.42 |
| CR | 0.18 | 2.44 * | 0.02 | 0.23 | 0.76 | 1.32 |
| ES | 0.01 | 0.08 | −0.11 | 0.12 | 0.91 | 1.1 |
| low-depression-risk: F (7,235) =2.252, R2 = 0.035 | ||||||
| PC | −0.12 | −1.77 | −3.82 | 0.20 | 0.56 | 1.80 |
| NC | −0.07 | −1.33 | −2.76 | 0.53 | 0.81 | 1.24 |
| PA | 0.06 | 0.89 | −0.08 | 0.21 | 0.59 | 1.71 |
| NA | 0.10 | 1.76 | −0.01 | 0.26 | 0.75 | 1.33 |
| LS | 0.03 | 0.57 | −0.12 | 0.21 | 0.73 | 1.37 |
| CR | 0.00 | 0.02 | −0.24 | 0.24 | 0.71 | 1.40 |
| ES | −0.07 | −1.37 | −0.45 | 0.08 | 0.89 | 1.13 |
| high-depression-risk: F (7,403) =1.825, R2 = 0.014 | ||||||
| Var | Group | M (SD) | t (df) | p Value | 95%CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| CES | Risk | 31.185 (7.31) | 61.947 (411.88) | 0.000 | 26.487 | 28.223 |
| NonRisk | 3.83 (2.27) | |||||
| PC | Risk | 2.952 (0.5) | −1.321 (505) | 0.187 | −0.149 | 0.029 |
| NonRisk | 3.012 (0.48) | |||||
| NC | Risk | 2.257 (0.49) | −1.913 (505) | 0.056 | −0.177 | 0.002 |
| NonRisk | 2.344 (0.5) | |||||
| PA | Risk | 28.047 (6.49) | −12.945 (505) | 0.000 | −8.970 | −6.606 |
| NonRisk | 35.835 (6.63) | |||||
| NA | Risk | 21.285 (6.14) | −10.765 (310.65) | 0.000 | −8.798 | −6.079 |
| NonRisk | 28.723 (8.22) | |||||
| LS | Risk | 17.777 (5.25) | 0.087 (505) | 0.931 | −0.937 | 1.024 |
| NonRisk | 17.734 (5.71) | |||||
| CR | Risk | 22.219 (3.65) | 1.113 (505) | 0.266 | −0.294 | 1.063 |
| NonRisk | 21.835 (3.93) | |||||
| ES | Risk | 11.245 (2.89) | 1.309 (505) | 0.191 | −0.179 | 0.891 |
| NonRisk | 10.888 (3.07) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, X.; Chen, Y.; Ao, N.; Xiao, Y.; Du, F. A Depression-Risk Mental Pattern Identified by Hidden Markov Model in Undergraduates. Int. J. Environ. Res. Public Health 2022, 19, 14411. https://doi.org/10.3390/ijerph192114411
Jiang X, Chen Y, Ao N, Xiao Y, Du F. A Depression-Risk Mental Pattern Identified by Hidden Markov Model in Undergraduates. International Journal of Environmental Research and Public Health. 2022; 19(21):14411. https://doi.org/10.3390/ijerph192114411
Chicago/Turabian StyleJiang, Xiaowei, Yanan Chen, Na Ao, Yang Xiao, and Feng Du. 2022. "A Depression-Risk Mental Pattern Identified by Hidden Markov Model in Undergraduates" International Journal of Environmental Research and Public Health 19, no. 21: 14411. https://doi.org/10.3390/ijerph192114411
APA StyleJiang, X., Chen, Y., Ao, N., Xiao, Y., & Du, F. (2022). A Depression-Risk Mental Pattern Identified by Hidden Markov Model in Undergraduates. International Journal of Environmental Research and Public Health, 19(21), 14411. https://doi.org/10.3390/ijerph192114411