




Estimation of Psychological Impairment and Coping Strategies during COVID-19 Pandemic among University Students in Saudi Arabia: A Large Regional Analysis

 ,
,  ,
,  ,
,  ,
,  , , , , , , ,
, , , , , , , 
Abstract
1. Introduction
2. Materials and Methods
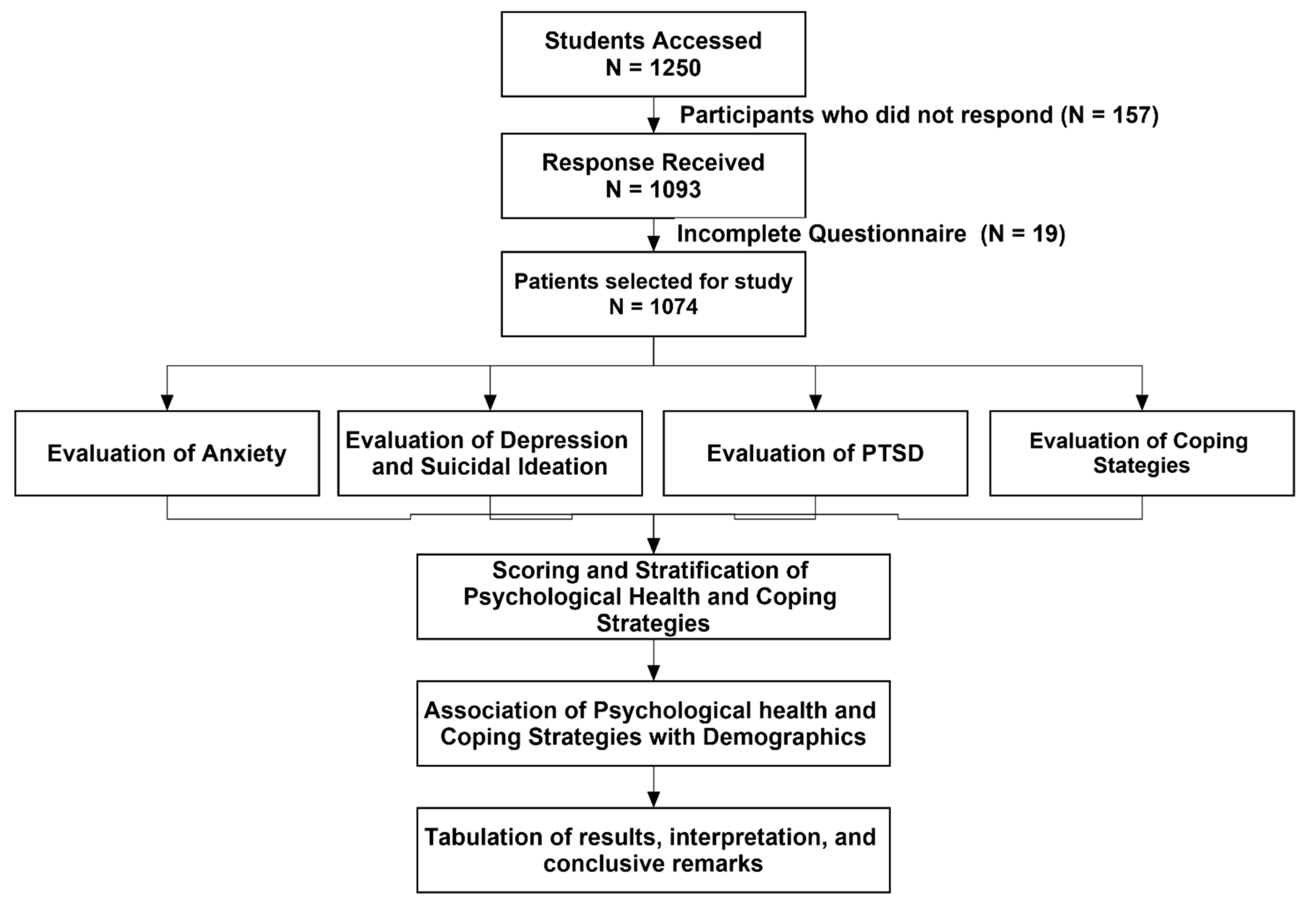
2.1. Study Design, Settings and Subjects
2.2. Ethical Approval and Considerations
2.3. Study Instruments
2.4. Outcome Measures
2.5. Validation of Study Instrument
2.6. Data Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Anxiety and Depression
3.3. Suicidal Ideation/Self-Harm
3.4. Post-Traumatic Stress Disorder (PTSD)
3.5. Coping Strategies Adopted by the Respondents
4. Discussion
4.1. Study Limitations
4.2. Implications for Future Research and Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Misbah, S.; Ahmad, A.; Butt, M.H.; Khan, Y.H.; Alotaibi, N.H.; Mallhi, T.H. A systematic analysis of studies on corona virus disease 19 (COVID-19) from viral emergence to treatment. J. Coll. Physicians Surg. Pak. 2020, 30, 9–18. [Google Scholar]
- Mallhi, T.H.; Ahmad, A.; Butt, M.H.; Misbah, S.; Khan, Y.H.; Alotaibi, N.H. Chloroquine and hydroxychloroquine in COVID-19: Practice implications for healthcare professionals. J. Coll. Physicians Surg. Pak. 2020, 30, 124–128. [Google Scholar] [PubMed]
- Lindahl, J.F.; Grace, D. The consequences of human actions on risks for infectious diseases: A review. Infect. Ecol. Epidemiol. 2015, 5, 30048. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.; Asif, N.; Mustafa, Z.U.; Khan, T.M.; Shehzadi, N.; Tahir, H.; Raza, M.H.; Khan, M.T.; Hussain, K.; Khan, Y.H. Psychological Impairment and Coping Strategies during the COVID-19 Pandemic among Students in Pakistan: A Cross-Sectional Analysis. Disaster Med. Public Health Prep. 2020; Online ahead of print. [Google Scholar] [CrossRef]
- Khan, Y.H.; Mallhi, T.H.; Alotaibi, N.H.; Alzarea, A.I.; Alanazi, A.S.; Tanveer, N.; Hashmi, F.K. Threat of COVID-19 vaccine hesitancy in Pakistan: The need for measures to neutralize misleading narratives. Am. J. Trop. Med. Hyg. 2020, 103, 603. [Google Scholar] [CrossRef] [PubMed]
- Tekir, Ö. The relationship between fear of COVID-19, psychological well-being and life satisfaction in nursing students: A cross-sectional study. PLoS ONE 2022, 17, e0264970. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Wu, K.K.; Chan, S.K.; Ma, T.M. Posttraumatic stress, anxiety, and depression in survivors of severe acute respiratory syndrome (SARS). J. Trauma. Stress Off. Publ. Int. Soc. Trauma. Stress Stud. 2005, 18, 39–42. [Google Scholar] [CrossRef]
- Zhu, X.; Liu, J. Education in and after Covid-19: Immediate responses and long-term visions. Postdigit. Sci. Educ. 2020, 2, 695–699. [Google Scholar] [CrossRef]
- Saudi Arabia to Close Schools Indefinitely from Monday. 2020. Available online: https://gulfbusiness.com/saudi-arabia-close-schools-monday/ (accessed on 6 June 2021).
- King Salman Imposes Curfew across Saudi Arabia to Contain COVID-19. 2020. Available online: https://www.arabnews.com/node/1645526/saudi-arabia (accessed on 6 June 2021).
- Alrasheedy, A.A.; Abdulsalim, S.; Farooqui, M.; Alsahali, S.; Godman, B. Knowledge, attitude and practice about coronavirus disease (COVID-19) pandemic and its psychological impact on students and their studies: A cross-sectional study among pharmacy students in Saudi Arabia. Risk Manag. Healthc. Policy 2021, 14, 729. [Google Scholar] [CrossRef]
- Browning, M.H.; Larson, L.R.; Sharaievska, I.; Rigolon, A.; McAnirlin, O.; Mullenbach, L.; Cloutier, S.; Vu, T.M.; Thomsen, J.; Reigner, N. Psychological impacts from COVID-19 among university students: Risk factors across seven states in the United States. PLoS ONE 2021, 16, e0245327. [Google Scholar] [CrossRef]
- Padrón, I.; Fraga, I.; Vieitez, L.; Montes, C.; Romero, E. A study on the psychological wound of COVID-19 in university students. Front. Psychol. 2021, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.; Asif, N.; Mustafa, Z.U.; Khan, T.M.; Shehzadi, N.; Hussain, K.; Tahir, H.; Raza, M.H.; Khan, M.T. Psychological impact of COVID-19 on Pakistani university students and how they are coping. Medrxiv 2020. [Google Scholar] [CrossRef]
- Wathelet, M.; Fovet, T.; Jousset, A.; Duhem, S.; Habran, E.; Horn, M.; Debien, C.; Notredame, C.-E.; Baubet, T.; Vaiva, G. Prevalence of and factors associated with post-traumatic stress disorder among French university students 1 month after the COVID-19 lockdown. Transl. Psychiatry 2021, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Faisal, R.A.; Jobe, M.C.; Ahmed, O.; Sharker, T. Mental health status, anxiety, and depression levels of Bangladeshi university students during the COVID-19 pandemic. Int. J. Ment. Health Addict. 2022, 20, 1500–1515. [Google Scholar] [CrossRef] [PubMed]
- Dodd, R.H.; Dadaczynski, K.; Okan, O.; McCaffery, K.J.; Pickles, K. Psychological wellbeing and academic experience of University students in Australia during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 866. [Google Scholar] [CrossRef]
- AlHadi, A.N.; AlAteeq, D.A.; Al-Sharif, E.; Bawazeer, H.M.; Alanazi, H.; AlShomrani, A.T.; Shuqdar, R.M.; AlOwaybil, R. An arabic translation, reliability, and validation of Patient Health Questionnaire in a Saudi sample. Ann. Gen. Psychiatry 2017, 16, 32. [Google Scholar] [CrossRef] [PubMed]
- AlHadi, A.N.; Alarabi, M.A.; AlMansoor, K.M. Mental health and its association with coping strategies and intolerance of uncertainty during the COVID-19 pandemic among the general population in Saudi Arabia: Cross-sectional study. BMC Psychiatry 2021, 21, 1–13. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. J. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef]
- Louzon, S.A.; Bossarte, R.; McCarthy, J.F.; Katz, I.R. Does Suicidal Ideation as Measured by the PHQ-9 Predict Suicide Among VA Patients? Psychiatr. Serv. 2016, 67, 517–522. [Google Scholar] [CrossRef]
- Kim, S.; Lee, H.-K.; Lee, K. Which PHQ-9 items can effectively screen for suicide? Machine learning approaches. Int. J. Environ. Res. Public Health 2021, 18, 3339. [Google Scholar] [CrossRef] [PubMed]
- Rossom, R.C.; Coleman, K.J.; Ahmedani, B.K.; Beck, A.; Johnson, E.; Oliver, M.; Simon, G.E. Suicidal ideation reported on the PHQ9 and risk of suicidal behavior across age groups. J. Affect. Disord. 2017, 215, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.W.; Lo, I.P.Y.; Yan, E. Health and social inclusion: The impact of psychological well-being and suicide attempts among older men who have sex with men. Am. J. Men’s Health 2022, 16, 15579883221120985. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, H.Y.; Harthi, S.S.A.L.; Alzahrani, A.S. Reliability and Validity of Arabic Translation of the Impact of Event Scale-Revised for COVID-19 Pandemic. Med. Sci. 2020, 2020, 3051–3060. [Google Scholar]
- Alghamdi, M. Cross-cultural validation and psychometric properties of the Arabic Brief COPE in Saudi population. Med. J. Malays. 2020, 75, 502–509. [Google Scholar]
- Allen, S.F.; Stevenson, J.; Lazuras, L.; Akram, U. The role of the COVID-19 pandemic in altered psychological well-being, mental health and sleep: An online cross-sectional study. Psychol. Health Med. 2022, 27, 343–351. [Google Scholar] [CrossRef]
- Salman, M.; Mustafa, Z.U.; Javaid, A.W.; Shehzadi, N.; Mallhi, T.H.; Khan, Y.H.; Masood, F.; Hussain, K. Assessment of corona-phobia in university students with the COVID-19 Phobia Scale (C19P-S): A cross-sectional analysis. Salud. Ment. 2022, 45, 253–260. [Google Scholar] [CrossRef]
- Grande, R.A.N.; Berdida, D.J.E.; Villagracia, H.N.; Cornejo, L.T.O.; Villacorte, L.M.; Borja, M.V.F. Association Between Perceived Resilience and Mental Well-Being of Saudi Nursing Students During COVID-19 Pandemic: A Cross-Sectional Study. J. Holist. Nurs. 2021, 39, 314–324. [Google Scholar] [CrossRef]
- Badr, A.F.; Binmahfouz, L.S. Impact of COVID-19 Pandemic on Mental Health Among Pharmacy Students at King Abdulaziz University, Jeddah, Saudi Arabia. Mediterr. J. Soc. Sci. 2020, 11, 12. [Google Scholar] [CrossRef]
- Alkwai, H.M. Graduating from Medical School amid a Pandemic: A Study of Graduates’ Mental Health and Concerns. Educ. Res. Int. 2021, 2021, 8854587. [Google Scholar] [CrossRef]
- AlJhani, S.; Alateeq, D.; Alwabili, A.; Alamro, A. Mental health and online learning among medical students during the COVID-19 pandemic: A Saudi national study. J. Ment. Health Train. Educ. Pract. 2022, 17, 323–334. [Google Scholar] [CrossRef]
- Mohammed, Z.; Arafa, A.; Atlam, E.-S.; El-Qerafi, N.; El-Shazly, M.; Al-Hazazi, O.; Ewis, A. Psychological problems among university students in Saudi Arabia during the COVID-19 pandemic. Int. J. Clin. Pract. 2021, 75, e14853. [Google Scholar] [CrossRef] [PubMed]
- Alkhamees, A.A.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the students of Saudi Arabia. Open Public Health J. 2021, 14, 1–9. [Google Scholar] [CrossRef]
- AlHadi, A.N.; Alhuwaydi, A.M. The mental health impact of pandemic COVID-19 crisis on university students in Saudi Arabia and associated factors. J. Am. Coll. Health 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Alyoubi, A.; Halstead, E.J.; Zambelli, Z.; Dimitriou, D. The impact of the COVID-19 pandemic on students’ mental health and sleep in Saudi Arabia. J. Int. J. Environ. Res. Public Health 2021, 18, 9344. [Google Scholar] [CrossRef]
- Alfakeh, S.A.J. Impact of COVID-19 on the Mental Health of University Students. Ann. Med. Health Sci. Res. 2021, 11, 1348–1353. [Google Scholar]
- Chinna, K.; Sundarasen, S.; Khoshaim, H.B.; Kamaludin, K.; Nurunnabi, M.; Baloch, G.M.; Hossain, S.F.A.; Sukayt, A.; Dalina, N.; Rajagopalan, U. Psychological impact of COVID-19 and lock down measures: An online cross-sectional multicounty study on Asian university students. PLoS ONE 2021, 16, e0253059. [Google Scholar] [CrossRef]
- Khoshaim, H.B.; Al-Sukayt, A.; Chinna, K.; Nurunnabi, M.; Sundarasen, S.; Kamaludin, K.; Baloch, G.M.; Hossain, S.F.A. How students in the Kingdom of Saudi Arabia are coping with COVID-19 pandemic. J. Public Health Res. 2020, 9 (Suppl. 1), 1898. [Google Scholar] [CrossRef]
- Fatima, M.; Habib, A.; Khan, S.; Butt, M.H.; Mallhi, T.H.; Khan, Y.H.; Zaheer, A.; Habib, M.U.; Khan, A.Q.; Khan, M.I.; et al. Knowledge, Attitude, Practice, Behavior and Risk Perception of COVID-19 Pandemic among Medical and non-Medical University Students. Disaster Med. Public Health Prep. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Jehi, T.; Khan, R.; Santos, H.D.; Majzoub, N. Effect of COVID-19 outbreak on anxiety among students of higher education; A review of literature. Curr. Psychol. 2022. [Google Scholar] [CrossRef]
- Liyanage, S.; Saqib, K.; Khan, A.F.; Thobani, T.R.; Tang, W.-C.; Chiarot, C.B.; AlShurman, B.A.; Butt, Z.A. Prevalence of Anxiety in University Students during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- Brailovskaia, J.; Teismann, T.; Friedrich, S.; Schneider, S.; Margraf, J. Suicide ideation during the COVID-19 outbreak in German university students: Comparison with pre-COVID 19 rates. J. Affect. Disord. Rep. 2021, 6, 100228. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.A.-O.; Shehzadi, N.; Mustafa, Z.A.-O.; Mallhi, T.H.; Khan, Y.H.; Khan, T.M.; Hussain, K. Self-harm and suicidal ideation in Pakistani youth amid COVID-19 pandemic: Findings of a large, cross-sectional study. Psychol. Health Med. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, Y.-p.; Wang, J.; Deng, Y.; Peng, D.; Zhao, L. Anxiety Status and Influencing Factors of Rural Residents in Hunan During the Coronavirus Disease 2019 Epidemic: A Web-Based Cross-Sectional Survey. Front. Psychiatry 2020, 11, 564745. [Google Scholar] [CrossRef] [PubMed]
- Davico, C.; Ghiggia, A.; Marcotulli, D.; Ricci, F.; Amianto, F.; Vitiello, B. Psychological impact of the COVID-19 pandemic on adults and their children in Italy. Front. Psychiatry 2021, 12, 239. [Google Scholar] [CrossRef]
- Idoiaga, N.; Legorburu, I.; Ozamiz-Etxebarria, N.; Lipnicki, D.M.; Villagrasa, B.; Santabárbara, J. Prevalence of Post-Traumatic Stress Disorder (PTSD) in University Students during the COVID-19 Pandemic: A Meta-Analysis Attending SDG 3 and 4 of the 2030 Agenda. Sustainability 2022, 14, 7914. [Google Scholar] [CrossRef]
- Al Dhaheri, A.S.; Bataineh, M.F.; Mohamad, M.N.; Ajab, A.; Al Marzouqi, A.; Jarrar, A.H.; Habib-Mourad, C.; Jamous, D.O.A.; Ali, H.I.; Al Sabbah, H.; et al. Impact of COVID-19 on mental health and quality of life: Is there any effect? A cross-sectional study of the MENA region. PLoS ONE 2021, 16, e0249107. [Google Scholar] [CrossRef]
- Chan, A.S.W.; Ho, J.M.C.; Li, J.S.F.; Tam, H.L.; Tang, P.M.K. Impacts of COVID-19 pandemic on psychological well-being of older chronic kidney disease patients. Front. Med. 2021, 8, 666973. [Google Scholar] [CrossRef]
- Salman, M.; Mustafa, Z.U.; Asif, N.; Shehzadi, N.; Hussain, K.; Khan, T.M.; Mallhi, T.H.; Khan, Y.H.; Butt, M.H.; Farrukh, M.J. Awareness of COVID-19 among illiterate Population in Pakistan: A Cross-Sectional analysis. Disaster Med. Public Health Prep. 2021, Online ahead of print. [CrossRef]
- El-Zoghby, S.M.; Soltan, E.M.; Salama, H.M. Impact of the COVID-19 pandemic on mental health and social support among adult Egyptians. J. Community Health Nurs. 2020, 45, 689–695. [Google Scholar] [CrossRef]
- Brown, S.M.; Doom, J.R.; Lechuga-Peña, S.; Watamura, S.E.; Koppels, T. Stress and parenting during the global COVID-19 pandemic. Child Abuse Neglect 2020, 110, 104699. [Google Scholar] [CrossRef] [PubMed]
- Currie, C.L. Adult PTSD symptoms and substance use during Wave 1 of the COVID-19 pandemic. Addict. Behav. Rep. 2021, 13, 100341. [Google Scholar] [CrossRef] [PubMed]
- Nastasi, B.K.; Sarkar, S.; Varjas, K.; Jayasena, A. Participatory model of mental health programming: Lessons learned from work in a developing country. Sch. Psychol. Rev. 1998, 27, 260–276. [Google Scholar] [CrossRef]
- Cappella, E.; Jackson, D.R.; Bilal, C.; Hamre, B.K.; Soulé, C. Bridging mental health and education in urban elementary schools: Participatory research to inform intervention development. Sch. Psychol. Rev. 2011, 40, 486–508. [Google Scholar] [CrossRef]
- Kumar, A.; Sarkar, M.; Davis, E.; Morphet, J.; Maloney, S.; Ilic, D.; Palermo, C. Impact of the COVID-19 pandemic on teaching and learning in health professional education: A mixed methods study protocol. BMC Med. Educ. 2021, 21, 439. [Google Scholar] [CrossRef]
- Zhao, Y.; Watterston, J. The changes we need: Education post COVID-19. J. Educ. Chang. 2021, 22, 3–12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographics | Subgroups | N (%) | Anxiety Score | Depression Score | PTSD Score |
|---|---|---|---|---|---|
| Overall Score | 7.50 ± 5.51 | 9.31 ± 6.72 | 21.64 ± 17.63 | ||
| Age | ≤20 years | 449 (41.8) | 7.70 ± 5.69 | 9.14 ± 6.84 | 22.04 ± 18.48 |
| 21–25 years | 603 (56.1) | 7.37 ± 5.39 | 9.48 ± 6.66 | 21.51 ± 17.10 | |
| ≥26 years | 22 (2.0) | 6.73 ± 5.18 | 8.41 ± 5.76 | 17.27 ± 13.88 | |
| p-value | -- | 0.512 | 0.587 | 0.312 * | |
| Gender | Male | 276 (25.7) | 7.51 ± 5.66 | 9.56 ± 6.64 | 22.01 ± 17.58 |
| Female | 798 (74.3) | 7.49 ± 5.46 | 9.23 ± 6.75 | 21.52 ± 17.66 | |
| p-value | -- | 0.959 | 0.484 | 0.69 | |
| Education | Health Sciences | 416 (38.7) | 7.30 ± 5.61 | 9.15 ± 6.82 | 21.55 ± 17.29 |
| Engineering | 195 (18.2) | 7.60 ± 5.94 | 9.48 ± 7.61 | 24.43 ± 20.20 | |
| Natural Sciences | 168 (15.6)295 (27.5) | 7.83 ± 5.25 | 9.29 ± 6.19 | 21.72 ± 17.09 | |
| Business and Humanities | 7.50 ± 5.29 | 9.44 ± 6.23 | 19.89 ± 16.42 | ||
| p-value | -- | 0.760 * | 0.930 * | 0.075 * | |
| Year of study | First | 269 (25.0) | 7.57 ± 5.77 | 8.87 ± 6.92 | 22.24 ± 19.28 |
| Second | 257 (23.9) | 7.62 ± 5.39 | 9.45 ± 6.77 | 22.47 ± 17.98 | |
| Third | 248 (23.1) | 7.62 ± 5.44 | 9.54 ± 6.42 | 21.67 ± 17.32 | |
| Forth | 300 (27.9) | 7.22 ± 5.45 | 9.41 ± 6.74 | 20.37 ± 15.99 | |
| p-value | 0.792 | 0.656 | 0.451 * | ||
| Family member, relative or acquaintances got COVID-19 | Yes | 878 (81.8) | 8.08 ± 6.05 | 9.76 ± 7.48 | 24.02 ± 19.51 |
| No | 196 (18.2) | 7.37 ± 5.38 | 9.21 ± 6.53 | 21.11 ± 17.15 | |
| p-value | -- | 0.1 | 0.346 | 0.055 | |
| Infected with COVID-19? | Yes | 189 (17.6) | 7.64 ± 5.49 | 9.40 ± 6.71 | 21.83 ± 17.50 |
| No | 885 (82.4) | 6.84 ± 5.58 | 8.90 ± 6.75 | 20.76 ± 18.28 | |
| p-value | 0.07 | 0.35 | 0.45 |
| Variable | Subgroups | Self-Distraction | Active Coping | Denial | Substance Use | Emotional Support | Instrumental Support | Behavioral Disengagement | Venting | Positive Reframing | Planning | Humor | Acceptance | Religion | Self-Blame |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | -- | 4.30 ± 1.742 | 4.65 ± 1.86 | 3.40 ± 1.71 | 2.64 ± 1.32 | 4.02 ± 1.80 | 4.01 ± 1.94 | 3.32 ± 1.59 | 38.3 ± 1.71 | 4.47 ± 1.97 | 4.51 ± 1.96 | 36.8 ± 1.81 | 5.15 ± 2.10 | 5.43 ± 2.15 | 3.59 ± 1.82 |
| Age | ≤20 years | 4.29 ± 1.79 | 4.70 ± 1.85 | 3.40 ± 1.76 | 2.60 ± 1.27 | 4.03 ± 1.81 | 3.94 ± 1.91 | 3.31 ± 1.64 | 3.82 ± 1.72 | 4.57 ± 2.03 | 4.57 ± 2.02 | 3.65 ± 1.80 | 5.13 ± 2.10 | 5.49 ± 2.19 | 3.58 ± 1.81 |
| 21–25 years | 4.31 ± 1.72 | 4.59 ± 1.86 | 3.40 ± 1.68 | 2.66 ± 1.36 | 3.99 ± 1.79 | 4.04 ± 1.94 | 3.34 ± 1.56 | 3.83 ± 1.70 | 4.41 ± 1.92 | 4.46 ± 1.92 | 3.71 ± 1.82 | 5.16 ± 2.09 | 5.39 ± 2.13 | 3.62 ± 1.82 | |
| ≥ 26 years | 4.14 ± 1.49 | 5.00 ± 2.02 | 3.45 ± 1.71 | 2.64 ± 1.00 | 4.68 ± 1.94 | 4.59 ± 2.20 | 3.05 ± 1.36 | 4.00 ± 1.75 | 4.14 ± 1.98 | 4.68 ± 1.86 | 3.23 ± 1.60 | 5.45 ± 2.30 | 5.64 ± 2.30 | 3.14 ± 1.86 | |
| p-value | 0.882 | 0.426 | 0.989 | 0.721 | 0.209 | 0.251 | 0.681 | 0.887 | 0.299 | 0.602 | 0.42 | 0.769 | 0.696 | 0.458 | |
| Gender | Male | 4.35 ± 1.77 | 4.88 ± 1.89 | 3.41 ± 1.78 | 2.72 ± 1.44 | 4.16 ± 1.92 | 4.28 ± 2.05 | 3.38 ± 1.72 | 3.80 ± 1.72 | 4.59 ± 1.97 | 4.83 ± 1.90 | 3.91 ± 1.91 | 5.46 ± 2.10 | 5.66 ± 2.10 | 3.67 ± 1.84 |
| Female | 4.28 ± 1.73 | 4.56 ± 1.84 | 3.40 ± 1.69 | 2.60 ± 1.27 | 3.97 ± 1.76 | 3.91 ± 1.89 | 3.30 ± 1.57 | 3.84 ± 1.70 | 4.43 ± 1.97 | 4.40 ± 1.97 | 3.60 ± 1.76 | 5.04 ± 2.09 | 5.36 ± 2.17 | 3.57 ± 1.81 | |
| p-value | 0.574 | 0.014 | 0.903 | 0.217 | 0.129 | 0.009 | 0.501 | 0.792 | 0.232 | 0.001 | 0.015 | 0.004 | 0.044 | 0.402 | |
| Education | Health Sciences | 4.25 ± 1.79 | 4.70 ± 1.96 | 3.37 ± 1.75 | 2.67 ± 1.39 | 4.07 ± 1.86 | 4.10 ± 1.96 | 3.33 ± 1.61 | 3.79 ± 1.69 | 4.48 ± 2.00 | 4.56 ± 1.94 | 3.64 ± 1.82 | 5.14 ± 2.12 | 5.45 ± 2.12 | 3.59 ± 1.79 |
| Engineering | 4.44 ± 1.87 | 4.75 ± 1.96 | 3.48 ± 1.84 | 2.71 ± 1.44 | 4.10 ± 1.82 | 4.08 ± 2.06 | 3.38 ± 1.79 | 3.93 ± 1.90 | 4.74 ± 2.04 | 4.81 ± 2.10 | 3.66 ± 1.93 | 5.28 ± 2.15 | 5.70 ± 2.23 | 3.75 ± 1.92 | |
| Natural Sciences | 4.29 ± 1.71 | 4.55 ± 1.73 | 3.34 ± 1.67 | 2.57 ± 1.22 | 4.07 ± 1.74 | 4.12 ± 1.91 | 3.29 ± 1.53 | 4.01 ± 1.73 | 4.57 ± 1.99 | 4.54 ± 2.01 | 3.83 ± 1.80 | 5.51 ± 2.11 | 5.63 ± 2.17 | 3.63 ± 1.87 | |
| Business and Humanities | 4.28 ± 1.60 | 4.56 ± 1.72 | 3.43 ± 1.59 | 2.57 ± 1.18 | 3.87 ± 1.73 | 3.78 ± 1.82 | 3.29 ± 1.46 | 3.71 ± 1.58 | 4.22 ± 1.85 | 4.21 ± 1.84 | 3.65 ± 1.71 | 4.88 ± 2.00 | 5.12 ± 2.11 | 3.47 ± 1.74 | |
| p-value | 0.695 | 0.551 | 0.849 | 0.551 | 0.411 | 0.095 | 0.922 | 0.256 | 0.032 | 0.008 | 0.681 | 0.015 | 0.012 | 0.43 | |
| Year of study | First | 4.18 ± 1.74 | 4.64 ± 1.91 | 3.23 ± 1.61 | 2.59 ± 1.30 | 3.86 ± 1.68 | 3.87 ± 1.78 | 3.17 ± 1.57 | 3.74 ± 1.68 | 4.53 ± 1.99 | 4.47 ± 1.97 | 3.58 ± 1.74 | 5.04 ± 2.06 | 5.49 ± 2.22 | 3.45 ± 1.74 |
| Second | 4.28 ± 1.71 | 4.67 ± 1.77 | 3.58 ± 1.78 | 2.76 ± 1.41 | 4.05 ± 1.90 | 4.01 ± 2.03 | 3.37 ± 1.68 | 3.95 ± 1.80 | 4.35 ± 2.00 | 4.53 ± 2.04 | 3.70 ± 1.94 | 5.02 ± 2.18 | 5.28 ± 2.15 | 3.66 ± 1.88 | |
| Third | 4.37 ± 1.72 | 4.75 ± 1.86 | 3.52 ± 1.82 | 2.70 ± 1.34 | 4.25 ± 1.87 | 4.15 ± 2.00 | 3.44 ± 1.57 | 3.74 ± 1.59 | 4.60 ± 1.95 | 4.59 ± 1.94 | 3.70 ± 1.76 | 5.33 ± 2.04 | 5.65 ± 2.08 | 3.60 ± 1.78 | |
| Forth | 4.36 ± 1.80 | 4.54 ± 1.86 | 3.31 ± 1.64 | 2.51 ± 1.26 | 3.96 ± 1.75 | 4.02 ± 1.93 | 3.32 ± 1.55 | 3.88 ± 1.74 | 4.41 ± 1.94 | 4.45 ± 1.90 | 3.73 ± 1.79 | 5.22 ± 2.11 | 5.34 ± 2.15 | 3.67 ± 1.86 | |
| p-value | 0.571 | 0.603 | 0.057 | 0.130 | 0.094 | 0.402 | 0.271 | 0.423 | 0.469 | 0.848 | 0.765 | 0.27 | 0.225 | 0.446 | |
| Family member, relative or acquaintances got COVID-19 | No | 4.37 ± 1.80 | 4.76 ± 1.95 | 3.35 ± 1.80 | 2.80 ± 1.47 | 4.23 ± 1.91 | 4.18 ± 1.96 | 3.39 ± 1.73 | 3.91 ± 1.84 | 4.60 ± 1.96 | 4.78 ± 2.04 | 3.67 ± 1.78 | 5.26 ± 2.18 | 5.55 ± 2.20 | 3.68 ± 1.91 |
| Yes | 4.28 ± 1.73 | 4.62 ± 1.84 | 3.41 ± 1.70 | 2.60 ± 1.28 | 3.97 ± 1.77 | 3.97 ± 1.77 | 3.31 ± 1.56 | 3.81 ± 1.68 | 4.44 ± 1.97 | 4.45 ± 1.94 | 3.68 ± 1.82 | 5.13 ± 2.08 | 5.41 ± 2.15 | 3.58 ± 1.79 | |
| p-value | 0.503 | 0.364 | 0.65 | 0.073 | 0.081 | 0.163 | 0.486 | 0.438 | 0.326 | 0.031 | 0.997 | 0.441 | 0.421 | 0.449 | |
| Infected with COVID-19? | No | 4.32 ± 1.74 | 4.67 ± 1.86 | 3.41 ± 1.72 | 2.67 ± 1.35 | 4.04 ± 1.81 | 4.01 ± 1.93 | 3.35 ± 1.61 | 3.85 ± 1.71 | 4.48 ± 1.94 | 4.53 ± 1.96 | 3.72 ± 1.83 | 5.17 ± 2.08 | 5.45 ± 2.14 | 3.64 ± 1.83 |
| Yes | 4.20 ± 1.77 | 4.52 ± 1.84 | 3.35 ± 1.67 | 2.48 ± 1.14 | 3.92 ± 1.75 | 4.00 ± 1.97 | 3.16 ± 1.50 | 3.72 ± 1.69 | 4.43 ± 2.12 | 4.42 ± 1.95 | 3.50 ± 1.71 | 5.05 ± 2.17 | 5.37 ± 2.25 | 3.38 ± 1.71 | |
| p-value | 0.379 | 0.319 | 0.673 | 0.043 | 0.397 | 0.942 | 0.134 | 0.362 | 0.753 | 0.489 | 0.133 | 0.456 | 0.655 | 0.074 |
| Variable | Education | Mean Difference | Standard Error | p-Value | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Positive reframing | Health Sciences vs. Engineering | −0.260 | 0.170 | 0.420 | −0.70 | 0.18 |
| Health Sciences vs. Natural Sciences | −0.082 | 0.179 | 0.968 | −0.54 | 0.38 | |
| Health Sciences vs. Business and Humanities | 0.259 | 0.149 | 0.305 | −0.12 | 0.64 | |
| Engineering vs. Natural Sciences | 0.178 | 0.207 | 0.824 | −0.35 | 0.71 | |
| Engineering vs. Business and Humanities | 0.520 | 0.181 | 0.022 | 0.05 | 0.99 | |
| Natural Sciences vs. Business and Humanities | 0.342 | 0.190 | 0.273 | −0.15 | 0.83 | |
| Planning | Health Sciences vs. Engineering | −0.248 | 0.169 | 0.460 | −0.68 | 0.19 |
| Health Sciences vs. Natural Sciences | 0.027 | 0.178 | 0.999 | −0.43 | 0.49 | |
| Health Sciences vs. Business and Humanities | 0.349 | 0.149 | 0.088 | −0.03 | 0.73 | |
| Engineering vs. Natural Sciences | 0.275 | 0.205 | 0.540 | −0.25 | 0.80 | |
| Engineering vs. Business and Humanities | 0.597 | 0.180 | 0.005 | 0.13 | 1.06 | |
| Natural Sciences vs. Business and Humanities | 0.322 | 0.189 | 0.320 | −0.16 | 0.81 | |
| Acceptance | Health Sciences vs. Engineering | −0.145 | 0.181 | 0.854 | −0.61 | 0.32 |
| Health Sciences vs. Natural Sciences | −0.369 | 0.191 | 0.215 | −0.86 | 0.12 | |
| Health Sciences vs. Business and Humanities | 0.256 | 0.159 | 0.375 | −0.15 | 0.66 | |
| Engineering vs. Natural Sciences | −0.224 | 0.220 | 0.739 | −0.79 | 0.34 | |
| Engineering vs. Business and Humanities | 0.401 | 0.193 | 0.161 | −0.10 | 0.90 | |
| Natural Sciences vs. Business and Humanities | 0.625 | 0.202 | 0.011 | 0.11 | 1.14 | |
| Religious coping | Health Sciences vs. Engineering | −0.248 | 0.186 | 0.542 | −0.73 | 0.23 |
| Health Sciences vs. Natural Sciences | −0.177 | 0.196 | 0.805 | −0.68 | 0.33 | |
| Health Sciences vs. Business and Humanities | 0.339 | 0.163 | 0.162 | −0.08 | 0.76 | |
| Engineering vs. Natural Sciences | 0.072 | 0.226 | 0.989 | −0.51 | 0.65 | |
| Engineering vs. Business and Humanities | 0.587 | 0.198 | 0.016 | 0.08 | 1.10 | |
| Natural Sciences vs. Business and Humanities | 0.516 | 0.207 | 0.063 | −0.02 | 1.05 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mallhi, T.H.; Ahmad, N.; Salman, M.; Tanveer, N.; Shah, S.; Butt, M.H.; Alatawi, A.D.; Alotaibi, N.H.; Rahman, H.U.; Alzarea, A.I.; et al. Estimation of Psychological Impairment and Coping Strategies during COVID-19 Pandemic among University Students in Saudi Arabia: A Large Regional Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14282. https://doi.org/10.3390/ijerph192114282
Mallhi TH, Ahmad N, Salman M, Tanveer N, Shah S, Butt MH, Alatawi AD, Alotaibi NH, Rahman HU, Alzarea AI, et al. Estimation of Psychological Impairment and Coping Strategies during COVID-19 Pandemic among University Students in Saudi Arabia: A Large Regional Analysis. International Journal of Environmental Research and Public Health. 2022; 19(21):14282. https://doi.org/10.3390/ijerph192114282
Chicago/Turabian StyleMallhi, Tauqeer Hussain, Naveed Ahmad, Muhammad Salman, Nida Tanveer, Shahid Shah, Muhammad Hammad Butt, Ahmed D. Alatawi, Nasser Hadal Alotaibi, Hidayat Ur Rahman, Abdulaziz Ibrahim Alzarea, and et al. 2022. "Estimation of Psychological Impairment and Coping Strategies during COVID-19 Pandemic among University Students in Saudi Arabia: A Large Regional Analysis" International Journal of Environmental Research and Public Health 19, no. 21: 14282. https://doi.org/10.3390/ijerph192114282
APA StyleMallhi, T. H., Ahmad, N., Salman, M., Tanveer, N., Shah, S., Butt, M. H., Alatawi, A. D., Alotaibi, N. H., Rahman, H. U., Alzarea, A. I., Alanazi, A. S., Alzahrani, M. S., Alshehri, S., Aljabri, A., & Khan, Y. H. (2022). Estimation of Psychological Impairment and Coping Strategies during COVID-19 Pandemic among University Students in Saudi Arabia: A Large Regional Analysis. International Journal of Environmental Research and Public Health, 19(21), 14282. https://doi.org/10.3390/ijerph192114282