


Minimal Dose of Resistance Exercise Required to Induce Immediate Hypotension Effect in Older Adults with Hypertension: Randomized Cross-Over Controlled Trial

 ,
,  ,
,  ,
,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Procedures
2.2.1. Familiarization Session and Intensity Calculation
2.2.2. Experimental Sessions
2.2.3. Outcomes
2.3. Statistical Analysis
3. Results
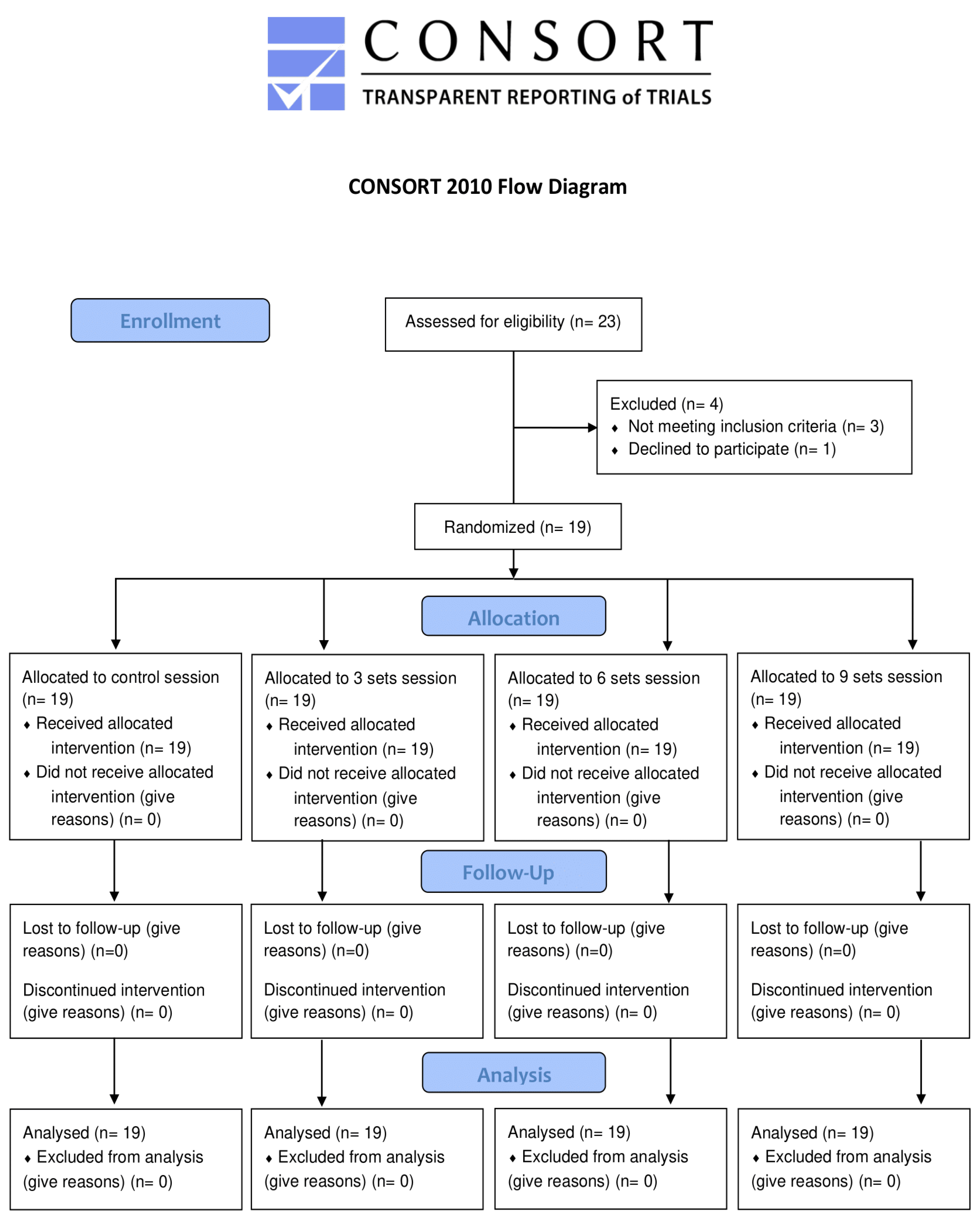
3.1. Flow Diagram and Characteristics of the Sample
3.2. Hemodynamic Effects
4. Discussion
4.1. Hemodynamic Effects
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, Regional, and National Age-Sex Specific Mortality for 264 Causes of Death, 1980–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- World Health Organization. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis: World Health Day 2013. Available online: https://www.who.int/publications-detail-redirect/a-global-brief-on-hypertension-silent-killer-global-public-health-crisis-world-health-day-2013 (accessed on 20 September 2021).
- Pimenta, F.C.; Montrezol, F.T.; Dourado, V.Z.; da Silva, L.F.M.; Borba, G.A.; de Oliveira Vieira, W.; Medeiros, A. High-Intensity Interval Exercise Promotes Post-Exercise Hypotension of Greater Magnitude Compared to Moderate-Intensity Continuous Exercise. Eur. J. Appl. Physiol. 2019, 119, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Prospective Studies Collaboration. Age-Specific Relevance of Usual Blood Pressure to Vascular Mortality: A Meta-Analysis of Individual Data for One Million Adults in 61 Prospective Studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef]
- Gąsowski, J.; Piotrowicz, K.; Messerli, F.H. Arterial Hypertension after Age 65: From Epidemiology and Pathophysiology to Therapy Do We Know Where We Stand? Kardiol. Pol. 2018, 76, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Appel, L.J.; Rubenfire, M.; Ogedegbe, G.; Bisognano, J.D.; Elliott, W.J.; Fuchs, F.D.; Hughes, J.W.; Lackland, D.T.; Staffileno, B.A.; et al. American Heart Association Professional Education Committee of the Council for High Blood Pressure Research, Council on Cardiovascular and Stroke Nursing, Council on Epidemiology and Prevention, and Council on Nutrition, Physical Activity. Beyond Medications and Diet: Alternative Approaches to Lowering Blood Pressure: A Scientific Statement from the American Heart Association. Hypertension 2013, 61, 1360–1383. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Smart, N.A. Exercise Training for Blood Pressure: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef]
- MacDonald, H.V.; Johnson, B.T.; Huedo-Medina, T.B.; Livingston, J.; Forsyth, K.C.; Kraemer, W.J.; Farinatti, P.T.V.; Pescatello, L.S. Dynamic Resistance Training as Stand-Alone Antihypertensive Lifestyle Therapy: A Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e003231. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement from the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Carpio-Rivera, E.; Moncada-Jiménez, J.; Salazar-Rojas, W.; Solera-Herrera, A. Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arq. Bras. Cardiol. 2016, 106, 422–433. [Google Scholar] [CrossRef]
- Brito, L.C.; Queiroz, A.C.C.; Forjaz, C.L.M. Influence of Population and Exercise Protocol Characteristics on Hemodynamic Determinants of Post-Aerobic Exercise Hypotension. Braz. J. Med. Biol. Res. 2014, 47, 626–636. [Google Scholar] [CrossRef]
- Casonatto, J.; Goessler, K.F.; Cornelissen, V.A.; Cardoso, J.R.; Polito, M.D. The Blood Pressure-Lowering Effect of a Single Bout of Resistance Exercise: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Eur. J. Prev. Cardiolog. 2016, 23, 1700–1714. [Google Scholar] [CrossRef] [PubMed]
- Brito, L.C.; Fecchio, R.Y.; Peçanha, T.; Andrade-Lima, A.; Halliwill, J.R.; Forjaz, C.L.M. Postexercise Hypotension as a Clinical Tool: A “Single Brick” in the Wall. J. Am. Soc. Hypertens. 2018, 12, e59–e64. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; Franklin, B.A.; Fagard, R.; Farquhar, W.B.; Kelley, G.A.; Ray, C.A.; American College of Sports Medicine. American College of Sports Medicine Position Stand. Exercise and Hypertension. Med. Sci. Sports Exerc. 2004, 36, 533–553. [Google Scholar] [CrossRef] [PubMed]
- Bentes, C.M.; Costa, P.B.; Corrêa Neto, V.G.; Simão, R.; Paz, G.A.; Maia, M.F.; Figueiredo, T.; Neto, G.R.; Novaes, J.S.; Miranda, H. Hypotensive Responses of Reciprocal Supersets versus Traditional Resistance Training in Apparently Healthy Men. Int. J. Exerc. Sci. 2017, 10, 434–445. [Google Scholar] [PubMed]
- Machado, C.L.F.; Bgeginski, R.; De Castro, C.; Wilhelm, E.N.; Pinto, R.S. Acute Hemodynamic Responses to Repetitions to Failure Using Different Resistance Exercises and Protocols in Normotensive Men: A Crossover Study. Clin. Exp. Hypertens. 2020, 42, 401–408. [Google Scholar] [CrossRef]
- Liu, S.; Goodman, J.; Nolan, R.; Lacombe, S.; Thomas, S.G. Blood Pressure Responses to Acute and Chronic Exercise Are Related in Prehypertension. Med. Sci. Sport. Exerc. 2012, 44, 1644–1652. [Google Scholar] [CrossRef]
- Mediano, M.F.F.; Paravidino, V.; Simão, R.; Pontes, F.L.; Polito, M.D. Subacute Behavior of the Blood Pressure after Power Training in Controlled Hypertensive Individuals. Rev. Bras. Med. Esporte 2005, 11, 337–340. [Google Scholar] [CrossRef]
- Brito, A.D.F.; Brasileiro-Santos, M.D.S.; de Oliveira, C.V.C.; Santos, A.D.C. Postexercise Hypotension Is Volume-Dependent in Hypertensives: Autonomic and Forearm Blood Responses. J. Strength Cond. Res. 2019, 33, 234–241. [Google Scholar] [CrossRef]
- De Oliveira, C.V.C.; Santos, A.D.C.; Brito, A.; Brasileiro, M.S.S. Resistance Exercise with Different Volumes: Blood Pressure Response and Forearm Blood Flow in the Hypertensive Elderly. Clin. Interv. Aging 2014, 9, 2151–2158. [Google Scholar] [CrossRef][Green Version]
- Scher, L.M.L.; Ferriolli, E.; Moriguti, J.C.; Scher, R.; Lima, N.K.C. The Effect of Different Volumes of Acute Resistance Exercise on Elderly Individuals with Treated Hypertension. J. Strength Cond. Res. 2011, 25, 1016–1023. [Google Scholar] [CrossRef]
- Polito, M.D.; Farinatti, P.T.V. The Effects of Muscle Mass and Number of Sets during Resistance Exercise on Postexercise Hypotension. J. Strength Cond. Res. 2009, 23, 2351–2357. [Google Scholar] [CrossRef] [PubMed]
- Simão, R.; Fleck, S.J.; Polito, M.; Monteiro, W.; Farinatti, P. Effects of Resistance Training Intensity, Volume, and Session Format on the Postexercise Hypotensive Response. J. Strength Cond. Res. 2005, 19, 853. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, T.; Rhea, M.R.; Peterson, M.; Miranda, H.; Bentes, C.M.; dos Reis, V.M.d.R.; Simão, R. Influence of Number of Sets on Blood Pressure and Heart Rate Variability after a Strength Training Session. J. Strength Cond. Res. 2015, 29, 1556–1563. [Google Scholar] [CrossRef]
- Rocha, A.C.; Sartori, M.; Rodrigues, B.; De Angelis, K. Influence of the Number of Sets in Cardiovascular and Autonomic Adjustments to Resistance Exercise in Physically Active Men. Rev. Bras. Med. Esporte 2013, 19, 332–335. [Google Scholar] [CrossRef]
- Burton, E.; Farrier, K.; Lewin, G.; Pettigrew, S.; Hill, A.-M.; Airey, P.; Bainbridge, L.; Hill, K.D. Motivators and Barriers for Older People Participating in Resistance Training: A Systematic Review. J. Aging Phys. Act. 2017, 25, 311–324. [Google Scholar] [CrossRef]
- Burton, E.; Hill, A.-M.; Pettigrew, S.; Lewin, G.; Bainbridge, L.; Farrier, K.; Airey, P.; Hill, K.D. Why Do Seniors Leave Resistance Training Programs? Clin. Interv. Aging 2017, 12, 585–592. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine Position Stand. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for Blood Pressure Measurement in Humans and Experimental Animals: Part 1: Blood Pressure Measurement in Humans: A Statement for Professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation 2005, 111, 697–716. [Google Scholar] [CrossRef]
- La Scala Teixeira, C.V.; Ferreira, S.E.; Azevedo, P.H.; Chulvi-Medrano, I.; Dorgo, S.; de Salles, B.F.; Simao, R.; Gomes, R.J. Effects of Manual Resistance Training and Free Weight Resistance Training on Postexercise Blood Pressure in Hypertensive Men: A Pilot Study. J. Sports Med. Phys. Fit. 2017, 57, 1367–1374. [Google Scholar] [CrossRef]
- Lemieux, J.; Beaton, D.E.; Hogg-Johnson, S.; Bordeleau, L.J.; Goodwin, P.J. Three Methods for Minimally Important Difference: No Relationship Was Found with the Net Proportion of Patients Improving. J. Clin. Epidemiol. 2007, 60, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Brito, A.D.F.; Brasileiro-Santos, M.D.S.; de Oliveira, C.V.C.; da Nóbrega, T.K.S.; Forjaz, C.L.D.M.; Santos, A.D.C. High-Intensity Resistance Exercise Promotes Postexercise Hypotension Greater than Moderate Intensity and Affects Cardiac Autonomic Responses in Women Who Are Hypertensive. J. Strength Cond. Res. 2015, 29, 3486–3493. [Google Scholar] [CrossRef] [PubMed]
- Keese, F.; Farinatti, P.; Pescatello, L.; Monteiro, W. A Comparison of the Immediate Effects of Resistance, Aerobic, and Concurrent Exercise on Postexercise Hypotension. J. Strength Cond. Res. 2011, 25, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Bonham, A.C. Postexercise Hypotension: Central Mechanisms. Exerc. Sport Sci. Rev. 2010, 38, 122–127. [Google Scholar] [CrossRef]
- Brandão Rondon, M.U.P.; Alves, M.J.N.N.; Braga, A.M.F.W.; Teixeira, O.T.U.N.; Barretto, A.C.P.; Krieger, E.M.; Negrão, C.E. Postexercise Blood Pressure Reduction in Elderly Hypertensive Patients. J. Am. Coll. Cardiol. 2002, 39, 676–682. [Google Scholar] [CrossRef]
- Queiroz, A.C.C.; Sousa, J.C.S.; Cavalli, A.A.P.; Silva, N.D.; Costa, L.A.R.; Tobaldini, E.; Montano, N.; Silva, G.V.; Ortega, K.; Mion, D.; et al. Post-Resistance Exercise Hemodynamic and Autonomic Responses: Comparison between Normotensive and Hypertensive Men. Scand. J. Med. Sci. Sports 2015, 25, 486–494. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Collier, S.R.; Kelly, E.E.; Jae, S.Y.; Fernhall, B. Arterial Stiffness and Baroreflex Sensitivity Following Bouts of Aerobic and Resistance Exercise. Int. J. Sports Med. 2007, 28, 197–203. [Google Scholar] [CrossRef]
- Halliwill, J.R.; Buck, T.M.; Lacewell, A.N.; Romero, S.A. Postexercise Hypotension and Sustained Postexercise Vasodilatation: What Happens after We Exercise? Exp. Physiol. 2013, 98, 7–18. [Google Scholar] [CrossRef]
- Zafeiridis, A. Mechanisms and Exercise Characteristics Influencing Postexercise Hypotension. J. Adv. Med. Med. Res. 2014, 4, 5699–5714. [Google Scholar] [CrossRef]
- Law, M.R.; Morris, J.K.; Wald, N.J. Use of Blood Pressure Lowering Drugs in the Prevention of Cardiovascular Disease: Meta-Analysis of 147 Randomised Trials in the Context of Expectations from Prospective Epidemiological Studies. BMJ 2009, 338, b1665. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total Sample (n = 19) |
|---|---|
| Mean age (range) 1 | 64.53 (55–70) |
| Gender (male) 2 | 13 (68.42) |
| Height 1 | 165.74 (7.37) |
| Weight 1 | 80.37 (14.45) |
| BMI 1 | 29.37 (5.37) |
| Diabetes 2 | 9 (47.37) |
| Type I or II hypertension 2 | 19 (100) |
| Antihypertensive medication 2 | 19 (100) |
| Monotherapy | |
| Angiotensin-converting enzyme inhibitors (ACEI) | 2 (10.52) |
| Angiotensin receptor blockers (ARBs) | 1 (5.26) |
| Dihydropyridine calcium channel blockers (CCBs) | 1 (5.26) |
| Diuretics | 3 (15.78) |
| ẞ-Blockers | 3 (15.78) |
| Angiotensin II receptor antagonist | 1 (5.26) |
| Combination therapy | |
| Diuretics + CCBs | 2 (10.52) |
| CCBs + ẞ-Blockers | 1 (5.26) |
| ẞ-Blockers + ACEI | 2 (10.52) |
| CCBs + ARBs | 1 (5.26) |
| Diuretics + ẞ-Blockers+ ACEI | 1 (5.26) |
| Diuretics + CCBs + ARBs | 1 (5.26) |
| Time (min) | SBP (mm Hg) | DBP (mm Hg) | ||||||
|---|---|---|---|---|---|---|---|---|
| Control | 3 Sets | 6 Sets | 9 Sets | Control | 3 Sets | 6 Sets | 9 Sets | |
| Basal | 135 (130–140) | 138 (133–143) | 137 (132–142) | 138 (133–142) | 77 (75–80) | 78 (76–81) | 78 (76–81) | 78 (75–81) |
| 0 | 137 (132–142) | 134 (129–139) | 132 (127–137) | 132 (127–137) | 78 (75–81) | 70 (68–73) | 72 (69–75) | 73 (71–76) |
| 30 | 138 (133–143) | 132 (127–137) | 130 (125–135) | 129 (124–134) | 80 (77–82) | 76 (73–78) | 75 (72–78) | 75 (73–78) |
| 60 | 141 (136–146) | 135 (130–140) | 130 (125–135) | 132 (127–137) | 79 (76–82) | 78 (75–80) | 77 (74–79) | 76 (73–78) |
| 240 | 129 (124–134) | 124 (119–129) | 130 (125–135) | 127 (122–132) | 74 (71–76) | 71 (69–74) | 73 (70–76) | 73 (70–76) |
| 300 | 127 (122–132) | 126 (121–132) | 129 (124–134) | 128 (123–133) | 74 (71–76) | 73 (70–76) | 73 (70–75) | 73 (70–76) |
| 360 | 130 (125–135) | 126 (120–131) | 128 (123–133) | 128 (123–133) | 75 (72–77) | 73 (70–76) | 73 (70–76) | 74 (71–77) |
| Time (min) | MBP (mm Hg) | MHR (bpm) | ||||||
|---|---|---|---|---|---|---|---|---|
| Control | 3 Sets | 6 Sets | 9 Sets | Control | 3 Sets | 6 Sets | 9 Sets | |
| Basal | 97 (94–100) | 98 (95–101) | 98 (95–101) | 98 (95–101) | 68 (65–71) | 68 (65–72) | 68 (65–71) | 68 (65–71) |
| 0 | 98 (94–101) | 92 (88–95) | 92 (89–95) | 93 (90–96) | 65 (62–68) | 70 (67–73) | 72 (69–75) | 73 (70–76) |
| 30 | 99 (96–102) | 95 (92–98) | 93 (90–96) | 93 (90–96) | 63 (60–66) | 65 (62–68) | 65 (62–68) | 65 (62–68) |
| 60 | 100 (97–103) | 97 (94–100) | 95 (92–98) | 95 (92–98) | 61 (58–64) | 62 (59–65) | 63 (60–66) | 63 (60–66) |
| 240 | 92 (89–95) | 89 (86–92) | 92 (89–95) | 91 (88–94) | 69 (66–72) | 70 (67–74) | 72 (68–75) | 67 (64–70) |
| 300 | 92 (89–95) | 91 (87–94) | 91 (88–94) | 91 (88–94) | 69 (66–72) | 73 (69–76) | 73 (70–76) | 68 (65–72) |
| 360 | 93 (90–96) | 90 (87–94) | 91 (88–94) | 92 (89–95) | 71 (68–74) | 72 (69–76) | 71 (68–74) | 67 (64–70) |
| Time (min) | SBP | DBP | MBP | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 3 Sets vs. Control | 6 Sets vs. Control | 9 Sets vs. Control | 3 Sets vs. Control | 6 Sets vs. Control | 9 Sets vs. Control | 3 Sets vs. Control | 6 Sets vs. Control | 9 Sets vs. Control | |
| 0 | 03 (−04 to 10) | 02 (−05 to 09) | 02 (−05 to 09) | 01 (−03 to 05) | 01 (−03 to 05) | 01 (−03 to 04) | 02 (−03 to 06) | 01 (−03 to 06) | 01 (−03 to 05) |
| 2 | −03 (−10 to 04) | −04 (−11 to 03) | −05 (−12 to 02) | −08 (−11 to −04) | −06 (−10 to −02) | −05 (−09 to −01) | −06 (−10 to −02) | −05 (−10 to −01) | −05 (−09 to −01) |
| 30 | −06 (−13 to 01) | −08 (−15 to −01) | −09 (−16 to −02) | −04 (−08 to 00) | −05 (−08 to −01) | −04 (−08 to −01) | −05 (−09 to 00) | −06 (−10 to −01) | −06 (−10 to −02) |
| 60 | −06 (−13 to 01) | −10 (−17 to −03) | −09 (−16 to −02) | −01 (−05 to 02) | −02 (−06 to 01) | −03 (−07 to 00) | −03 (−07 to 02) | −05 (−09 to −01) | −05 (−09 to −01) |
| 240 | −05 (−12 to 03) | 01 (−06 to 08) | −02 (−09 to 05) | −02 (−06 to 02) | −01 (−04 to 03) | 00 (−04 to 03) | −03 (−07 to 02) | 00 (−04 to 04) | −01 (−05 to 03) |
| 300 | −01 (−08 to 07) | 02 (−06 to 09) | 01 (−06 to 08) | −01 (−05 to 03) | −01 (−05 to 03) | −01 (−05 to 03) | −01 (−05 to 04) | 00 (−05 to 04) | 00 (−05 to 04) |
| 360 | −04 (−11 to 03) | −02 (−09 to 06) | −02 (−09 to 06) | −02 (−06 to 02) | −02 (−06 to 02) | −01 (−05 to 03) | −03 (−07 to 02) | −02 (−06 to 03) | −01 (−05 to 03) |
| Basal | 0 min | 30 min | 60 min | 240 min | 300 min | 360 min | |||
|---|---|---|---|---|---|---|---|---|---|
| SBP | Control vs. 3 sets | Magnitude | 0.41 | 0.96 | 0.92 | 0.95 | −0.26 | −0.13 | −0.28 |
| Classification | small | large | large | large | small | trivial | small | ||
| MCID | 3.75 | 3.25 | 3.05 | 3.62 | 7.26 | 6.17 | 8.39 | ||
| Control vs. 6 sets | Magnitude | 0.35 | 0.82 | 0.93 | 0.79 | 0.27 | 0.81 | 0.02 | |
| Classification | small | large | large | moderate | small | large | trivial | ||
| MCID | 3.31 | 3.10 | 2.73 | 3.24 | 5.15 | 3.14 | 4.06 | ||
| Control vs. 9 sets | Magnitude | 0.41 | 0.80 | 0.79 | 0.90 | 0.12 | 0.74 | 6.65 | |
| Classification | small | large | moderate | large | trivial | moderate | trivial | ||
| MCID | 3.24 | 3.31 | 2.65 | 3 | 3.14 | 2.58 | 6.51 | ||
| DBP | Control vs. 3 sets | Magnitude | 0.42 | 0.29 | 0.82 | 0.96 | −0.36 | −0.05 | −0.23 |
| Classification | small | trivial | large | large | small | trivial | small | ||
| MCID | 2.06 | 2.11 | 2.07 | 2.18 | 4.38 | 3.80 | 4.94 | ||
| Control vs. 6 sets | Magnitude | 0.30 | 0.63 | 0.67 | 0.60 | 0.49 | 0.67 | 0.00 | |
| Classification | small | moderate | moderate | moderate | small | moderate | trivial | ||
| MCID | 2.11 | 1.93 | 1.81 | 2.03 | 3.08 | 1.81 | 3.75 | ||
| Control vs. 9 sets | Magnitude | 0.23 | 0.45 | 0.74 | 0.68 | 0.53 | 0.47 | 0.09 | |
| Classification | small | small | moderate | moderate | moderate | moderate | trivial | ||
| MCID | 1.70 | 1.87 | 1.73 | 1.97 | 2.11 | 1.62 | 3.82 | ||
| MBP | Control vs. 3 sets | Magnitude | 0.50 | −0.21 | −0.06 | 0.09 | −0.48 | −0.24 | −0.25 |
| Classification | moderate | small | trivial | trivial | small | small | small | ||
| MCID | 2.16 | 2.04 | 2.03 | 2.22 | 5.25 | 4.43 | 5.97 | ||
| Control vs. 6 sets | Magnitude | 0.37 | -0.11 | -0.31 | −0.20 | −0.16 | 0.28 | 0.00 | |
| Classification | small | trivial | small | small | trivial | small | trivial | ||
| MCID | 2.19 | 1.97 | 1.84 | 2.09 | 3.57 | 1.91 | 4.57 | ||
| Control vs. 9 sets | Magnitude | 0.39 | −0.23 | −0.38 | −0.27 | 0.15 | 0.21 | 0.09 | |
| Classification | small | small | small | small | trivial | small | trivial | ||
| MCID | 1.81 | 1.91 | 1.70 | 1.92 | 2.11 | 1.56 | 4.58 | ||
| MHR | Control vs. 3 sets | Magnitude | 0.23 | 0.44 | 0.04 | −0.17 | −0.31 | 0.01 | −0.15 |
| Classification | small | small | trivial | trivial | small | trivial | trivial | ||
| MCID | 2.46 | 2.64 | 2.49 | 2.46 | 4.56 | 4.24 | 5.21 | ||
| Control vs. 6 sets | Magnitude | 0.07 | 0.35 | 0.37 | 0.37 | 0.39 | 0.37 | 0.05 | |
| Classification | trivial | small | small | small | small | small | trivial | ||
| MCID | 2.51 | 2.59 | 2.48 | 2.44 | 3.32 | 2.42 | 4.06 | ||
| Control vs. 9 sets | Magnitude | 0.07 | 0.47 | −0.05 | −0.25 | 0.38 | 0.21 | −0.07 | |
| Classification | trivial | small | trivial | small | small | small | trivial | ||
| MCID | 2.53 | 2.92 | 2.57 | 2.57 | 2.23 | 2.33 | 3.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gargallo, P.; Casaña, J.; Suso-Martí, L.; Cuenca-Martínez, F.; López-Bueno, R.; Andersen, L.L.; López-Bueno, L.; Cuerda-del Pino, A.; Calatayud, J. Minimal Dose of Resistance Exercise Required to Induce Immediate Hypotension Effect in Older Adults with Hypertension: Randomized Cross-Over Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 14218. https://doi.org/10.3390/ijerph192114218
Gargallo P, Casaña J, Suso-Martí L, Cuenca-Martínez F, López-Bueno R, Andersen LL, López-Bueno L, Cuerda-del Pino A, Calatayud J. Minimal Dose of Resistance Exercise Required to Induce Immediate Hypotension Effect in Older Adults with Hypertension: Randomized Cross-Over Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(21):14218. https://doi.org/10.3390/ijerph192114218
Chicago/Turabian StyleGargallo, Pedro, José Casaña, Luis Suso-Martí, Ferran Cuenca-Martínez, Rubén López-Bueno, Lars Louis Andersen, Laura López-Bueno, Alba Cuerda-del Pino, and Joaquín Calatayud. 2022. "Minimal Dose of Resistance Exercise Required to Induce Immediate Hypotension Effect in Older Adults with Hypertension: Randomized Cross-Over Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 21: 14218. https://doi.org/10.3390/ijerph192114218
APA StyleGargallo, P., Casaña, J., Suso-Martí, L., Cuenca-Martínez, F., López-Bueno, R., Andersen, L. L., López-Bueno, L., Cuerda-del Pino, A., & Calatayud, J. (2022). Minimal Dose of Resistance Exercise Required to Induce Immediate Hypotension Effect in Older Adults with Hypertension: Randomized Cross-Over Controlled Trial. International Journal of Environmental Research and Public Health, 19(21), 14218. https://doi.org/10.3390/ijerph192114218