Abstract
Introduction: Although high-risk work environments and heavy workload expose medical professionals to long-term risks of disease, no comprehensive analysis has been conducted on the corresponding risks of diseases to each type of medical professionals. This study pre-analyzed the risks of medical professionals in developing various systemic diseases in Taiwan to provide a comprehensive examination of the differences between each type of systemic disease. Methods: From the secondary databases of 2002–2013, 15,407 medical professionals were selected for analysis. A chi-squared test and logistic regression were performed to identify the relationship between types of medical professionals and systemic diseases. The life trajectories of diagnosis sequence of the medical professionals were illustrated accordingly. Results: The physicians were the most vulnerable to infectious, parasitic, and digestive diseases. This was possibly associated with their work characteristics and occupational risks. Conclusion: According to the life trajectories, all types of the medical professionals exhibited a similar trend in the orders of risks to each type of systemic disease, which suggests that their work environment exposes them to real risks of health hazard.
1. Introduction
The Ministry of Health and Welfare of Taiwan published the top ten causes of death for 2020. In addition to transportation accidents, the causes of death were neoplasms; endocrine diseases, nutritional diseases, metabolic and immune diseases; digestive diseases; diseases of the circulatory system; diseases of the respiratory system, and diseases of the genitourinary system [1], classified according to the International Classification of Diseases, Ninth Revision (ICD-9). These causes of death have been in the top ten causes of death in Taiwan for more than ten years. According to the World Health Organization (WHO), the top three causes of death worldwide for 2019 were diseases of the circulatory system, diseases of the respiratory system, and certain conditions originating in the perinatal period [2]. The top two causes of death worldwide are similar to those in Taiwan. Furthermore, the WHO has indicated that heart diseases (diseases of the circulatory system) have been a leading cause of death worldwide for the past 20 years. These diseases impose a heavy burden on national insurance and therefore need to be taken seriously, but unfortunately, we do not have any database of death-related cases to explore mortality or survival.
Multiple studies have indicated that medical workers are susceptible to infectious and parasitic diseases [3,4]; neoplasms [5,6]; endocrine diseases, nutritional diseases, metabolic and immune diseases [7,8]; psychosis [9,10]; neurological disorders and eye and adnexa diseases [11,12]; diseases of the circulatory system [6,12]; diseases of the respiratory system [13,14]; digestive diseases [15,16]; diseases of the genitourinary system [15]; diseases of the skin and subcutaneous tissue [17,18], and diseases of the musculoskeletal system and connective tissue [19,20,21]. Many risk factors have been associated with medical workers to develop systemic diseases, such as occupation [6,22], gender [23], age [24], work experience, Charlson comorbidity index [16], payroll bracket, medical institution class [25], medical institution ownership, division of the National Health Insurance Administration, and degree of urbanization [26]. The International Labour Organization (ILO) has reported a high correlation between working environments and occupational diseases [27]. Medical workers are exposed to high-risk working environments for long periods; hence, they are more susceptible to occupational diseases. The ILO has stated that, for a disease to be defined as occupational, a causal relationship must be proven to exist; however, verifying the causal relationship between medical occupations and systemic diseases is difficult. Therefore, whether the aforementioned systemic diseases are definable as occupational disease remains debatable. However, the investigations performed in this study can serve as a reference for relevant institutions seeking to implement precautionary measures in the future.
Although it is generally known that medical providers are in occupations subject to higher risk of contracting disease, there are few effective protections. Furthermore, past studies on the diseases of medical providers have predominantly focused on specific diseases and the environmental risk factors that caused such diseases; they have rarely provided comprehensive analyses of the types of systemic diseases medical workers may have. Therefore, we designed a complete analysis of diseases contracted by medical providers, and chose not to focus on specific diseases. We classified multiple diseases with the same characteristics into one kind of systemic diseases. We expect to be able to predict which medical providers will develop certain kinds of systemic diseases and want to further understand which factors correlate with systemic diseases. This study hypothesized that medical providers will suffer from multiple occupational systemic diseases. We also expect that the results of this study can provide institutions developing national health policies with insights into future formulation of preventive measures to reduce occupational risks for medical workers.
2. Methods
2.1. Data Sources
This retrospective study used a secondary database. The study period was from 2002 to 2013, and the data were collected from 1 million random records provided by the National Health Insurance Research Database (NHIRD). Established in 1995, NHIRD is the most complete electronic health record in Taiwan. The NHIRD contains demographic variables, outpatient and inpatient information, prescriptions, diagnosis information, medical personnel information, and other detailed clinical information [28]. Our data sources were five types of registration files, Registry for beneficiaries (ID), Registry for contracted medical facilities (HOSB), Registry for medical personnel (PER), Ambulatory care expenditures by visits (CD), and Inpatient expenditures by admissions (DD). Our study was approved by the Research Ethics Committee of China Medical University Hospital, Taiwan. To protect the patients’ privacy, all personal identification numbers were encrypted by the National Health Research Institutes before the data were released. The Taiwan National Health Research Institutes encrypts patients’ personal information to protect privacy and provides researchers with anonymous scrambled identification numbers associated with relevant disease information. Therefore, a patient informed consent is not required for authorized researchers to access this research database.
2.2. Inclusion and Exclusion Criteria
Our study included 77,035 people with systemic diseases, and systemic diseases defined according to the ICD-9 standard from the 2002 to 2013 NHIRD database. Later, we excluded 228 people whose incomplete data or lost date of diagnosis. Then, we divided the study sample into two groups: non-medical professionals and medical professionals (N = 15,179). In a second stage, we divided the medical professionals into three groups according to occupation, e.g., physician, nursing personnel, and other medical personnel. Other medical personnel included pharmacists, midwives, medical technologists, dental technicians, physical therapists, radiographers, counseling psychologists, dietitians, and social workers (Figure S1).
2.3. ICD-9 of Systemic Diseases
Our research objectives were to explore the relationship between medical providers and diseases. The authors try to cover all diseases; however, there are currently more than a hundred thousand ICD-9 codes. Therefore, we referred to the top 10 causes of death published in Taiwan, and identified 11 disease categories as follows: infectious and parasitic diseases; neoplasms; endocrine, nutritional, metabolic, and immune diseases; psychosis; neurological disorders and eye and adnexa diseases; diseases of the circulatory system; diseases of the respiratory system; digestive diseases; diseases of the genitourinary system; diseases of the skin and subcutaneous tissue; and diseases of the musculoskeletal system and connective tissue. The codes are presented in Table 1 below.

Table 1.
ICD-9-CM codes to systemic diseases.
2.4. Charlson Comorbidities Index
Our research used the Charlson Comorbidity Index (CCI) developed by Charlson in 1984, to evaluate the mortality risk and burden of disease, address the confounding influence of comorbidities, and predict outcomes. We followed the method proposed by Charlson; the CCI consists of 17 comorbidities, weighted from 1 to 6 according to mortality risk and disease severity, and then summed scores to form the total CCI score [29]. However, subjects rarely displayed high CCI scores in our research, so we divided the CCI categories into three groups as follows: 0 points, 1 point, and more than 2 points.
2.5. Statistical Analysis
First, we used adjusted logistic regression and a 95% confidence interval to compare the risk of developing systemic disease between workers and non-medical professionals and medical professionals. Second, we further analyzed the association of the three groups among medical professionals with developing systemic diseases. We used descriptive statistics, namely frequencies and percentages, to understand the sample distribution with respect to each variable. The chi-squared test of independence was used to test the correlation between occupations and the 11 systemic diseases. Collinearity diagnostics were performed to verify whether the independent variables had high correlations with each other; the diagnostic results did not reveal any collinearity. Adjusted logistic regression and a 95% confidence interval were used to investigate the risk of developing systemic diseases in relation to each independent variable. Finally, we designed the first day of work for medical professional as a baseline, and we calculated the time from the baseline to the diagnosis-date for each individual, and calculated separately for each systemic disease. We used the average developing years of each systemic disease to plot a life trajectory, and to explore how long after working do medical providers develop systemic diseases. These analyses were conducted using SPSS 22 software.
3. Results
3.1. Non-Medical Professionals and Medical Professionals
We divided the study samples into two groups: medical professionals and non-medical professionals. The medical professional group has 15,179 (19.76%) study samples and the non-medical professional group has 61,628 (80.24%) study samples. All variable diagnostic results did not reveal any collinearity after collinearity diagnostics. After adjusting for logistic regression analysis, medical professionals displayed a 1.160 times higher risk than non-medical professionals. We further analyzed the risk of each systemic disease between those two groups and found that the medical professional group displayed a higher risk of infectious and parasitic diseases; neoplasms; digestive diseases, and diseases of the skin and subcutaneous tissue, and conversely, diseases of the respiratory system and diseases of the musculoskeletal system and connective tissue displayed a higher risk for the non-medical professionals (Table S1).
3.2. Participant Characteristics
The study sample comprised the data of 15,179 Taiwanese medical workers. Table 2 illustrates the sample distribution with respect to each variable; 24.28% were male and 75.72% were female. The medical workers were classified as physicians (12.83%), nursing personnel (59.13%), or other medical personnel (28.04%). The average age of the medical workers was 39.67 ± 12.87 years. A higher proportion of the workers had a low Charlson comorbidity index score; had a small amount of insured salary; worked in clinics, private hospitals, or private institutions; belonged to the Taipei National Health Insurance Regional Division; lived in highly urbanized areas; and had a small amount of work experience.
Table 2.
Characteristics of the samples studied (N = 15,179).
3.3. Association between Person Type of Medical and Category Disease
The results, presented in Table 3, revealed a correlation of occupation with 10 of the 11 systemic disease categories, namely infectious and parasitic diseases; endocrine diseases, nutritional, metabolic, and immune diseases; psychosis; neurological disorders and eye and adnexa diseases; diseases of the circulatory system; diseases of the respiratory system; digestive diseases; diseases of the genitourinary system; diseases of the skin and subcutaneous tissue; and diseases of the musculoskeletal system and connective tissue. When the demographic and regional variables were controlled, physicians were 1.376 times at higher risk than other medical personnel of developing infectious and parasitic diseases (p = 0.020, odds ratio (OR) = 1.376) and 1.402 times higher risk than other medical personnel of contracting digestive diseases (p < 0.001, OR = 1.402). As indicated in Table 4, male medical providers showed 1.426 times (p = 0.009, OR = 1.426) higher risk of developing infectious and parasitic diseases than female providers, and medical providers with CCI scores of 0 and 1 were at 2.782 (p = 0.044, OR = 2.782) and 2.909 times (p = 0.038, OR = 2.909) higher risk of developing risk of infectious and parasitic diseases than medical providers with CCI scores of more than 2 points. Medical workers who worked in medical centers displayed 1.645 times (p = 0.016, OR = 1.646) higher risk of developing infectious and parasitic diseases than those working in district hospitals. In addition, medical workers living in Taipei (p = 0.003, OR = 1.578), Northern (p = <0.001, OR = 1.897), Central (p = <0.001, OR = 2.129), Southern (p = <0.001, OR = 2.033) and Eastern Divisions (p = 0.037, OR = 1.952) were all at higher risk of developing infectious and parasitic diseases than medical workers who lived in the Kaoping Division. Medical workers living in moderately urbanized, emerging, and agricultural areas were at 2.131 to 2.510 times higher risk of developing infectious and parasitic diseases than those living in remote areas. In addition, in Table 5, male medical providers (p = 0.011, OR = 1.171) were at 1.171 times higher risk of contracting digestive diseases than female medical providers, and medical providers who worked in regional hospitals (p = 0.021, OR = 1.332) and clinics (p < 0.001, OR = 1.713) displayed 1.332 and 1.713 times higher risk of developing digestive diseases than those who worked in district hospitals. Medical providers working in private hospitals or institutions (p < 0.001, OR = 1.809) displayed 1.809 times higher prevalence of digestive diseases than those working in public hospitals or institutions, and medical providers who belonged to the Taipei (p < 0.001, OR = 1.341) and the Northern Division (p = 0.004, OR = 1.240) displayed 1.341 and 1.240 times higher prevalence of digestive diseases than those belonging to the Kaoping Division.
Table 3.
Association of different medical provider in Taiwan with systemic diseases (N = 15,179).
Table 4.
Multivariable Analysis of Associations Between medical providers and infectious and parasitic disease (N = 15,179).
Table 5.
Multivariable analysis of associations between medical providers and digestive diseases (N = 15,179).
3.4. Life Trajectory
The results for the three occupation categories are listed in Figure 1. The top five systemic diseases of diagnosis sequence in each category were identified. On average, the physician group developed diseases of the respiratory system most quickly in time sequence (within 4.88 years), followed by diseases of the skin and subcutaneous tissue; infectious and parasitic diseases; digestive diseases, neurological disorders, and eye and adnexa diseases. The top five diseases for all three occupation categories included diseases of the respiratory system, diseases of the skin and subcutaneous tissue, and digestive diseases. In addition, for all three categories of occupation, diseases of the respiratory system and diseases of the skin and subcutaneous tissue were the first and second fastest diseases to develop, respectively. This result warrants further verification through research in the future. We also discovered that the average period before physicians started developing systemic diseases was longer than it was for the other two groups. This could be attributed to the health awareness and behaviors of physicians.
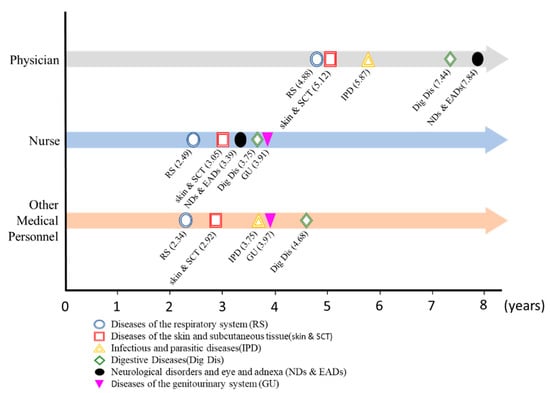
Figure 1.
Time between beginning of career and development of systemic diseases among medical professionals in Taiwan.
4. Discussion
In this study, first, we examined 11 systemic diseases between medical workers and non-medical workers. We found that medical workers have a higher risk (p < 0.001, OR = 1.160) to be diagnosed with the systemic disease than non-medical workers after adjusting the control factors. Next, we used the ICD-9 to categorize 11 systemic diseases that medical workers were susceptible to and investigated the difference between the occurrence of systemic diseases in physicians, nursing personnel, and other medical personnel. The results revealed that nursing personnel had the highest prevalence of systemic diseases (59.13%). In addition, 10 systemic diseases had significant relationships with occupation; only neoplasms did not. We further controlled related influencing factors and revealed significant relationships of infectious and parasitic diseases and digestive diseases with occupation. The risk of developing such diseases in the physician group (OR = 1.376 and 1.402, respectively) was higher than that in the other two groups. These results are consistent with the results of a previous research study, which included 90 nursing students and 110 medical residents in hospitals in India; the research study found that medical residents were at two-fold greater risk of incident latent tuberculosis infection than nursing students (Relative Risk, 2.16; 95% CI, 1.05–4.42) [30]. In addition, our results for infectious and parasitic diseases may be explained by the results of a past review research, which indicated that health care workers are more likely to be exposed to infectious and parasitic diseases, but this study does not specify whether the workers are physicians or nurses [31]. One previous research study exploring the incidence rate between physicians and the general population found that physicians had higher incidence rates of endocrine, nutritional, metabolic, and immune diseases [30], but we did not find this characteristic in our research. Finally, this study investigated the life trajectory of medical workers who developed the 11 systemic diseases after they started working in the medical industry and revealed that the median time before physicians developed infectious and parasitic diseases or digestive diseases was longer than that for nursing or other medical personnel.
4.1. Non-Medical Professionals and Medical Professionals
Our study used logistic regression and adjusting other control variables. We found that medical professionals displayed higher risk than non-medical professionals to be diagnosed with systemic diseases. One past study found the increased time spent in healthcare by medical professionals as an important risk factor for latent TB infection [32], which is consistent with our results. Another study about asthma displayed that male healthcare workers were at higher risk to suffer from asthma [33], but we did not find this result in our study. In addition, our research displayed that medical professionals have a higher risk of infectious and parasitic diseases; neoplasms; digestive diseases, and diseases of the skin and subcutaneous tissue; so, we further subdivided medical professionals into three groups: physician, nursing personnel, and other medical personnel.
4.2. Factors Correlated to the Development of Systemic Diseases in Medical Workers
We used the chi-squared test of independence and discovered that the 10 systemic diseases (excluding only neoplasms) significantly differed with occupation. Other studies have identified a correlation of systemic diseases with occupation, gender, age, Charlson comorbidity index, amount of insured salary, medical institution class, medical institution ownership, division of National Health Insurance Administration, degree of urbanization, and work experience. Therefore, this study included these factors and adjusted them to obtain the following results. Physicians had a high risk of infectious and parasitic diseases or digestive diseases, with ORs of 1.376 and 1.402, respectively. This indicated that physicians were susceptible to digestive diseases, which supports the results of past studies [34,35].
4.3. Risk of Medical Workers Developing Systemic Diseases
An adjusted logistic regression analysis revealed that infectious and parasitic diseases and digestive diseases were significantly correlated with occupation. We believe that the possible reason physicians are susceptible to infectious and parasitic diseases (e.g., Helminthiasis, Tuberculosis, Hepatitis B/C) may be related to the characteristics of their work. A plausible reason is perhaps that most physicians in Taiwan will participate in one or more clinical research projects, e.g., microbiological experiments and drug experiments that increase the chance of exposure to infectious sources [36,37]. Past research has shown that laboratory workers are more susceptible to hepatitis B infection [38]. A second possible reason, physicians in Taiwan also have a higher rate of syringe prick injury than other medical providers except for nurses [39]. A few years ago, some experts proposed that transmission of infectious microorganisms poses a threat not just to healthcare workers in direct contact with patients, but can also be spread via contaminated hands, apparel/uniforms, patient care items (e.g., IV poles, privacy curtains, blood pressure cuffs) or environmental surfaces [40]. Both may cause the spread of infectious diseases; in addition, failure to use appropriate PPE will increase the risk of exposure to splashes and splatters at work [40]. As a third possible reason, we thought that the working hours of physicians may also play a role. The findings reveal that the average total work hours per a week of an attending physician in Taiwan is around 69.1 h [41], physicians in US work about 50 h per week [42,43], nurses in Taiwan work about 50 to 60 h per a week [44,45]; physicians in Taiwan work longer than physicians in the US or nurses in Taiwan. Long-time face-to-face patient meetings indirectly increase the prevalence of infectious and parasitic diseases. In addition, there is a high incidence of burnout among Taiwan physicians, which will cause negligence in work [46].
The observation that physicians are at a higher risk of developing digestive diseases (e.g. Peptic Ulcer; Gastritis) is possibly due to their long working hours [34]. In Taiwanese hospitals, physicians working in outpatient clinics generally have numerous patients, and they require extensive time to provide all of these patients with diagnoses. Therefore, physicians often use their lunch breaks or work overtime to treat patients, which prevents them from keeping life routines and this may increase their risk of developing digestive diseases. This study also revealed that medical workers working in clinics in the Taipei or Northern Divisions of the National Health Insurance Administration had the highest risk of developing digestive diseases. This could be due to the reimbursement system of the National Health Insurance of Taiwan. According to data published by the Department of Statistics of the Ministry of Health and Welfare, more than 30% of all clinics in Taiwan are dental clinics [1]. Dental clinics have more self-payment service items than other types of clinics, and they do not have a limit on the number of patients they can receive. Because treating more patients leads to a higher income, physicians working in such clinics work overtime, thereby disrupting their life routines and maybe increasing their risk of developing digestive diseases.
4.4. Diagnosis Sequence of Systemic Diseases
In our study, we design the worker’s career start date as the baseline for the life trajectory, and listed the top five systemic diseases that medical workers developed most quickly after they began working in medical institutions and compared the results between the three categories of medical personnel. Both the types and order (regarding the time sequence of development) of diseases were similar between the three categories. This may indicate that the reason for medical workers to develop systemic diseases was not due to personal factors or habits. Rather, the diseases may have resulted from a similar working environment or other common factors. Although the results of Table 2 indicate that only two systemic diseases were significant with the occupations in our research, a similar diagnosis sequence observed in Figure 1 is still exciting. The diagnosis sequences in three occupations are coincidentally similar, this diagnosis sequence result may indirectly indicate that the systemic diseases in Figure 1 present significantly with certain occupations; and the authors may be limited by the database or undiscovered influencing factors. Future studies may further investigate this topic. This study also revealed that the average period before physicians developed systemic diseases was longer than that for the other two groups. This may be because physicians have more knowledge related to medicine and diseases [47].
5. Conclusions
Occupation as a physician was associated with infectious, parasitic, and digestive diseases. Particularly, sexes, comorbidity, types of contracts with medical institutions, insurance branches, and urbanization levels were factors presenting significant correlations with the medical professionals’ risks of disease. Furthermore, according to the life trajectories plotted in this study, a consistency was observed in the 3 groups in terms of the highest annual average occurrences, with RS occurring the most frequently, followed by skin and SCT, and Dig Dis. Accordingly, career risks are critical to medical professionals’ risks of disease. Health authorities must endeavor to promote preventive medicine education to improve the health and well-being of medical professionals.
5.1. Strengths
This study’s review of data, which was representative of medical workers across Taiwan, revealed potential factors correlated to systemic disease development in medical workers, such as their gender, age, occupation, and Charlson comorbidity index. The medical workers’ risk of developing diseases was analyzed to facilitate development of preventive measures for high-risk groups. This study can serve as a reference for medical institutions and government agencies planning preventive intervention measures. In addition, our research identified types of systemic diseases shared by different categories of medical workers. The results can serve as a reference for medical institutions and government agencies in planning disease prevention interventions.
5.2. Limitations
Our research had four limitations. First, our database used in this study did not include the average working time of medical personnel. The average working time may be a crucial factor leading medical workers to develop diseases. In addition, there are no discipline data in the NHIRD database, so we cannot classify the disciplines to which the study samples belong; secondly, other crucial correlation factors that may have contributed to medical workers to develop the included systemic diseases could not be obtained from the National Health Insurance Research Database. Such factors include family history, educational attainment, marital status, religion, work stress, and personality traits. Third, when we identified this research project, the 2002–2013 NHIRD was the most current source that allowed us to address our key populations. Although the data are not as current as we would like, but it is a database with 12 years of data. Our results can establish a baseline for future research. Fourth, our definition of control participants was based on systemic diseases ICD-9 codes and did not include other potential indicators of diseases. Fifth, after the COVID-19 pandemic, the risk of infection among medical personnel has increased significantly, which may reverse the results of the past, and it may be interesting to explore the trend of morbidity rates before and after the COVID-19 pandemic.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph192114017/s1, Figure S1. Flow chart. Table S1. Association between medical professionals and non-medical professionals in Taiwan with systemic diseases (N = 75,981).
Author Contributions
K.-J.M., J.-L.H. and J.-Y.W. designed and conceptualized the study and analyzed the data. K.-J.M. drafted the first version of the article. J.-L.H., M.-H.C. and J.-Y.W. performed the literature search and reviewed the article. All authors have revised the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Taiwan Ministry of Science and Technology [grant number: MOST110-2410-H-039-001 and MOST111-2410-H-039-001-MY2] and China Medical University [grant number: CMU110-MF-123 and CMU111-MF-90].
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of China Medical University Hospital (protocol code: CRREC-104-012 and date of approval: 10 July 2015).
Informed Consent Statement
Patient consent was waived due to all personal identification numbers were encrypted by the National Health Research Institutes before the data were released. The Taiwan National Health Research Institutes encrypts patients’ personal information to protect privacy and provides researchers with anonymous scrambled identification numbers associated with relevant disease information. Therefore, a patient informed con-sent is not required for authorized researchers to access this research database.
Data Availability Statement
This study used national databases obtained from the Health and Welfare Data Science Center (HWDC), Ministry of Health and Welfare in Taiwan. All data obtained were anonymized and deidentified by the HWDC. The data used in this study must be accessed and analyzed in the HWDC under its regulation after filling out an application and thus cannot be shared. However, such data can be accessed from the authors upon reasonable request and with permission from HWDC (https://dep.mohw.gov.tw/DOS/cp-2516-59203-113.html, accessed on 1 January 2022). Data are also available from the China medical University & Hospital Research Ethics Committee (http://61.66.117.10/2007/IRB/index.html, accessed on 1 January 2022) for researchers who satisfy the criteria for accessing confidential data.
Acknowledgments
We are grateful to Ministry of Health and Welfare (MOHW) Health and Welfare Data Science Center at China Medical University for providing support and assistance in administrative, technical and fee discount.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Statistics Ministry of Health and Welfare. Available online: https://www.mohw.gov.tw/cp-5017-61533-1.html (accessed on 1 May 2022).
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 1 May 2022).
- Kinikar, A.; Chandanwale, A.; Kadam, D.; Joshi, S.; Basavaraj, A.; Pardeshi, G.; Girish, S.; Shelke, S.; DeLuca, A.; Dhumal, G. High risk for latent tuberculosis infection among medical residents and nursing students in India. PLoS ONE 2019, 14, e0219131. [Google Scholar] [CrossRef] [PubMed]
- Hatherill, M.; Scriba, T.J.; Udwadia, Z.F.; Mullerpattan, J.B.; Hawkridge, A.; Mahomed, H.; Dye, C. BCG and new preventive tuberculosis vaccines: Implications for healthcare workers. Clin. Infect. Dis. 2016, 62, S262–S267. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, J.; Boffetta, P. Epidemiology of Occupational Lung Cancer. In Occupational Cancers; Anttila, S., Boffetta, P., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 287–294. [Google Scholar]
- Bourne, P.A. Health, lifestyle and health care utilization among health professionals. Health 2010, 2, 557–565. [Google Scholar] [CrossRef][Green Version]
- Sutanto, N.; Putra, M.A. Value of Aspect Differences Towards Theory of Planned Behavior Between Hospital Personnels of a Private Hospital in Mataram. ANIMA Indones. Psychol. J. 2019, 34, 148–162. [Google Scholar] [CrossRef]
- Chuang, C.-H.C.H.-H.; Chen, J.-Y. Prevalence of Central Obesity and Associated Health Risks in Healthcare Workers. Chin. J. Occup. Med. 2017, 24, 115–120. [Google Scholar]
- Greenberg, N. Mental health of health-care workers in the COVID-19 era. Nat. Rev. Nephrol. 2020, 16, 425–426. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef]
- Huang, W.-T.; Hung-Jung, L. Comparison of the Risk for Peripheral Vertigo between Physicians and the General Population. Iran. J. Public Health 2021, 50, 180. [Google Scholar] [CrossRef]
- Wilczyńska, U.; Szeszenia-Dabrowska, N. Occupational diseases among health and social workers in Poland. Med. Pr. 2010, 61, 597–605. [Google Scholar]
- Caridi, M.N.; Humann, M.J.; Liang, X.; Su, F.-C.; Stefaniak, A.B.; LeBouf, R.F.; Stanton, M.L.; Virji, M.A.; Henneberger, P.K. Occupation and task as risk factors for asthma-related outcomes among healthcare workers in New York City. Int. J. Hyg. Environ. Health 2019, 222, 211–220. [Google Scholar] [CrossRef]
- Walters, G.; Moore, V.; McGrath, E.; Burge, P.; Henneberger, P. Agents and trends in health care workers’ occupational asthma. Occup. Med. 2013, 63, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.-Y.; Hsieh, C.-C.; Tseng, Y.-C.; Hung, C.-H.; Chen, K.-T.; Wang, C.-H.; Tseng, Y.-T. Increased Long-Term Risks of Occupational Diseases in Homecare Nurses: A Nationwide Population-Based Retrospective Cohort Study. Women’s Health Rep. 2020, 1, 259–269. [Google Scholar] [CrossRef]
- Lin, H.-Y.; Weng, S.-F.; Lin, H.-J.; Hsu, C.-C.; Wang, J.-J.; Su, S.-B.; Guo, H.-R.; Huang, C.-C. Peptic ulcer disease in healthcare workers: A nationwide population-based cohort study. PLoS ONE 2015, 10, e0135456. [Google Scholar] [CrossRef] [PubMed]
- Alhaji, M.M.; Lai, A.; Naing, L.; Tuah, N.A. Self-reported skin disorders among health care workers. Workplace Health Saf. 2019, 67, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Alluhayyan, O.B.; Alshahri, B.K.; Farhat, A.M.; Alsugair, S.; Siddiqui, J.J.; Alghabawy, K.; AlQefari, G.B.; Alolayan, W.O.; Hashem, I.A.A. Occupational-Related Contact Dermatitis: Prevalence and Risk Factors Among Healthcare Workers in the Al’Qassim Region, Saudi Arabia During the COVID-19 Pandemic. Cureus 2020, 12, e10975. [Google Scholar] [CrossRef]
- Chan, F.-K.; Hsu, C.-C.; Lin, H.-J.; Wang, J.-J.; Su, S.-B.; Huang, C.-C.; Weng, S.-F. Physicians as well as nonphysician health care professionals in Taiwan have higher risk for lumbar herniated intervertebral disc than general population. Medicine 2018, 97, e9561. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Oka, H.; Takano, K.; Asada, F.; Nomura, T.; Kawamata, K.; Okazaki, H.; Tanaka, S.; Matsudaira, K. Association between high fear-avoidance beliefs about physical activity and chronic disabling low back pain in nurses in Japan. BMC Musculoskelet. Disord. 2019, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.-C.; Chung, J.-Y.; Feng, I.-J.; Yang, S.-H.; Hsu, C.-C.; Lin, H.-J.; Wang, J.-J.; Huang, C.-C. Plantar fasciitis in physicians and nurses: A nationwide population-based study. Ind. Health 2020, 58, 153–160. [Google Scholar] [CrossRef]
- Tam, C.; Leung, C. Occupational tuberculosis: A review of the literature and the local situation. Hong Kong Med. J. 2006, 12, 448–455. [Google Scholar]
- Hsu, Y.-H.; Kung, P.-T.; Wang, Y.-H.; Chang, Y.-M.; Tsai, W.-C. A comparison of the stages at which cancer is diagnosed in physicians and in the general population in Taiwan. CMAJ 2015, 187, E412–E418. [Google Scholar] [CrossRef]
- Chang, S.-J.; Liao, W.-C. Prevalence and Associated Risk Factors of Metabolic Syndrome among Nurses. Taiwan J. Public Health 2015, 34, 268–285. [Google Scholar]
- Lee, Y.-S.; Hsu, C.-C.; Weng, S.-F.; Lin, H.-J.; Wang, J.-J.; Su, S.-B.; Huang, C.-C.; Guo, H.-R. Cancer incidence in physicians: A Taiwan national population-based cohort study. Medicine 2015, 94, e2079. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D.; Joshi, R.; Pai, M. Risk of tuberculosis infection and disease associated with work in health care settings [state of the art series. Occupational lung disease in high-and low-income countries, edited by M. Chan-Yeung. Number 5 in the series]. Int. J. Tuberc. Lung Dis. 2007, 11, 593–605. [Google Scholar] [PubMed]
- International Labour Organization. Occupational Injuries. Available online: https://www.ilo.org/ilostat-files/Documents/description_INJ_EN.pdf (accessed on 1 May 2022).
- Lin, L.-Y.; Warren-Gash, C.; Smeeth, L.; Chen, P.-C. Data resource profile: The national health insurance research database (NHIRD). Epidemiol. Health 2018, 40, e2018062. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Ramachandran, A.; Snehalatha, C.; Yamuna, A.; Murugesan, N. High prevalence of cardiometabolic risk factors among young physicians in India. JAPI 2008, 56, 17–20. [Google Scholar]
- Tarantola, A.; Abiteboul, D.; Rachline, A. Infection risks following accidental exposure to blood or body fluids in health care workers: A review of pathogens transmitted in published cases. Am. J. Infect. Control 2006, 34, 367–375. [Google Scholar] [CrossRef]
- Vaman, R.S.; Valamparampil, M.J.; Nair, S. Prevalence and determinants of latent tuberculosis infection among healthcare personnel in India: A scoping review. J. Patient Saf. Infect. Control 2021, 9, 35. [Google Scholar]
- Koehoorn, M.; Tamburic, L.; McLeod, C.; Demers, P. Population-based surveillance of asthma among workers in British Columbia, Canada. Chronic Dis. Inj. Can. 2013, 33, 88–94. [Google Scholar] [CrossRef]
- Jang, E.S.; Park, S.M.; Park, Y.S.; Lee, J.C.; Kim, N. Work–Life Conflict and Its Health Effects on Korean Gastroenterologists According to Age and Sex. Dig. Dis. Sci. 2020, 65, 86–95. [Google Scholar] [CrossRef]
- Liu, H.; Zou, Y.; Kan, Y.; Li, X.; Zhang, Y. Prevalence and Influencing Factors of Irritable Bowel Syndrome in Medical Staff: A Meta-Analysis. Dig. Dis. Sci. 2022, 67, 5019–5028. [Google Scholar] [CrossRef] [PubMed]
- Herwaldt, B.L.; Juranek, D.D. Laboratory-acquired malaria, leishmaniasis, trypanosomiasis, and toxoplasmosis. Am. J. Trop. Med. Hyg. 1993, 48, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Herwaldt, B.L. Laboratory-acquired parasitic infections from accidental exposures. Clin. Microbiol. Rev. 2001, 14, 659–688. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.S.; Harris, J.C.; Smith, J.L.; Washburn, J.W.; Mature, J.; Davis, A.; Crosson, J.T.; Polesky, H.; Hanson, M. Hepatitis B In ward and clinical laboratory employees of a general hospital. Am. J. Epidemiol. 1977, 106, 330–335. [Google Scholar] [CrossRef]
- Shiao, J.; Guo, L.; McLaws, M.-L. Estimation of the risk of bloodborne pathogens to health care workers after a needlestick injury in Taiwan. Am. J. Infect. Control 2002, 30, 15–20. [Google Scholar] [CrossRef]
- Mitchell, H.; Jagger, J.; Parker, G. Occupational exposures to blood and body fluid splashes and splatters: A 10-year surveillance collaborative. AOHP J. [Internet] 2015, 35, 24–38. [Google Scholar]
- Chang, R.-E.; Yu, T.-H.; Shih, C.-L. The number and composition of work hours for attending physicians in Taiwan. Sci. Rep. 2020, 10, 14934. [Google Scholar] [CrossRef]
- Christopher, A.S.; Smith, C.S.; Tivis, R.; Wilper, A.P. Trends in United States physician work hours and career satisfaction. Am. J. Med. 2014, 127, 674–680. [Google Scholar] [CrossRef]
- Davies, E. US physicians work fewer hours and see fewer patients than in 2008. BMJ: Br. Med. J. 2012, 345, e6863. [Google Scholar] [CrossRef]
- Lo, W.-Y.; Chiou, S.-T.; Huang, N.; Chien, L.-Y. Long work hours and chronic insomnia are associated with needlestick and sharps injuries among hospital nurses in Taiwan: A national survey. Int. J. Nurs. Stud. 2016, 64, 130–136. [Google Scholar] [CrossRef]
- Wu, Y.; Fujita, S.; Seto, K.; Ito, S.; Matsumoto, K.; Huang, C.-C.; Hasegawa, T. The impact of nurse working hours on patient safety culture: A cross-national survey including Japan, the United States and Chinese Taiwan using the Hospital Survey on Patient Safety Culture. BMC Health Serv. Res. 2013, 13, 394. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-Y.; Yang, C.-M.; Lien, C.-H.; Chiou, H.-Y.; Lin, M.-R.; Chang, H.-R.; Chiu, W.-T. Burnout, job satisfaction, and medical malpractice among physicians. Int. J. Med. Sci. 2013, 10, 1471. [Google Scholar] [CrossRef] [PubMed]
- Alduraywish, S.A.; Altamimi, L.A.; Aldhuwayhi, R.A.; AlZamil, L.R.; Alzeghayer, L.Y.; Alsaleh, F.S.; Aldakheel, F.M.; Tharkar, S. Sources of health information and their impacts on medical knowledge perception among the Saudi Arabian population: Cross-sectional study. J. Med. Internet Res. 2020, 22, e14414. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).