






COVID-19 Incidence and Death Rates in the Southern Region of the United States: A Racial and Ethnic Association


Abstract
1. Introduction
2. Materials and Methods
2.1. GIS Mapping
2.2. Study Area for the GIS Map
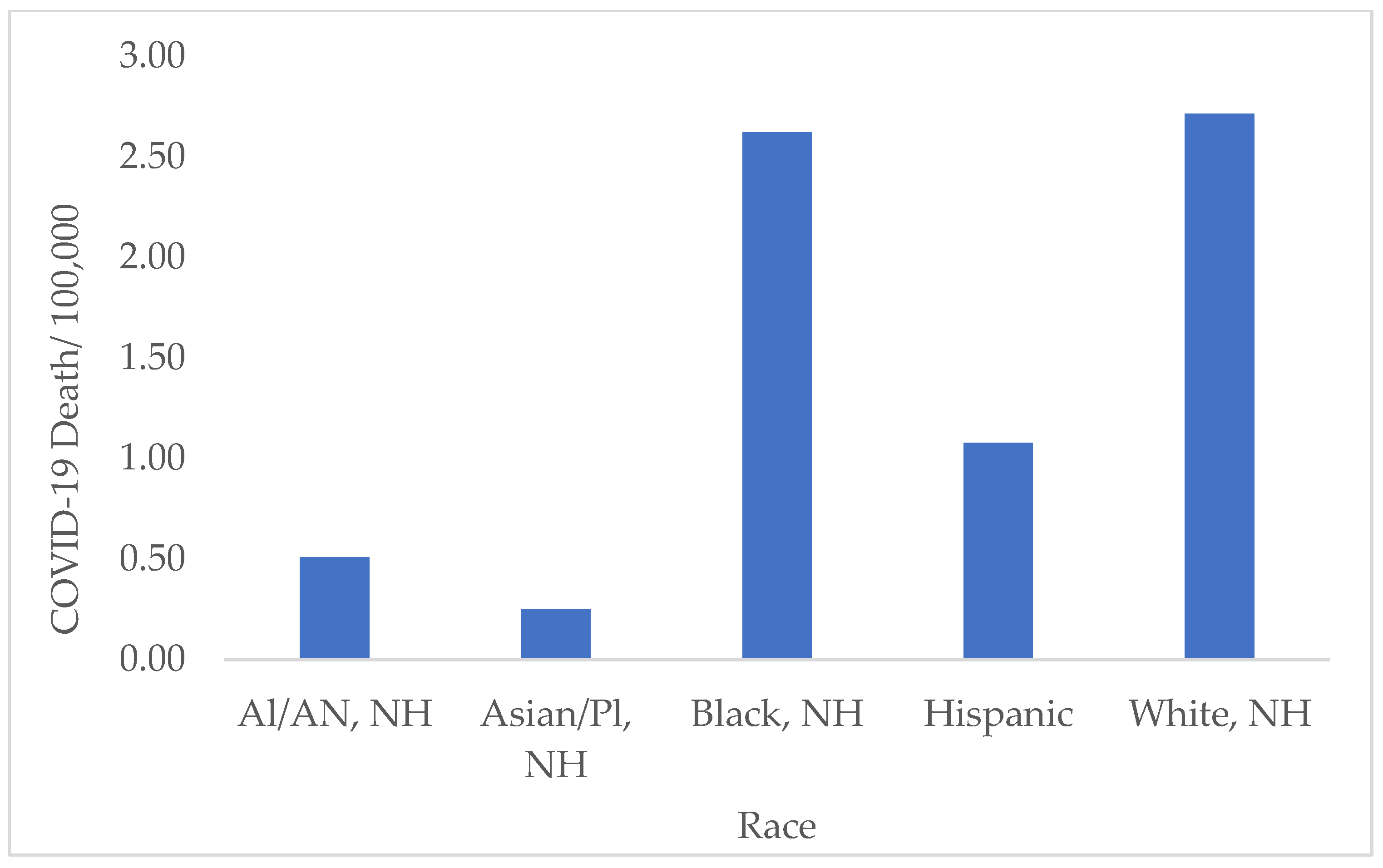
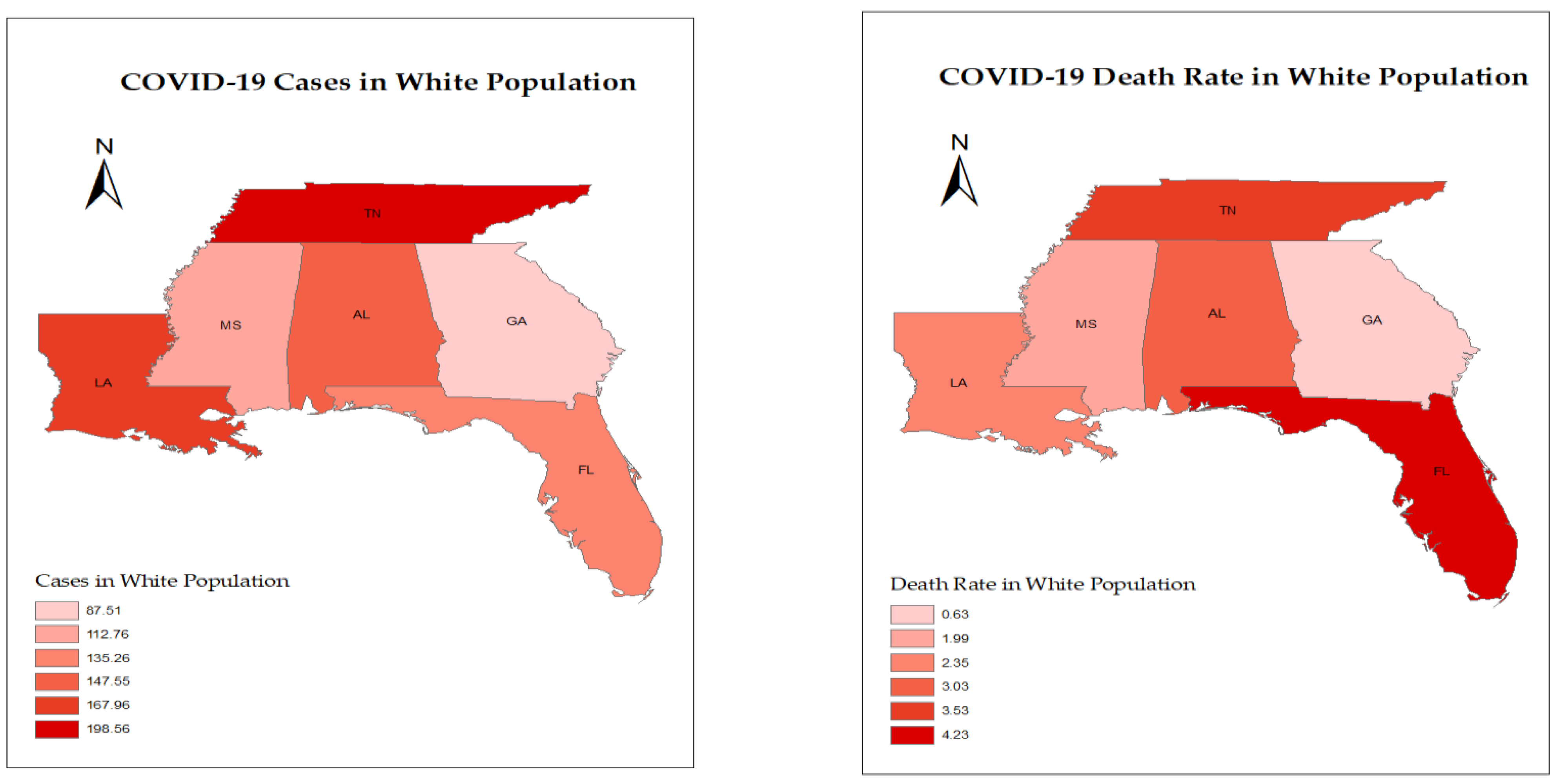
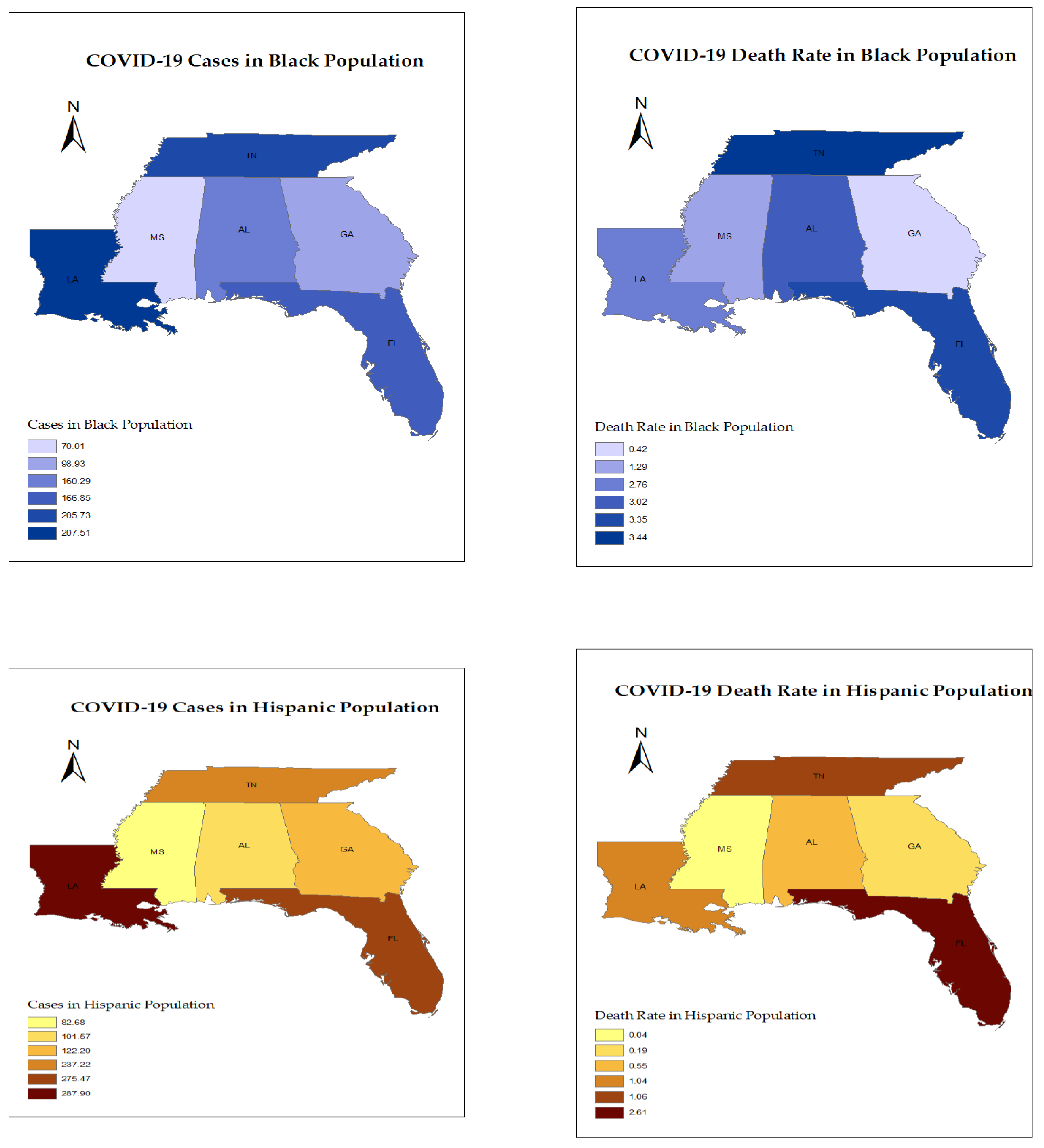
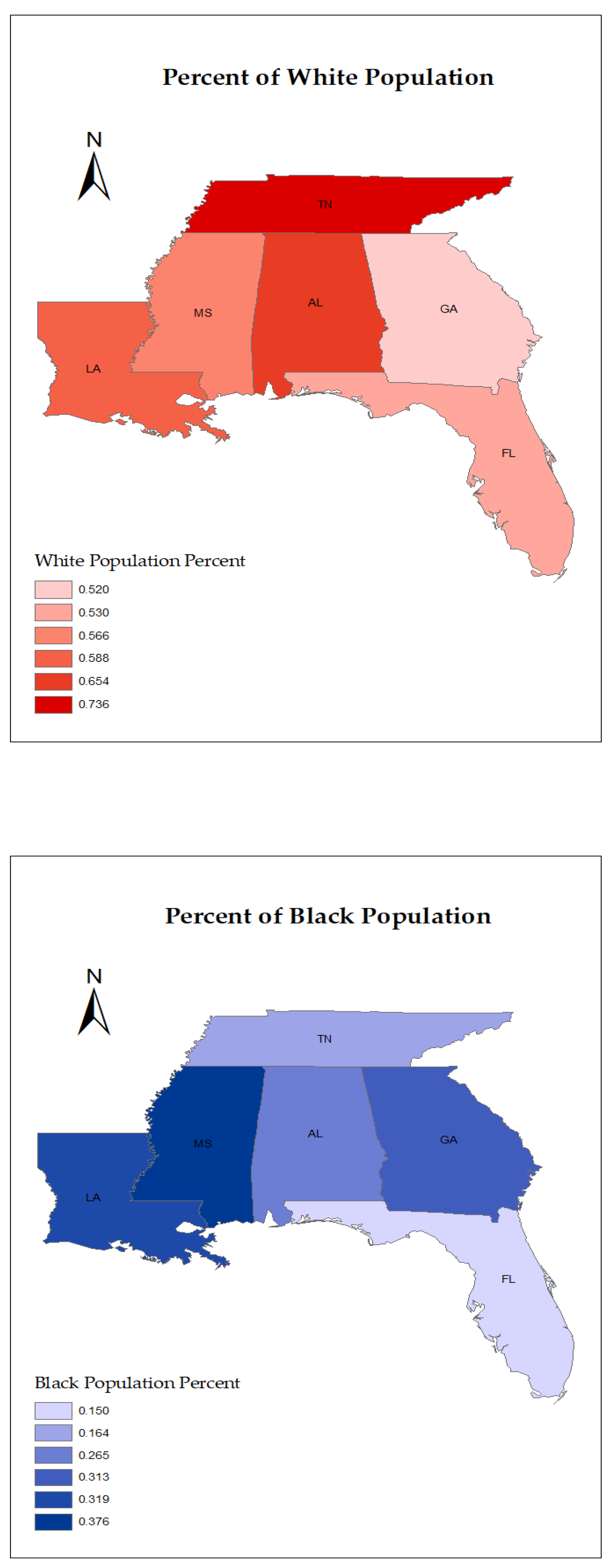
3. Results
4. Discussion
5. Conclusions
6. Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus COVID-19 Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 30 March 2022).
- The Centers for Disease Control and Prevention. COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/index.html (accessed on 30 March 2022).
- The Centers for Disease Control and Prevention. Underlying Medical Conditions. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clincial-care/underlyingconditions.html (accessed on 30 March 2022).
- Pei, S.; Yamana, T.K.; Kandula, S. Burden and characteristics of COVID-19 in the United States during 2020. Nature 2021, 598, 338–341. Available online: https://www.nature.com/articles/s41586-021-03914-4 (accessed on 10 March 2022). [CrossRef]
- Brzezinski, A.; Kecht, V.; Van Dijcke, D. Science skepticism reduced compliance with COVID-19 shelter-in-place policies in the United States. Nat. Hum. Behav. 2021, 5, 1519–1527. [Google Scholar] [CrossRef]
- Cheng, K.J.G.; Sun, Y.; Monnat, S.M. COVID-19 death rates are higher in rural counties with larger shares of blacks and Hispanics. J. Rural. Health 2020, 36, 602–608. [Google Scholar] [CrossRef]
- Artiga, S.; Damico, A. Health and Health Coverage in the South: A Data Update. Kaiser Family Foundation, 2016. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-and-health-coverage-in-the-south-a-data-update/ (accessed on 15 February 2022).
- The United States Census Bureau. 2020 U.S. Population More Racially and Ethnically Diverse Than Measured in 2010. Available online: https://www.census.gov/library/stories/2021/08/2020-united-states-population-more-racially-ethnically-diverse-than-2010.html (accessed on 25 May 2022).
- Mathur, R.; Rentsch, C.T.; Morton, C.E.; Hulme, W.J.; Schultze, A.; MacKenna, B.; Eggo, R.M.; Bhaskaran, K.; Wong, A.Y.S.; Williamson, E.J.; et al. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: An observational cohort study using the Open Safely platform. Lancet 2021, 397, 1711–1724. [Google Scholar] [CrossRef]
- Rentsch, C.T.; Kidwai-Khan, F.; Tate, J.P.; Park, L.S.; King, J.T., Jr.; Skanderson, M.; Justice, A.C. Patterns of COVID-19 testing and mortality by race and ethnicity among United States veterans: A nationwide cohort study. PLoS Med. 2020, 17, e1003379. [Google Scholar] [CrossRef]
- Figueroa, J.F.; Wadhera, R.K.; Mehtsun, W.T.; Riley, K.; Phelan, J.; Jha, A.K. Association of race, ethnicity, and community-level factors with COVID-19 cases and deaths across US counties. In Healthcare; Elsevier: Amsterdam, The Netherlands, 2021; Volume 9, p. 100495. [Google Scholar]
- Athavale, P.; Kumar, V.; Clark, J.; Mondal, S.; Sur, S. Differential impact of COVID-19 risk factors on ethnicities in the United States. Front. Public Health 2021, 9, 743003. [Google Scholar] [CrossRef]
- Hooper, M.W.; Nápoles, A.M.; Pérez-Stable, E.J. COVID-19 and racial/ethnic disparities. JAMA 2020, 323, 2466–2467. [Google Scholar] [CrossRef] [PubMed]
- Abedi, V.; Olulana, O.; Avula, V.; Chaudhary, D.; Khan, A.; Shahjouei, S.; Li, J.; Zand, R. Racial, economic, and health inequalitiy and COVID-19 infection in the United States. J. Racial Ethn. Health Disparities 2020, 8, 732–742. [Google Scholar] [CrossRef] [PubMed]
- Khazanchi, R.; Beiter, E.R.; Gondi, S.; Beckman, A.L.; Bilinski, A.; Ganguli, I. County-Level Association of Social Vulnerability with COVID-19 Cases and Deaths in the USA. J. Gen. Intern. Med. 2020, 35, 2784–2787. [Google Scholar] [CrossRef] [PubMed]
- Dobin, D.; Dobin, A. Racial/ethnic and socioeconomic disparities of COVID-19 attacks rates in Suffolk County communities. arXiv 2020, arXiv:2004.12175. [Google Scholar] [CrossRef]
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Kansagara, D. Racial and ethnic disparities in COVID-19—Related infections, hospitalizations, and deaths: A systematic review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef]
- Goyal, M.K.; Simpson, J.N.; Boyle, M.D.; Badolato, G.M.; Delaney, M.; McCarter, R.; Cora-Bramble, D. Racial and/or ethnic and socioeconomic disparities of SARS-CoV-2 infection among children. Pediatrics 2020, 146, e2020009951. [Google Scholar] [CrossRef]
- The Centers for Disease Control and Prevention. CDC-COVID-19 Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 18 March 2022).
- The Centers for Disease Control and Prevention. COVID-19 Weekly Cases and Deaths per 100,000 Population by Age, Race/Ethnicity, and Sex. Available online: https://covid.cdc.gov/covid-data-tracker/#demographicsovertime (accessed on 18 March 2022).
- Mississippi State Department of Health. Mississippi COVID-19 Cases and Deaths by County Reports. Available online: https://msdh.ms.gov/msdhsite/_static/14,0,420,884.html#page_end (accessed on 5 October 2022).
- United States Census Bureau. Quick Facts. United States. Available online: https://www.census.gov/quickfacts/fact/table/US/RHI225219 (accessed on 29 September 2022).
- Bureau of Labor Statistics. Economic News Release, State Employment and Unemployment. Available online: https://www.bls.gov/web/laus/laumstrk.htm (accessed on 5 October 2022).
- U.S. Department of Agriculture, Economic Research Service. Available online: https://data.ers.usda.gov/reports.aspx?ID=17829 (accessed on 5 October 2022).
- Health Insurance Coverage of the Total Population, 2019. Kaiser Family Foundation. Available online: https://www.kff.org/other/state-indicator/total-population/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed on 2 October 2022).
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0; IBM Corp: Armonk, NY, USA, 2022.
- ESRI. ArcGIS Desktop Application, Version 10.8.2; ESRI: Redlands, CA, USA, 2022.
- Mississippi: State-by-State COVID-19 Guidance, Mississippi. Husch Blackwell. Available online: https://www.huschblackwell.com/mississippi-state-by-state-covid-19-guidance (accessed on 15 February 2022).
- T.N. Office of the Governor. COVID-19 Timeline. Available online: https://www.tn.gov/governor/covid-19/covid19timeline.html (accessed on 15 February 2022).
- Documenting Alabama’s Path to Recovery from the Coronavirus (COVID-19) Pandemic, 2020–2021 Ballotpedia. Available online: https://ballotpedia.org/Documenting_Alabama%27s_path_to_recovery_from_the_coronavirus_(COVID-19)_pandemic,_2020-202 (accessed on 15 February 2022).
- Documenting Florida’s Path to Recovery from the Coronavirus (COVID-19) Pandemic, 2020–2021—Ballotpedia. Available online: https://ballotpedia.org/Documenting_Florida%27s_path_to_recovery_from_the_coronavirus_(COVID-19)_pandemic,_2020-2021 (accessed on 15 February 2022).
- Documenting Georgia’s Path to Recovery from the Coronavirus (COVID-19) Pandemic, 2020–2021. Available online: https://ballotpedia.org/Documenting_Georgia%27s_path_to_recovery_from_the_coronavirus_(COVID-19)_pandemic,_2020-2021 (accessed on 15 February 2022).
- Documenting Louisiana’s Path to Recovery from the Coronavirus (COVID-19) Pandemic, 2020–2021. Available online: https://ballotpedia.org/Documenting_Louisiana%27s_path_to_recovery_from_the_coronavirus_(COVID-19)_pandemic,_2020-2021 (accessed on 15 February 2022).
- KFF Estimates Based on the 2008–2019 American Community Survey, 1-Year Estimates. Available online: https://www.kff.org/other/state-indicator/distribution-by-age/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed on 15 February 2022).
- Gelfand, M.; Li, R.; Stamkou, E.; Pieper, D.; Denison, E.; Fernandez, J.; Choi, V.; Chatman, J.; Jackson, J.; Dimant, E. Persuading republicans and democrats to comply with mask wearing: An intervention tournament. J. Exp. Soc. Psychol. 2022, 101, 104299. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Marmo-Roman, S.; Krase, K.; Phanord, L. Compliance with preventative measures during the COVID-19 pandemic in the USA and Canada: Results from an online survey. Soc. Work. Health Care 2021, 60, 240–255. [Google Scholar] [CrossRef]
- Nov, O.; Dove, G.; Balestra, M. Preferences and patterns of response to public health advice during the COVID-19 pandemic. Sci. Rep. 2021, 11, 21700. [Google Scholar] [CrossRef]
- Biswas, M.; Rahaman, S.; Biswas, T.K.; Haque, Z.; Ibrahim, B. Association of sex, age, and comorbidities with mortality in COVID-19 patients: A systematic review and meta-analysis. Intervirology 2021, 64, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Bubar, K.M.; Reinholt, K.; Kissler, S.M.; Lipsitch, M.; Cobey, S.; Grad, Y.H.; Larremore, D.B. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. Science 2021, 371, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Paul, A.; Englert, P.; Varga, M. Socioeconomic disparities and COVID-19 in the USA. J. Phys. Complex. 2021, 2, 035017. [Google Scholar] [CrossRef]
- Quan, D.; Luna Wong, L.; Shallal, A.; Madan, R.; Hamdan, A.; Ahdi, H.; Zervos, M. Impact of race and socioeconomic status on outcomes in patients hospitalized with COVID-19. J. Gen. Intern. Med. 2021, 36, 1302–1309. [Google Scholar] [CrossRef]
- The US Census Bureau’s World Population Review. Available online: https://worldpopulationreview.com/states/states-by-race (accessed on 2 October 2022).
- Rodriguez, F.; Solomon, N.; De Lemos, J.A.; Das, S.R.; Morrow, D.A.; Bradley, S.M.; Wang, T.Y. Racial and ethnic differences in presentation and outcomes for patients hospitalized with COVID-19: Findings from the American Heart Association’s COVID-19 Cardiovascular Disease Registry. Circulation 2021, 143, 2332–2342. [Google Scholar] [CrossRef]
- Price-Haywood, E.G.; Burton, J.; Fort, D.; Seoane, L. Hospitalization and mortality among black patients and white patients with COVID-19. N. Engl. J. Med. 2020, 382, 2534–2543. [Google Scholar] [CrossRef] [PubMed]
- Kanjilal, S.; Gregg, E.W.; Cheng, Y.J.; Zhang, P.; Nelson, D.E.; Mensah, G.; Beckles, G.L. Socioeconomic status and trends in disparities in 4 major risk factors for cardiovascular disease among US adults, 1971–2002. Arch. Intern. Med. 2006, 166, 2348–2355. [Google Scholar] [CrossRef]
- Mueller, J.T.; McConnell, K.; Burow, P.B.; Pofahl, K.; Merdjanoff, A.A.; Farrell, J. Impacts of the COVID-19 pandemic on rural America. Proc. Natl. Acad. Sci. USA 2021, 118, 2019378118. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, A.; Khavarian-Garmsir, A.R. The COVID-19 pandemic: Impacts on cities and major lessons for urban planning, design, and management. Sci. Total Environ. 2020, 749, 142391. [Google Scholar] [CrossRef] [PubMed]
- Tirupathi, R.; Muradova, V.; Shekhar, R.; Salim, S.A.; Al-Tawfiq, J.A.; Palabindala, V. COVID-19 disparity among racial and ethnic minorities in the U.S.: A cross sectional analysis. Travel Med. Infect. Dis. 2020, 38, 101904. [Google Scholar] [CrossRef]
- Drefahl, S.; Wallace, M.; Mussino, E.; Aradhya, S.; Kolk, M.; Brandén, M.; Andersson, G. A population-based cohort study of socio-demographic risk factors for COVID-19 deaths in Sweden. Nat. Commun. 2020, 11, 5097. [Google Scholar] [CrossRef] [PubMed]
- Health Care Access Ranking, Measuring Affordability and Access of Health Care in the States, US News. Available online: https://www.usnews.com/news/best-states/rankings/health-care/healthcare-access (accessed on 10 October 2022).
- Germain, S.; Yong, A. COVID-19 Highlighting Inequalities in Access to Healthcare in England: A Case Study of Ethnic Minority and Migrant Women. Fem. Leg. Stud. 2020, 28, 301–310. [Google Scholar] [CrossRef]
- Patel, J.A.; Nielsen, F.B.H.; Badiani, A.A.; Assi, S.; Unadkat, V.A.; Patel, B.; Wardle, H. Poverty, inequality and COVID-19: The forgotten vulnerable. Public Health 2020, 183, 110. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| State | Sex | Weekly Average Cases/100,000 | STD | Average 7 Day Death Rate/100,000 | STD |
|---|---|---|---|---|---|
| AL | Female | 256.31 | 333.01 | 3.10 | 2.84 |
| Male | 212.86 | 263.53 | 3.84 | 3.55 | |
| FL | Female | 151.28 | 143.18 | 8.49 | 42.17 |
| Male | 138.92 | 131.39 | 3.64 | 3.18 | |
| GA | Female | 203.62 | 256.70 | 0.49 | 0.62 |
| Male | 170.83 | 205.52 | 0.65 | 0.81 | |
| LA | Female | 260.02 | 350.32 | 2.73 | 2.38 |
| Male | 217.18 | 280.32 | 8.48 | 45.94 | |
| MS | Female | 49.73 | 46.48 | 3.43 | 6.72 |
| Male | 39.27 | 37.19 | 3.06 | 3.73 | |
| TN | Female | 297.92 | 381.62 | 15.03 | 113.93 |
| Male | 275.31 | 334.54 | 4.57 | 7.52 |
| State | Age Group | 0–4 | 5–11 | 12–15 | 16–17 | 18–29 | 30–39 | 40–49 | 50–64 | 65–74 | 75+ |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AL | Cases/100,000 | 62.22 | 74.05 | 107.95 | 138.87 | 147.46 | 137.98 | 136.19 | 117.57 | 99.85 | 113.45 |
| Death/100,00 | 0.05 | 0.00 | 0.00 | 0.04 | 0.15 | 0.56 | 1.50 | 3.86 | 8.64 | 21.69 | |
| FL | Cases/100,000 | 73.89 | 113.86 | 135.57 | 159.39 | 195.85 | 197.06 | 180.72 | 143.73 | 97.82 | 93.87 |
| Death/100,00 | 0.02 | 0.01 | 0.02 | 0.06 | 0.21 | 0.48 | 1.55 | 2.84 | 6.10 | 18.88 | |
| GA | Cases/100,000 | 89.87 | 130.85 | 175.11 | 204.33 | 235.33 | 235.47 | 219.38 | 184.80 | 137.23 | 139.09 |
| Death/100,000 | 0.01 | 0.00 | 0.01 | 0.01 | 0.04 | 0.12 | 0.28 | 1.16 | 1.71 | 4.01 | |
| LA | Cases/100,000 | 138.91 | 163.21 | 231.03 | 269.25 | 296.22 | 291.24 | 288.64 | 232.59 | 193.25 | 186.67 |
| Death/100,000 | 0.01 | 0.00 | 0.02 | 0.02 | 0.13 | 0.47 | 1.17 | 3.17 | 7.82 | 21.73 | |
| MS | Cases/100,000 | 14.44 | 13.33 | 21.70 | 37.19 | 57.95 | 54.11 | 56.52 | 48.47 | 42.51 | 61.24 |
| Death/100,000 | 0.02 | 0.00 | 0.00 | 0.00 | 0.08 | 0.30 | 0.67 | 2.12 | 5.29 | 15.21 | |
| TN | Cases/100,000 | 167.57 | 221.72 | 288.37 | 338.63 | 359.13 | 350.86 | 324.70 | 270.07 | 208.07 | 200.42 |
| Death/100,000 | 0.03 | 0.01 | 0.02 | 0.03 | 0.15 | 0.56 | 1.40 | 3.79 | 8.84 | 23.75 |
| State | Race | COVID-19 7-Day Average | Standard Deviation | COVID-19 7-Day Average Death | Standard Deviation |
|---|---|---|---|---|---|
| AL | Al/AN, NH | 91.82 | 203.43 | 0.00 | 0.00 |
| Asian/Pl, NH | 99.34 | 207.20 | 0.00 | 0.00 | |
| Black, NH | 160.29 | 250.28 | 3.02 | 2.51 | |
| Hispanic | 101.57 | 86.56 | 0.55 | 1.34 | |
| White, NH | 147.55 | 212.00 | 3.03 | 2.73 | |
| FL | Al/AN, NH | 102.91 | 109.98 | 0.11 | 1.09 |
| Asian/Pl, NH | 109.35 | 123.70 | 0.94 | 1.32 | |
| Black, NH | 166.85 | 156.22 | 3.35 | 3.29 | |
| Hispanic | 275.47 | 407.00 | 2.61 | 2.22 | |
| White, NH | 135.26 | 125.25 | 4.23 | 9.80 | |
| GA | Al/AN, NH | 61.03 | 96.55 | 0.00 | 0.00 |
| Asian/Pl, NH | 66.27 | 119.56 | 0.08 | 0.40 | |
| Black, NH | 98.93 | 151.01 | 0.42 | 0.59 | |
| Hispanic | 122.20 | 184.58 | 0.19 | 0.42 | |
| White, NH | 87.51 | 117.39 | 0.63 | 0.85 | |
| LA | Al/AN, NH | 116.18 | 158.17 | 0.00 | 0.00 |
| Asian/Pl, NH | 160.30 | 217.33 | 0.32 | 1.65 | |
| Black, NH | 207.51 | 317.59 | 2.76 | 2.85 | |
| Hispanic | 287.90 | 432.94 | 1.04 | 1.94 | |
| White, NH | 167.96 | 223.16 | 2.35 | 2.06 | |
| MS | Al/AN, NH | 2.08 | NA | 0.01 | NA |
| Asian/Pl, NH | 1.12 | NA | 0.03 | NA | |
| Black, NH | 70.01 | NA | 1.29 | NA | |
| Hispanic | 82.68 | NA | 0.04 | NA | |
| White, NH | 112.76 | NA | 1.99 | NA | |
| Unknown | 59.81 | NA | 0.53 | NA | |
| TN | Al/AN, NH | 101.01 | 142.80 | 0.00 | 0.00 |
| Asian/Pl, NH | 109.05 | 137.86 | 0.00 | 0.00 | |
| Black, NH | 205.73 | 266.96 | 3.44 | 2.79 | |
| Hispanic | 237.22 | 250.30 | 1.06 | 1.42 | |
| White, NH | 198.56 | 234.77 | 3.53 | 3.20 |
| State | Poverty Rate | Uninsured Rate | Medicaid Insurance | Unemployment | High School Education | College Education | White | Black | Hispanic | Asian | American Indian/ Alaska Native |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AL | 15.03 | 9.7 | 19.5 | 2.60 | 35.9 | 16.1 | 60.10 | 12.20 | 18.50 | 5.60 | 0.70 |
| FL | 12.56 | 13.1 | 17.4 | 2.70 | 39.2 | 15.1 | 65.40 | 26.50 | 4.40% | 1.40 | 0.40 |
| GA | 13.39 | 13.4 | 17.3 | 2.80 | 36.7 | 17.3 | 53.00 | 15.00 | 26.60 | 2.70 | 0.20 |
| LA | 19.05 | 8.9 | 29.3 | 3.50 | 40.8 | 15.4 | 52.00 | 31.30 | 9.80% | 4.10 | 0.20 |
| MS | 19.07 | 12.9 | 24.2 | 3.60 | 32.5 | 18.9 | 58.80 | 31.90 | 5.20% | 1.70 | 0.50 |
| TN | 13.74 | 10.2 | 19.5 | 3.40 | 41.7 | 16.3 | 56.60 | 37.60 | 3.00 | 1.00 | 0.40 |
| USA | 12.3 | 9.2 | 19.8 | 3.5 | 35.4 | 20.7 | 73.60 | 16.40 | 5.70 | 1.80 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akil, L.; Barner, Y.M.; Bisht, A.; Okoye, E.; Ahmad, H.A. COVID-19 Incidence and Death Rates in the Southern Region of the United States: A Racial and Ethnic Association. Int. J. Environ. Res. Public Health 2022, 19, 13990. https://doi.org/10.3390/ijerph192113990
Akil L, Barner YM, Bisht A, Okoye E, Ahmad HA. COVID-19 Incidence and Death Rates in the Southern Region of the United States: A Racial and Ethnic Association. International Journal of Environmental Research and Public Health. 2022; 19(21):13990. https://doi.org/10.3390/ijerph192113990
Chicago/Turabian StyleAkil, Luma, Yalanda M. Barner, Anamika Bisht, Ebele Okoye, and Hafiz Anwar Ahmad. 2022. "COVID-19 Incidence and Death Rates in the Southern Region of the United States: A Racial and Ethnic Association" International Journal of Environmental Research and Public Health 19, no. 21: 13990. https://doi.org/10.3390/ijerph192113990
APA StyleAkil, L., Barner, Y. M., Bisht, A., Okoye, E., & Ahmad, H. A. (2022). COVID-19 Incidence and Death Rates in the Southern Region of the United States: A Racial and Ethnic Association. International Journal of Environmental Research and Public Health, 19(21), 13990. https://doi.org/10.3390/ijerph192113990