
Kefir and the Gut–Skin Axis

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
Baseline Conditions
2.2. Kefir Intervention
2.3. Skin Measurements
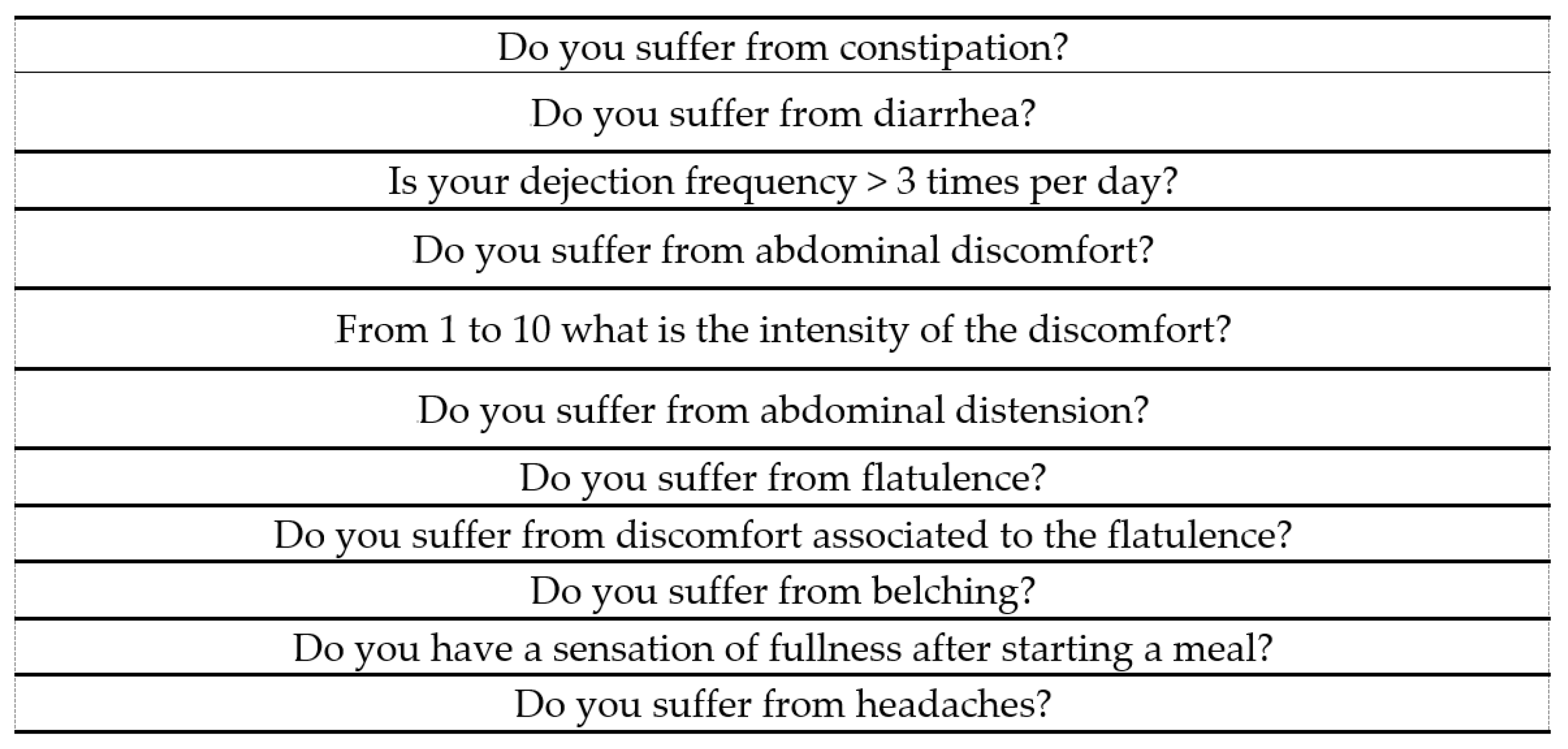
2.4. GI Status Assessment
2.5. Statistical Analysis
3. Results
3.1. GI Status Assessment
3.2. Adjusted Models for GI Status
3.3. GI Status and Modification of Skin Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, C.J.; Drossman, D.A.; Talley, N.J.; Ruddy, J.; Ford, A.C. Functional Gastrointestinal Disorders: Advances in Understanding and Management. Lancet 2020, 396, 1664–1674. [Google Scholar] [CrossRef]
- Rome Foundation Rome IV Questionnaire—Rome Foundation. Available online: https://theromefoundation.org/rome-iv/rome-iv-questionnaire/ (accessed on 22 May 2018).
- Talley, N.J. What Causes Functional Gastrointestinal Disorders? A Proposed Disease Model. Off. J. Am. Coll. Gastroenterol. ACG 2020, 115, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J. Neurogastroenterol. Motil. 2017, 23, 151–163. [Google Scholar] [CrossRef]
- Talley, N.J. Editorial: Moving Away from Focussing on Gastric Pathophysiology in Functional Dyspepsia: New Insights and Therapeutic Implications. Off. J. Am. Coll. Gastroenterol. ACG 2017, 112, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Arsiè, E.; Coletta, M.; Cesana, B.M.; Basilisco, G. Symptom-Association Probability between Meal Ingestion and Abdominal Pain in Patients with Irritable Bowel Syndrome. Does Somatization Play a Role? Neurogastroenterol. Motil. 2015, 27, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Peluzio, M.D.C.G.; Dias, M.D.M.E.; Martinez, J.A.; Milagro, F.I. Kefir and Intestinal Microbiota Modulation: Implications in Human Health. Front. Nutr. 2021, 8, 638740. [Google Scholar] [CrossRef]
- Weiss, G.A.; Hennet, T. Mechanisms and Consequences of Intestinal Dysbiosis. Cell. Mol. Life Sci. 2017, 74, 2959–2977. [Google Scholar] [CrossRef]
- Salem, I.; Ramser, A.; Isham, N.; Ghannoum, M.A. The Gut Microbiome as a Major Regulator of the Gut-Skin Axis. Front. Microbiol. 2018, 9, 1459. [Google Scholar] [CrossRef]
- Kim, J.; Kim, H. Microbiome of the Skin and Gut in Atopic Dermatitis (AD): Understanding the Pathophysiology and Finding Novel Management Strategies. J. Clin. Med. 2019, 8, 444. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Lee, E.; Park, Y.M.; Hong, S.J. Gut-Skin Axis in Atopic Dermatitis. Allergy Asthma Immunol. Res. 2018, 10, 354–362. [Google Scholar] [CrossRef]
- Simonyte Sjödin, K.; Vidman, L.; Rydén, P.; West, C.E. Emerging Evidence of the Role of Gut Microbiota in the Development of Allergic Diseases. Curr. Opin. Allergy Clin. Immunol. 2016, 16, 390–395. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, C.A.; Monteleone, G.; McLaughlin, J.T.; Paus, R. The Gut-Skin Axis in Health and Disease: A Paradigm with Therapeutic Implications. BioEssays 2016, 38, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Bellikci-Koyu, E.; Sarer-Yurekli, B.P.; Akyon, Y.; Aydin-Kose, F.; Karagozlu, C.; Ozgen, A.G.; Brinkmann, A.; Nitsche, A.; Ergunay, K.; Yilmaz, E.; et al. Effects of Regular Kefir Consumption on Gut Microbiota in Patients with Metabolic Syndrome: A Parallel-Group, Randomized, Controlled Study. Nutrients 2019, 11, 2089. [Google Scholar] [CrossRef] [PubMed]
- Stiemsma, L.T.; Nakamura, R.E.; Nguyen, J.G.; Michels, K.B. Does Consumption of Fermented Foods Modify the Human Gut Microbiota? J. Nutr. 2020, 150, 1680–1692. [Google Scholar] [CrossRef] [PubMed]
- Dimidi, E.; Cox, S.; Rossi, M.; Whelan, K. Fermented Foods: Definitions and Characteristics, Gastrointestinal Health and Disease. Nutrients 2019, 11, 1806. [Google Scholar] [CrossRef]
- Narla, S.; Silverberg, J.I. The Role of Environmental Exposures in Atopic Dermatitis. Curr. Allergy Asthma Rep. 2020, 20, 74. [Google Scholar] [CrossRef]
- Pražnikar, Z.J.; Kenig, S.; Vardjan, T.; Bizjak, M.Č.; Petelin, A. Effects of Kefir or Milk Supplementation on Zonulin in Overweight Subjects. J. Dairy Sci. 2020, 103, 3961–3970. [Google Scholar] [CrossRef]
- Wieërs, G.; Belkhir, L.; Enaud, R.; Leclercq, S.; Philippart de Foy, J.-M.; Dequenne, I.; de Timary, P.; Cani, P.D. How Probiotics Affect the Microbiota. Front. Cell. Infect. Microbiol. 2020, 9, 454. [Google Scholar] [CrossRef]
- Slattery, C.; Cotter, P.D.; O’Toole, P.W. Analysis of Health Benefits Conferred by Lactobacillus Species from Kefir. Nutrients 2019, 11, 1252. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, K.; Kanjanasuntree, R.; Kim, W. Kazachstania Turicensis CAU Y1706 Ameliorates Atopic Dermatitis by Regulation of the Gut–Skin Axis. J. Dairy Sci. 2019, 102, 2854–2862. [Google Scholar] [CrossRef]
- Bengoa, A.A.; Iraporda, C.; Garrote, G.L.; Abraham, A.G. Kefir Micro-Organisms: Their Role in Grain Assembly and Health Properties of Fermented Milk. J. Appl. Microbiol. 2019, 126, 686–700. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.J.; Huang, W.C.; Lin, J.S.; Chen, Y.M.; Ho, S.T.; Huang, C.C.; Tung, Y.T. Kefir Supplementation Modifies Gut Microbiota Composition, Reduces Physical Fatigue, and Improves Exercise Performance in Mice. Nutrients 2018, 10, 862. [Google Scholar] [CrossRef] [PubMed]
- Bekar, O.; Yilmaz, Y.; Gulten, M. Kefir Improves the Efficacy and Tolerability of Triple Therapy in Eradicating Helicobacter Pylori. J. Med. Food 2010, 14, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Maki, R.; Matsukawa, M.; Matsuduka, A.; Hashinaga, M.; Anai, H.; Yamaoka, Y.; Hanada, K.; Fujii, C. Therapeutic Effect of Lyophilized, Kefir-Fermented Milk on Constipation among Persons with Mental and Physical Disabilities. Japan J. Nurs. Sci. 2018, 15, 218–225. [Google Scholar] [CrossRef]
- Üstün-Aytekin, Ö.; Şeker, A.; Arısoy, S. The Effect of in Vitro Gastrointestinal Simulation on Bioactivities of Kefir. Int. J. Food Sci. Technol. 2020, 55, 283–292. [Google Scholar] [CrossRef]
- Kim, D.H.; Jeong, D.; Kim, H.; Seo, K.H. Modern Perspectives on the Health Benefits of Kefir in next Generation Sequencing Era: Improvement of the Host Gut Microbiota. Crit. Rev. Food Sci. Nutr. 2019, 59, 1782–1793. [Google Scholar] [CrossRef] [PubMed]
- Alves, E.; Rijo, P.; Rodrigues, L.M.; Rosado, C. Probiotics in the Gut-Skin Axis—The Case of Kefir. Biomed. Biopharm. Res. 2021, 18, 1–15. [Google Scholar] [CrossRef]
- Stefanovic, N.; Irvine, A.D.; Flohr, C. The Role of the Environment and Exposome in Atopic Dermatitis. Curr. Treat. Options Allergy 2021, 8, 222–241. [Google Scholar] [CrossRef]
- Petersen, E.B.M.; Skov, L.; Thyssen, J.P.; Jensen, P. Role of the Gut Microbiota in Atopic Dermatitis: A Systematic Review. Acta Derm. Venereol. 2018, 99, 5–11. [Google Scholar] [CrossRef]
- Lolou, V.; Panayiotidis, M.I. Functional Role of Probiotics and Prebiotics on Skin Health and Disease. Fermentation 2019, 5, 41. [Google Scholar] [CrossRef]
- Zhao, M.; Shen, C.; Ma, L. Treatment Efficacy of Probiotics on Atopic Dermatitis, Zooming in on Infants: A Systematic Review and Meta-Analysis. Int. J. Dermatol. 2018, 57, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.S.; Trivedi, M.K.; Jha, A.; Lin, Y.F.; Dimaano, L.; García-Romero, M.T. Synbiotics for Prevention and Treatment of Atopic Dermatitis: A Meta-Analysis of Randomized Clinical Trials. JAMA Pediatr. 2016, 170, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Beam, A.; Clinger, E.; Hao, L. Effect of Diet and Dietary Components on the Composition of the Gut Microbiota. Nutrients 2021, 13, 2795. [Google Scholar] [CrossRef] [PubMed]
- Alves, E.; Gregório, J.; Baby, A.R.; Rijo, P.; Rodrigues, L.M.; Rosado, C. Homemade Kefir Consumption Improves Skin Condition—A Study Conducted in Healthy and Atopic Volunteers. Foods 2021, 10, 2794. [Google Scholar] [CrossRef]
- Saito, Y.; Mihara, T.; Maruyama, K.; Saito, J.; Ikeda, M.; Tomonaga, A.; Kumagai, T. Effects of Intake of Lactobacillus Casei Subsp. Casei 327 on Skin Conditions: A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study in Women. Biosci. Microbiota Food Health 2017, 36, 111–120. [Google Scholar] [CrossRef]
- Matsumoto, M.; Ebata, T.; Hirooka, J.; Hosoya, R.; Inoue, N.; Itami, S.; Tsuji, K.; Yaginuma, T.; Muramatsu, K.; Nakamura, A.; et al. Antipruritic Effects of the Probiotic Strain LKM512 in Adults with Atopic Dermatitis. Ann. Allergy Asthma Immunol. 2014, 113, 209–216. [Google Scholar] [CrossRef]
- Ogawa, M.; Saiki, A.; Matsui, Y.; Tsuchimoto, N.; Nakakita, Y.; Takata, Y.; Nakamura, T. Effects of Oral Intake of Heat-Killed Lactobacillus Brevis SBC8803 (SBL88TM) on Dry Skin Conditions: A Randomized, Double-Blind, Placebo-Controlled Study. Exp. Ther. Med. 2016, 12, 3863–3872. [Google Scholar] [CrossRef]
- Yoshida, Y.; Seki, T.; Matsunaka, H.; Watanabe, T.; Shindo, M.; Yamada, N.; Yamamoto, O. Clinical Effects of Probiotic Bifidobacterium Breve Supplementation in Adult Patients with Atopic Dermatitis. Yonago Acta Med. 2010, 53, 37–45. [Google Scholar]
- Roessler, A.; Friedrich, U.; Vogelsang, H.; Bauer, A.; Kaatz, M.; Hipler, U.C.; Schmidt, I.; Jahreis, G. The Immune System in Healthy Adults and Patients with Atopic Dermatitis Seems to Be Affected Differently by a Probiotic Intervention. Clin. Exp. Allergy 2008, 38, 93–102. [Google Scholar] [CrossRef]
- Instituto Portugês do Mar e da Atmosfera—IPMA Clima de Portugal Continental. Available online: https://www.ipma.pt/pt/educativa/tempo.clima/ (accessed on 10 February 2021).
- Alves, E.; Ntungwe, E.N.; Gregório, J.; Rodrigues, L.M.; Pereira-Leite, C.; Caleja, C.; Pereira, E.; Barros, L.; Aguilar-Vilas, M.V.; Rosado, C.; et al. Characterization of Kefir Produced in Household Conditions: Physicochemical and Nutritional Profile, and Storage Stability. Foods 2021, 10, 1057. [Google Scholar] [CrossRef]
- Nantes; Bordeaux. Severity Scoring of Atopic Dermatitis: The SCORAD Index. Dermatology 1993, 186, 23–31. [Google Scholar] [CrossRef]
- Oranje, A.P. Practical Issues on Interpretation of Scoring Atopic Dermatitis: SCORAD Index, Objective SCORAD, Patient-Oriented SCORAD and Three-Item Severity Score. Curr. Probl. Dermatol. 2011, 41, 149–155. [Google Scholar] [CrossRef]
- Healey, G.R.; Murphy, R.; Brough, L.; Butts, C.A.; Coad, J. Interindividual Variability in Gut Microbiota and Host Response to Dietary Interventions. Nutr. Rev. 2017, 75, 1059–1080. [Google Scholar] [CrossRef] [PubMed]
- Soenen, S.; Rayner, C.K.; Jones, K.L.; Horowitz, M. The Ageing Gastrointestinal Tract. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Hertzler, S.R.; Clancy, S.M. Kefir Improves Lactose Digestion and Tolerance in Adults with Lactose Maldigestion. J. Am. Diet. Assoc. 2003, 103, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Turan, I.; Dedeli, O.; Bor, S.; Ilter, T. Effects of a Kefir Supplement on Symptoms, Colonic Transit, and Bowel Satisfaction Score in Patients with Chronic Constipation: A Pilot Study. Turkish J. Gastroenterol. 2014, 25, 650–656. [Google Scholar] [CrossRef]
- St-Onge, M.-P.; Farnworth, E.R.; Savard, T.; Chabot, D.; Mafu, A.; Jones, P.J.H. Kefir Consumption Does Not Alter Plasma Lipid Levels or Cholesterol Fractional Synthesis Rates Relative to Milk in Hyperlipidemic Men: A Randomized Controlled Trial [ISRCTN10820810]. BMC Complement. Altern. Med. 2002, 2, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ellis, S.R.; Nguyen, M.; Vaughn, A.R.; Notay, M.; Burney, W.A.; Sandhu, S.; Sivamani, R.K. The Skin and Gut Microbiome and Its Role in Common Dermatologic Conditions. Microorganisms 2019, 7, 550. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Lu, W.; Zhao, J.; Zhang, H.; Qian, L.; Wang, Q.; Chen, W. Probiotics Modulate the Gut Microbiota Composition and Immune Responses in Patients with Atopic Dermatitis: A Pilot Study. Eur. J. Nutr. 2020, 59, 2119–2130. [Google Scholar] [CrossRef]
- Kim, S.O.; Ah, Y.M.; Yu, Y.M.; Choi, K.H.; Shin, W.G.; Lee, J.Y. Effects of Probiotics for the Treatment of Atopic Dermatitis: A Meta-Analysis of Randomized Controlled Trials. Ann. Allergy Asthma Immunol. 2014, 113, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Möller, H.-J. Effectiveness Studies: Advantages and Disadvantages. Dialogues Clin. Neurosci. 2011, 13, 199–207. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, P.; Slaets, J.P.J. Response Sets in Self-Report Data and Their Associations with Personality Traits. Eur. J. Psychiatry 2005, 19, 209–214. [Google Scholar] [CrossRef]
- Althubaiti, A. Information Bias in Health Research: Definition, Pitfalls, and Adjustment Methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Farag, M.; Jomaa, S.; El-Wahed, A.; El-Seedi, H. The Many Faces of Kefir Fermented Dairy Products: Quality Characteristics, Flavour Chemistry, Nutritional Value, Health Benefits, and Safety. Nutrients 2020, 12, 346. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Improved GI Status | Healthy Group (n = 33) | Atopic Group (n = 19) | ||||
|---|---|---|---|---|---|---|
| HK | H0 | p-Value | AK | A0 | p-Value | |
| Functional constipation, % (n) | 38.5 (5) | 0.0 (0) | 0.003 | 55.6 (5) | 10.0 (1) | 0.033 |
| Functional diarrhea, % (n) | 30.8 (4) | 0.0 (0) | 0.008 | 11.1 (1) | 20.0 (2) | 0.596 |
| Dejection frequency > 3 times per day, % (n) | 23.1 (3) | 0.0 (0) | 0.024 | 22.2 (2) | 20.0 (2) | 0.906 |
| Intensity of abdominal discomfort ≥ 5, % (n) | 30.8 (4) | 0.0 (0) | 0.008 | 55.6 (5) | 30.0 (3) | 0.260 |
| Functional abdominal distension, % (n) | 53.8 (7) | 0.0 (0) | <0.001 | 66.7 (6) | 20.0 (2) | 0.040 |
| Flatulence frequency, % (n) | 38.5 (5) | 10.0 (2) | 0.051 | 55.6 (5) | 40.0 (4) | 0.498 |
| Associated discomfort, % (n) | 23.1 (3) | 0.0 (0) | 0.024 | 77.8 (7) | 60.0 (6) | 0.405 |
| Belching, % (n) | 15.4 (2) | 0.0 (0) | 0.070 | 44.4 (4) | 20.0 (2) | 0.252 |
| Fullness sensation, % (n) | n.a. | n.a. | -- | 22.2 (2) | 30.0 (3) | 0.701 |
| Headache, % (n) | 30.8 (4) | 0 | 0.008 | 33.3 (3) | 20.0 (2) | 0.510 |
| Improved GI Status | Odds Ratio (p-Value) | ||
|---|---|---|---|
| Crude OR | aOR1 | aOR2 | |
| Functional constipation | 24.17 (0.004) | 33.93 (0.003) | 32.22 (0.003) |
| Functional diarrhea | 4.118 (0.112) | 3.901 (0.138) | 4.150 (0.128) |
| Dejection frequency > 3 times per day | 4.118 (0.112) | 3.869 (0.137) | 3.868 (0.137) |
| Intensity of abdominal discomfort ≥ 5 | 6.231 (0.014) | 6.208 (0.015) | 6.153 (0.016) |
| Functional abdominal distension | 20.22 (<0.001) | 27.74 (<0.001) | 30.29 (<0.001) |
| Flatulence frequency | 3.333 (0.054) | 3.326 (0.056) | 3.994 (0.040) |
| Associated discomfort | 3.333 (0.054) | 3.321 (0.056) | 3.446 (0.052) |
| Belching | 5.250 (0.058) | 6.103 (0.046) | 8.125 (0.033) |
| Fullness sensation | 0.900 (0.913) | 0.920 (0.931) | 0.836 (0.854) |
| Headache | 6.533 (0.030) | 6.719 (0.028) | 6.635 (0.031) |
| Modification of Skin Parameters | Improved GI Status | |||||
|---|---|---|---|---|---|---|
| Functional Constipation | Functional Diarrhea | Dejection Frequency > 3 Times per Day | Intensity of Abdominal Discomfort ≥ 5 | Functional Abdominal Distension | Discomfort Associated to Flatulence | |
| TEWL, n (%) | ||||||
| Forearm | 10 (45.4%) (0.644) | 5 (22.7%) (0.557) | 5 (22.7%) (0.906) | 9 (40.9%) (0.301) | 13 (59.1 %) (0.271) | 10 (45.4 %) (0.235) |
| Forehead | 10 (45.4%) (0.510) | 5 (22.7%) (0.327) | 5 (22.7%) (0.225) | 9 (40.9%) (0.271) | 13 (59.1 %) (0.815) | 10 (45.4 %) (0.041) |
| Forearm Hydration, n (%) | 10 (45.4%) (0.668) | 5 (22.7%) (0.038) | 5 (22.7%) (0.196) | 9 (40.9%) (0.894) | 13 (59.1 %) (0.229) | 10 (45.4 %) (0.070) |
| SCORAD Index O, n (%) | 5 (55.6%) (1.000) | 1 (11.1%) (0.439) | 2 (22.2%) (0.558) | 5 (55.6%) (0.327) | 6 (66.7%) (0.197) | 7 (77.8%) (0.380) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves, E.; Gregório, J.; Rijo, P.; Rosado, C.; Monteiro Rodrigues, L. Kefir and the Gut–Skin Axis. Int. J. Environ. Res. Public Health 2022, 19, 13791. https://doi.org/10.3390/ijerph192113791
Alves E, Gregório J, Rijo P, Rosado C, Monteiro Rodrigues L. Kefir and the Gut–Skin Axis. International Journal of Environmental Research and Public Health. 2022; 19(21):13791. https://doi.org/10.3390/ijerph192113791
Chicago/Turabian StyleAlves, Emília, João Gregório, Patrícia Rijo, Catarina Rosado, and Luis Monteiro Rodrigues. 2022. "Kefir and the Gut–Skin Axis" International Journal of Environmental Research and Public Health 19, no. 21: 13791. https://doi.org/10.3390/ijerph192113791
APA StyleAlves, E., Gregório, J., Rijo, P., Rosado, C., & Monteiro Rodrigues, L. (2022). Kefir and the Gut–Skin Axis. International Journal of Environmental Research and Public Health, 19(21), 13791. https://doi.org/10.3390/ijerph192113791