

Examining the Relationship between Death Anxiety and Well-Being of Frontline Medical Staff during the COVID-19 Pandemic
Abstract
1. Introduction
1.1. Hedonic and Eudaimonic Well-Being
1.2. Death Anxiety and Well-Being among Medical Staff during the COVID-19 Pandemic
1.3. The Role of the Narcissistic Personality
2. Materials and Methods
2.1. Data Collection and Sample
2.2. Measurement
2.2.1. Death Anxiety
2.2.2. Hedonic Well-Being
2.2.3. Eudaimonic Well-Being
2.2.4. Narcissistic Personality
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
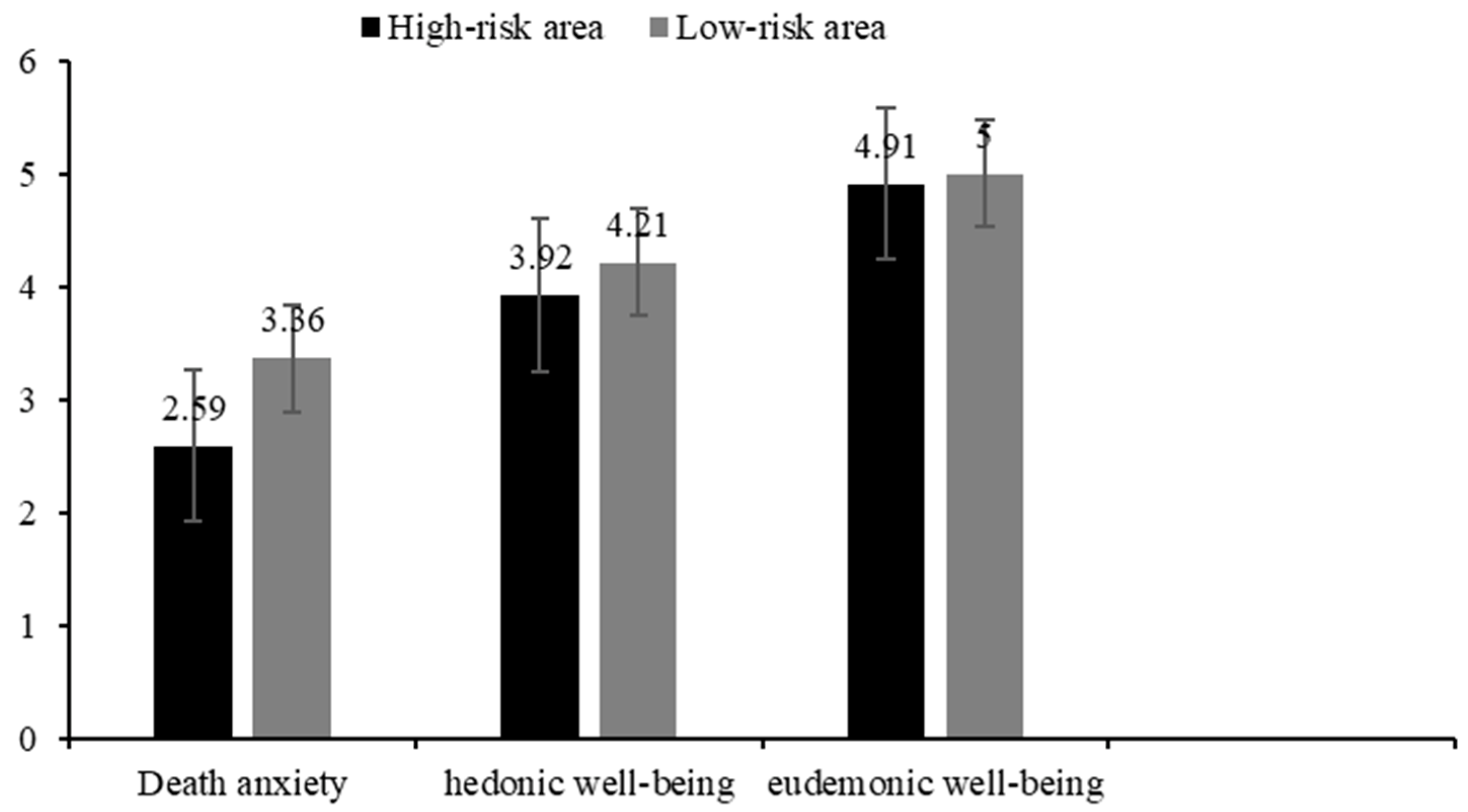
3.2. The Life Profiles of Medical Staff during the COVID-19 Pandemic
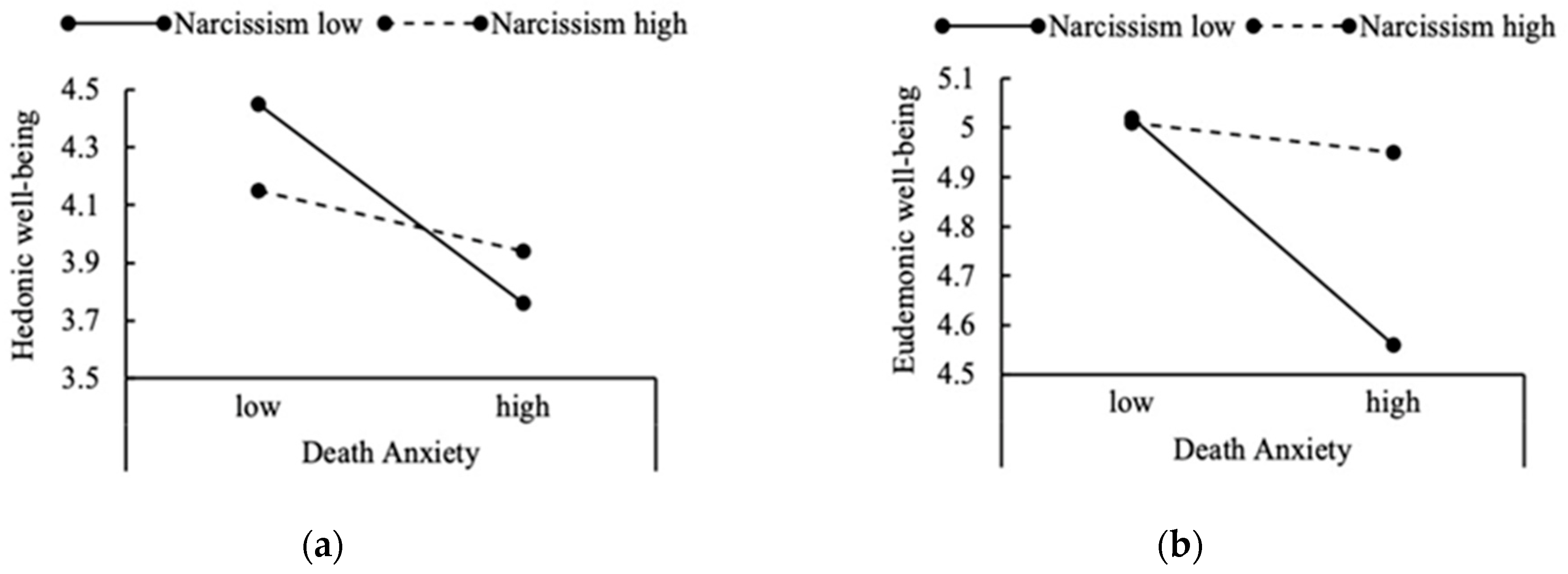
3.3. The Relationship between Death Anxiety, Narcissistic Personality, and Well-Being
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef]
- Menzies, R.E.; Neimeyer, R.A.; Menzies, R.G. Death Anxiety, Loss, and Grief in the Time of COVID-19. Behav. Chang. 2020, 37, 111–115. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Paleari, F.G.; Pivetti, M.; Galati, D.; Fincham, F.D. Hedonic and eudaimonic well-being during the COVID-19 lockdown in Italy: The role of stigma and appraisals. Br. J. Health Psychol. 2020, 26, 657–678. [Google Scholar] [CrossRef]
- Nelson-Coffey, S.K.; Fuller, J.A.K.; Choi, I.; Lyubomirsky, S. Beyond self-protection: Self-affirmation benefits hedonic and eudaimonic well-being. Personal. Soc. Psychol. Bull. 2014, 40, 998–1011. [Google Scholar] [CrossRef]
- Kahneman, D.; Diener, E.; Schwarz, N. Well-Being: Foundations of Hedonic Psychology; Russell Sage Foundation: New York, NY, USA, 1999. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Waterman, A.S.; Schwartz, S.J.; Zamboanga, B.L.; Ravert, R.D.; Williams, M.K.; Agocha, V.B.; Kim, S.Y.; Donnellan, M.B. The questionnaire for eudaimonic well-being: Psychometric properties, demographic comparisons, and evidence of validity. J. Posit. Psychol. 2010, 5, 41–61. [Google Scholar] [CrossRef]
- Huta, V. An overview of hedonic and eudaimonic well-being concepts. In The Routledge Handbook of Media Use and Well-Being; Reinecke, L., Oliver, M.B., Eds.; Routledge: Abingdon-on-Thames, UK, 2016; pp. 14–33. [Google Scholar]
- Huta, V.; Waterman, A.S. Eudaimonia and its distinction from Hedonia: Developing a classification and terminology for understanding conceptual and operational definitions. J. Happiness Stud. 2014, 15, 1425–1456. [Google Scholar] [CrossRef]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Personal. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef]
- Fischer, I.C.; Shanahan, M.L.; Hirsh, A.T.; Stewart, J.C.; Rand, K.L. The relationship between meaning in life and post-traumatic stress symptoms in US military personnel: A meta-analysis. J. Affect. Disord. 2020, 277, 658–670. [Google Scholar] [CrossRef]
- Prime, H.; Wade, M.; Browne, D.T. Risk and resilience in family well-being during the COVID-19 pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef]
- Gubler, D.A.; Makowski, L.M.; Troche, S.J.; Schlegel, K. Loneliness and well-being during the COVID-19 pandemic: Associations with personality and emotion regulation. J. Happiness Stud. 2021, 22, 2323–2342. [Google Scholar] [CrossRef]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: Rapid review of the evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological adjustment of healthcare workers in Italy during the COVID-19 pandemic: Differences in stress, anxiety, depression, burnout, secondary trauma, and compassion satisfaction between frontline and non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef]
- Greenberg, J.; Pyszczynski, T.; Solomon, S. The causes and consequences of a need for self-esteem: A terror management theory. In Public Self and Private Self; Baumeister, R.F., Ed.; Springer: Cham, Switzerland, 1986; pp. 189–212. [Google Scholar]
- Juhl, J. Terror management theory: A theory of psychological well-being. In Handbook of Terror Management Theory; Vess, M.C., Ed.; Routledge Academic Press: Abingdon-on-Thames, UK, 2019; pp. 303–324. [Google Scholar]
- Templer, D.I. The construction and validation of a death anxiety scale. J. Gen. Psychol. 1970, 82, 165–177. [Google Scholar] [CrossRef]
- Chung, M.C.; Berger, Z.; Jones, R.; Rudd, H. Posttraumatic stress disorder and general health problems following myocar- dial infarction (post-MI PTSD) among older patients: The role of personality. Int. J. Geriatr. Psychiatry 2006, 21, 1163–1174. [Google Scholar] [CrossRef]
- Hoelterhoff, M.; Chung, M.C. Death anxiety and well-being: Coping with life-threatening events. Traumatology 2013, 19, 280–291. [Google Scholar] [CrossRef]
- Juhl, J.; Routledge, C. Putting the terror in terror management theory: Evidence that the awareness of death does cause anxiety and undermine psychological well-being. Curr. Dir. Psychol. Sci. 2016, 25, 99–103. [Google Scholar] [CrossRef]
- Klackl, J.; Jonas, E. Effects of mortality salience on physiological arousal. Front. Psychol. 2019, 10, 1893. [Google Scholar] [CrossRef]
- Shakil, M.; Ashraf, F.; Muazzam, A.; Amjad, M.; Javed, S. Work status, death anxiety and psychological distress during COVID-19 pandemic: Implications of the terror management theory. Death Stud. 2021, 44, 1100–1105. [Google Scholar] [CrossRef]
- Linley, P.A.; Joseph, S.; Goodfellow, B. Positive changes in outlook following trauma. and their relationship to subsequent posttraumatic stress, depression, and anxiety. J. Soc. Clin. Psychol. 2008, 27, 877–891. [Google Scholar] [CrossRef]
- Overcash, W.S.; Calhoun, L.G.; Cann, A.; Tedeschi, R.G. Coping with crises: An examination of the impact of traumatic event on religious beliefs. J. Genet. Psychol. 1996, 157, 455–464. [Google Scholar] [CrossRef]
- Henson, C.; Truchot, D.; Canevello, A. What promotes post traumatic growth? A systematic review. Eur. J. Trauma Dissociation 2021, 5, 100195. [Google Scholar] [CrossRef]
- Yaakobi, E. Desire to work as a death anxiety buffer mechanism. Exp. Psychol. 2015, 62, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Landau, M.J.; Kosloff, S.; Schmeichel, B. Imbuing everyday actions with meaning in response to existential threat. Self Identity 2011, 10, 64–76. [Google Scholar] [CrossRef]
- Yaakobi, E.; Mikulincer, M.; Shaver, P.R. Parenthood as a terror management mechanism: The moderating role of attachment orientations. Personal. Soc. Psychol. Bull. 2014, 40, 762–774. [Google Scholar] [CrossRef] [PubMed]
- King, L.A.; Hicks, J.A.; Abdelkhalik, J. Death, life, scarcity, and value: An alternative perspective on the meaning of death. Psychol. Sci. 2010, 20, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.-Y.; Shiah, Y.-J.; Hwang, K.-K.; Chuang, S.F. Life and death: Scarcity linking to enhanced meaning of life. J. Kaohsiung Behav. Sci. 2012, 3, 143–157. [Google Scholar]
- Baumeister, R.F.; Vohs, K.D.; Aaker, J.L.; Garbinsky, E.N. Some key differences between a happy life and a meaningful life. J. Posit. Psychol. 2013, 8, 505–516. [Google Scholar] [CrossRef]
- Anglim, J.; Horwood, S.; Smillie, L.D.; Marrero, R.J.; Wood, J.K. Predicting psychological and subjective well-being from personality: A meta-analysis. Psychol. Bull. 2020, 146, 279–323. [Google Scholar] [CrossRef]
- Soto, C.J. Is happiness good for your personality? Concurrent and prospective relations of the big five with subjective well-being. J. Personal. 2015, 83, 45–55. [Google Scholar] [CrossRef]
- Sun, J.; Kaufman, S.B.; Smillie, L.D. Unique associations between big five personality aspects and multiple dimensions of well-being. J. Personal. 2018, 86, 158–172. [Google Scholar] [CrossRef]
- Ackerman, R.A.; Witt, E.A.; Donnellan, M.B.; Trzesniewski, K.H.; Robins, R.W.; Kashy, D.A. What does the narcissistic personality inventory really measure? Assessment 2010, 18, 67–87. [Google Scholar] [CrossRef]
- Jonason, P.K.; Schmitt, D.P. What have you done for me lately? Friendship-selection in the shadows of Dark Triad trait. Evol. Psychol. 2012, 10, 400–421. [Google Scholar] [CrossRef]
- Morf, C.; Rhodewalt, F. Unraveling the paradoxes of narcissism: A dynamic self- regulatory processing model. Psychol. Inq. 2001, 12, 177–196. [Google Scholar] [CrossRef]
- Rose, P.; Campbell, W.K. Greatness feels good: A telic model of narcissism and subjective well-being. In Advances in Psychology Research; Shohov, S.P., Ed.; Nova Sciences Publisher: Hauppauge, NY, USA, 2004. [Google Scholar]
- Jonason, P.K.; Baughman, H.M.; Carter, G.L.; Parker, P. Dorian gray without his portrait: Psychological, social, and physical health costs associated with the Dark Triad. Personal. Individ. Differ. 2015, 78, 5–13. [Google Scholar] [CrossRef]
- Papageorgiou, K.A.; Gianniou, F.M.; Wilson, P.; Moneta, K.A.; Bilello, D.; Clough, P. The bright side of dark: Exploring the positive effect of narcissism on perceived stress through mental toughness. Personal. Individ. Differ. 2019, 139, 116–124. [Google Scholar] [CrossRef]
- Stamp, E.; Crust, L.; Swann, C.; Perry, J.; Marchant, D.; Clough, P.J. Relationships between mental toughness and psychological well-being in undergraduate university students. Personal. Individ. Differ. 2015, 75, 170–174. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, N.; Ma, M. The dark traits and the prediction of eduaimonic wellbeing. Front. Psychol. 2021, 12, 4940. [Google Scholar] [CrossRef]
- Rose, P. The happy and unhappy faces of Narcissism. Personal. Individ. Differ. 2002, 33, 379–391. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Liang Wannian, Head of Leading Group of Novel Coronavirus Prevention and Control, Said the Rapid Rise of the Pandemic in Wuhan Has Been Contained. Xinhuanet. Available online: http://www.nhc.gov.cn/wjw/xwdt/202002/de8415817d274c0da43f61f8d8c70b3d.shtml (accessed on 29 February 2020).
- Huang, Y.; Zhao, N. Mental health burden for the public affected by the COVID-19 outbreak in China: Who will be the high-risk group? Psychol. Health Med. 2021, 26, 23–34. [Google Scholar] [CrossRef]
- Goodman, L.A. Snowball sampling. Ann. Math. Stat. 1961, 32, 148–170. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Madnawat, A.V.S.; Kachhawa, P.S. Age, gender, and living circumstances: Discriminating older adults on death anxiety. Death Stud. 2007, 31, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Vittersø, J.; Søholt, Y. Life satisfaction goes with pleasure and personal growth goes with interest: Further arguments for separating hedonic and eudaimonic well-being. J. Posit. Psychol. 2011, 6, 326–335. [Google Scholar] [CrossRef]
- Proctor, C.; Tweed, R. Measuring eudaimonic well-being. In Handbook of Eudaimonic Well-Being; Vittersø, J., Ed.; Springer: Cham, Switzerland, 2016; pp. 277–294. [Google Scholar]
- Steger, M.F.; Frazier, P.; Oishi, S.; Kaler, M. The meaning in life questionnaire: Assessing the presence of and search for meaning in life. J. Couns. Psychol. 2006, 53, 80–93. [Google Scholar] [CrossRef]
- Steger, M.F.; Kawabata, Y.; Shimai, S.; Otake, K. The meaningful life in Japan and the United States: Levels and correlates of meaning in life. J. Res. Personal. 2008, 42, 660–678. [Google Scholar] [CrossRef]
- Steger, M.F.; Kashdan, T.B.; Sullivan, B.A.; Lorentz, D. Understanding the search for meaning in life: Personality, cognitive style, and the dynamic between seeking and experiencing meaning. J. Personal. 2008, 76, 199–228. [Google Scholar] [CrossRef]
- Jonason, P.K.; Webster, G.D. The dirty dozen: A concise measure of the dark triad. Psychol. Assess. 2010, 22, 420–432. [Google Scholar] [CrossRef]
- Wang, M.C. Latent Variable Modeling Using Mplus; Chongqing University Press: Chongqing, China, 2014. [Google Scholar]
- Li, S.; Liu, H.; Bai, X.W.; Ren, X.P.; Zheng, R.; Li, J.Z.; Rao, L.L.; Wang, Z.J. Psychological Typhoon Eye in 2008 Wenchuan Earthquake of May 12. Sci. Technol. Rev. 2009, 27, 87–89. [Google Scholar] [CrossRef]
- Zheng, R.; Rao, L.L.; Zheng, X.L.; Cai, C.; Wei, Z.H.; Li, S.; Xuan, Y.H. The more involved in lead-zinc mining risk the less frightened: A Psychological Typhoon Eye perspective. J. Environ. Psychol. 2015, 44, 126–134. [Google Scholar] [CrossRef]
- Xu, M.X.; Zheng, R.; Rao, L.L.; Kuang, Y.; Yang, S.W.; Ding, Y.; Ki, J.L.; Li, S. Proposals for coping with “psychological typhoon eye” effect detected in COVID-19. Bull. Chin. Acad. Sci. 2020, 35, 273–282. [Google Scholar] [CrossRef]
- Simione, L.; Gnagnarella, C. Differences between health workers and general population in risk perception, behaviors, and psychological distress related to COVID-19 spread in Italy. Front. Psychol. 2020, 11, 2166. [Google Scholar] [CrossRef]
- Li, S.; Rao, L.-L.; Bai, X.-W.; Zheng, R.; Ren, X.-P.; Li, J.-Z.; Wang, Z.-J.; Liu, H.; Zhang, K. Progression of the “psychological typhoon eye” and variations since the Wenchuan earthquake. PLoS ONE 2010, 5, e9727. [Google Scholar] [CrossRef]
- Russac, R.J.; Gatliff, C.; Reece, M.; Spottswood, D. Death anxiety across the adult years: An examination of age and gender effects. Death Stud. 2007, 31, 549–561. [Google Scholar] [CrossRef]
- Thiemann, P.; Quince, T.; Benson, J.; Wood, D.; Barclay, S. Medical students’ death anxiety: Severity and association with psychological health and attitudes toward palliative care. J. Pain Symptom. Manag. 2015, 50, 335–342. [Google Scholar] [CrossRef]
- Gillies, J.; Neimeyer, R.A. Loss, grief, and the search for significance: Toward a model of meaning reconstruction in bereavement. J. Constr. Psychol. 2006, 19, 31–65. [Google Scholar] [CrossRef]
- Trzebinski, J.; Cabanski, M.; Czarnecka, J.Z. Reaction to the COVID-19 pandemic: The influence of meaning in life, life satisfaction, and assumptions on world orderliness and positivity. J. Loss Trauma 2020, 25, 544–557. [Google Scholar] [CrossRef]
- Routledge, C.; Fiorito, T.A. Why meaning in life matters for societal flourishing. Front. Psychol. 2021, 11, 601899. [Google Scholar] [CrossRef]
- Lyke, J. Associations among aspects of meaning in life and death anxiety in young adults. Death Stud. 2013, 37, 471–482. [Google Scholar] [CrossRef]
- Zhang, J.; Peng, J.; Gao, P.; Huang, H.; Cao, Y.; Zheng, L.; Miao, D. Relationship between meaning in life and death anxiety in the elderly: Self-esteem as a mediator. BMC Geriatr. 2019, 19, 308. [Google Scholar] [CrossRef]
- O’Regan. How to Promote Positive Mental Health for Healthcare Workers. 2022. Available online: https://www.highspeedtraining.co.uk/hub/stress-in-healthcare-workers/ (accessed on 18 February 2022).
- Llorente-Alonso, M.; García-Ael, C.; Topa, G.; Sanz-Muñoz, M.L.; Muñoz-Alcalde, I.; Cortés-Abejer, B. Can psychological empowerment prevent emotional disorders in presence of fear of COVID-19 in health workers? A cross-sectional validation study. J. Clin. Med. 2021, 10, 1614. [Google Scholar] [CrossRef]
- Krok, D.; Zarzycka, B.; Telka, E. Risk of contracting COVID-19, personal resources and subjective well-being among healthcare workers: The mediating role of stress and meaning-making. J. Clin. Med. 2021, 10, 132. [Google Scholar] [CrossRef]
- Barnett, M.D.; Moore, J.M.; Garza, C.J. Meaning in life and self-esteem help hospice nurses withstand prolonged exposure to death. J. Nurs. Manag. 2019, 27, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Tongeren, D.R.V.; Green, J.D.; Davis, D.E.; Hook, J.N.; Hulsey, T.L. Prosociality enhance meaning in life. J. Posit. Psychol. 2015, 11, 225–236. [Google Scholar] [CrossRef]
- Hicks, J.A.; Trent, J.; Davis, W.E.; King, L.A. Positive affect, meaning in life and future time perspective: An application of socioemotional selectivity theory. Psychol. Ageing 2012, 27, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Hare, R.D. Comparison of procedures for the assessment of psychopathy. J. Consult. Clin. Psychol. 1985, 53, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Jonason, P.K.; Lyons, M.; Bethell, E. The making of Darth Vader: Parent-child care and the Dark Triad. Personal. Individ. Differ. 2014, 67, 30–34. [Google Scholar] [CrossRef]
- Abeyta, A.A.; Routledge, C.; Sedikides, C. Material meaning: Narcissists gain existential benefits from extrinsic goals. Soc. Psychol. Personal. Sci. 2017, 8, 219–228. [Google Scholar] [CrossRef]
- Tepper, S.J.; Lewis, N.A. When the going gets tough, how do we perceive the future? Soc. Cogn. 2021, 39, 526–541. [Google Scholar] [CrossRef]
- Peterson, C.; Park, N.; Seligman, M. Orientations to happiness and life satisfaction: The full life versus the empty life. J. Happiness Stud. 2005, 6, 25–41. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| M(SD) | Skewness | Kurtosis | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Age | 35.27(7.98) | ---- | ---- | 1 | ||||||||
| 2 Sex | ---- | ---- | ---- | ---- | 1 | |||||||
| 3 Area | ---- | ---- | ---- | ---- | ---- | 1 | ||||||
| 4 Death anxiety | 2.97(2.03) | 0.63 | −0.26 | 0.07 | 0.03 | −0.21 ** | 1 | |||||
| 5 Hedonic well-being | 4.11(1.48) | −0.04 | −0.61 | −0.09 | −0.04 | −0.12 ** | −0.15 ** | 1 | ||||
| 6 Eudaimonic well-being | 4.91(0.96) | −0.34 | 0.09 | 0.07 | −0.04 | −0.09 | −0.06 | 0.51 ** | 1 | |||
| 7 Presence of meaning | 4.81(1.16) | −0.21 | −0.13 | 0.04 | −0.03 | −0.08 * | −0.11 * | 0.50 ** | 0.87 ** | 1 | ||
| 8 Search for meaning | 5.14(1.15) | −0.56 | 0.62 | −0.02 | −0.01 | −0.04 | −0.06 | 0.36 ** | 0.86 ** | 0.51 ** | 1 | |
| 9 Narcissistic personality | 3.78(1.50) | −0.23 | −0.59 | 0.02 | −0.09 * | 0.06 | 0.27 ** | −0.06 | 0.06 | 0.10 * | −0.03 | 1 |
| Hedonic Well-Being | Eudaimonic Well-Being | |||||
|---|---|---|---|---|---|---|
| Standardized Estimate | t | CI | Standardized Estimate | t | CI | |
| Constant | 4.93 | 20.35 | [4.52 5.25] | 5.30 | 43.74 | [5.06 5.54] |
| Death Anxiety | −0.26 | −3.41 ** | [4.45 5.40] | −0.11 | −1.92 | [−0.29 0.09] |
| Narcissism | −0.14 | −2.25 ** | [−0.26 −0.02] | −0.03 | −0.85 | [−1.11 0.45] |
| Death Anxiety * Narcissism | 0.06 | 2.84 ** | [0.01 0.09] | 0.03 | 1.99 * | [0.01 0.05] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, N.; Liu, B.; Wang, Y. Examining the Relationship between Death Anxiety and Well-Being of Frontline Medical Staff during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 13430. https://doi.org/10.3390/ijerph192013430
Zhao N, Liu B, Wang Y. Examining the Relationship between Death Anxiety and Well-Being of Frontline Medical Staff during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(20):13430. https://doi.org/10.3390/ijerph192013430
Chicago/Turabian StyleZhao, Na, Beikun Liu, and Yiheng Wang. 2022. "Examining the Relationship between Death Anxiety and Well-Being of Frontline Medical Staff during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 20: 13430. https://doi.org/10.3390/ijerph192013430
APA StyleZhao, N., Liu, B., & Wang, Y. (2022). Examining the Relationship between Death Anxiety and Well-Being of Frontline Medical Staff during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(20), 13430. https://doi.org/10.3390/ijerph192013430