
Pain in the Cervical and Lumbar Spine as a Result of High G-Force Values in Military Pilots—A Systematic Review and Meta-Analysis


 and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
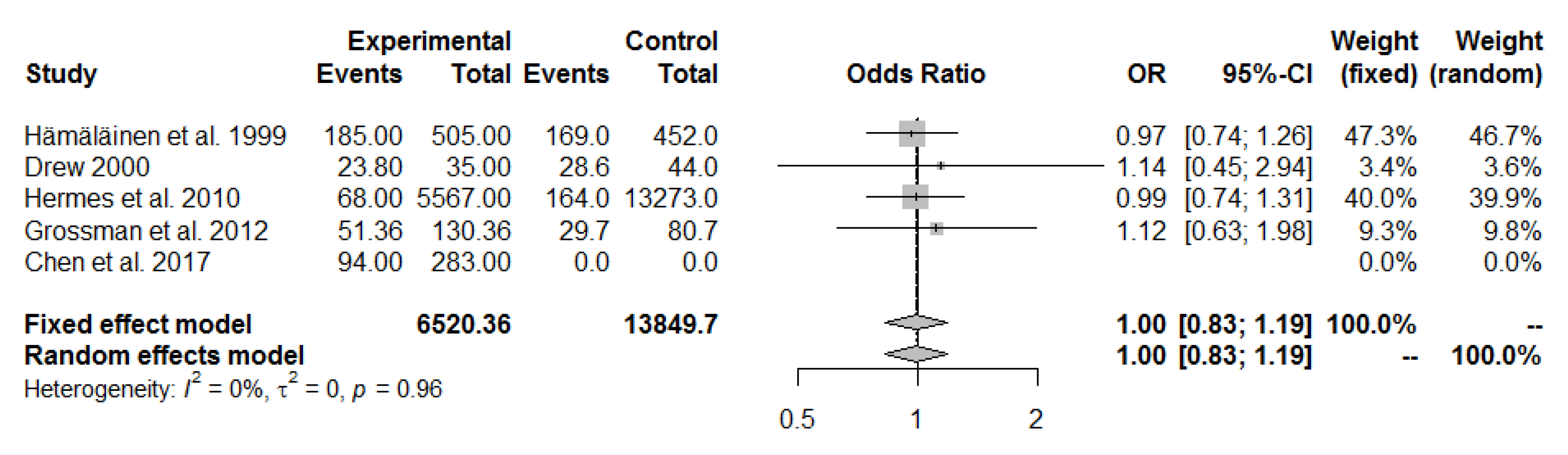
3.1. G-Induced Cervical and Lumbar Pain
3.1.1. Pain in the Cervical Spine
3.1.2. Pain in the Lumbar Spine
3.2. Prevalence of Neck and Lumbar Pain
4. Discussion
4.1. Pain in the Cervical and Lumbar Spine
4.2. Prevalence of Neck and Lumbar Pain
4.3. Limitation and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parr, J.C.; Miller, M.E.; Pellettiere, J.A.; Erich, R.A. Neck injury criteria formulation and injury risk curves for the ejection environment: A pilot study. Aviat. Space Environ. Med. 2013, 84, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Burnett, A.F.; Naumann, F.L.; Burton, E.J. Flight-training effect on the cervical muscle isometric strength of trainee pilots. Aviat. Space Environ. Med. 2004, 75, 611–615. [Google Scholar] [PubMed]
- Drew, W.E. Spinal symptoms on aviators and their relationship to G-exposure and aircraft seating angle. Aviat. Space Environ. Med. 2000, 71, 22–30. [Google Scholar] [PubMed]
- Freeman, S.; Karpowicz, A.; Gray, J.; McGill, S. Quantifying muscle patterns and spine load during various forms of the push-up. Med. Sci. Sports Exerc. 2006, 38, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Knudson, R.; Macmillan, D.; Doucette, D.; Seidel, M. A comparative study of G-induced neck injury in pilots of the F/A-18, A-7 and A-4. Aviat. Space Environ. Med. 1988, 59, 758–760. [Google Scholar]
- Newman, D.G. +Gz-induced neck injuries in Royal Australian Air Force fighter pilots. Aviat. Space Environ. Med. 1997, 68, 520–524. [Google Scholar]
- Petrén-Mallmin, M.; Linder, J. Cervical spine degeneration in fighter pilots and controls: A 5 year follow-up. Aviat. Space Environ. Med. 2001, 72, 443–446. [Google Scholar]
- Schall, D.G. Non-ejection cervical spine injuries due to +Gz in high performance aircraft. Aviat. Space Environ. Med. 1989, 60, 445–456. [Google Scholar]
- Vanderbeek, R.D. Period prevalence of acute neck injury in U.S. Air Force pilots exposed to high G forces. Aviat. Space Environ. Med. 1988, 59, 1176–1180. [Google Scholar]
- Hershkovich, O.; Friedlander, A.; Gordon, B.; Arzi, H.; Derazne, E.; Tzur, D.; Shamis, A.; Afek, A. Associations of body mass index and body height with low back pain in 829,791 adolescents. Am. J. Epidemiol. 2013, 178, 603–609. [Google Scholar] [CrossRef]
- Kikukawa, A.; Tachibana, S.; Yagura, S. G-related musculoskeletal spine symptoms in Japan Air Self Defense Force F-15 pilots. Aviat. Space Environ. Med. 1995, 66, 269–272. [Google Scholar] [PubMed]
- Hämäläinen, O.; Vanharanta, H.; Hupli, M.; Karhu, M.; Kuronen, P.; Kinnunen, H. Spinal shrinkage due to +Gz forces. Aviat. Space Environ. Med. 1996, 67, 659–661. [Google Scholar] [PubMed]
- Banks, R.D.; Gray, G. “Bunt bradycardia”: Two cases of slowing of heart rate inflight during negative Gz. Aviat. Space Environ. Med. 1994, 65, 330–331. [Google Scholar] [PubMed]
- Buckey, J.C.; Gaffney, F.A.; Lane, L.D.; Levine, B.D.; Watenpaugh, D.E.; Wright, S.J.; Yancy, C.W.; Meyer, D.M.; Blomqvist, C.G. Central Venous Pressure in Space. J. Appl. Physiol. 1996, 81, 19–25. [Google Scholar] [CrossRef]
- Prisk, G.K. Microgravity and the respiratory system. Eur. Respir. J. 2014, 43, 1459–1471. [Google Scholar] [CrossRef]
- Norsk, P. Adaptation of the Cardiovascular System to Weightlessness: Surprises, Paradoxes and Implications for Deep Space Missions. Acta Physiol. 2020, 228, e13434. [Google Scholar] [CrossRef] [PubMed]
- Thomae, M.K.; Porteous, J.E.; Brock, J.R.; Allen, G.D.; Heller, R.F. Back pain in Australian military helicopter pilots: A preliminary study. Aviat. Space Environ. Med. 1998, 69, 468–473. [Google Scholar]
- Grant, K.A. Ergonomic assessment of a helicopter crew seat: The HH-60G. Aviat. Space Environ. Med. 2002, 73, 913–918. [Google Scholar] [PubMed]
- Harrison, M.; Neary, J.; Albert, W.; Kuruganti, U.; Croll, J.; Chancey, V.; Bumgardner, B. Measuring neuromuscular fatigue in cervical spinal musculature of military helicopter aircrew. Mil. Med. 2009, 174, 1183–1189. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Visser, B.; van Dieen, J.H. Pathophysiology of upper extremity muscle disorders. J. Electromyogr. Kinesiol. 2006, 16, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Thuresson, M.; Ang, B.; Linder, J.; Harms-Ringdahl, K. Mechanical load and EMG activity in the neck induced by different head-worn equipment and neck postures. Int. J. Ind. Ergon. 2005, 35, 13–18. [Google Scholar] [CrossRef]
- Forde, K.A.; Albert, W.J.; Harrison, M.F.; Neary, J.P.; Croll, J.; Callaghan, J.P. Neck loads and posture exposure of helicopter pilots during simulated day and night flights. Int. J. Ind. Ergon. 2011, 41, 128–135. [Google Scholar] [CrossRef]
- Lange, B.; Torp-Svendsen, J.; Toft, P. Neck pain among fighter pilots after the introduction of the JHMCS helmet and NVG in their environment. Aviat. Space Environ. Med. 2011, 82, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Albano, J.J.; Stanford, J.B. Prevention of minor neck injuries in F-16 pilots. Aviat. Space Environ. Med. 1998, 69, 1193–1199. [Google Scholar] [PubMed]
- Jones, J.A.; Hart, S.F.; Baskin, D.S.; Effenhauser, R.; Johnson, S.L.; Novas, M.A.; Jennings, R.; Davis, J. Human and behavioral factors contributing to spine-based neurological cockpit injuries in pilots of high-performance aircraft: Recommendations for management and prevention. Mil. Med. 2000, 165, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.; Pennick, V.; Bombardier, C.; van Tulder, M. Updated method guidelines for systematic reviews in the cochrane back review group. Spine 2009, 34, 1929–1941. [Google Scholar] [CrossRef]
- Hämäläinen, O. Thoracolumbar pain among fighter pilots. Mil. Med. 1999, 164, 595–596. [Google Scholar] [CrossRef] [PubMed]
- Hermes, E.D.; Webb, T.S.; Wells, T.S. Aircraft type and other risk factors for spinal disorders: Data from 19,673 military cockpit aircrew. Aviat. Space Environ. Med. 2010, 81, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Grossman, A.; Nakdimon, I.; Chapnik, L.; Levy, Y. Back symptoms in aviators flying different aircraft. Aviat. Space Environ. Med. 2012, 83, 702–705. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Chung, C.H.; Lee, C.C.; Yang, C.S.; Wen, Y.S.; Lee, C.L.; Chiang, K.T. Analysis of intervertebral angulations and musculoskeletal symptoms of the spine in the military aircrews of Taiwan. Biomed. Eng. Appl. Basis Commun. 2017, 29, 1750010. [Google Scholar] [CrossRef]
- Ang, B.; Linder, J.; Harms-Ringdahl, K. Neck strength and myoelectric fatigue in fighter and helicopter pilots with a history of neck pain. Aviat. Space Environ. Med. 2005, 76, 375–380. [Google Scholar] [PubMed]
- Kang, S.; Hwang, S.; Lee, E.T.; Yang, S.; Park, J. Measuring the cumulative effect of G force on aviator neck pain. Aviat. Space Environ. Med. 2011, 82, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Moon, B.J.; Choi, K.H.; Yun, C.; Ha, Y. Cross-sectional study of neck pain and cervical sagittal alignment in air force pilots. Aerosp. Med. Hum. Perform. 2015, 86, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Verde, P.; Trivelloni, P.; Angelino, G.; Morgagni, F.; Tomao, E. Neck pain in F-16 vs. Typhoon fighter pilots. Aerosp. Med. Hum. Perform. 2015, 86, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Thoolen, S.J.; van den Oord, M.H. Modern air combat developments and their influence on neck and back pain in f-16 pilots. Aerosp. Med. Hum. Perform. 2015, 86, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Netto, K.; Hampson, G.; Oppermann, B.; Carstairs, G.; Aisbett, B. Management of neck pain in Royal Australian Air Force fast jet aircrew. Mil. Med. 2011, 176, 106–109. [Google Scholar] [CrossRef]
- Sovelius, R.; Oksa, J.; Rintala, H.; Siitonen, S. Neck and back muscle loading in pilots flying high G(z) sorties with and without lumbar support. Aviat. Space Environ. Med. 2008, 79, 616–619. [Google Scholar] [CrossRef]
- Tucker, B.; Netto, K.; Hampson, G.; Oppermann, B.; Aisbett, B. Predicting neck pain in Royal Australian Air Force fighter pilots. Mil. Med. 2012, 177, 444–450. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wagstaff, A.; Jahr, K.; Rodskier, S. +Gz-induced spinal symptoms in fighter pilots: Operational and individual associated factors. Aviat. Space Environ. Med. 2012, 83, 1092–1096. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.; Toft, P.; Myburgh, C.; Sjøgaard, G. Effect of targeted strength, endurance, and coordination exercise on neck and shoulder pain among fighter pilots: A randomized-controlled trial. Clin. J. Pain. 2013, 29, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Rintala, H.; Häkkinen, A.; Siitonen, S.; Kyröläinen, H. Relationships between physical fitness, demands of flight duty, and musculoskeletal symptoms among military pilots. Mil. Med. 2015, 180, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Rausch, M.; Weber, F.; Kühn, S.; Ledderhos, C.; Zinner, C.; Sperlich, B. The effects of 12 weeks of functional strength training on muscle strength, volume and activity upon exposure to elevated Gz forces in high-performance aircraft personnel. Mil. Med. Res. 2021, 8, 15. [Google Scholar] [CrossRef]
- Field, A.P.; Gillett, R. How to do a meta-analysis. Br. J. Math. Stat. Psychol. 2010, 63, 665–694. [Google Scholar] [CrossRef]
- Shiri, R.; Frilander, H.; Sainio, M.; Karvala, K.; Sovelius, R.; Vehmas, T.; Viikari-Juntura, E. Cervical and lumbar pain and radiological degeneration among fighter pilots: A systematic review and meta-analysis. Occup. Environ. Med. 2015, 72, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Hämäläinen, O.; Vanharanta, H.; Kuusela, T. Degeneration of cervical intervertebral disks in fighter pilots frequently exposed to high +Gz forces. Aviat. Space Environ. Med. 1993, 8, 692–696. [Google Scholar]
- Andersson, G.B. Epidemiological features of chronic low-back pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine J. 2006, 15, 834–848. [Google Scholar] [CrossRef] [PubMed]
- Lawson, B.K.; Scott, O.; Egbulefu, F.J.; Ramos, R.; Jenne, J.W.; Anderson, E.R. Demographic and occupational predictors of neck pain in pilots: Analysis and multinational comparison. Aviat. Space Environ. Med. 2014, 85, 1185–1189. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The epidemiology of low back pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef]
- Eiken, O.; Kölegärd, R.; Bergsten, E.; Grönkvist, M. G protection: Interaction of straining maneuvers and positive pressure breathing. Aviat. Space Environ. Med. 2007, 78, 392–398. [Google Scholar] [PubMed]
- Coakwell, M.; Bloswick, D.; Moser, R. High-risk head and neck movements at high G and interventions to reduce associated neck injury. Aviat. Space Environ. Med. 2004, 75, 68–80. [Google Scholar] [PubMed]
- Hämäläinen, O.; Vanharanta, H.; Bloigu, R. +Gz-related neck pain: A follow-up study. Aviat. Space Environ. Med. 1994, 1, 16–18. [Google Scholar]
- Harrison, D.D.; Harrison, C.O.; Croft, A.C.; Harrison, D.E.; Troyanovich, S.J. Sitting biomechanics part I: Review of the literature. J. Manipulative Physiol. Ther. 1999, 22, 594–609. [Google Scholar] [CrossRef]
- Hoek van Dijke, G.A.; Snijders, C.J.; Roosch, E.R.; Burgers, P.I. Analysis of biomechanical and ergonomic aspects of the cervical spine in F-16 flight situations. J. Biomech. 1993, 26, 1017–1025. [Google Scholar] [CrossRef]
- Harms-Ringdahl, K.; Ekholm, J.; Schüldt, K.; Németh, G.; Arborelius, U.P. Load moments and myoelectric activity when the cervical spine is held in full flexion and extension. Ergonomics 1986, 29, 1539–1552. [Google Scholar] [CrossRef]
- Hendriksen, I.J.; Holewijn, M. Degenerative changes of the spine of fighter pilots of the Royal Netherlands Air Force (RNLAF). Aviat. Space Environ. Med. 1999, 70, 1057–1063. [Google Scholar]
- Kerstman, E.L.; Scheuring, R.A.; Barnes, M.G.; DeKorse, T.B.; Saile, L.G. Space adaptation back pain: A retrospective study. Aviat. Space Environ. Med. 2012, 83, 2–7. [Google Scholar] [CrossRef]
- Posch, M.; Schranz, A.; Lener, M.; Senn, W.; Äng, B.O.; Burtscher, M.; Ruedl, G. Prevalence and potential risk factors of flight-related neck, shoulder and low back pain among helicopter pilots and crewmembers: A questionnaire-based study. BMC Musculoskelet. Disord. 2019, 20, 44. [Google Scholar] [CrossRef]
- Greeves, J.; Wickes, S. Review of the United Kingdom national work programme on the long-term effects of sustained high G on the cervical spine. In NATO RTO Review of National Work Programmes on the Long-Term Effects of Sustained High G on the Cervical Spine; Harms-Ringdahl, K., Ed.; The National Technical Information Service: Springfield, IL, USA, 2008; pp. 1–10. [Google Scholar]
- De Loose, V.; Van den Oord, M.; Burnotte, F.; Van Tiggelen, D.; Stevens, V.; Cagnie, B.; Danneels, L.; Witvrouw, E. Functional assessment of the cervical spine in F-16 pilots with and without neck pain. Aviat. Space Environ. Med. 2009, 80, 477–481. [Google Scholar] [CrossRef]
- Seng, K.Y.; Lam, P.M.; Lee, V.S. Acceleration effects on neck muscle strength: Pilots vs. non-pilots. Aviat. Space Environ. Med. 2003, 74, 164–168. [Google Scholar]
- Oksa, J.; Hämäläinen, O.; Rissanen, S.; Salminen, M.; Kuronen, P. Muscle fatigue caused by repeated aerial combat maneuvering exercises. Aviat. Space Environ. Med. 1999, 70, 556–560. [Google Scholar] [PubMed]
- Haddock, C.K.; Poston, W.S.; Heinrich, K.M.; Jahnke, S.A.; Jitnarin, N. The benefits of high-intensity functional training fitness programs for military personnel. Mil. Med. 2016, 181, e1508–e1514. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain Number for the Risk of Bias Assessment | ||||||
|---|---|---|---|---|---|---|
| First Author and Year | 1 | 2 | 3 | 4 | 5 | 6 |
| Hämäläinen et al., 1999 [27] | Low | Low | Low | Low | Low | Low |
| Drew 2000 [3] | Moderate | Moderate | Low | High | Low | Moderate |
| Hermes et al., 2010 [28] | Low | Low | Low | Low | Low | Low |
| Grossman et al., 2012 [29] | Moderate | Moderate | Moderate | Moderate | Low | Moderate |
| Chen et al., 2017 [30] | Moderate | Moderate | Moderate | Moderate | Low | Moderate |
| Ang et al., 2005 [31] | High | Moderate | Moderate | High | Low | High |
| Kang et al., 2011 [32] | Low | Low | Low | Low | Low | Low |
| Moon et al., 2015 [33] | Low | Low | Low | Low | Low | Low |
| Verde et al., 2015 [34] | Moderate | Moderate | Moderate | Moderate | Low | Low |
| Thoolen et al., 2015 [35] | High | Moderate | Low | High | Low | High |
| Netto et al., 2011 [36] | Moderate | Moderate | Low | Moderate | Low | Moderate |
| Domain Number for the Risk of Bias Assessment | ||||||
|---|---|---|---|---|---|---|
| First Author and Year | 1 | 2 | 3 | 4 | 5 | 6 |
| Newman 1997 [6] | Low | Low | Low | Low | Low | Low |
| Albano et al., 1998 [24] | Moderate | Moderate | Low | High | Low | Moderate |
| Drew 2000, [3] | Moderate | Moderate | Low | High | Low | Moderate |
| Jones et al., 2000 [25] | Moderate | Moderate | Moderate | Moderate | Low | Moderate |
| Sovelius et al., 2008 [37] | Moderate | Moderate | Moderate | Moderate | Low | Moderate |
| Netto et al., 2011 [36] | Moderate | Moderate | Low | Moderate | Low | Moderate |
| Tucker et al., 2012 [38] | Low | Low | Low | Low | Low | Low |
| Wagstaff et al., 2012 [39] | 40Low | Low | Low | Low | Low | Low |
| Lange et al., 2013 [40] | Moderate | Moderate | Moderate | Moderate | Low | Low |
| Rintala et al., 2015 [41] | High | Moderate | Low | High | Low | High |
| Rausch et al., 2021 [42] | Moderate | Moderate | Low | Moderate | Low | Moderate |
| Author and Year | Neck/Lumbar | n/ Airplane Type | Pre-Flight Warm-Ups | In-FlightTechniques | Specific Training | Statistical Significance |
|---|---|---|---|---|---|---|
| Newman 1997 [6] | Neck | 52/ F/A-18 Hornet, MB326H Macchi | Warming up | Neck stretches | Neck strengthening exercise | ns |
| Albano et al., 1998 [24] | Neck | 268/ F-16 | Warming up, isometrics | Head vs. seat, prepositioning the head, unloading, | Neck and body strengthening exercises | p < 0.05 |
| Drew 2000 [3] | Neck/lumbar | 35/ F-16 s and F-15 s | Warming up, isometrics | Neck stretches, prepositioning the head, lumbar support | Aerobic exercises, running | ns |
| Jones et al., 2000 [25] | Neck | 95/ T-38, F-14, F-16, F/A-18 | Warming up | Weight training | ns | |
| Sovelius et al., 2008 [37] | Lumbar | 11/ BAe Systems Hawk MK51 | Individually shaped lumbar support | ns | ||
| Netto et al., 2011 [36] | Neck | 86/ not specified | Functional strength training | p < 0.05 | ||
| Tucker et al., 2012 [38] | Neck | 82/ F/A 18 | Warming up | In-flight Gz warm-up | Functional strength training | p < 0.05 |
| Wagstaff et al., 2012 [39] | Neck | 105/ F-16, F-5, T-38, T37, CF-104 | Functional strength training | ns | ||
| Lange et al., 2013 [40] | Neck | 55/ F-16 | Functional strength training | p = 0.01 | ||
| Rintala et al., 2015 [41] | Neck/ lumbar | 267/ not specified | Functional strength training | ns | ||
| Rausch et al., 2021 [42] | Neck | 18/ not specified | Functional strength training | p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastalerz, A.; Maruszyńska, I.; Kowalczuk, K.; Garbacz, A.; Maculewicz, E. Pain in the Cervical and Lumbar Spine as a Result of High G-Force Values in Military Pilots—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 13413. https://doi.org/10.3390/ijerph192013413
Mastalerz A, Maruszyńska I, Kowalczuk K, Garbacz A, Maculewicz E. Pain in the Cervical and Lumbar Spine as a Result of High G-Force Values in Military Pilots—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(20):13413. https://doi.org/10.3390/ijerph192013413
Chicago/Turabian StyleMastalerz, Andrzej, Inga Maruszyńska, Krzysztof Kowalczuk, Aleksandra Garbacz, and Ewelina Maculewicz. 2022. "Pain in the Cervical and Lumbar Spine as a Result of High G-Force Values in Military Pilots—A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 20: 13413. https://doi.org/10.3390/ijerph192013413
APA StyleMastalerz, A., Maruszyńska, I., Kowalczuk, K., Garbacz, A., & Maculewicz, E. (2022). Pain in the Cervical and Lumbar Spine as a Result of High G-Force Values in Military Pilots—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(20), 13413. https://doi.org/10.3390/ijerph192013413