
A Meta-Analysis of the Effects of Different Training Modalities on the Inflammatory Response in Adolescents with Obesity


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection and Exclusion Criteria of the Literature
2.3. Study Selection and Data Extraction
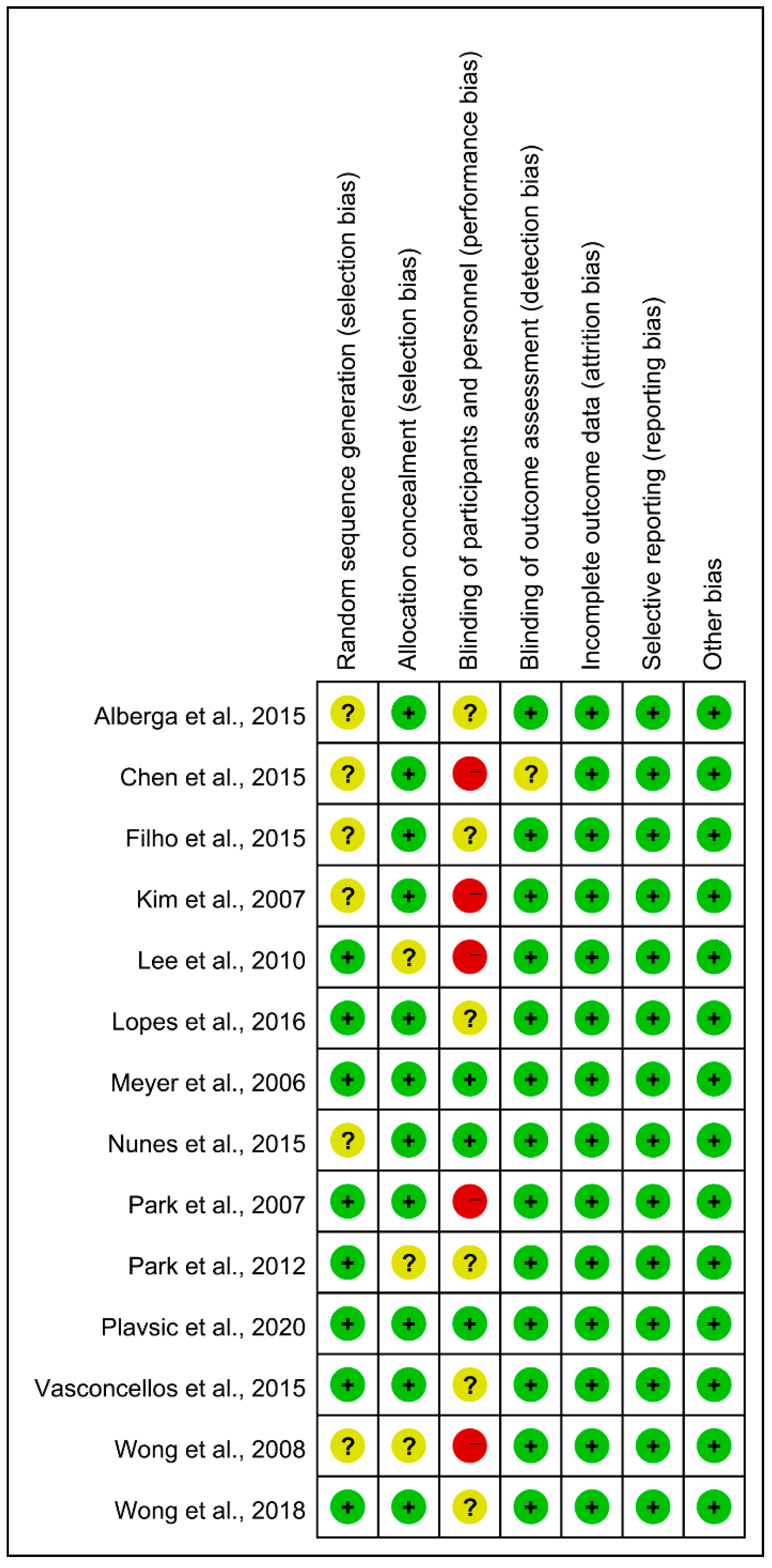
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. General Results of the Selected Research Literature
3.2. General Features of the Selected Research Literature
3.3. Quality Evaluation of the Selected Literature
3.4. Meta-Analysis of the Effect of Different Training Modalities on the Level of IL-6 in Adolescents with Obesity
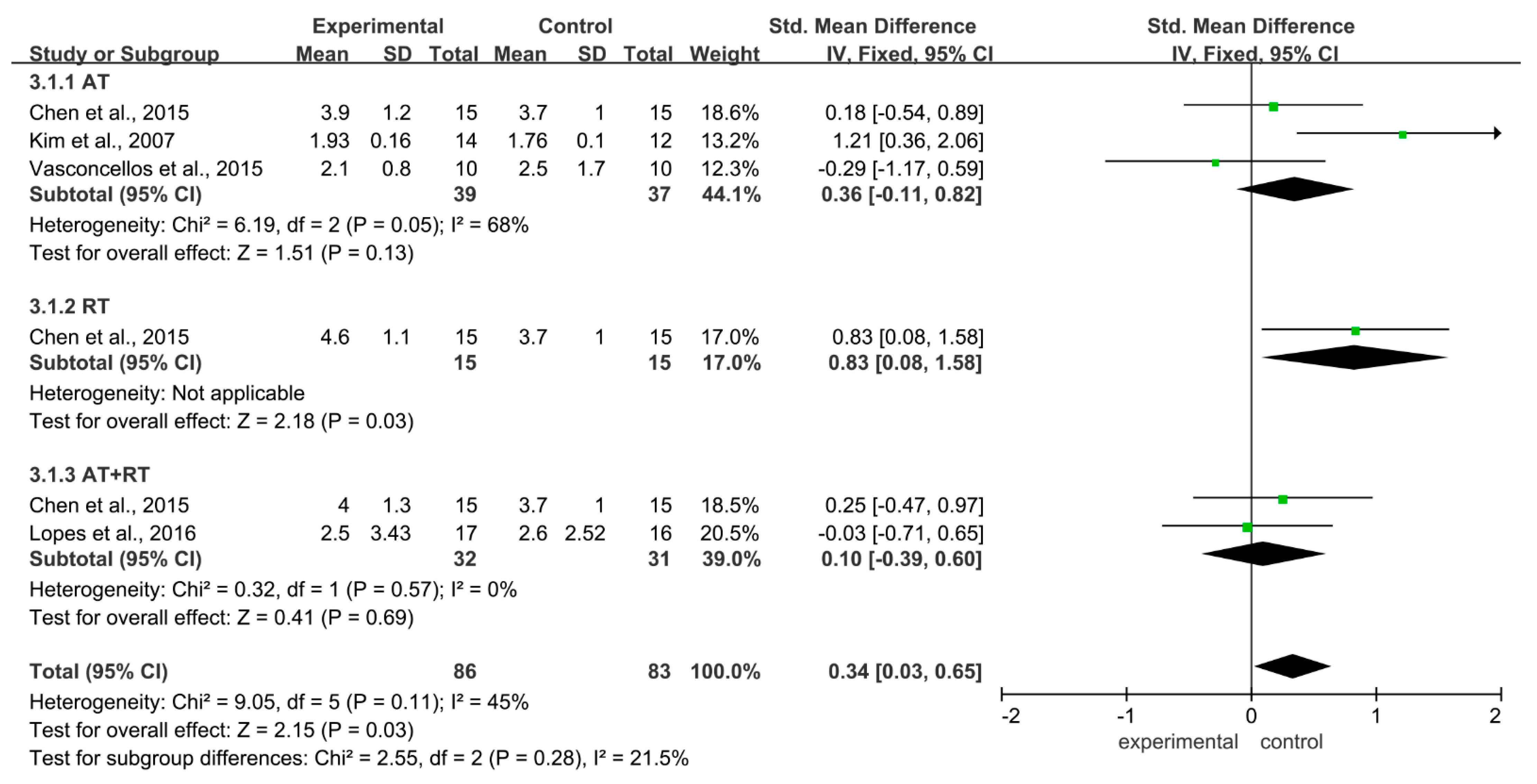
3.5. Meta-Analysis of The Effects of Different Training Modalities on the Level of Tnf-A in Adolescents with Obesity
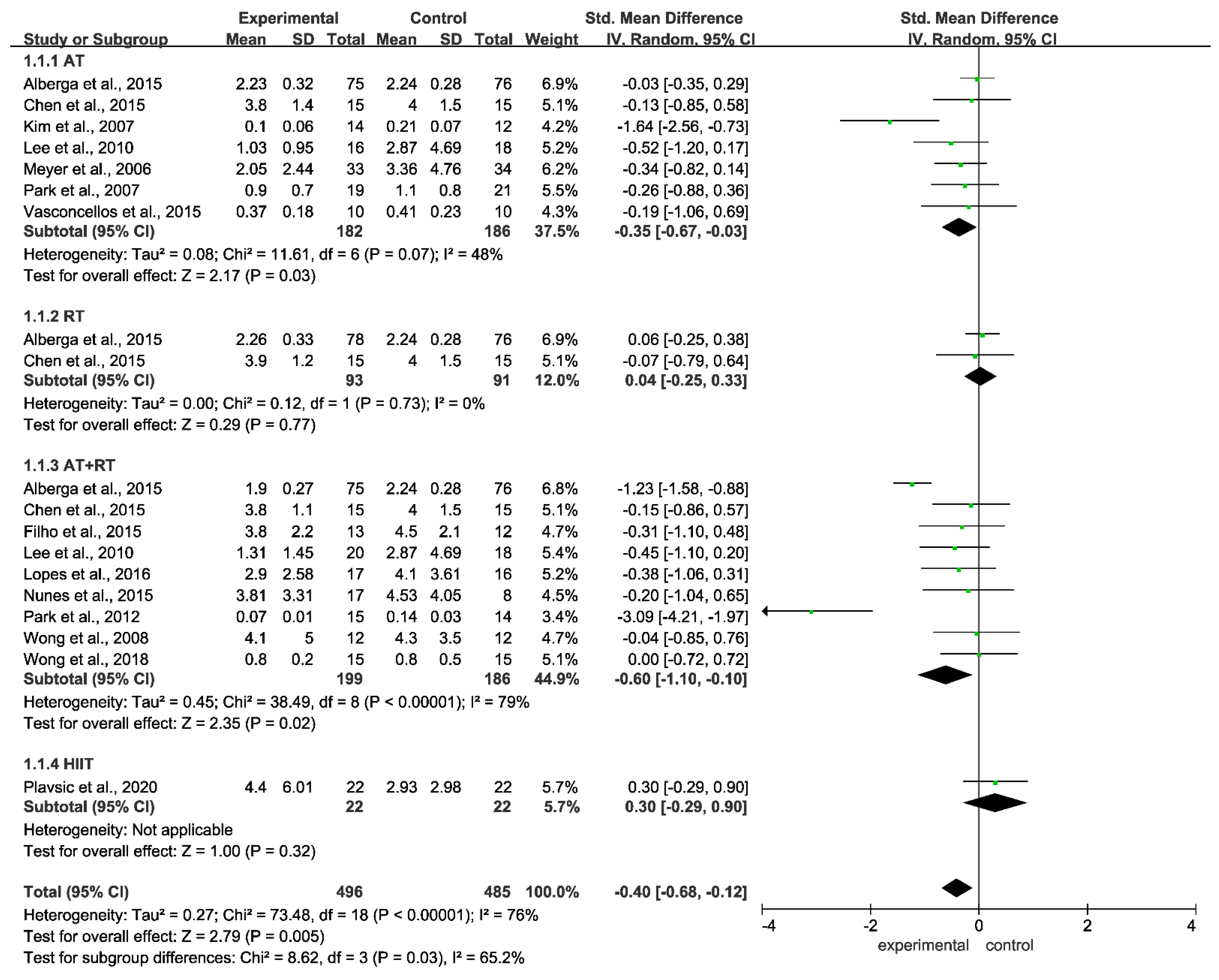
3.6. Meta-Analysis of the Effect of Different Training Modalities on the Level of CRP in Adolescents with Obesity
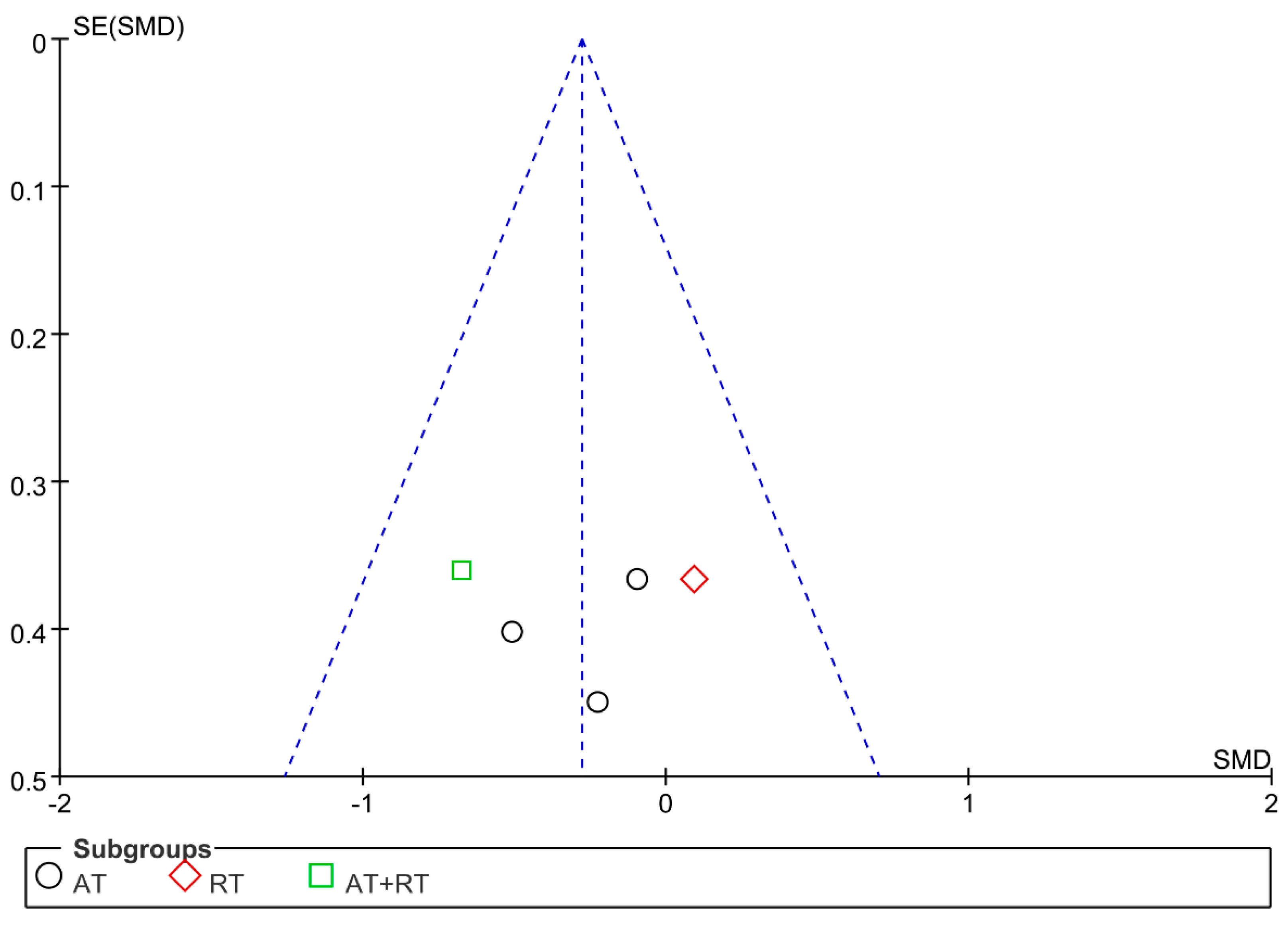
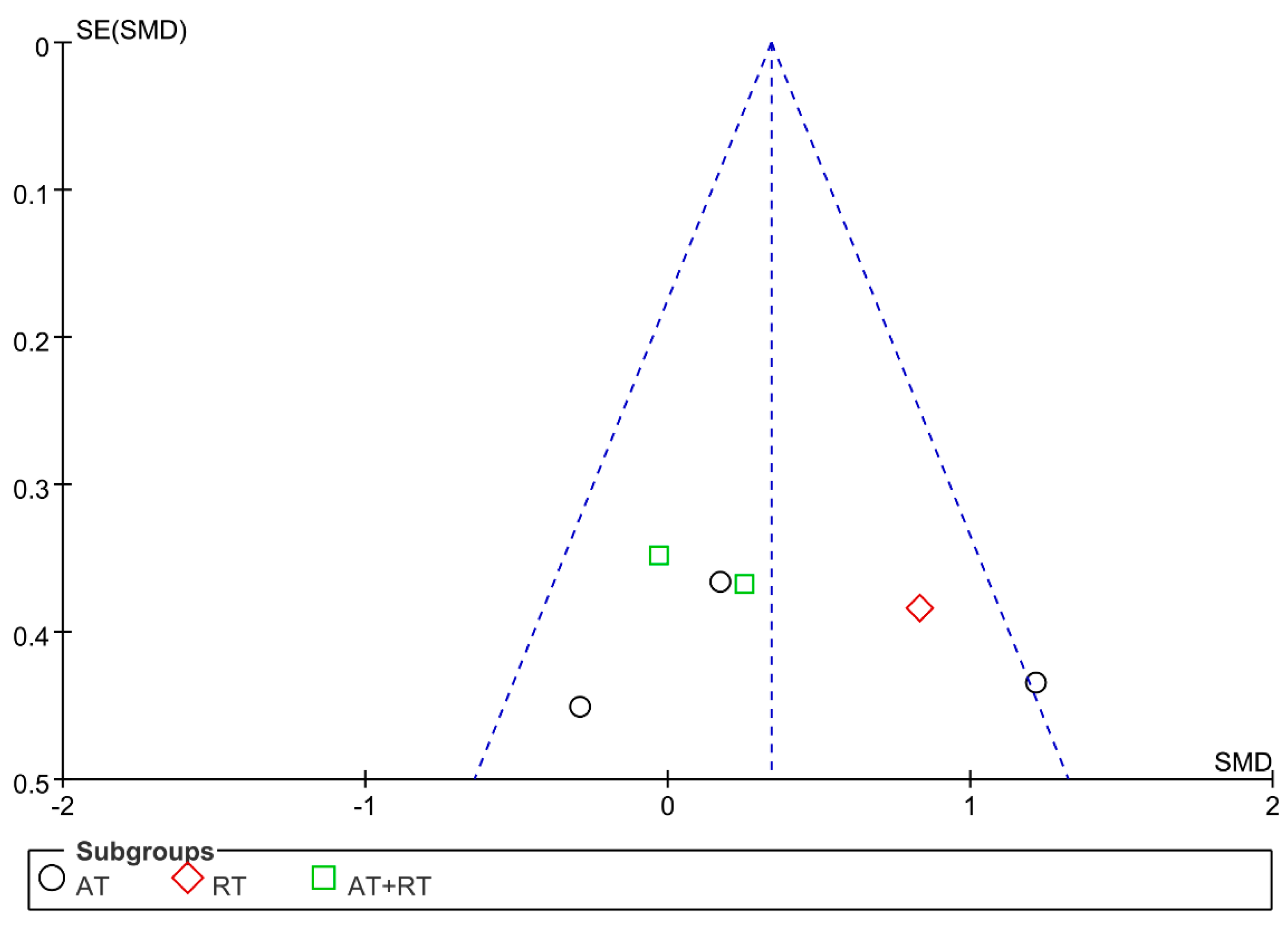
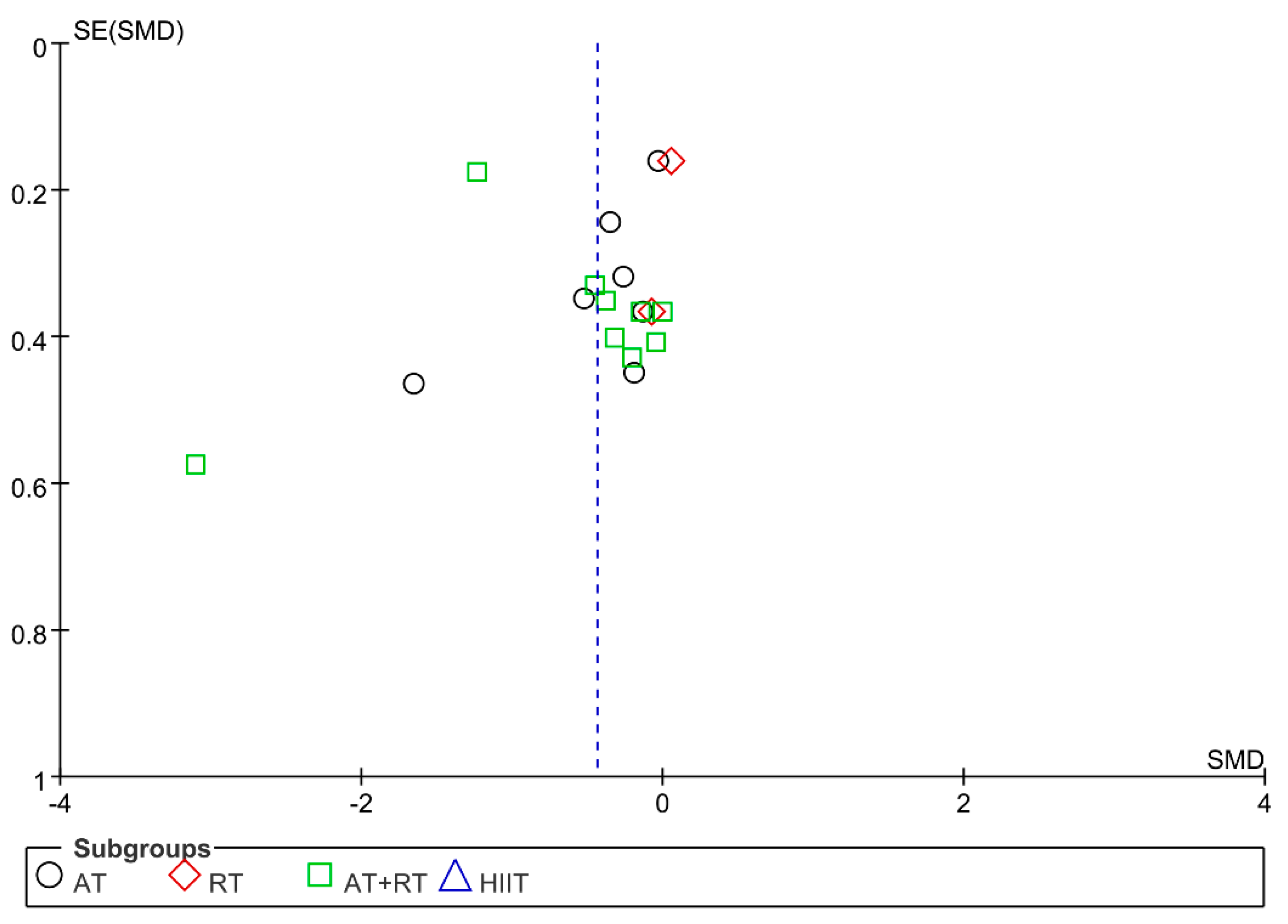
3.7. Publication Bias and Sensitivity Analysis
4. Discussion
5. Limitations of Current Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| China National Knowledge Infrastructure (CNKI) (lines 16) |
| Cochrane Risk of Bias (ROB) (lines 18) |
| aerobic training (AT) (lines 21) |
| aerobic + resistance training (AT + RT) (lines 21) |
| resistance training (RT) (lines 25) |
| World Health Organization (WHO) (lines 34) |
| World Obesity Federation (WOF) (lines 34) |
| C-reactive protein (CRP) (lines 54) |
| tumor necrosis factor alpha (TNF-α) (lines 54) |
| interleukin 6 (IL-6) (lines 55) |
| superoxide dismutase (SOD) (lines 58) |
| catalase (CAT) (lines 58) |
| glutathione peroxidase (GPX) (lines 58) |
| High-Intensity Interval Training (HIIT) (lines 69) |
| Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (lines 78) |
| Cochrane Risk of Bias (ROB) (lines 107) |
| weighted mean differences (WMD) (lines 118) |
| randomized controlled trials (RCTs) (lines 137) |
| adenosine monophosphate-activated protein kinase (AMPK) (lines 249) |
References
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef]
- Rocha, V.Z.; Folco, E.J. Inflammatory concepts of obesity. Int. J. Inflam. 2011, 2011, 529061. [Google Scholar] [CrossRef]
- Kansra, A.R.; Lakkunarajah, S.; Jay, M.S. Childhood and Adolescent Obesity: A Review. Front. Pediatr. 2020, 8, 581461. [Google Scholar] [CrossRef] [PubMed]
- Gurnani, M.; Birken, C.; Hamilton, J. Childhood Obesity: Causes, Consequences, and Management. Pediatr. Clin. N. Am. 2015, 62, 821–840. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, J.; Beeraka, N.M.; Tang, C.; Babayeva, Y.V.; Sinelnikov, M.Y.; Zhang, X.; Zhang, J.; Liu, J.; Reshetov, I.V.; et al. Advances in the Prevention and Treatment of Obesity-Driven Effects in Breast Cancers. Front. Oncol. 2022, 12, 820968. [Google Scholar] [CrossRef]
- Koskinen, J.; Magnussen, C.G.; Sabin, M.A.; Kahonen, M.; Hutri-Kahonen, N.; Laitinen, T.; Taittonen, L.; Jokinen, E.; Lehtimaki, T.; Viikari, J.S.; et al. Youth overweight and metabolic disturbances in predicting carotid intima-media thickness, type 2 diabetes, and metabolic syndrome in adulthood: The Cardiovascular Risk in Young Finns study. Diabetes Care 2014, 37, 1870–1877. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, S.; Weinstock, R.S. Youth-onset type 2 diabetes mellitus: Lessons learned from the TODAY study. Mayo Clin. Proc. 2014, 89, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Ballantyne, C.M. Skeletal muscle inflammation and insulin resistance in obesity. J. Clin. Investig. 2017, 127, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Stoner, L.; Rowlands, D.; Morrison, A.; Credeur, D.; Hamlin, M.; Gaffney, K.; Lambrick, D.; Matheson, A. Efficacy of Exercise Intervention for Weight Loss in Overweight and Obese Adolescents: Meta-Analysis and Implications. Sports Med. 2016, 46, 1737–1751. [Google Scholar] [CrossRef] [PubMed]
- Rybka, J.; Kupczyk, D.; Kedziora-Kornatowska, K.; Pawluk, H.; Czuczejko, J.; Szewczyk-Golec, K.; Kozakiewicz, M.; Antonioli, M.; Carvalho, L.A.; Kedziora, J. Age-related changes in an antioxidant defense system in elderly patients with essential hypertension compared with healthy controls. Redox Rep. 2011, 16, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Luan, Y.Y.; Yao, Y.M. The Clinical Significance and Potential Role of C-Reactive Protein in Chronic Inflammatory and Neurodegenerative Diseases. Front. Immunol. 2018, 9, 1302. [Google Scholar] [CrossRef]
- Jang, D.I.; Lee, A.H.; Shin, H.Y.; Song, H.R.; Park, J.H.; Kang, T.B.; Lee, S.R.; Yang, S.H. The Role of Tumor Necrosis Factor Alpha (TNF-alpha) in Autoimmune Disease and Current TNF-alpha Inhibitors in Therapeutics. Int. J. Mol. Sci. 2021, 22, 2719. [Google Scholar] [CrossRef]
- Gonzalez, L.E.; Landa, G.J.; Martin-Rabadan, M.M.; Kloppe, V.P. Cholesterol: What levels should be considered? Aten. Prim. 1989, 6, 73–74. [Google Scholar]
- Cheng, Y.; Sun, Z.; Ya, X.; Zhou, L.; Wang, M.; Wang, X.; Liu, Y. Effect of exercise training on arterial stiffness in obese and overweight children: A meta-analysis. Eur. J. Pediatr. 2022, 181, 2633–2642. [Google Scholar] [CrossRef]
- Park, T.G.; Hong, H.R.; Lee, J.; Kang, H.S. Lifestyle plus exercise intervention improves metabolic syndrome markers without change in adiponectin in obese girls. Ann. Nutr. Metab. 2007, 51, 197–203. [Google Scholar] [CrossRef]
- Kim, E.S.; Im, J.A.; Kim, K.C.; Park, J.H.; Suh, S.H.; Kang, E.S.; Kim, S.H.; Jekal, Y.; Lee, C.W.; Yoon, Y.J.; et al. Improved insulin sensitivity and adiponectin level after exercise training in obese Korean youth. Obes. Silver Spring 2007, 15, 3023–3030. [Google Scholar] [CrossRef]
- Wong, P.C.; Chia, M.Y.; Tsou, I.Y.; Wansaicheong, G.K.; Tan, B.; Wang, J.C.; Tan, J.; Kim, C.G.; Boh, G.; Lim, D. Effects of a 12-week exercise training programme on aerobic fitness, body composition, blood lipids and C-reactive protein in adolescents with obesity. Ann. Acad. Med. Singap. 2008, 37, 286–293. [Google Scholar]
- Alberga, A.S.; Prud’Homme, D.; Kenny, G.P.; Goldfield, G.S.; Hadjiyannakis, S.; Gougeon, R.; Phillips, P.; Malcolm, J.; Wells, G.; Doucette, S.; et al. Effects of aerobic and resistance training on abdominal fat, apolipoproteins and high-sensitivity C-reactive protein in adolescents with obesity: The HEARTY randomized clinical trial. Int. J. Obes. Lond. 2015, 39, 1494–1500. [Google Scholar] [CrossRef]
- Park, J.H.; Miyashita, M.; Kwon, Y.C.; Park, H.T.; Kim, E.H.; Park, J.K.; Park, K.B.; Yoon, S.R.; Chung, J.W.; Nakamura, Y.; et al. A 12-week after-school physical activity programme improves endothelial cell function in overweight and obese children: A randomised controlled study. BMC Pediatr. 2012, 12, 111. [Google Scholar] [CrossRef]
- Wong, A.; Sanchez-Gonzalez, M.A.; Son, W.M.; Kwak, Y.S.; Park, S.Y. The Effects of a 12-Week Combined Exercise Training Program on Arterial Stiffness, Vasoactive Substances, Inflammatory Markers, Metabolic Profile, and Body Composition in Obese Adolescent Girls. Pediatr. Exerc. Sci. 2018, 30, 480–486. [Google Scholar] [CrossRef]
- Nunes, J.E.; Cunha, H.S.; Freitas, Z.R.; Nogueira, A.M.; Damaso, A.R.; Espindola, F.S.; Cheik, N.C. Interdisciplinary therapy changes superoxide dismutase activity and adiponectin in obese adolescents: A randomised controlled trial. J. Sports. Sci. 2016, 34, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Vasconcellos, F.; Seabra, A.; Cunha, F.; Montenegro, R.; Penha, J.; Bouskela, E.; Nogueira, N.J.; Collett-Solberg, P.; Farinatti, P. Health markers in obese adolescents improved by a 12-week recreational soccer program: A randomised controlled trial. J. Sports Sci. 2016, 34, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Lopes, W.A.; Leite, N.; Da, S.L.; Brunelli, D.T.; Gaspari, A.F.; Radominski, R.B.; Chacon-Mikahil, M.P.; Cavaglieri, C.R. Effects of 12 weeks of combined training without caloric restriction on inflammatory markers in overweight girls. J. Sports Sci. 2016, 34, 1902–1912. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.A.; Kundt, G.; Lenschow, U.; Schuff-Werner, P.; Kienast, W. Improvement of early vascular changes and cardiovascular risk factors in obese children after a six-month exercise program. J. Am. Coll. Cardiol. 2006, 48, 1865–1870. [Google Scholar] [CrossRef]
- Lee, Y.H.; Song, Y.W.; Kim, H.S.; Lee, S.Y.; Jeong, H.S.; Suh, S.H.; Park, J.K.; Jung, J.W.; Kim, N.S.; Noh, C.I.; et al. The effects of an exercise program on anthropometric, metabolic, and cardiovascular parameters in obese children. Korean Circ. J. 2010, 40, 179–184. [Google Scholar] [CrossRef]
- Brandão, A.F.N.J.; Bellaguarda, E.R.F.; Rebouças, G.M.; Felipe, T.R.; Dantas, P.M.S.; Knackfuss, M.I.; Medeiros, H.J. Concurrent exercise program plus diet intervention on body adiposity and lipid profile in obese adolescents. Gazz. Med. Ital. Arch. Sci. Med. 2015, 174, 259–266. [Google Scholar]
- Plavsic, L.; Knezevic, O.M.; Sovtic, A.; Minic, P.; Vukovic, R.; Mazibrada, I.; Stanojlovic, O.; Hrncic, D.; Rasic-Markovic, A.; Macut, D. Effects of high-intensity interval training and nutrition advice on cardiometabolic markers and aerobic fitness in adolescent girls with obesity. Appl. Physiol. Nutr. Metab. 2020, 45, 294–300. [Google Scholar] [CrossRef]
- Chen, Q.; Cao, J.; Zhao, L.J.; Nan, Y. Effect of different exercise modes on body composition, inflammatory factors, and exercise capacity of obese teenagers. J. Jilin Univ. Med. Ed. 2015, 41, 1070–1075. [Google Scholar]
- Welsh, C.; Celis-Morales, C.A.; Brown, R.; Mackay, D.F.; Lewsey, J.; Mark, P.B.; Gray, S.R.; Ferguson, L.D.; Anderson, J.J.; Lyall, D.M.; et al. Comparison of Conventional Lipoprotein Tests and Apolipoproteins in the Prediction of Cardiovascular Disease. Circulation 2019, 140, 542–552. [Google Scholar] [CrossRef]
- Sato, K.; Iemitsu, M.; Matsutani, K.; Kurihara, T.; Hamaoka, T.; Fujita, S. Resistance training restores muscle sex steroid hormone steroidogenesis in older men. FASEB J. 2014, 28, 1891–1897. [Google Scholar] [CrossRef]
- Costa, R.R.; Buttelli, A.; Vieira, A.F.; Coconcelli, L.; Magalhaes, R.L.; Delevatti, R.S.; Kruel, L. Effect of Strength Training on Lipid and Inflammatory Outcomes: Systematic Review With Meta-Analysis and Meta-Regression. J. Phys. Act. Health 2019, 16, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Stepanikova, I.; Oates, G.R.; Bateman, L.B. Does one size fit all? The role of body mass index and waist circumference in systemic inflammation in midlife by race and gender. Ethn. Health 2017, 22, 169–183. [Google Scholar] [CrossRef]
- Wedell-Neergaard, A.S.; Lang, L.L.; Christensen, R.H.; Legaard, G.E.; Dorph, E.; Larsen, M.K.; Launbo, N.; Fagerlind, S.R.; Seide, S.K.; Nymand, S.; et al. Exercise-Induced Changes in Visceral Adipose Tissue Mass Are Regulated by IL-6 Signaling: A Randomized Controlled Trial. Cell Metab. 2019, 29, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Lee, J. Influences of exercise interventions on overweight and obesity in children and adolescents. Public Health Nurs. 2021, 38, 502–516. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Hume, P.; Maxwell, L. Delayed onset muscle soreness: Treatment strategies and performance factors. Sports Med. 2003, 33, 145–164. [Google Scholar] [CrossRef]
- Shi, M.L. Effects of Different Modes of Exercise Training on IL-6, TNF-α and hs-CRP in Post-menopausal Women. J. Xi’an Phys. Educ. Univ. 2011, 28, 481–488. [Google Scholar]
- Monteiro-Junior, R.S.; de Tarso, M.P.; Da, M.M.P.E.; Da, S.F.L.; Terra, R.; Carneiro, L.; Rodrigues, V.D.; Nascimento, O.; Deslandes, A.C.; Laks, J. Effect of Exercise on Inflammatory Profile of Older Persons: Systematic Review and Meta-Analyses. J. Phys. Act. Health 2018, 15, 64–71. [Google Scholar] [CrossRef]
- Bremer, A.A.; Jialal, I. Adipose tissue dysfunction in nascent metabolic syndrome. J. Obes. 2013, 2013, 393192. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.L.; Irving, B.A.; Lanza, I.R.; Vendelbo, M.H.; Konopka, A.R.; Robinson, M.M.; Henderson, G.C.; Klaus, K.A.; Morse, D.M.; Heppelmann, C.; et al. Differential Effect of Endurance Training on Mitochondrial Protein Damage, Degradation, and Acetylation in the Context of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1386–1393. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Research Subject | Training Mode Set | Outcomes | |||
|---|---|---|---|---|---|---|---|
| Age | Sample Size (Male/Female) | Training Mode | Training Frequency (n/Week) | Training Duration (Week) | |||
| Park et al., [15] | 2007 | AT:14.2 ± 0.5 | 19 (0/19) | AT | 6 | 12 | CRP |
| C: 14.1 ± 0.5 | 21 (0/21) | ||||||
| Kim et al., [16] | 2007 | AT: 17 ± 0.11 | 14 (14/0) | AT | 5 | 6 | CRP, TNF-α, IL-6, |
| C: 17 ± 0.11 | 12 (12/0) | ||||||
| Wong et al., [17] | 2008 | AT + RT: 13.75 ± 1.06 | 12 (12/0) | AT + RT | 2 | 12 | CRP |
| C: 14.25 ± 1.54 | 12 (12/0) | ||||||
| Alberga et al., [18] | 2015 | AT: 15.5 ± 1.4 | 75 (22/53) | AT | 4 | 22 | CRP |
| RT: 15.9 ± 1.5 | 78 (23/55) | RT | |||||
| AT + RT: 15.5 ± 1.3 | 75 (22/53) | AT + RT | |||||
| C: 15.6 ± 1.3 | 76 (24/52) | ||||||
| Park et al., [19] | 2012 | AT + RT: 12.1 ± 0.1 | 15 (7/8) | AT + RT | 3 | 12 | CRP |
| C: 12.2 ± 0.1 | 14 (7/7) | ||||||
| Wong et al., [20] | 2018 | AT + RT: 15.2 ± 1.2 | 15 (0/15) | AT + RT | 3 | 12 | CRP |
| C: 15.3 ± 1.1 | 15 (0/15) | ||||||
| Nunes et al., [21] | 2015 | AT + RT: 16.18 ± 1.51 | 17 (8/9) | AT + RT | :2 | 24 | CRP |
| C: 15.4 ± 1.2 | 8 (4/4) | ||||||
| Vasconcellos et al., [22] | 2015 | AT: 14.1 ± 1.3 | 10 (8/2) | AT | 3 | 12 | CRP, TNF-α, IL-6 |
| C: 14.8 ± 1.4 | 10 (6/4) | ||||||
| Lopes et al., [23] | 2016 | AT + RT: 14.6 ± 1.15 | 17 (0/17) | AT + RT | 3 | 12 | CRP, TNF-α, IL-6, |
| C: 14.4 ± 1.16 | 16 (0/16) | ||||||
| Meyer et al., [24] | 2006 | AT: 13.7 ± 2.1 | 33 (17/16) | AT | 3 | 24 | CRP |
| C: 14.7 ± 2.2 | 34 (17/17) | ||||||
| Lee et al., [25] | 2010 | AT: 13 ± 1.0 | 16 (45/9) | AT | 3 | 10 | CRP |
| AT + RT: 13 ± 1 | 20 | AT + RT | |||||
| C: 13 ± 1 | 18 | ||||||
| Filho et al., [26] | 2015 | AT + RT: 13.4 ± 1.3 | 13 (6/7) | AT + RT | 3 | 8 | CRP |
| C: 13.7 ± 0.9 | 12 (6/6) | ||||||
| Plavsic et al., [27] | 2020 | HIIT: 15.5 ± 1.5 | 22 (0/22) | HIIT | 2 | 12 | CRP |
| C: 16.2 ± 1.3 | 22 (0/22) | ||||||
| Chen et al., [28] | 2015 | AT: 14.1 ± 3.1 | 15 (15/0) | AT | 3 | 8 | CRP, TNF-α, IL-6, |
| RT: 13.9 ± 2.2 | 15 (15/0) | RT | |||||
| AT + RT: 14.2 ± 3.8 | 15 (15/0) | AT + RT | |||||
| C: 14.4 ± 3.2 | 15 (15/0) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, H.; Cheng, R.; Teng, J.; Song, G.; Huang, C.; Yuan, S.; Lu, Y.; Shen, S.; Liu, J.; Liu, C. A Meta-Analysis of the Effects of Different Training Modalities on the Inflammatory Response in Adolescents with Obesity. Int. J. Environ. Res. Public Health 2022, 19, 13224. https://doi.org/10.3390/ijerph192013224
Zhao H, Cheng R, Teng J, Song G, Huang C, Yuan S, Lu Y, Shen S, Liu J, Liu C. A Meta-Analysis of the Effects of Different Training Modalities on the Inflammatory Response in Adolescents with Obesity. International Journal of Environmental Research and Public Health. 2022; 19(20):13224. https://doi.org/10.3390/ijerph192013224
Chicago/Turabian StyleZhao, Haotian, Ruihong Cheng, Jin Teng, Ge Song, Chenjian Huang, Shuo Yuan, Yuxuan Lu, Siqin Shen, Jingqi Liu, and Chang Liu. 2022. "A Meta-Analysis of the Effects of Different Training Modalities on the Inflammatory Response in Adolescents with Obesity" International Journal of Environmental Research and Public Health 19, no. 20: 13224. https://doi.org/10.3390/ijerph192013224
APA StyleZhao, H., Cheng, R., Teng, J., Song, G., Huang, C., Yuan, S., Lu, Y., Shen, S., Liu, J., & Liu, C. (2022). A Meta-Analysis of the Effects of Different Training Modalities on the Inflammatory Response in Adolescents with Obesity. International Journal of Environmental Research and Public Health, 19(20), 13224. https://doi.org/10.3390/ijerph192013224