
Undertaking Healthy Nutrition Behaviors by Patients with Type 1 Diabetes as an Important Element of Self-Care

 , , ,
, , ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Data Collection
2.3. Ethics
2.4. Tools and Variables
2.5. Data Analysis
3. Results
3.1. Patient Characteristics
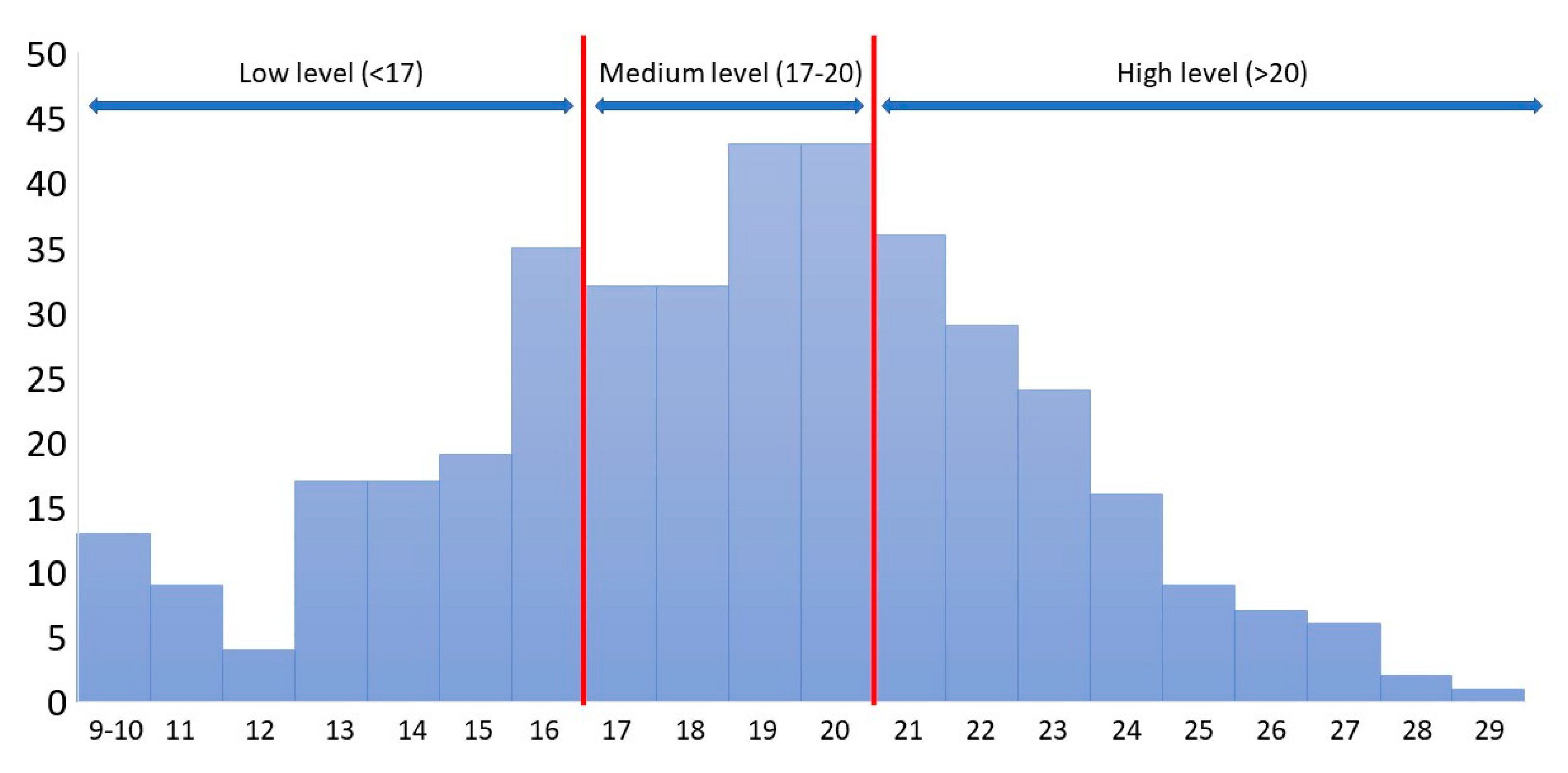
3.2. Adherence to Dietary Recommendations
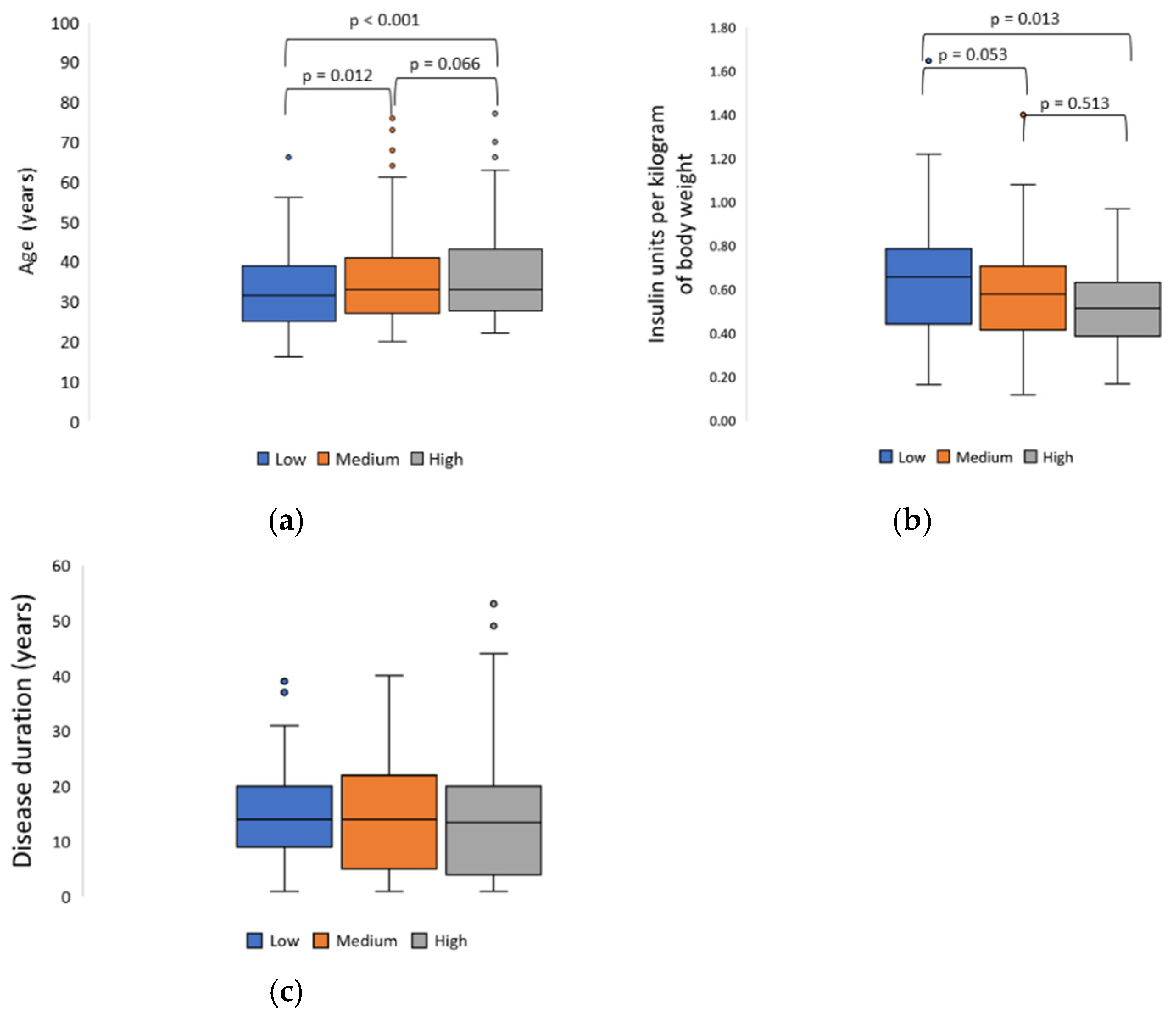
3.3. Factors Influencing Adherence to Dietary Recommendations
3.4. Responsibility for Health
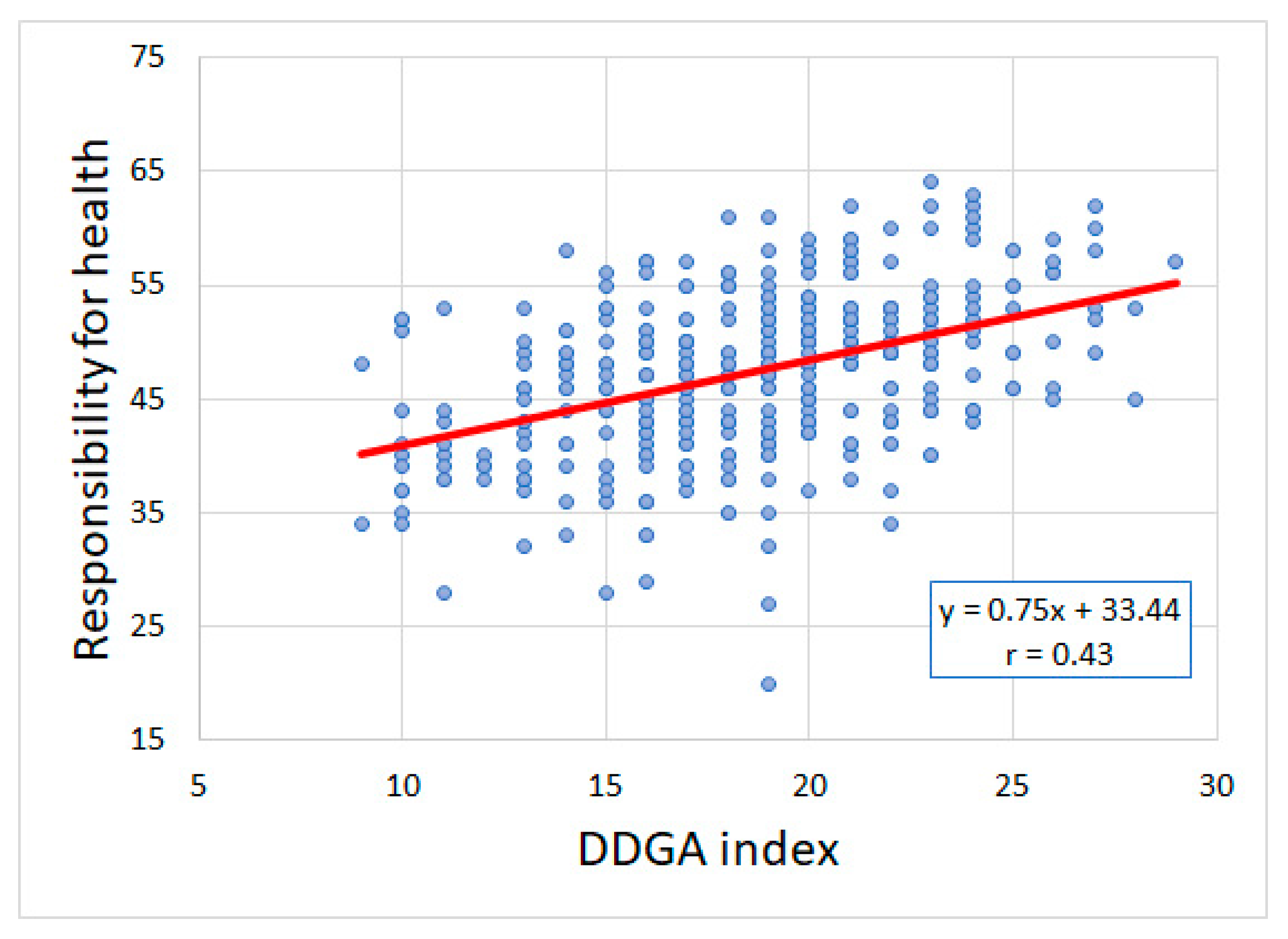
3.5. Responsibility for Health and Adherence to Dietary Recommendations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petroni, M.L.; Brodosi, L.; Marchignoli, F.; Sasdelli, A.S.; Caraceni, P.; Marchesini, G.; Ravaioli, F. Nutrition in patients with type 2 diabetes: Present knowledge and remaining challenges. Nutrients 2021, 13, 2748. [Google Scholar] [CrossRef] [PubMed]
- Reisi, M.; Mostafavi, F.; Javadzade, H.; Jalilian, F.; Mahaki, B.; Sharifirad, G. Effect of theory based education on blood sugar control in Type-2 diabetic patients. Iran J. Endocrinol. Metab. 2017, 18, 420–431. [Google Scholar]
- Bukhsh, A.; Goh, B.H.; Zimbudzi, E.; Lo, C.; Zoungas, S.; Chan, K.G.; Khan, T.M. Type 2 diabetes patients’ perspectives, experiences, and barriers toward diabetes-related self-care: A qualitative study from Pakistan. Front. Endocrinol. 2020, 11, 534873. [Google Scholar] [CrossRef] [PubMed]
- ADA. Facilitating behavior change and well-being to improve health outcomes: Standards of Medical Care in Diabetes. Diabetes Care 2021, 44, S53–S72. [Google Scholar] [CrossRef]
- Guidelines on the management of patients with diabetes. A position of diabetes Poland. Clin. Diabetol. 2021, 10, 1. [CrossRef]
- Smart, C.E.; Annan, F.; Higgins, L.A.; Jelleryd, E.; Lopez, M.; Acerini, C.L. ISPAD Clinical Practice Consensus Guidelines 2018: Nutritional management in children and adolescents with diabetes. Pediatr. Diabetes 2018, 19, 136–154. [Google Scholar] [CrossRef]
- Al-Sahouri, A.; Merrell, J.; Snelgrove, S. Barriers to good glycemic control levels and adherence to diabetes management plan in adults with Type-2 diabetes in Jordan: A literature review. Patient Prefer. Adherence 2019, 13, 675–693. [Google Scholar] [CrossRef]
- Grammatikopoulou, M.G.; Iosifidou, P.; Maraki, M.I.; Baltzis, D.; Mitsos, D.; Tsigga, M. Nutritional surveillance and diabetes knowledge among patients with type 2 diabetes. Obes. Med. 2017, 5, 44–49. [Google Scholar] [CrossRef]
- Tirfie, M.; Tadesse, S.; Woldie, H.; Weldegiorgis, T.; Birhanu, M.; Shibabaw, T. Dietary non-adherence and associated factors among individuals with diabetes who are on treatment follow up at Felege-Hiwot Referral Hospital, Northwest Ethiopia. Heliyon 2020, 6, e04544. [Google Scholar] [CrossRef]
- Parajuli, J.; Saleh, F.; Thapa, N.; Ali, L. Factors associated with nonadherence to diet and physical activity among Nepalese type 2 diabetes patients; a cross sectional study. BMC Res. Notes 2014, 7, 758. [Google Scholar] [CrossRef]
- Aminde, L.N.; Tindong, M.; Ngwasiri, C.A.; Aminde, J.A.; Njim, T.; Fondong, A.A.; Takah, N.F. Adherence to antidiabetic medication and factors associated with non-adherence among patients with type-2 diabetes mellitus in two regional hospitals in Cameroon. BMC Endocr. Disord. 2019, 19, 35. [Google Scholar] [CrossRef]
- Bin Rakhis, S.A.; AlDuwayhis, N.M.; Aleid, N.; AlBarrak, A.N.; Aloraini, A.A. Glycemic control for type 2 diabetes mellitus patients: A systematic review. Cureus 2022, 14, e26180. [Google Scholar] [CrossRef]
- Al-Salmi, N.; Cook, P.; D’Souza, M.S. Diet adherence among adults with type 2 diabetes mellitus: A concept analysis. Oman Med. J. 2022, 37, e361. [Google Scholar] [CrossRef]
- Almomani, M.H.; Al-Tawalbeh, S. Glycemic Control and its relationship with diabetes self-care behaviors among patients with type 2 diabetes in Northern Jordan: A cross-sectional study. Patient Prefer. Adherence 2022, 16, 449–465. [Google Scholar] [CrossRef]
- Lee, A.A.; Piette, J.D.; Heisler, M.; Rosland, A.M. Diabetes distress and glycemic control: The buffering effect of autonomy support from important family members and friends. Diabetes Care 2018, 41, 1157–1163. [Google Scholar] [CrossRef]
- Woynarowska, B. Health Education [Edukacja Zdrowotna]; Naukowe PWN Publisher: Warszawa, Poland, 2022. [Google Scholar]
- Jaworski, M.; Adamus, M.M. Health suggestibility, optimism and sense of responsibility for health in diabetic patients. Int. J. Diabetes Dev. Ctries 2016, 36, 290–294. [Google Scholar] [CrossRef]
- The Sense of Responsibility for the Health as an Important Element of Health Education. Available online: http://dpi-journals.com/index.php/dtssehs/article/view/3511. (accessed on 15 September 2021).
- Jaworski, M.; Adamus, M.M. A Sense of Responsibility for Health in Adolescents the Presentation of a new Research Tool. In Proceedings of the European Health Psychology Research (EHPS) 2016, Aberdeen, Scotland, 23–27 August 2016. [Google Scholar]
- Jaworski, M.; Adamus, M. The role of health-related Suggestibility and Sense of reSponsibility for health in Students’emotional eating. Kwartalnik Naukowy Uczelni Vistula 2017, 2, 259–274. [Google Scholar]
- Adamus, M.M.; Jaworski, M.; Owczarek, K. A sense of responsibility for health and health-related behaviour in patients with back pains. In Proceedings of the International Congress on Clinical and Counselling Psychology 2016, Kyrenia, Cyprus, 10–12 May 2016. [Google Scholar]
- Suchocka, L. Psychology of Responsibility in Health and Disease [Psychologia Odpowiedzialności w Zdrowiu i Chorobie]; Publisher Difin: Warszawa, Poland, 2011. [Google Scholar]
- Pendrey, A. The Little Book of Reflective Practice: A Practical Guide to the Early Years; Routledge: London, UK, 2022. [Google Scholar]
- Fearon-Lynch, J.A.; Sethares, K.A.; Asselin, M.E.; Batty, K.; Stover, C.M. Effects of Guided Reflection on Diabetes Self-Care: A Randomized Controlled Trial. Diabetes Educ. 2019, 45, 66–79. [Google Scholar] [CrossRef]
- Lie, S.S.; Karlsen, B.; Niemiec, C.P.; Graue, M.; Oftedal, B. Written reflection in an eHealth intervention for adults with type 2 diabetes mellitus: A qualitative study. Patient Prefer. Adherence 2018, 12, 311–320. [Google Scholar] [CrossRef]
- Sak, J.; Jarosz, M.; Mosiewicz, J.; Sagan, D.; Wiechetek, M.; Pawlikowski, J.; Wloszczak-Szubzda, A.; Olszewska, E. Self-perception and sense of responsibility for own health among chronically-ill patients [Postrzeganie własnej choroby a poczucie odpowiedzialności za swoje zdrowie osób przewlekle chorych]. Med. Ogólna I Nauk. O Zdrowiu 2011, 17, 169–173. [Google Scholar]
- Jaworski, M. The Sense of responsibility for health in diabetic patients: Is it important? Curr. Res. Diabetes Obes. J. 2017, 1, 555573. [Google Scholar]
- Sińska, B.; Jaworski, M.; Panczyk, M.; Traczyk, I.; Kucharska, A. The Role of Resilience and Basic Hope in the Adherence to Dietary Recommendations in the Polish Population during the COVID-19 Pandemic. Nutrients 2021, 13, 2108. [Google Scholar] [CrossRef]
- NIZP PZH—PIB. Healthy Eating Plate [Talerz Zdrowego Żywienia]. Available online: https://ncez.pzh.gov.pl/abc-zywienia/talerz-zdrowego-zywienia/ (accessed on 15 February 2021).
- Guidelines on the management of diabetic patients. A position of Diabetes Poland. Clin. Diabet 2019, 8, 1.
- World Health Organization (WHO). Obesity: Preventing and Managing the Global Pandemic; WHO: Geneva, Switzerland, 2000; Available online: https://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/ (accessed on 15 September 2021).
- Jaworski, M.; Panczyk, M.; Cedro, M.; Kucharska, A. Adherence to dietary recommendations in diabetes mellitus: Disease acceptance as a potential mediator. Patient Prefer. Adherence 2018, 12, 163. [Google Scholar] [CrossRef]
- Erikson, E.H. Identity and the Cycle of Life [Tożsamość a Cykl Życia]; Zysk i S-ka: Warsaw, Poland, 2004. [Google Scholar]
- Katsaridis, S.; Grammatikopoulou, M.G.; Gkiouras, K.; Tzimos, C.; Papageorgiou, S.T.; Markaki, A.G.; Exiara, T.; Goulis, D.G.; Papamitsou, T. Low reported adherence to the 2019 American diabetes association nutrition recommendations among patients with type 2 diabetes mellitus, indicating the need for improved nutrition education and diet care. Nutrients 2020, 12, 3516. [Google Scholar] [CrossRef] [PubMed]
- Mahmmoed, H.J.; Ibrahim, R.H.; Abdulgani, M.F. Awareness and dietary adherence of patients with type 2 diabetes mellitus in the city of Mosul: A cross-sectional study. Biomed. Pharmacol. J. 2020, 13, 1415–1422. [Google Scholar] [CrossRef]
- Trikkalinou, A.; Papazafiropoulou, A.K.; Melidonis, A. Type 2 diabetes and quality of life. World J. Diabetes 2017, 8, 120. [Google Scholar] [CrossRef]
- Kalra, S.; Jena, B.N.; Yeravdekar, R. Emotional and Psychological Needs of People with Diabetes. Indian J. Endocrinol. Metab. 2018, 22, 696–704. [Google Scholar]
- Oftedal, B.; Kolltveit, B.H.; Zoffmann, V.; Hörnsten, Å.; Graue, M. Learning to practise the Guided Self-Determination approach in type 2 diabetes in primary care: A qualitative pilot study. Nurs. Open. 2017, 4, 134–142. [Google Scholar] [CrossRef]
- Peleg, O. The relationship between type 2 diabetes, differentiation of self, and emotional distress: Jews and Arabs in Israel. Nutrients 2021, 14, 39. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group of Products | Recommended Consumption Frequency |
|---|---|
| Healthy groups of products | |
| (1) Fresh vegetables | several times a day |
| (2) Boiled vegetables and vegetable soups | once a day or more |
| (3) Fresh fruits | once a day or more |
| (4) Whole grain bread | once a day or more |
| (5) Other whole grains | once a day or more |
| (6) Dairy products (no added sugar) | once a day or more |
| (7) Legumes | several times a week or more |
| (8) Fish | once a week or more |
| (9) Unsalted nuts and seeds | several times a week or more |
| (10) White meat | several times a week or less |
| (11) Oils | once a day or more |
| (12) Margarines | once a day or more |
| (13) Eggs | several times a week or more |
| (14) Water | several times a day |
| Unhealthy groups of products | |
| (15) Red and processed meat | once a week or less |
| (16) Sweets | once a week or less |
| (17) Salty snacks | once a week or less |
| (18) Sweetened beverages | once a week or less |
| (19) Fast food | 1–3 times a month or less |
| (20) Butter | once a week or less |
| (21) Lard | once a week or less |
| (22) Processed cheese | several times a week or less |
| (23) Sweetened dairy products | once a week or less |
| (24) White bread | once a day or less |
| (25) White rice, fine-grained groats | once a day or less |
| (26) Refined grains/Breakfast cereals | once a week or less |
| (27) Flour dishes | once a week or less |
| (28) Ready-made sauces and/or instant products | 1–3 times a month or less |
| (29) Canned meat/fish/vegetables | once a week or less |
| Healthy nutritional habits | |
| (30) Consume meals at regular times | all of them/some of them |
| Gender, n (%) | |
| female | 256 (65.0) |
| male | 138 (35.0) |
| Age (years) | |
| M ± SD | 35.34 ± 11.36 |
| Min-Max | 18.0–77.0 |
| Education, n (%) | |
| Primary/vocational | 23 (5.9) |
| Secondary | 145 (36.9) |
| Tertiary | 225 (57.3) |
| Place of residence, n (%) | |
| Countryside | 88 (22.3) |
| Small town | 125 (31.7) |
| Big city | 181 (45.9) |
| Disease duration (years) | |
| M ± SD | 14.88 ± 10.71 |
| Min-Max | 1.0–54.0 |
| BMI categories, n (%) | |
| <18.5 kg/m2 | 5 (1.3) |
| 18.6–24.9 kg/m2 | 208 (52.8) |
| 25.0–29.9 kg/m2 | 126 (32.0) |
| 30.0–34.9 kg/m2 | 40 (10.2) |
| >35.0 kg/m2 | 15 (3.8) |
| Type of insulin therapy, n (%) | |
| Insulin pen | 221 (56.1) |
| Insulin pump | 173 (43.9) |
| Insulin units per day | |
| M ± SD | 43.04 ± 19.32 |
| Min–Max | 10.0–140.0 |
| Insulin units per kilogram of body weight | |
| M ± SD | 0.58 ± 0.22 |
| Min–Max | 0.1–1.6 |
| Hypoglycemia episodes, n (%) | |
| every day | 23 (5.8) |
| 5–6 times a week | 35 (8.9) |
| 4–3 times a week | 78 (19.8) |
| 1–2 times a week | 123 (31.2) |
| only once | 70 (17.8) |
| never | 65 (16.5) |
| Hyperglycemia episodes, n (%) | |
| every day | 74 (18.8) |
| 5–6 times a week | 75 (19.0) |
| 4–3 times a week | 87 (22.1) |
| 1–2 times a week | 72 (18.3) |
| only once | 47 (11.9) |
| never | 39 (9.9) |
| Knowledge of insulin/CEs ratio, n (%) | 320 (81.2) |
| Knowledge of CEs consumed daily, n (%) | 261 (66.2) |
| Knowing the calorie value of one’s diet, n (%) | 170 (43.1) |
| Group of Products | Percentage of Respondents Who Adhered to Recommendations (%) |
|---|---|
| Healthy groups of products | |
| (1) Fresh vegetables | 27.4 |
| (2) Boiled vegetables and vegetable soups | 25.6 |
| (3) Fresh fruits | 54.3 |
| (4) Whole grain bread | 49.0 |
| (5) Other whole grains | 22.8 |
| (6) Dairy products (no added sugar) | 26.1 |
| (7) Legumes | 18.0 |
| (8) Fish | 56.9 |
| (9) Unsalted nuts and seeds | 37.3 |
| (10) White meat | 87.6 |
| (11) Oils | 23.1 |
| (12) Margarines | 16.8 |
| (13) Eggs | 57.6 |
| (14) Water | 81.5 |
| Mean percentage of respondents who adhered to healthy product recommendations | 44.1 |
| Unhealthy groups of products | |
| (15) Red and processed meat | 80.2 |
| (16) Sweets | 53.8 |
| (17) Salty snacks | 81.2 |
| (18) Sweetened beverages | 83.5 |
| (19) Fast food | 75.9 |
| (20) Butter | 50.8 |
| (21) Lard | 98.0 |
| (22) Processed cheese | 79.4 |
| (23) Sweetened dairy products | 73.6 |
| (24) White bread | 83.5 |
| (25) White rice, fine-grained groats | 99.5 |
| (26) Refined grains/Breakfast cereals | 88.6 |
| (27) Flour dishes | 74.9 |
| (28) Ready-made sauces and/or instant products | 91.4 |
| (29) Canned meat/fish/vegetables | 91.9 |
| Mean percentage of respondents who adhered to unhealthy product recommendations | 80.4 |
| Healthy nutritional habits | |
| (30) Consume meals at regular times | 77.9 |
| Variable | Low Level | Medium Level | High Level | χ2 | p-Value * | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Gender | ||||||||
| Woman | 72 | 63.2 | 99 | 66.4 | 85 | 64.9 | 0.307 | 0.858 |
| Man | 42 | 36.8 | 50 | 33.6 | 46 | 35.1 | ||
| Education | ||||||||
| Primary/vocational | 11 | 9.6 | 8 | 5.4 | 4 | 3.1 | 24.427 | 0.000 |
| Secondary | 58 | 50.9 | 52 | 34.9 | 35 | 26.9 | ||
| Tertiary | 45 | 39.5 | 89 | 59.7 | 91 | 70.0 | ||
| Place of residence | ||||||||
| Village | 35 | 30.7 | 27 | 18.1 | 26 | 19.8 | 6.678 | 0.154 |
| Town | 32 | 28.1 | 51 | 34.2 | 42 | 32.1 | ||
| City | 47 | 41.2 | 71 | 47.7 | 63 | 48.1 | ||
| BMI categories (kg/m2) | ||||||||
| <18.5 | 1 | 0.9 | 1 | 0.7 | 3 | 2.3 | 6.398 | 0.603 |
| 18.6–24.9 | 58 | 50.9 | 75 | 50.3 | 75 | 57.3 | ||
| 25.0–29.9 | 35 | 30.7 | 51 | 34.2 | 40 | 30.5 | ||
| 30.0–34.9 | 14 | 12.3 | 15 | 10.1 | 11 | 8.4 | ||
| >35.0 | 6 | 5.3 | 7 | 4.7 | 2 | 1.5 | ||
| Type of insulin therapy | ||||||||
| Pens | 62 | 54.4 | 91 | 61.1 | 68 | 51.9 | 2.567 | 0.277 |
| Insulin pumps | 52 | 45.6 | 58 | 38.9 | 63 | 48.1 | ||
| Hypoglycemia episodes | ||||||||
| Every day | 5 | 4.4 | 12 | 8.1 | 6 | 4.6 | 6.182 | 0.800 |
| 5–6 times a week | 8 | 7.0 | 16 | 10.7 | 11 | 8.4 | ||
| 4–3 times a week | 21 | 18.4 | 30 | 20.1 | 27 | 20.6 | ||
| 1–2 times a week | 38 | 33.3 | 48 | 32.2 | 37 | 28.2 | ||
| Only once | 23 | 20.2 | 21 | 14.1 | 26 | 19.8 | ||
| Never | 19 | 16.7 | 22 | 14.8 | 24 | 18.3 | ||
| Hyperglycemia episodes | ||||||||
| Every day | 28 | 24.6 | 28 | 18.8 | 18 | 13.7 | 20.121 | 0.028 |
| 5–6 times a week | 28 | 24.6 | 24 | 16.1 | 23 | 17.6 | ||
| 4–3 times a week | 15 | 13.2 | 31 | 20.8 | 41 | 31.3 | ||
| 1–2 times a week | 19 | 16.7 | 35 | 23.5 | 18 | 13.7 | ||
| Only once | 14 | 12.3 | 17 | 11.4 | 16 | 12.2 | ||
| Never | 10 | 8.8 | 14 | 9.4 | 15 | 11.5 | ||
| Knowledge of insulin/CEs ratio | ||||||||
| No | 27 | 23.7 | 25 | 16.8 | 22 | 16.8 | 2.527 | 0.283 |
| Yes | 87 | 76.3 | 124 | 83.2 | 109 | 83.2 | ||
| Knowledge of average CEs consumed daily, N (%) | ||||||||
| No | 54 | 47.4 | 42 | 28.2 | 37 | 28.2 | 13.292 | 0.001 |
| Yes | 60 | 52.6 | 107 | 71.8 | 94 | 71.8 | ||
| Knowing the calorie value of one’s diet | ||||||||
| No | 85 | 74.6 | 82 | 55.0 | 57 | 43.5 | 24.280 | 0.000 |
| Yes | 29 | 25.4 | 67 | 45.0 | 74 | 56.5 | ||
| Independent Variable | b | βstd. | −95% CI | +95% CI | t | p-Value |
|---|---|---|---|---|---|---|
| Intercept | 10.32 | 4.847 | 0.000 | |||
| Responsibility for health | 0.17 | 0.30 | 0.21 | 0.40 | 6.317 | 0.000 |
| Age (years) | 0.03 | 0.10 | 0.01 | 0.19 | 2.098 | 0.037 |
| Gender | ||||||
| Male (ref.) | ||||||
| Female | 0.69 | 0.16 | 0.06 | 0.27 | 3.205 | 0.001 |
| BMI | −0.03 | −0.03 | −0.17 | 0.11 | −0.440 | 0.660 |
| Disease duration | −0.02 | −0.10 | −0.21 | 0.00 | −1.931 | 0.054 |
| Insulin units per day | −0.02 | −0.07 | −0.37 | 0.23 | −0.480 | 0.631 |
| Insulin units/kg/bw | −0.81 | −0.04 | −0.32 | 0.23 | −0.322 | 0.748 |
| Knows the average CE consumption | 0.43 | 0.10 | 0.01 | 0.19 | 2.234 | 0.026 |
| Knows the calorie value of the diet | 0.68 | 0.17 | 0.08 | 0.26 | 3.613 | 0.000 |
| Education | ||||||
| Primary/vocational (ref.) | ||||||
| Secondary | −0.31 | −0.04 | −0.13 | 0.05 | −0.968 | 0.334 |
| Tertiary | 0.61 | 0.09 | 0.00 | 0.19 | 1.977 | 0.049 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sińska, B.I.; Dłużniak-Gołaska, K.; Jaworski, M.; Panczyk, M.; Duda-Zalewska, A.; Traczyk, I.; Religioni, U.; Kucharska, A. Undertaking Healthy Nutrition Behaviors by Patients with Type 1 Diabetes as an Important Element of Self-Care. Int. J. Environ. Res. Public Health 2022, 19, 13173. https://doi.org/10.3390/ijerph192013173
Sińska BI, Dłużniak-Gołaska K, Jaworski M, Panczyk M, Duda-Zalewska A, Traczyk I, Religioni U, Kucharska A. Undertaking Healthy Nutrition Behaviors by Patients with Type 1 Diabetes as an Important Element of Self-Care. International Journal of Environmental Research and Public Health. 2022; 19(20):13173. https://doi.org/10.3390/ijerph192013173
Chicago/Turabian StyleSińska, Beata Irena, Karolina Dłużniak-Gołaska, Mariusz Jaworski, Mariusz Panczyk, Aneta Duda-Zalewska, Iwona Traczyk, Urszula Religioni, and Alicja Kucharska. 2022. "Undertaking Healthy Nutrition Behaviors by Patients with Type 1 Diabetes as an Important Element of Self-Care" International Journal of Environmental Research and Public Health 19, no. 20: 13173. https://doi.org/10.3390/ijerph192013173
APA StyleSińska, B. I., Dłużniak-Gołaska, K., Jaworski, M., Panczyk, M., Duda-Zalewska, A., Traczyk, I., Religioni, U., & Kucharska, A. (2022). Undertaking Healthy Nutrition Behaviors by Patients with Type 1 Diabetes as an Important Element of Self-Care. International Journal of Environmental Research and Public Health, 19(20), 13173. https://doi.org/10.3390/ijerph192013173