



Head Trauma Exposure in Mixed Martial Arts


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Description
2.2. Statistical Analysis
3. Results
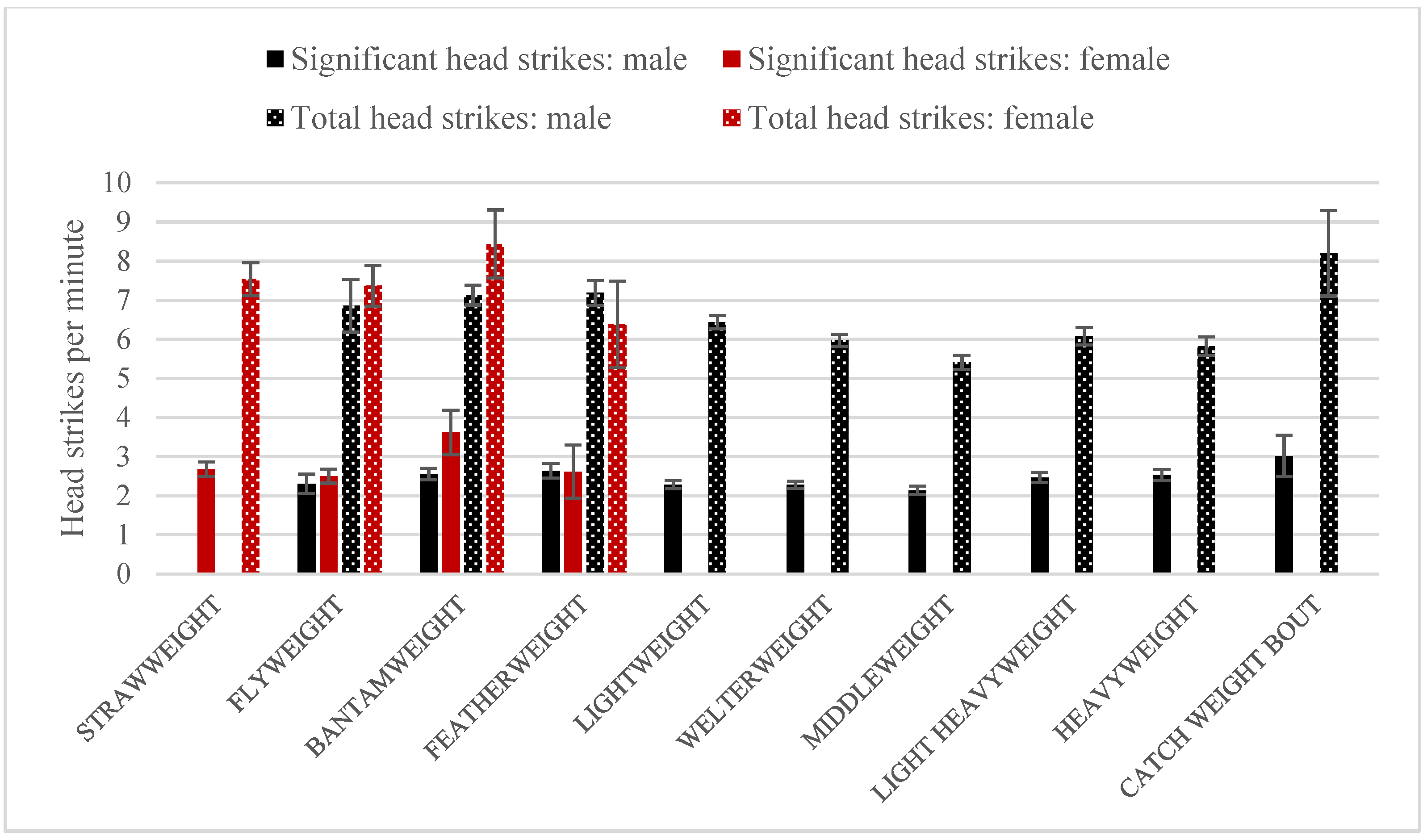
3.1. Head Strikes
3.2. Knockdowns
3.3. All Strikes
3.4. Fight Results
3.5. Fight Duration and Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lachlan, P.J.; Haff, G.G.; Kelly, V.G.; Beckman, E.M. Towards a determination of the physiological characteristics distinguishing successful Mixed Martial Arts athletes: A systematic review of combat sports literature. Sport. Med. 2016, 46, 1525–1551. [Google Scholar]
- White, C. Mixed martial arts and boxing should be banned, says BMA. BMJ 2007, 335, 469. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Available online: https://www.wma.net/policies-post/wma-statement-on-boxing/ (accessed on 2 October 2022).
- American Medical Association. Available online: https://policysearch.ama-assn.org/policyfinder/detail/boxing?uri=%2FAMADoc%2FHOD.xml-0-4296.xml (accessed on 2 October 2022).
- Available online: https://www.espn.com/mma/story/_/id/8766646/future-mma-kids-crazy-rayfield-espn-magazine (accessed on 26 July 2022).
- Lystad, R.P.; Gregory, K.; Wilson, J. The epidemiology of injuries in mixed martial arts: A systematic review and meta-analysis. Orthop. J. Sport. Med. 2014, 2, 2325967113518492. [Google Scholar] [CrossRef] [PubMed]
- Rainey, C.E. Determining the prevalence and assessing the severity of injuries in mixed martial arts athletes. N. Am. J. Sport. Phys. Ther. 2009, 4, 190–199. [Google Scholar]
- Fares, M.Y.; Salhab, H.A.; Fares, J.; Khachfe, H.H.; Fares, Y.; Baydoun, H.; Abboud, J.A.; Alaaeddine, N. Craniofacial and traumatic brain injuries in mixed martial arts. Phys. Sportsmed. 2021, 49, 420–428. [Google Scholar] [CrossRef]
- Curran-Sills, G.; Abedin, T. Risk factors associated with injury and concussion in sanctioned amateur and professional mixed martial arts bouts in Calgary, Alberta. BMJ Open Sport. Exerc. Med. 2018, 4, e000348. [Google Scholar] [CrossRef]
- Curran-Sills, G. Safety in Mixed Martial Arts: A 7-Year Review of Cancelled MMA Bouts in Calgary, Alberta, During the Pre-bout Medical Examination Period. Sport. Med. Open 2018, 12, 6. [Google Scholar] [CrossRef]
- Polman, H.; Melo, G.; Conti Réus, J.; Domingos, F.L.; de Souza, B.D.M.; Padilha, A.C.; Duque, T.M.; Porporatti, A.L.; Flores-Mir, C.; De Luca Canto, G. Prevalence of dentofacial injuries among combat sports practitioners: A systematic review and meta-analysis. Dent. Traumatol. 2020, 36, 124–140. [Google Scholar] [CrossRef]
- Karton, C.; Blaine Hoshizaki, T.; Gilchrist, M.D. A novel repetitive head impact exposure measurement tool differentiates player position in National Football League. Sci. Rep. 2020, 10, 1200. [Google Scholar] [CrossRef]
- Chen, W.; Post, A.; Karton, C.; Gilchrist, M.; Robidoux, M.; Hoshizaki, T.B. A comparison of frequency and magnitude of head impacts between Pee Wee and Bantam youth ice hockey. Sport. Biomech. 2020, 1–24. [Google Scholar] [CrossRef]
- Stein, T.; Alvarez, V.E.; McKee, A.C. Concussion in chronic traumatic encephalopathy. Curr. Pain Headache Rep. 2015, 19, 47. [Google Scholar] [CrossRef]
- Gavett, B.E.; Stern, R.A.; McKee, A.T. Chronic traumatic encephalopathy: A potential late effect of sport-related concussive and subconcussive head trauma. Clin. Sport. Med. 2011, 30, 179–188. [Google Scholar] [CrossRef]
- Baugh, C.M.; Stamm, J.M.; Riley, D.O.; Gavett, B.E.; Shenton, M.E.; Lin, A.; Nowinski, C.J.; Cantu, R.; McKee, A.C.; Stern, R.A. Chronic traumatic encephalopathy: Neurodegeneration following repetitive concussive and subconcusive brain trauma. Brain Imaging Behav. 2012, 6, 244–254. [Google Scholar] [CrossRef]
- Barbic, D.; Pater, J.; Brison, R.J. Comparison of mouthguard designs and concussion prevention in contact sports: A multicenter randomized controlled trial. Clin. J. Sport Med. 2005, 15, 294–298. [Google Scholar] [CrossRef]
- Gawlak, D.; Mańka-Malara, K.; Mierzwińska-Nastalska, E.; Waśniewski, B.; Ryszkowska, J. Comparison of hardness, energy absorption and water absorbability of polymeric materials used in the manufacture of mouthguards. Dent. Med. Probl. 2015, 52, 78–85. [Google Scholar]
- Tribst, J.P.M.; Dal Piva, A.M.O.; Bottino, M.A.; Kleverlaan, C.J.; Koolstra, J.H. Mouthguard use and TMJ injury prevention with different occlusions: A three-dimensional finite element analysis. Dent. Traumatol. 2020, 36, 662–669. [Google Scholar] [CrossRef]
- Hutchison, M.G.; Lawrence, D.W.; Cusimano, M.D.; Schweizer, T.A. Head trauma in Mixed Martial Arts. Am. J. Sport. Med. 2014, 42, 1352–1358. [Google Scholar] [CrossRef]
- McKee, A.C.; Stern, R.A.; Nowinski, C.J.; Stein, T.D.; Alvarez, V.E.; Daneshvar, D.H.; Lee, H.S.; Wojtowicz, S.M.; Hall, G.; Baugh, C.M.; et al. The spectrum of disease in chronic traumatic encephalopathy. Brain 2013, 136, 43–64. [Google Scholar] [CrossRef]
- Caccese, J.B. Head accelerations across collegiate, high school and youth female and male soccer players. Br. J. Sport. Med. 2018, 52, 98–99. [Google Scholar] [CrossRef]
- Ngai, K.M.; Levy, F.; Hsu, E.B. Injury trends in sanctioned mixed martial arts competition: A 5-year review from 2002 to 2007. Br. J. Sport. Med. 2008, 42, 686–689. [Google Scholar] [CrossRef]
- McClain, R.; Wassermen, J.; Mayfield, C.; Berry, A.C.; Grenier, G.; Suminski, R.R. Injury profile of mixed martial arts competitors. Clin. J. Sport Med. 2014, 24, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Davis, P.; Benson, P.R.; Waldock, R.; Connorton, A.J. Performance analysis of elite female amateur boxers and comparison with their male counterparts. Int. J. Sport. Physiol. Perform. 2016, 11, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Bianco, M.; Sanna, N.; Bucari, S.; Fabiano, C.; Palmieri, V.; Zeppilli, P. Female boxing in Italy: 2002–2007 report. Br. J. Sport. Med. 2011, 45, 563–570. [Google Scholar]
- Davis, P.; Benson, P.R.; Pitty, J.D.; Connorton, A.J.; Waldock, R. The activity profile of elite male amateur boxing. Int. J. Sport. Physiol. Perform. 2015, 10, 53–57. [Google Scholar] [CrossRef]
- Jansen, A.E.; McGrath, M.; Samorezov, S.; Johnston, J.; Bartsch, A.; Alberts, J. Characterizing Head Impact Exposure in Men and Women During Boxing and Mixed Martial Arts. Orthop. J. Sport. Med. 2021, 9, 23259671211059815. [Google Scholar] [CrossRef]
- Herring, S.; Kibler, W.B.; Putukian, M.; Solomon, G.S.; Boyajian-O’Neill, L.; Dec, K.L.; Franks, R.R.; Indelicato, P.A.; LaBella, C.R.; Leddy, J.J.; et al. Selected issues in sport-related concussion (SRC|mild traumatic brain injury) for the team physician: A consensus statement. Br. J. Sport. Med. 2021, 55, 1251–1261. [Google Scholar] [CrossRef]
- Roos, K.G.; Wasserman, E.B.; Dalton, S.L.; Gray, A.; Djoko, A.; Dompier, T.P.; Kerr, Z.Y. Epidemiology of 3825 injuries sustained in six seasons of National Collegiate Athletic Association men’s and women’s soccer (2009/2010–2014/2015). Br. J. Sport. Med. 2017, 51, 1029–1034. [Google Scholar] [CrossRef]
- Covassin, T.; Moran, R.; Elbin, R.J. Sex differences in reported concussion injury rates and time loss from participation: An update of the National Collegiate Athletic Association Injury Surveillance Program from 2004–2005 through 2008–2009. J. Athl. Train. 2016, 51, 189–194. [Google Scholar] [CrossRef]
- Neidecker, J.; Sethi, N.K.; Taylor, R.; Monsell, R.; Muzzi, D.; Spizler, B.; Lovelace, L.; Ayoub, E.; Weinstein, R.; Estwanik, J.; et al. Concussion management in combat sports: Consensus statement from the Association of Ringside Physicians. Br. J. Sport. Med. 2019, 53, 328–333. [Google Scholar] [CrossRef]
- Master, C.L.; Katz, B.P.; Arbogast, K.B.; McCrea, M.A.; McAllister, T.W.; Pasquina, P.F.; Lapradd, M.; Zhou, W.; Broglio, S.P. CARE Consortium Investigators. Differences in sport-related concussion for female and male athletes in comparable collegiate sports: A study from the NCAA-DoD Concussion Assessment, Research and Education (CARE) Consortium. Br. J. Sport. Med. 2021, 55, 1387–1394. [Google Scholar] [CrossRef]
- Hamer, J.; Churchill, N.W.; Hutchinson, M.; Graham, S.J.; Schweizer, T.A. Sex differences in cerebral blood flow associated with a history of concussion. J. Neurotrauma 2020, 37, 1197–1203. [Google Scholar] [CrossRef]
- Wunderle, M.K.; Hoeger, K.M.; Wasserman, M.E.; Bazarian, J.J. Menstrual phase as predictor of outcome after mild traumatic brain injury in women. J. Head Trauma Rehabil. 2014, 29, E1–E8. [Google Scholar] [CrossRef]
- Stein, D.G.; Hoffman, S.W. Estrogen and progesterone as neuroprotective agents in the treatment of acute brain injuries. Pediatr. Rehabil. 2003, 6, 13–22. [Google Scholar] [CrossRef]
- Covassin, T.; Swanik, C.B.; Sachs, M.L. Sex differences and the incidence of concussions among collegiate athletes. J. Athl. Train. 2003, 38, 238–244. [Google Scholar]
- Dollé, J.P.; Jaye, A.; Anderson, S.A.; Ahmadzadeh, H.; Shenoy, V.B.; Smith, D.H. Newfound sex differences in axonal structure underlie differential outcomes from in vitro traumatic axonal injury. Exp. Neurol. 2018, 300, 121–134. [Google Scholar] [CrossRef]
- Tierney, R.T.; Sitler, M.R.; Swanik, C.B.; Swanik, K.A.; Higgins, M.; Torg, J. Gender differences in head-neck segment dynamic stabilization during head acceleration. Med. Sci. Sport. Exerc. 2005, 37, 272–279. [Google Scholar] [CrossRef]
- Bennett, L.L.; Stephen, S.J.; Bernick, C.; Shan, G.; Banks, S.J. Sex Moderates the Relationship That Number of Professional Fights Has With Cognition and Brain Volumes. Front. Neurol. 2020, 11, 574458. [Google Scholar] [CrossRef]
- Covassin, T.; Elbin, R.; Bleecker, A.; Lipchik, A.; Kontos, A.P. Are there differences in neurocognitive functions and symptoms between male and women soccer players after concussion? Am. J. Sport. Med. 2013, 41, 2890–2895. [Google Scholar] [CrossRef]
- Covassin, T.; Schatz, P.; Swanik, C.B. Sex differences in neuropsychological function and post-concussion symptoms of concussed collegiate athletes. Neurosurgery 2007, 61, 345–351. [Google Scholar] [CrossRef]
- Chiang Colvin, A.; Mullen, J.; Lovell, M.R.; Vereeke West, R.; Collins, M.W.; Groh, M. The role of concussion history and gender in recovery form soccer-related concussion. Am. J. Sport. Med. 2009, 37, 1699–1704. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fight Result | M | W | Total |
|---|---|---|---|
| KO with head trauma | 32.2% (746) | 23.1% (39) | 31.6% (785) |
| Other cause | 67.8% (1573) | 76.9% (130) | 68.4% (1703) |
| Total | 2319 | 169 | 2488 |
| Weight Category | KO with Head Trauma | Other Reason | Total | |
|---|---|---|---|---|
| Male fights | Flyweight | 12.5% (9) | 87.5% (63) | 72 |
| Bantamweight | 28.7% (49) | 71.3% (122) | 171 | |
| Featherweight | 26.9% (49) | 73.1% (133) | 182 | |
| Lightweight | 24.5% (108) | 75.5% (333) | 441 | |
| Middleweight | 31% (111) | 69% (247) | 358 | |
| Welterweight | 29.5% (143) | 341 (70.5%) | 484 | |
| Light heavyweight | 38% (116) | 62% (189) | 305 | |
| Heavyweight | 54% (156) | 46% (133) | 289 | |
| Catch weight bout | 29.4% (5) | 70.6% (12) | 17 | |
| Female fights | Strawweight | 16.9% (11) | 83.1% (54) | 65 |
| Flyweight | 16.7% (6) | 83.3% (30) | 36 | |
| Bantamweight | 31.6% (18) | 68.4% (39) | 57 | |
| Featherweight | 36.4% (4) | 63.6% (7) | 11 | |
| Total | 31.6% (785) | 68.4% (1703) | 2488 | |
| Fight Result | M | W | Total |
|---|---|---|---|
| KO with head trauma | 88.1% (741) | 88.6% (39) | 88.1% (780) |
| Other reason | 11.9% (100) | 11.4% (5) | 11.9% (105) |
| Total | 841 | 44 | 885 |
| Weight Category | N | Duration of Fight to End by KO with Head Injury | ||
|---|---|---|---|---|
| M | SD | |||
| Male fights | Flyweight | 9 * | 4 min 30 s | 1 min 33 s |
| Bantamweight | 49 | 7 min 36 s | 6 min 3 s | |
| Featherweight | 49 | 7 min 36 s | 4 min 35 s | |
| Lightweight | 108 | 5 min 41 s | 4 min 20 s | |
| Middleweight | 111 | 6 min 8 s | 3 min 59 s | |
| Welterweight | 143 | 5 min 37 s | 4 min 37 s | |
| Light heavyweight | 116 | 4 min 58 s | 3 min 41 s | |
| Heavyweight | 156 | 5 min 59 s | 4 min 40 s | |
| Catch weight bout | 5 * | 3 min 24 s | 1 min 26 s | |
| Female fights | Strawweight | 11 * | 7 min 12 s | 4 min 45 s |
| Flyweight | 6 * | 8 min 54 s | 1 min 55 s | |
| Bantamweight | 18 * | 6 min 25 s | 5 min 50 s | |
| Featherweight | 4 * | 4 min 18 s | 5 min 13 s | |
| Total | 785 | 5 min 57 s | 4 min 31 s | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mańka-Malara, K.; Mierzwińska-Nastalska, E. Head Trauma Exposure in Mixed Martial Arts. Int. J. Environ. Res. Public Health 2022, 19, 13050. https://doi.org/10.3390/ijerph192013050
Mańka-Malara K, Mierzwińska-Nastalska E. Head Trauma Exposure in Mixed Martial Arts. International Journal of Environmental Research and Public Health. 2022; 19(20):13050. https://doi.org/10.3390/ijerph192013050
Chicago/Turabian StyleMańka-Malara, Katarzyna, and Elżbieta Mierzwińska-Nastalska. 2022. "Head Trauma Exposure in Mixed Martial Arts" International Journal of Environmental Research and Public Health 19, no. 20: 13050. https://doi.org/10.3390/ijerph192013050
APA StyleMańka-Malara, K., & Mierzwińska-Nastalska, E. (2022). Head Trauma Exposure in Mixed Martial Arts. International Journal of Environmental Research and Public Health, 19(20), 13050. https://doi.org/10.3390/ijerph192013050