Abstract
Zoonotic epidemics and pandemics have become frequent. From HIV/AIDS through COVID-19, they demonstrate that pandemics are social processes as well as health occurrences. The roots of these pandemics lie in changes in the socioeconomic interface between humanity and non-human host species that facilitate interspecies transmission. The degree to which zoonoses spread has been increased by the greater speed and extent of modern transportation and trade. Pre-existing sociopolitical and economic structures and conflicts in societies also affect pathogen propagation. As an epidemic develops, it can itself become a social and political factor, and change and interact with pre-existing sociobehavioral norms and institutional structures. This paper uses a “Big Events” approach to frame these processes. Based on this framework, we discuss how social readiness surveys implemented both before and during an outbreak might help public health predict how overall systems might react to an epidemic and/or to disease control measures, and thus might inform interventions to mitigate potential adverse outcomes or possibly preventing outbreaks from developing into epidemics. We conclude by considering what “pathways measures”, in addition to those we and others have already developed, might usefully be developed and validated to assist outbreak and epidemic disease responses.
1. Introduction
Zoonotic pandemics and emerging infectious disease highlight the challenges that emerge from varying interfaces and interactions among humans and non-human organisms in environments. Some of the changes in interaction patterns are caused by environmental changes due to global climate change which alters the environments in which human and other organism interact [1,2,3,4]. Other gradual or sudden changes in human social processes, such as changes in the meat industry or military conquests can also lead to zoonotic pandemics and novel human infectious diseases if they lead to novel encounters with non-human animals and other organisms [5,6,7,8,9,10,11,12,13]. Theoretic frameworks for the study of zoonotic infections that incorporate measures of human social processes can help us understand, predict and address zoonotic pandemics.
We have previously developed a “Big Events” framework for research and interventions on pandemics, including zoonotic pandemics, that create, or occur under, situations of social emergency and interact with pre-existing social structures and processes [14,15]. We developed this perspective out of analysis of HIV/AIDS outbreaks that took place in the countries of the former Soviet Union after the dissolution of the USSR; in South Africa after the end of apartheid; and in Indonesia after the economic crisis and overthrow of the dictatorship in the late 1990s [7,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34]. The global HIV epidemic is a zoonotic pandemic that arose from the transmission of a primate retrovirus to humans. This transmission took place due to new patterns of human-primate interaction during the European conquest and exploitation of Africa, and HIV then spread from colonial Africa across the world during the mid-20th century and beyond [35,36,37]. We refined this framework based on what we learned by applying it to an HIV upsurge which occurred in Athens, Greece, amidst financial and economic crisis [15,23]. Importantly, such HIV outbreaks appear to be historically and contextually contingent–similar events in Argentina early this century did not lead to an HIV outbreak despite there being a sizable number of infected people who could have served as seeds for a wide epidemic [14,15].
As the COVID-19 pandemic has made clear, zoonotic pandemics can create economic and social crises as well as a generalized sociopolitical discontinuity in society as in South Africa during the late 1990s and for some years thereafter [12,38]. Historically, in the mid-400s BC a zoonotic epidemic (which may been either plague or typhus) devastated the Athenian city-state causing major social and economic disruption and probably contributing to its collapse and loss in the Peloponnesian war, and in the 6th Century AD, plague epidemics (caused by Yersinia pestis) caused sociopolitical crises that contributed (along with other factors) to the decline of the Roman Empire [39]. Subsequent plague epidemics in the 13th and 14th centuries, introduced by increased trade among geographic regions, caused massive mortality, demographic and social upheavals that contributed to the decline of feudalism in Europe and to the rise of capitalism as the dominant mode of social production in Europe (and subsequently elsewhere) [38,40,41,42,43]. The invasion of the Americas by European settler-colonialists and slave traders in the 16th century, and critically the zoonotic pathogens which traveled with them, led to massive disruption and destruction of indigenous cultures and political systems [38,41]. A cholera epidemic which occurred in Paris in 1832 interacted with pre-existing social tensions to contribute to the Paris Uprising of that year and to subsequent government repression [44]. The 1918 influenza pandemic occurred in the context of the human morbidity mortality and destruction of built environments caused by World War I, and caused further massive social disruption in Europe, Russia, the US and elsewhere [45,46]. A recent International Monetary Fund working paper found a strong, but complex, relationship between epidemics and ‘social unrest’ events in the period 1990–2019 [44]. These selected examples demonstrate the long history of pandemics both arising in the context of sociopolitical stresses, and causing significant sociopolitical disruption.
Standard approaches to understand the epidemiology of pandemics and to inform planning and mitigation strategies are often based on forms of the agent-host-environment model [47]. The agent-host-environment model used in these standard approaches typically incorporates measures of individual human biologic and behavioral characteristics, group-level human characteristics (e.g., population prevalence of pathogen, or ‘herd’ immunity), measures of pathogen (agent) characteristics (e.g., virulence and transmissibility) and measures of selected environmental (contextual) characteristics. While these factors are necessary to understand epidemic curves (i.e., trajectories of epidemics over time), they do not fully account for how the agent, the host or the environment interact and change over time. Neither the standard measures nor the agent-host-environment model in-and-of-itself adequately reflects or articulates many important social processes which are both socially plausible (where social plausibility is a form of face validity analogous to biologic plausibility) and available data suggest to be key factors that shape how pandemics change over time [48] A framework to understand zoonotic epidemics should more fully consider the time-varying and dialectical interactions among pathogenic evolution, medical interventions, policies, social and economic processes and conditions, and human behavior. The “Big Events” framework, which is the focus of this paper, could be useful in understanding and seeking to prevent and mitigate such epidemics.
One key element of this framework is that it includes many social processes and relationships that are rarely considered in epidemiologic or prevention research and policy. These include processes and structures that can currently be measured, as well as others for which measurements could be developed. Measuring these processes and how they change before and during an epidemic could enhance the understanding of pandemic trajectories, as well as their prediction and mitigation. We propose that a number of novel measures should be included in a system of “social readiness surveys” that ideally should be begun and maintained over time before, during and between epidemics.
We developed a “pathways model” based on our and others’ previous work to explain how Big Events affect social, behavioral and economic processes that in turn affect HIV incidence rates or other epidemiologic outcomes [27,29,30,31,32,33]. These pathways include a large number of social processes for which no then-existing measures existed. We conducted mixed methods research to develop and validate a number of survey scales and free-standing items to measure social processes including intergenerational normative disjuncture [30], increases in the magnitude or sources of dignity attacks on various groups in the population [31], of individual and group altruism and solidarity [32], and other important social process constructs [29,30,49].
As a considerable body of past research shows [10,13,50], there is every reason to predict that the combined and interacting impacts of economically-driven human incursions into, and the redevelopment of, forestlands, savannahs, and other areas where potential vectors and potential emerging pathogens exist; the ecological interface between industrialized animal husbandry and naturally occurring wildlife; the commodification and privatization of sources of water and of aquatic food chains and destruction of aquatic ecosystems; and global climate change will lead to major future zoonotic pandemics that may well be socially disruptive [51,52,53]. Further, as has occurred in the United States, France, and Brazil during the COVID-19 pandemic, pandemic related socioeconomic disruptions may interact with pre-existing social and political inequities and/or pre-existing political divisions to render public health policy and practice a contentious political issue. This then may feed back to weaken public health policies and contribute to disease spread. In addition, the COVID-19 pandemic and responses to it have led to delays in elections, some of which have been contentious and contested (e.g., in Ethiopia) and have been used a means of justifying repression and suspension of the rule of law (e.g., in Uganda in which the party in power held large rally events but cited the pandemic as a putative rationale to prevent opposition party rallies) [54].
In this brief article, we will present a preliminary framework and model of how these processes might form an interactive system in a nation or other jurisdiction. Based on this model, we will discuss how social readiness surveys implemented both before and during an outbreak might help public health actors predict how the overall system might react to an epidemic and/or to disease control measures and thus might help inform interventions to mitigate potential adverse outcomes (including possibly preventing outbreaks from developing into epidemics). We will conclude by considering what additional “pathways measures”, in addition to those we and others have developed, might usefully be developed and validated by researchers to be incorporated in outbreak and epidemic disease responses.
2. A General Framework of Response to a Zoonotic Outbreak
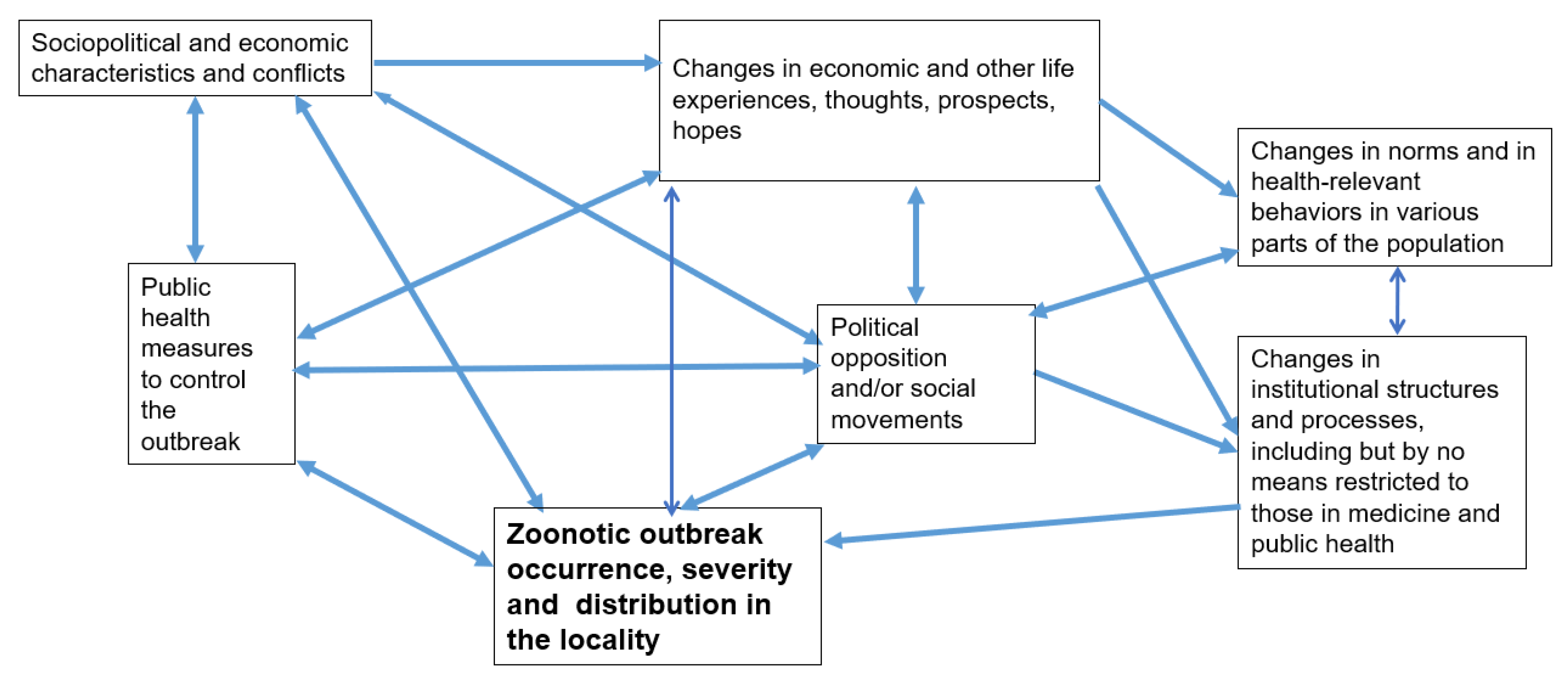
Experience with both HIV/AIDS and COVID-19 makes it clear that the effects of a zoonotic disease outbreak on a population depend on pre-existing sociopolitical conditions (a term that includes economics as well), public health responses, the ways in which the outbreak and responses to it affect the life experiences, thoughts and hopes of different sections of the population, and changes in the norms and health-relevant behaviors of various parts of the population [27]. (See Figure 1) Importantly, all of these considerations can precipitate mass political and social movements, shaped to varying degrees by pre-existing patterns of political conflict, stigmatization, household organization, economic inequality and exploitation, and institutionalized oppression or subordination [27,55,56]. In the case of COVID-19 in the United States (US), for example, the pandemic has caused far greater mortality for Native American, Latinx, and Black people than for white people; these disparities were also reflected both in politics (where the great majority of anti-vaccination and anti-masking activists have been white people, many of them overt racists) and perhaps in the huge antiracist demonstrations across the US in the summer of 2020 [14,57,58].
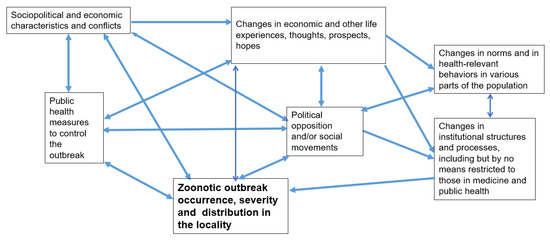
Figure 1.
General model of zoonotic outbreaks in a locality in a Big Events framework and what pre-existing social surveillance might be useful. Social surveillance should consider measuring all of the social variables referred to in the Figure. It should be noted that more than one Big Event can take place concurrently. If this occurs, complex interactions may lead to greater peril, depending on the social readiness to meet these other Big Events.
COVID-19 in the US (and elsewhere) has led to more financial hardship and job loss among women than men (particularly comparing those with children with those without or those who are immigrant with those who are not), with Latinx, Black, and indigenous females further impacted than their White female counterparts [59,60,61,62]. It is not clear what the political and long-range impacts of these disparities will be, nor of how they may influence change in the pandemic.
Social-level responses during times of zoonotic disease outbreaks can affect institutional structures and processes, including the funding, personnel, and structure of health departments, other health care and prevention services, other social and economic support systems, and police and the policies implemented to address the zoonotic outbreak, which can affect the effectiveness of responses and can sometimes lead to inequities in how groups experience outbreak or pandemic conditions [63,64,65]. Further, there is a considerable degree of interaction and reverse causation in these causal chains.
The Big Events framework is complex. Other global and local crises—specifically including global climate change and its local manifestations and the possibility of more than one, sometimes interacting, zoonotic outbreak at the same time and place—can shape these complex processes and potentially affect the pattern, distribution and severity of human and non-human zoonotic disease.
The current Big Events framework—and the social readiness surveys based on it—may be limited by their genesis in studying the HIV/AIDS and (to an extent) the COVID-19 pandemics. Future modifications should increase their power to explain other potential zoonotic pandemics such as those driven by vector-borne or waterborne disease transmission. Further specification of the economic processes involved in pandemics, such as supply-chain disruptions, should be based on understanding economic processes (which are best understood as social relations that are continually changing.) Production, finance and trade are all forms of social relations that can greatly shape emerging epidemics and efforts to mitigate, control or eliminate them [38,66].
Zoonotic pandemics have long been linked to trade routes including infections such as the plague, small pox, and HIV [38,66]. Commercial transportation and leisure travel (e.g., via cruise ships) were important venues for COVID-19 and SARS-1 disease transmission. Similarly, the congruence of human, birds and pigs in locations used by humans for commercial food production, such as rice paddies, brings these animal populations into contact and creates niches in which influenza variants emerge [1,62]. Food production in meatpacking plants also provided venues for widespread COVID-19 transmission, a process that was, in the USA at least, closely linked with racist social and economic practices that concentrated subordinated race/ethnicities in meatpacking jobs [67,68].
One measure of the degree to which governments have adopted neoliberal trade, taxation and other policies is the “economic freedom index” developed by the conservative Heritage Society. Although this measure has not, insofar as we are aware, been used to study zoonotic epidemics, it did prove useful in a study of the “non-communicable epidemic” of obesity. Higher “economic freedom” increases or ‘easier’ trade was associated with the prevalence of obesity, plausibly though increased trade in and increased consumption of fatty foods. This and analogous measures of socially mediated trade relationships could be explored for their relationship to zoonotic pandemics. Similarly, one could imagine measures of trade that relate volume on specific trade routes to global patterns of pathogen dissemination [69,70].
As an additional complication, pathogens constantly mutate at the genetic level due to errors in the replication process. These mutations may accumulate and generate strain variations which may be intrinsically more or less transmissible, more or less virulent, and more or less able to escape existing individual- and population-level immunity. These new strain variations are then subject to selection pressures in specific niches which may favor their replication and spread in that niche. Interventions such as antiretroviral treatment (e.g., for HIV/AIDS) or vaccination of human populations (for various infections) exert selection pressure on both original and newly emerged strains and may result in the selection and dissemination of new, and possibly more virulent or more transmissible strains. Further, as Paul Ewald and others have discussed, social structures and changing social contexts can create “social niches” that favor the rapid emergence and dissemination of pathogen variants [71,72,73,74]. As an example, Ewald discussed how the niches created by the social organization of military trenches and military medicine in World War I may have contributed to the emergence and dissemination of more virulent influenza strains. For HIV, such social niches probably included multi-person psychoactive drug injection sites, some brothels or sex worker “strolls”, and the multi-person use of syringes in clinical settings in some parts of Africa in the 1950s and after, and sex parties and other multi-partner settings prominent in gay clone cultures that developed in the US in the 1970s [71,73,75,76,77].
3. Example: The Covid-19 Outbreak in the US in a Big Events Framework
In order to illustrate in further detail how the general framework in Figure 1 might be applied, we discuss how upstream domains (boxes) highlighted in the framework have shaped the development of the Covid-19 epidemic in the US.
Pre-existing sociopolitical and economic characteristics and conflicts led to political polarization within multiple domains which directly relate to the COVID-19 epidemic and such responses to it as assessments of infection importance [78], “stay-at-home” measures [79], food production [80], regulation of religious gatherings [81], safety and effectiveness of medical treatments for COVID-19 infection [49,82], and “mandates” of both mask wearing [83] and COVID-19 vaccination [84]. These conflicts were reflected in the media, contributing as much to confusion and misinformation as to accurate health literacy (although differentially so for different subpopulations) [85,86]. This confusion interfered with the implementation of consistent and coordinated responses to the epidemic. These dynamics further contributed to a widely inequitable and unequal implementation of public health and public policy responses across US states [87] resulting in inconsistent and contradictory public health messages and in states, agencies and institutions competing for Federal support, as for example, in access to personal protective equipment, respirators, and medications and vaccines made available through emergency use authorizations prior to full product approval [88]. This early politicization emboldened political opposition to many public health responses. Social movements such as white nationalism and sections of anti-vaccine movements expanded their reach aided by the use social media platforms by humans and by the use of social media bots and artificial intelligence on these platforms [78,85]. At times anti-vaccine reactions manifested in physical threats to public health officials [89] and sometimes in armed demonstrations and violent attacks in state capitols [90,91].
This on-going multi-pronged polarization led to various patterns and changes in social norms and health relevant behaviors. Gardarian, et al. (2021) found that political party affiliation consistently predicted differences in health behaviors, beliefs, and attitudes related to COVID-19 [92]. Similarly, COVID-19 vaccination uptake has been consistently higher in counties that voted Democratic in the US presidential election compared with those which voted Republican, with the gap widening over time [93]; COVID-19 case rates, morbidity and mortality were also distributed differentially similarly.
Other changes caused by interactions across these domains were less contentious. These included some changes in behavioral practices such as handshaking and changes in institutional structures with possibly lasting impact such as normalization of remote working for occupations relying on primarily mental rather than manual labor (a COVID-19 response that may have exacerbated inequities in COVID-19 risk based on occupation and linked to race, ethnicity, gender and class inequities in employment and occupation), [94] expansion and acceptance of telemedicine [95,96], and reductions in the authority of many local and state health departments, including the dissolution of at least one health department (Tri-County, in Colorado) and rancorous policy disputes and elections focused on masks in schools.
The HIV/AIDS epidemic, thanks in great measure to self-mobilization of the most affected marginalized groups [97], led to medical advances such as redefining AIDS to include HIV-related conditions that affect women and people who use drugs, expanded access to clinical trials and accelerated approval of effective medicines. Activists’ efforts also led to public health measures such as promotion and distribution of condoms, harm reduction services and greater mainstream acceptance of LGBTQ communities and extension of their rights [98,99]. In contrast, the COVID-19 pandemic might have arguably weakened the ability of the US to respond to future epidemics by undermining its collective ability to enact and accept public health laws [100] that might be perceived (and politically promoted) as an attack on individual liberties.
4. Social Readiness Monitoring and Other Forms of Preparation and Learning
Very little research has been conducted on how the various factors in our pandemic framework interact with each other as a dynamic system. One reason is that many of the constructs involved have rarely been measured. For some of them, validated measures may not exist. Our team developed a set of “pathways measures” to describe changing local social conditions and including emerging new norms that might shape how Big Events or macrosocial “structural” interventions would affect HIV/AIDS epidemics [27,30,31,32,33]. For example, we used one set of these measures (i.e., of norms that encouraged risky behaviors including use of unsterile injection equipment) in Athens, Greece following an outbreak of HIV among people who inject drugs (PWID) between 2011–2013 [101,102]. Although numbers of diagnosed HIV infections had decreased when we collected these data (2013–2015), both overall socioeconomic conditions and the norms of many people who inject drugs favored high risk drug injection contexts and behaviors. Unsurprisingly, in 2018–2020, the prevalence of HIV among PWID in Athens had increased to 22% from 14% in 2013, and there is also evidence for high transmission in Greece’s second largest city (Thessaloniki) [103].
Further, social movement scholars and others have developed methods to study political and social movements, and both large population level surveys (e.g., census data, national labor statistic surveys) and market research often measure other variables highlighted in Figure 1. Insofar as we are aware, little-to-no work has yet combined these sets of variables with data on pathogen phylogenetics, the emergence, diversity and dissemination of pathogen variants and epidemic curves, and relevant outcomes in human (or non-human) populations. This is an area of potentially important future work with direct implications to both public health and public policy.
As discussed above, we suggest that it might be very useful to establish integrated real-time social readiness monitoring and surveillance systems for as many of these variables as can be measured to allow development of both predictive and explanatory models to help prepare responses for potential outbreaks and to prevent or respond quickly to potential outbreaks. Social readiness surveys could be combined with other population-level census and economic census data, along with pathogen surveillance systems, to provide measures of many of the variables in our framework. If such systems can be established in enough localities, it would also enable researchers to begin to understand the interactions of the complex system depicted in Figure 1. The relevance of different “pathways variables” may vary depending on characteristics of the pathogen in question. Some of the measures we developed to study HIV epidemics may be useful for other zoonotic infection epidemics as well [29,30,32]. For respiratory infections such as COVID-19, patterns of close proximity at workplaces (particularly indoor, poorly ventilated workplaces), housing (particularly crowded, poorly ventilated housing, including congregate settings such as shelters, homes for aged populations, prisons and jails), as well as the norms, institutions and laws that affect these, will be crucial measures [55,104,105,106,107,108]. For vector-borne infections or water-borne infections, still other pathways variables might need to be developed. We expect that other pathways variables, such as those on altruism and patterns of solidarity and conflict within a population, are relevant to all pandemics.
In conclusion, we suggest that establishing both pathogenic real-time surveillance systems and social readiness surveys could help the human response to zoonotic outbreaks by more fully considering changes in human social process that affect, respond to, and form part of the environment in which human zoonotic pathogens emerge and disseminate. The transdisciplinary nature of the Big Events framework and of forms of social readiness monitoring bring challenges. Yet, the development of measures and methods of enhanced social readiness monitoring, and pandemic surveillance models to inform public health and societal responses, hold promise for improving human responses to current and future pandemics.
Author Contributions
Each author contributed to the conceptualization and writing of this paper. Each author has approved the final version, and agrees to be personally responsible for the paper. S.R.F. was the initiating author; during the writing, each author has made a substantial contribution to all aspects of the paper. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the US National Institute on Drug Abuse under Grant numbers P30DA011041, R01DA031597, R01DA041298, R01DA041501, 5T32DA007233, and DP1DA034989. The funding sources had no role in the design and conduct of the paper; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Institutional Review Board Statement
This paper is a contribution to zoonotic epidemic theory, policy discussion, monitoring, and prevention and does not involve human subjects research. Each of the research projects listed above as sources of support has been approved by the relevant Institutional Review Boards. For purposes of this paper, “not applicable” is the relevant category.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The sponsors had no role in the design, execution, interpretation, or writing of the study.
References
- Wallace, R. Dead Epidemiologists: On the Origins of COVID-19; Monthly Review Press: New York, NY, USA, 2020. [Google Scholar]
- Baylis, M. Potential impact of climate change on emerging vector-borne and other infections in the UK. Environ. Health 2017, 16, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Short, E.E.; Caminade, C.; Thomas, B.N. Climate change contribution to the emergence or re-emergence of parasitic diseases. Infect. Dis. Res. Treat. 2017, 10, 1178633617732296. [Google Scholar] [CrossRef] [Green Version]
- Bartlow, A.W.; Manore, C.; Xu, C.; Kaufeld, K.A.; Del Valle, S.; Ziemann, A.; Fairchild, G.; Fair, J.M. Forecasting Zoonotic Infectious Disease Response to Climate Change: Mosquito Vectors and a Changing Environment. Vet. Sci. 2019, 6, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobson, A.P.; Pimm, S.L.; Hannah, L.; Kaufman, L.; Ahumada, J.A.; Ando, A.W.; Bernstein, A.; Busch, J.; Daszak, P.; Engelmann, J.; et al. Ecology and economics for pandemic prevention. Science 2020, 369, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Davis, M. Monster at Our Door: The Global Threat of Avian Flu. BMJ 2005, 331, 1275. [Google Scholar]
- Friedman, S.R. Environmental change and infectious diseases in the Mediterranean region and the world: An interpretive dialectical analysis. Euro-Mediterr. J. Environ. Integr. 2021, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Malm, A. Corona, Climate, Chronic Emergency: War Communism in the Twenty-First Century; Verso Books: London, UK, 2020. [Google Scholar]
- Sharp, P.M.; Hahn, B.H. Origins of HIV and the AIDS Pandemic. Cold Spring Harb. Perspect. Med. 2011, 1, a006841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wernecke, B.; Millar, D.A.; Walters, M.; Ganswindt, A.; Dziba, L.; Wright, C.Y. Preventing the next pandemic’—A 2020 UNEP Frontiers Series Report on zoonotic diseases with reflections for South Africa. S. Afr. J. Sci. 2020, 116, 1–4. [Google Scholar] [CrossRef]
- Wallace, R. Big Farms Make Big Flu: Dispatches on Infectious Disease, Agribusiness, and the Nature of Science; Monthly Review Press: New York, NY, USA, 2016. [Google Scholar]
- Wallace, R.; Liebman, A.; Chaves, L.F.; Wallace, R. COVID-19 and the Circuits of Capital: New York to China and Back. Mon. Rev. 2020, 72, 1–15. [Google Scholar] [CrossRef]
- Weiss, R.A.; McMichael, A.J. Social and environmental risk factors in the emergence of infectious diseases. Nat. Med. 2004, 10 (Suppl. 12), S70–S76. [Google Scholar] [CrossRef]
- Friedman, S.R.; Mateu-Gelabert, P.; Nikolopoulos, G.K.; Cerdá, M.; Rossi, D.; Jordan, A.E.; Townsend, T.; Khan, M.R.; Perlman, D.C. Big Events theory and measures may help explain emerging long-term effects of current crises. Glob. Public Heal. 2021, 16, 1167–1186. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.R.; Rossi, D.; Braine, N. Theorizing “Big Events” as a potential risk environment for drug use, drug-related harm and HIV epidemic outbreaks. Int. J. Drug Policy 2009, 20, 283–291. [Google Scholar] [CrossRef]
- Rhodes, T.; Lowndes, C.; Judd, A.; Mikhailova, L.A.; Sarang, A.; Rylkov, A.; Tichonov, M.; Lewis, K.; Ulyanova, N.; Alpatova, T.; et al. Explosive spread and high prevalence of HIV infection among injecting drug users in Togliatti City, Russia. AIDS 2002, 16, F25–F31. [Google Scholar] [CrossRef] [PubMed]
- Aral, S.O.; Lawrence, J.S.S. The Ecology of Sex Work and Drug Use in Saratov Oblast, Russia. Sex. Transm. Dis. 2002, 29, 798–805. [Google Scholar] [CrossRef] [Green Version]
- Strathdee, S.A.; Stachowiak, J.A.; Todd, C.S.; Al-Delaimy, W.K.; Wiebel, W.; Hankins, C.; Patterson, T.L. Complex emergencies, HIV, and substance use: No “big easy” solution. Subst. Use Misuse 2006, 41, 1637–1651. [Google Scholar] [CrossRef]
- Lagerspetz, M.; Moskalewicz, J. Drugs in the Postsocialist Transitions of Estonia, Latvia, Lithuania and Poland. Eur. Addict. Res. 2002, 8, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.; Rossi, D.; Phaswana-Mafuya, N. Globalization and Interacting Large-Scale Processes and How They May Affect the HIV/AIDS Epidemic. In Globalizing Theory on HIV/AIDS; Routledge, Inc.: New York, NY, USA, 2009; pp. 491–500. [Google Scholar]
- Friedman, S.R.R. Gary, The need for dialectical models as shown in the response to the HIV/AIDS epidemic. Int. J. Sociol. Soc. Policy 2002, 22, 177–200. [Google Scholar] [CrossRef]
- Jenkins, R.; Klein, J.; Parker, C. Mental health in post-communist countries. BMJ 2005, 331, 173–174. [Google Scholar] [CrossRef] [Green Version]
- Nikolopoulos, G.K.; Sypsa, V.; Bonovas, S.; Paraskevis, D.; Malliori-Minerva, M.; Hatzakis, A.; Friedman, S.R. Big Events in Greece and HIV Infection Among People Who Inject Drugs. Subst. Use Misuse 2015, 50, 825–838. [Google Scholar] [CrossRef] [Green Version]
- Vasylyeva, T.I.; Liulchuk, M.; Friedman, S.R.; Sazonova, I.; Faria, N.R.; Katzourakis, A.; Babii, N.; Scherbinska, A.; Thézé, J.; Pybus, O.G.; et al. Molecular epidemiology reveals the role of war in the spread of HIV in Ukraine. Proc. Natl. Acad. Sci. USA 2018, 115, 1051–1056. [Google Scholar] [CrossRef] [Green Version]
- Pouget, E.R.; Sandoval, M.; Nikolopoulos, G.K.; Friedman, S.R. Immediate Impact of Hurricane Sandy on People Who Inject Drugs in New York City. Subst. Use Misuse 2015, 50, 878–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, S.R.; Rossi, D. Some Musings About Big Events and the Past and Future of Drug Use and of HIV and Other Epidemics. Subst. Use Misuse 2015, 50, 899–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, S.R.; Sandoval, M.; Mateu-Gelabert, P.; Rossi, D.; Gwadz, M.; Dombrowski, K.; Smyrnov, P.; Vasylyeva, T.; Pouget, E.R.; Perlman, D. Theory, measurement and hard times: Some issues for HIV/AIDS research. AIDS Behav. 2013, 17, 1915–1925. [Google Scholar] [CrossRef] [Green Version]
- Friedman, S.R.; Kippax, S.C.; Phaswana-Mafuya, N.; Rossi, D.; Newman, C.E. Emerging future issues in HIV/AIDS social research. AIDS 2006, 20, 959–965. [Google Scholar] [CrossRef]
- Friedman, S.R.; Pouget, E.R.; Sandoval, M.; Nikolopoulos, G.K.; Mateu-Gelabert, P.; Rossi, D.; Auerbach, J.D. New Measures for Research on Men Who Have Sex with Men and for At-Risk Heterosexuals: Tools to Study Links Between Structural Interventions or Large-Scale Social Change and HIV Risk Behaviors, Service Use, and Infection. AIDS Behav. 2020, 24, 257–273. [Google Scholar] [CrossRef]
- Pouget, E.R.; Sandoval, M.; Nikolopoulos, G.K.; Mateu-Gelabert, P.; Rossi, D.; Smyrnov, P.; Jones, Y.; Friedman, S.R. Developing Measures of Pathways that May Link Macro Social/Structural Changes with HIV Epidemiology. AIDS Behav. 2016, 20, 1808–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, S.R.; Pouget, E.R.; Sandoval, M.; Rossi, D.; Mateu-Gelabert, P.; Nikolopoulos, G.K.; Schneider, J.A.; Smyrnov, P.; Stall, R.D. Interpersonal Attacks on the Dignity of Members of HIV Key Populations: A Descriptive and Exploratory Study. AIDS Behav. 2017, 21, 2561–2578. [Google Scholar] [CrossRef]
- Friedman, S.R.; Pouget, E.R.; Sandoval, M.; Jones, Y.; Nikolopoulos, G.K.; Mateu-Gelabert, P. Measuring Altruistic and Solidaristic Orientations Toward Others Among People Who Inject Drugs. J. Addict. Dis. 2015, 34, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Friedman, S.R.; Pouget, E.R.; Sandoval, M.; Jones, Y.; Mateu-Gelabert, P. Formal and Informal Organizational Activities of People Who Inject Drugs in New York City: Description and Correlates. J. Addict. Dis. 2015, 34, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunting, A.M.; Frank, D.; Arshonsky, J.; Bragg, M.A.; Friedman, S.R.; Krawczyk, N. Socially-supportive norms and mutual aid of people who use opioids: An analysis of Reddit during the initial COVID-19 pandemic. Drug Alcohol Depend. 2021, 222, 108672. [Google Scholar] [CrossRef]
- Jones, K.E.; Patel, N.G.; Levy, M.A.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global trends in emerging infectious diseases. Nature 2008, 451, 990–993. [Google Scholar] [CrossRef]
- Wolfe, N.D.; Dunavan, C.P.; Diamond, J. Origins of major human infectious diseases. Nature 2007, 447, 279–283. [Google Scholar] [CrossRef]
- Hahn, B.H.; Shaw, G.M.; De, K.M.; Cock; Sharp, P.M. AIDS as a zoonosis: Scientific and public health implications. Science 2000, 287, 607–614. [Google Scholar] [CrossRef] [Green Version]
- McNeill, W.H.; McNeill, W. Plagues and Peoples; Anchor: New York, NY, USA, 1998. [Google Scholar]
- Harper, K. The Fate of Rome; Princeton University Press: Princeton, NJ, USA, 2017. [Google Scholar]
- Anievas, A.; Nişancıoğlu, K. How the West Came to Rule: The Geopolitical Origins of Capitalism; Pluto Press: London, UK, 2015. [Google Scholar]
- Crosby, A.W. Ecological Imperialism: The Biological Expansion of Europe, 900–1900; Cambridge University Press: New York, NY, USA, 2004. [Google Scholar]
- Tudela, F. El encuentro entre dos mundos: Impacto ambiental de la conquista. In Nueva Sociedad; NUEVA SOCIEDAD: Ciudad de Buenos Aires, Argentina, 1992; Volume 122, pp. 198–209. [Google Scholar]
- Abu-Lughod, J.L. Before European Hegemony: The World System A.D. 1250–1350; Oxford University Press: New York, NY, USA, 1989; p. 443. [Google Scholar]
- Barrett, P.; Chen, S. Social repercussions of pandemics. International Monetary Fund. 2021. Available online: https://www.imf.org/en/Publications/WP/Issues/2021/01/29/Social-Repercussions-of-Pandemics-50041 (accessed on 23 December 2021).
- Bristow, N. American Pandemic: The Lost Worlds of the 1918 Influenza Epidemic; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Martini, M.; Gazzaniga, V.; Bragazzi, N.L.; Barberis, I. The Spanish Influenza Pandemic: A lesson from history 100 years after 1918. J. Prev. Med. Hyg. 2019, 60, E64. [Google Scholar]
- Da Silva, P.G.; Mesquita, J.R.; Nascimento, M.d.S.J.; Ferreira, V.A.M. Viral, host and environmental factors that favor anthropozoonotic spillover of coronaviruses: An opinionated review, focusing on SARS-CoV, MERS-CoV and SARS-CoV-2. Sci. Total Environ. 2021, 750, 141483. [Google Scholar] [CrossRef] [PubMed]
- Adimora, A.A.; Auerbach, J.D. Structural interventions for HIV prevention in the United States. J. Acquir. Immune Defic. Syndr. 2010, 55, S132–S135. [Google Scholar] [CrossRef] [Green Version]
- Baker, P.; Rogers, K.; Enrich, D.; Haberman, M. Trump’s aggressive advocacy of malaria drug for treating coronavirus divides medical community. New York Times, 6 April 2021. Available online: https://www.nytimes.com/2020/04/06/us/politics/coronavirus-trump-malaria-drug.html (accessed on 10 January 2022).
- Baker, R.E.; Mahmud, A.S.; Miller, I.F.; Rajeev, M.; Rasambainarivo, F.; Rice, B.L.; Takahashi, S.; Tatem, A.J.; Wagner, C.E.; Wang, L.-F.; et al. Infectious disease in an era of global change. Nat. Rev. Genet. 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Xagoraraki, I. A water-focused one-health approach for early detection and prevention of viral outbreaks. One Health 2019, 7, 100094. [Google Scholar] [CrossRef]
- Solomon, S. Water: The Epic Struggle for Wealth, Power, and Civilizatio; Harper: New York, NY, USA, 2010. [Google Scholar]
- Partelow, S. Private Oceans: The Enclosure and Marketisation of the Seas by Fiona Mccormack, London, Pluto Press, 2017, 184 Pp.£ 24.99 (Paperback), ISBN: 978-0-7453-9910. J. Marit. Res. 2019, 21, 155–158. [Google Scholar] [CrossRef]
- Kennedy, A.; Resnick, D. Governing a Crisis and Crises of Governance: The Political Dimensions of COVID-19; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2021. [Google Scholar] [CrossRef]
- Lönnroth, K.; Jaramillo, E.; Williams, B.; Dye, C.; Raviglione, M. Drivers of tuberculosis epidemics: The role of risk factors and social determinants. Soc. Sci. Med. 2009, 68, 2240–2246. [Google Scholar] [CrossRef] [PubMed]
- Morris, A. Reflections on social movement theory: Criticisms and proposals. Contemp. Sociol. 2000, 29, 445–454. [Google Scholar] [CrossRef]
- O’Connor, C. The Conspiracy Consortium Examining Discussions of COVID-19 Among Right-Wing Extremist Telegram Channels; Institute for Strategic Dialogue (ISD): London, UK, 2021. [Google Scholar]
- Umair Majid, J.T.; Wasim, A.; Truong, M. Anti-Mask Protests and Racism: What Is the Link? Longwoods Insights 2020. Available online: https://www.longwoods.com/content/26390/anti-mask-protests-and-racism-what-is-the-link- (accessed on 18 December 2021).
- Holder, M.; Jones, J.; Masterson, T. The Early Impact of Covid-19 on Job Losses among Black Women in the United States. Fem. Econ. 2021, 27, 103–116. [Google Scholar] [CrossRef]
- Dias, F.A.; Chance, J.; Buchanan, A. The motherhood penalty and The fatherhood premium in employment during covid-19: Evidence from The united states. Res. Soc. Strat. Mobil. 2020, 69, 100542. [Google Scholar] [CrossRef]
- Saenz, R.; Sparks, C. The Inequities of Job Loss and Recovery Amid the COVID-19 Pandemic. 2020. Available online: https://doi.org/10.34051/p/2021.3 (accessed on 23 December 2021).
- Fearnley, L. Virulent Zones: Animal Disease and Global Health at China’s Pandemic Epicenter; Duke University Press: Durham, NC, USA, 2020. [Google Scholar]
- Galea, S. The Contagion Next Time; Oxford University Press: Oxford, UK, 2021. [Google Scholar]
- Krieger, N. Ecosocial Theory, Embodied Truths, and the People’s Health; Oxford University Press: Oxford, UK, 2021. [Google Scholar]
- Scientists under attack and weird viruses—The week in infographics. Nature 2021. Available online: https://doi.org/10.1038/d41586-021-02817-8 (accessed on 1 January 2022). [CrossRef]
- Piret, J.; Boivin, G. Pandemics throughout history. Front. Microbiol. 2020, 11, 631736. [Google Scholar] [CrossRef]
- Saitone, T.L.; Schaefer, K.A.; Scheitrum, D.P. COVID-19 Morbidity and Mortality in U.S. Meatpacking Counties. Food Policy 2021, 101, 102072. [Google Scholar] [CrossRef]
- Taylor, C.A.; Boulos, C.; Almond, D. Livestock plants and COVID-19 transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 31706–31715. [Google Scholar] [CrossRef]
- Lawson, R.A.; Murphy, R.H.; Williamson, C.R. The relationship between income, economic freedom, and BMI. Public Health 2016, 134, 18–25. [Google Scholar] [CrossRef]
- Vogli, R.D.; Kouvonen, A.; Elovainio, M.; Marmot, M. Economic globalization, inequality and body mass index: A cross-national analysis of 127 countries. Crit. Public Health 2014, 24, 7–21. [Google Scholar] [CrossRef]
- Ewald, P.W. Evolution of Infectious Disease; Oxford University Press: Oxford, UK, 1994. [Google Scholar]
- Ewald, P.W. Host-parasite relations, vectors, and the evolution of disease severity. Annu. Rev. Ecol. Syst. 1983, 14, 465–485. [Google Scholar] [CrossRef]
- Friedman, S.R.; Rossi, D. Dialectical theory and the study of HIV/AIDS and other epidemics. Dialect. Anthr. 2011, 35, 403–427. [Google Scholar] [CrossRef] [Green Version]
- Goodman, J.R. An evolving crisis. New Sci. 2020, 246, 41–45. [Google Scholar] [CrossRef]
- Weinstein, L. Street Corner Secrets: Sex, Work, and Migration in the City of Mumbai; SAGE Publications: Los Angeles, CA, USA, 2016. [Google Scholar]
- Beheyt, P. Contribution a l’etude des hepatites en Afrique. L’hepatite epidemique et l’hepatite par inoculation. Ann. Soc. Bel. Med. Trop. 1953, 33, 297–340. [Google Scholar]
- Levine, M.P.; Kimmel, M. Gay Macho: The Life and Death of the Homosexual Clone; NYU Press: New York, NY, USA, 1998. [Google Scholar]
- Wadman, M. Antivaccine forces gaining online. Science 2020, 368, 699. [Google Scholar] [CrossRef]
- Mervosh, S.; Lu, D.; Swales, V. See which states and cities have told residents to stay at home. New York Times, 20 April 2020. Available online: https://www.nytimes.com/interactive/2020/us/coronavirus-stay-at-home-order.html (accessed on 31 March 2020).
- Kimberly Kindy, T.M.A.R.H. The Trump administration approved faster line speeds at chicken plants. Those facilities are more likely to have covid-19 cases. Washington Post 2021. Available online: https://www.washingtonpost.com/politics/trump-chicken-covid-coronavirus-biden/2021/01/03/ea8902b0-3a39-11eb-98c4-25dc9f4987e8_story.html (accessed on 3 January 2021).
- Liptak, A. Splitting 5 to 4, Supreme Court Backs Religious Challenge to Cuomo’s Virus Shutdown Order. New York Times, 26 November 2020. Available online: https://www.nytimes.com/2020/11/26/us/supreme-court-coronavirus-religion-new-york.html (accessed on 1 January 2022).
- Blevins, J.L.; Edgerton, E.; Jason, D.P.; Lee, J.J. Shouting Into the Wind: Medical Science versus “B.S.” in the Twitter Maelstrom of Politics and Misinformation About Hydroxychloroquine. Soc. Media + Soc. 2021, 7. [Google Scholar] [CrossRef]
- Shin, S.H.; Ji, H.; Lim, H. Heterogeneity in preventive behaviors during COVID-19: Health risk, economic insecurity, and slanted information. Soc. Sci. Med. 2021, 278, 113944. [Google Scholar] [CrossRef] [PubMed]
- Pennycook, G.; McPhetres, J.; Bago, B.; Rand, D. Beliefs about COVID-19 in Canada, the UK, and the USA: A novel test of political polarization and motivated reasoning. PsyArXiv 2021. [Google Scholar] [CrossRef]
- Himelein-Wachowiak, M.; Giorgi, S.; Devoto, A.; Rahman, M.; Ungar, L.; Schwartz, H.A.; Epstein, D.H.; Leggio, L.; Curtis, B. Bots and Misinformation Spread on Social Media: Implications for COVID-19. J. Med. Internet Res. 2021, 23, e26933. [Google Scholar] [CrossRef]
- Al Khaja, K.A.; AlKhaja, A.K.; Sequeira, R.P. Drug information, misinformation, and disinformation on social media: A content analysis study. J. Public Health Policy 2018, 39, 343–357. [Google Scholar] [CrossRef] [PubMed]
- Cornwall, W.; Kaiser, J.; Kupferschmidt, K.; Malakoff, D.; Servick, K. The United States leads in coronavirus cases, but not pandemic response. Science News, 1 April 2020. [Google Scholar]
- Ranney, M.L.; Griffeth, V.; Jha, A.K. Critical supply shortages—the need for ventilators and personal protective equipment during the Covid-19 pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef]
- Ivory, M.B.A.D. Why Public Health Faces a Crisis Across the U.S. New York Times, 18 October 2021. Available online: https://www.nytimes.com/2021/10/18/us/coronavirus-public-health.html (accessed on 23 December 2021).
- Coronavirus: Armed protesters enter Michigan statehouse. BBC, 1 May 2020. Available online: https://www.bbc.com/news/world-us-canada-52496514 (accessed on 23 December 2021).
- Sokolow, A. Hundreds protest in front of the State House over vaccine, mask mandates. Boston Herald, 17 September 2021. Available online: https://www.bostonherald.com/2021/09/17/hundreds-protest-in-front-of-the-state-house-over-vaccine-mask-mandates/ (accessed on 23 December 2021).
- Kushner, G.S.; Wallace, G.S.; Pepinsky Thomas, B. Partisanship, health behavior, and policy attitudes in the early stages of the COVID-19 pandemic. PLoS ONE 2021, 16, e0249596. [Google Scholar]
- Kates, J.; Orgera, K. The red/blue divide in COVID-19 vaccination rates is growing. Kaiser Family Foundation, 14 September 2021. Available online: https://www.kff.org/policy-watch/the-red-blue-divide-in-covid-19-vaccination-rates/ (accessed on 23 December 2021).
- Parker, K.; Menasce Horowitz, J.; Minkin, R. How the Coronavirus Outbreak Has–and Hasn’t–Changed the Way Americans Work. Pew Res. Cent. 2020. Available online: https://www.pewresearch.org/social-trends/2020/12/09/how-the-coronavirus-outbreak-has-and-hasnt-changed-the-way-americans-work/ (accessed on 10 January 2022).
- Lukas, H.; Xu, C.; Yu, Y.; Gao, W. Emerging telemedicine tools for remote COVID-19 diagnosis, monitoring, and management. ACS Nano 2020, 14, 16180–16193. [Google Scholar] [CrossRef]
- Hincapié, M.A.; Gallego, J.C.; Gempeler, A.; Piñeros, J.A.; Nasner, D.; Escobar, M.F. Implementation and Usefulness of Telemedicine During the COVID-19 Pandemic: A Scoping Review. J. Prim. Care Community Heal. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Stockdill, B.C. ACT UP (Aids Coalition to Unleash Power). In The Wiley-Blackwell Encyclopedia of Social and Political Movements; Wiley: Malden, MA, USA, 2013; Available online: https://onlinelibrary.wiley.com/doi/book/10.1002/9780470674871 (accessed on 10 January 2022).
- Chappell, B. Supreme Court declares same-sex marriage legal in all 50 states. National Public Radio, 26 June 2015. Available online: https://www.npr.org/sections/thetwo-way/2015/06/26/417717613/supreme-court-rules-all-states-must-allow-same-sex-marriages (accessed on 23 December 2021).
- Epstein, S. Impure Science: Aids, Activism, and the Politics of Knowledge; University of California Press: Berkeley, CA, USA, 1996; p. 466. [Google Scholar]
- National Association of County and City Health Officials (NACCHO). Proposed Limits on Public Health Authority: Dangerous for Public Health. 2021. Available online: https://www.naccho.org/uploads/downloadable-resources/Proposed-Limits-on-Public-Health-Authority-Dangerous-for-Public-Health-FINAL-5.24.21pm.pdf (accessed on 10 January 2022).
- Hadjikou, A.; Pavlopoulou, I.D.; Pantavou, K.; Georgiou, A.N.; Williams, L.D.; Christaki, E.; Voskarides, K.; Lavranos, G.; Lamnisos, D.; Pouget, E.R.; et al. Drug Injection-Related Norms and High-Risk Behaviors of People Who Inject Drugs in Athens, Greece. AIDS Res. Hum. Retroviruses 2021, 37, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Paraskevis, D.; Paraschiv, S.; Sypsa, V.; Nikolopoulos, G.; Tsiara, C.; Magiorkinis, G.; Psichogiou, M.; Flampouris, A.; Mardarescu, M.; Niculescu, I.; et al. Enhanced HIV-1 surveillance using molecular epidemiology to study and monitor HIV-1 outbreaks among intravenous drug users (IDUs) in Athens and Bucharest. Infect. Genet. Evol. 2015, 35, 109–121. [Google Scholar] [CrossRef]
- Roussos, S.; Paraskevis, D.; Psichogiou, M.; Kostaki, E.G.; Flountzi, E.; Angelopoulos, T.; Chaikalis, S.; Papadopoulou, M.; Pavlopoulou, I.D.; Malliori, M. Ongoing HIV transmission following a large outbreak among people with long term injecting drug use in Athens, Greece (2014-2020). medRxiv 2021. [Google Scholar] [CrossRef]
- Lobato-Cordero, A.; Quentin, E.; Lobato-Cordero, G. Spatiotemporal Analysis of Influenza Morbidity and Its Association with Climatic and Housing Conditions in Ecuador. J. Environ. Public Health 2019, 2019, 6741202-10. [Google Scholar] [CrossRef]
- Clark, M.; Riben, P.; Nowgesic, E. The association of housing density, isolation and tuberculosis in Canadian First Nations communities. Int. J. Epidemiol. 2002, 31, 940–945. [Google Scholar] [CrossRef] [Green Version]
- Acevedo-Garcia, D. Zip code-level risk factors for tuberculosis: Neighborhood environment and residential segregation in New Jersey, 1985-1992. Am. J. Public Health 2001, 91, 734–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Tawfiq, J.A.; Memish, Z.A. Drivers of MERS-CoV transmission: What do we know? Expert Rev. Respir. Med. 2016, 10, 331–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sehgal, A.R.; Himmelstein, D.U.; Woolhandler, S. Feasibility of separate rooms for home isolation and quarantine for COVID-19 in the United States. Ann. Intern. Med. 2021, 174, 127–129. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).