
LGBTQI + Migrants: A Systematic Review and Conceptual Framework of Health, Safety and Wellbeing during Migration


Abstract
:1. Introduction
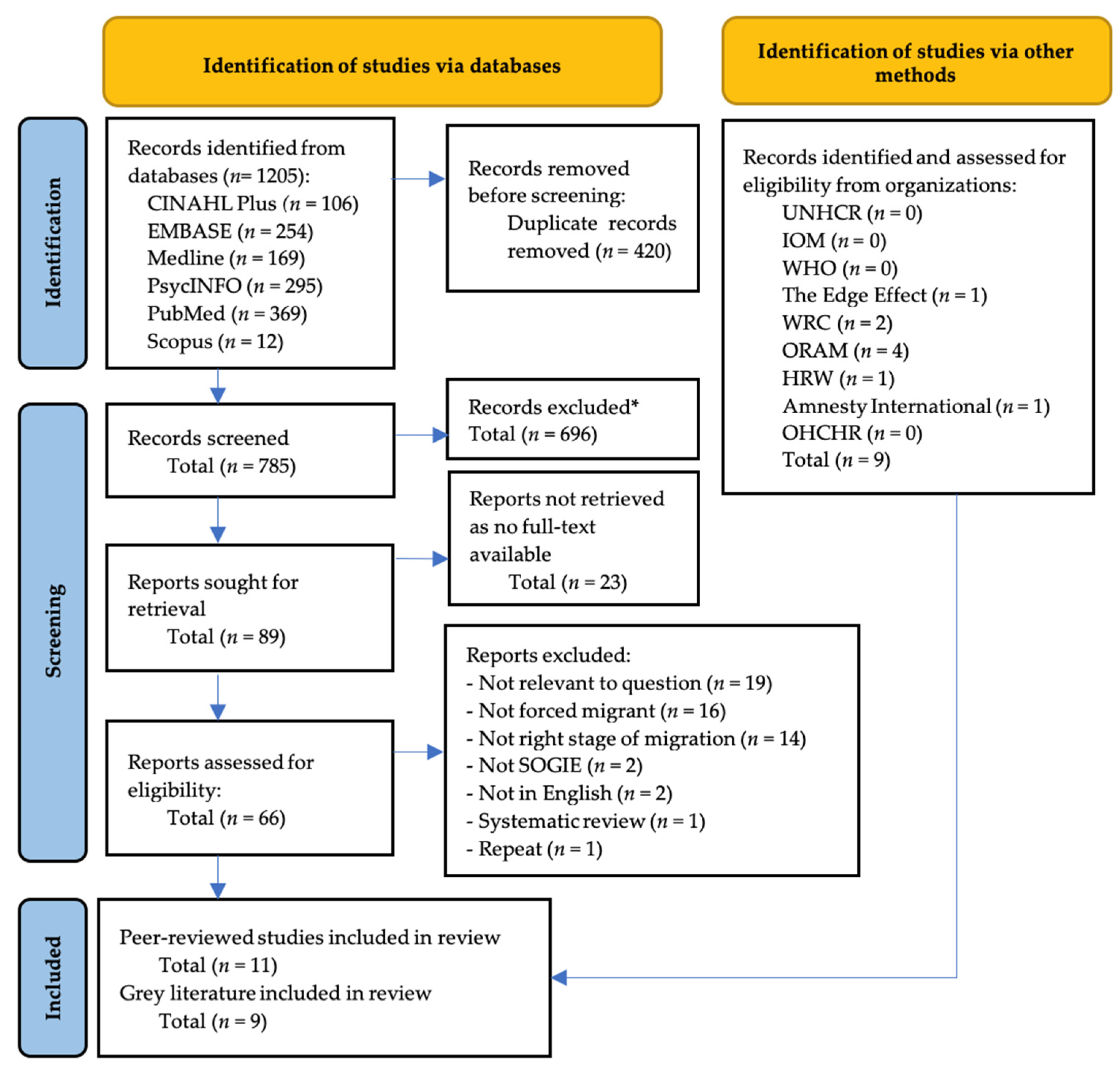
2. Materials and Methods
- Key term 1:
- MH “refugees” or MH “undocumented immigrants”or refugee* or asylum seeker* or undocumented migra* or forced migra* or irregular migra* or displace*;
- Key term 2:
- MH “sexual and gender minorities”or gender non-conform* or gender minorit* or gay or lesbian* or LGBT* or queer* or bisexual* or intersex or SOGIE* or transsex* or transgend* or trans peop* or non-binary or homosex*;
- Limit to y = “2000 − Current”.
3. Results
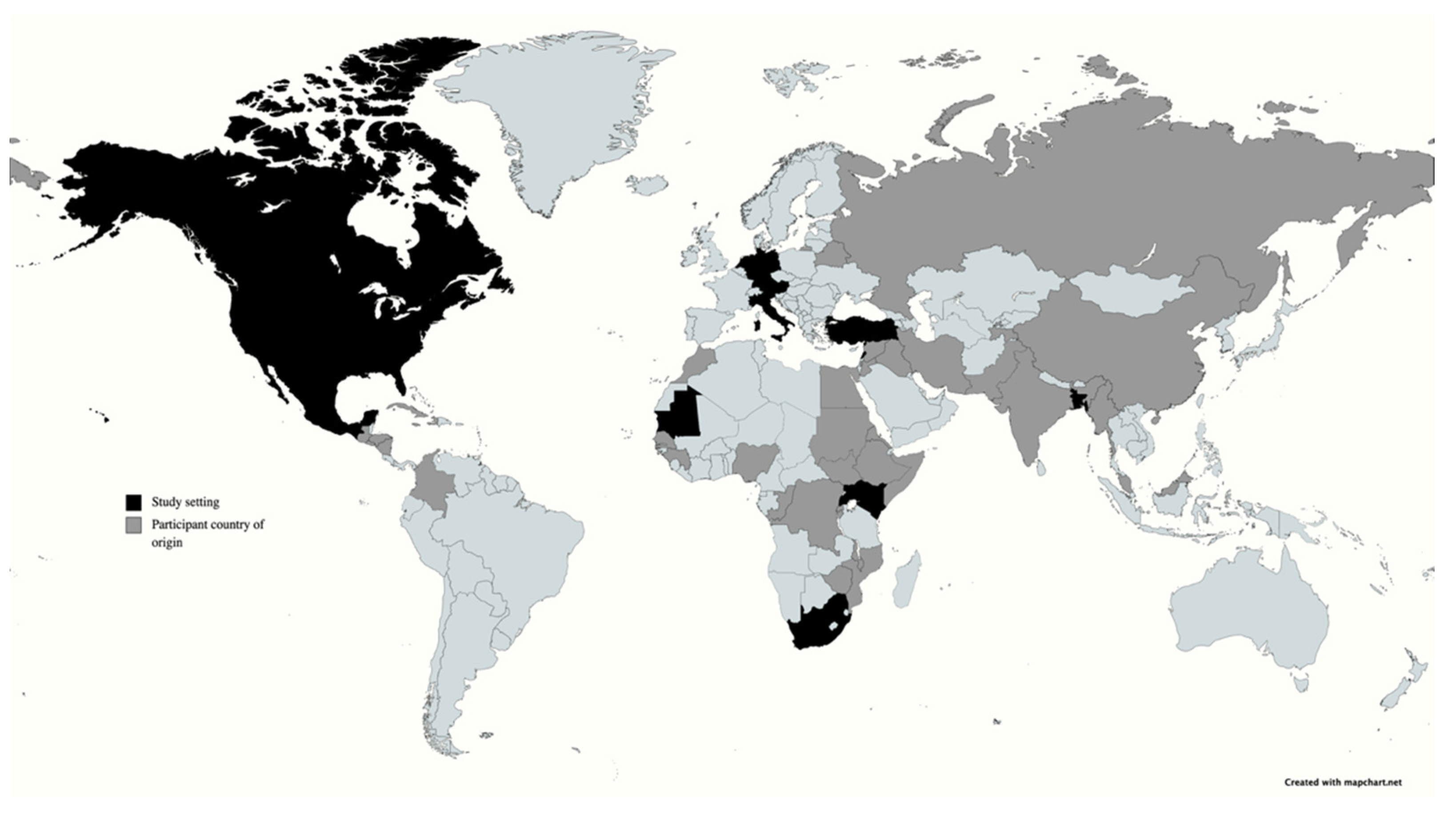
3.1. Study Characteristics
3.2. Gender Terminology
3.3. Summary of Findings
- Daily exposure to discrimination, harassment and violence;
- Coping, social support and resilience;
- Access to services;
- Mental health; and
- Physical and sexual health
3.3.1. Daily Exposure to Discrimination, Harassment and Violence
3.3.2. Coping, Social Support and Resilience
3.3.3. Access to Services
3.3.4. Mental Health
3.3.5. Physical and Sexual Health
4. Discussion
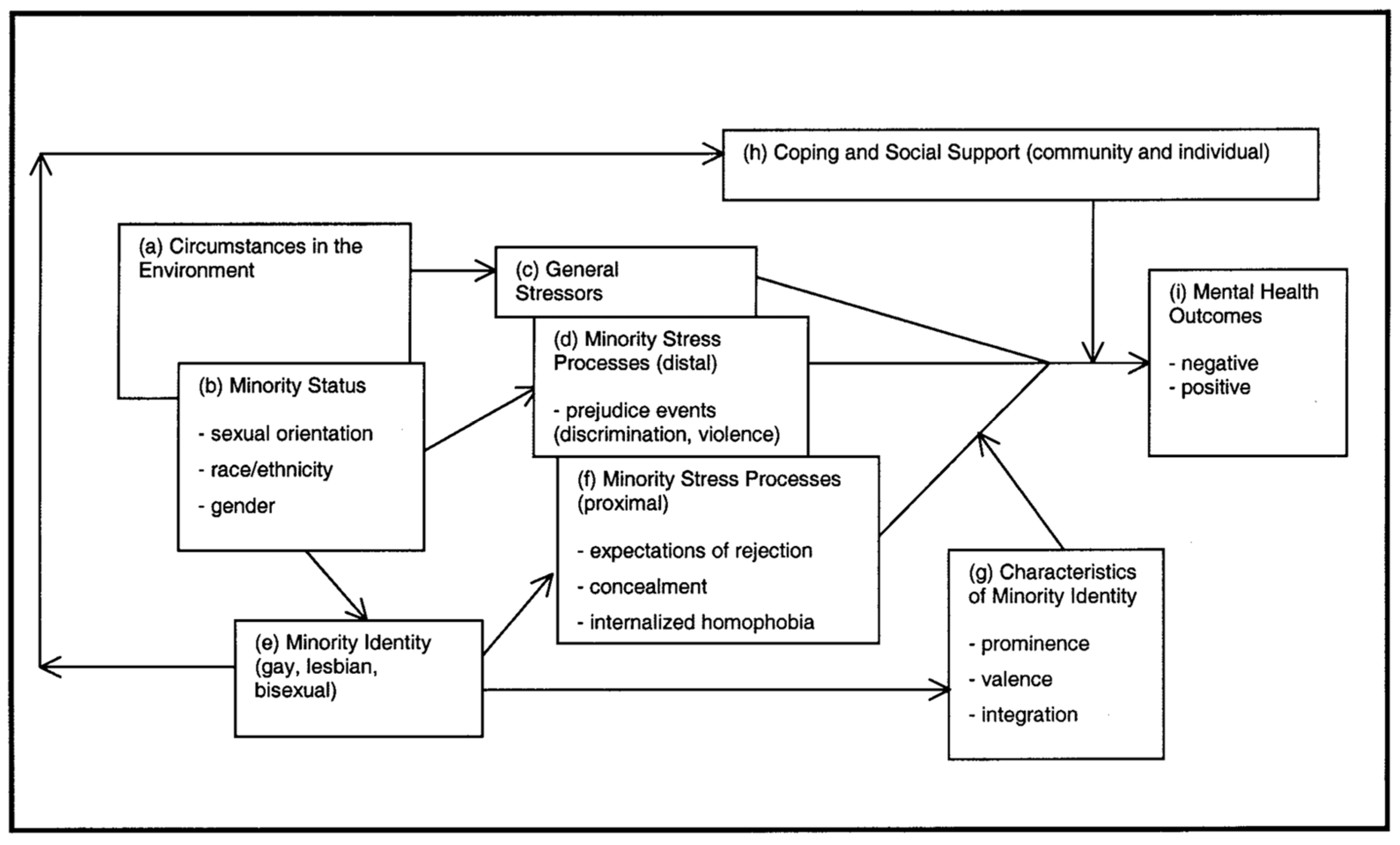
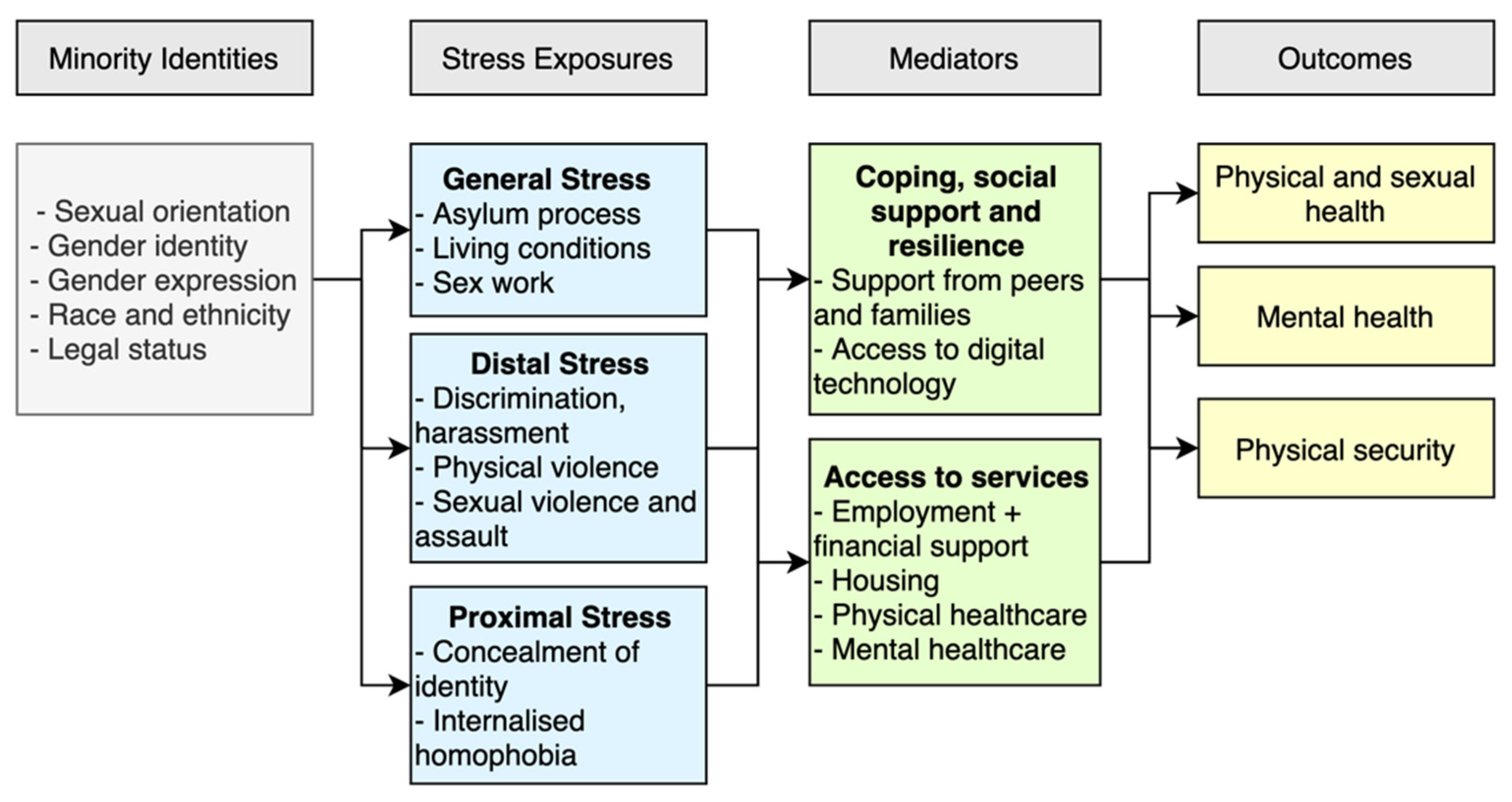
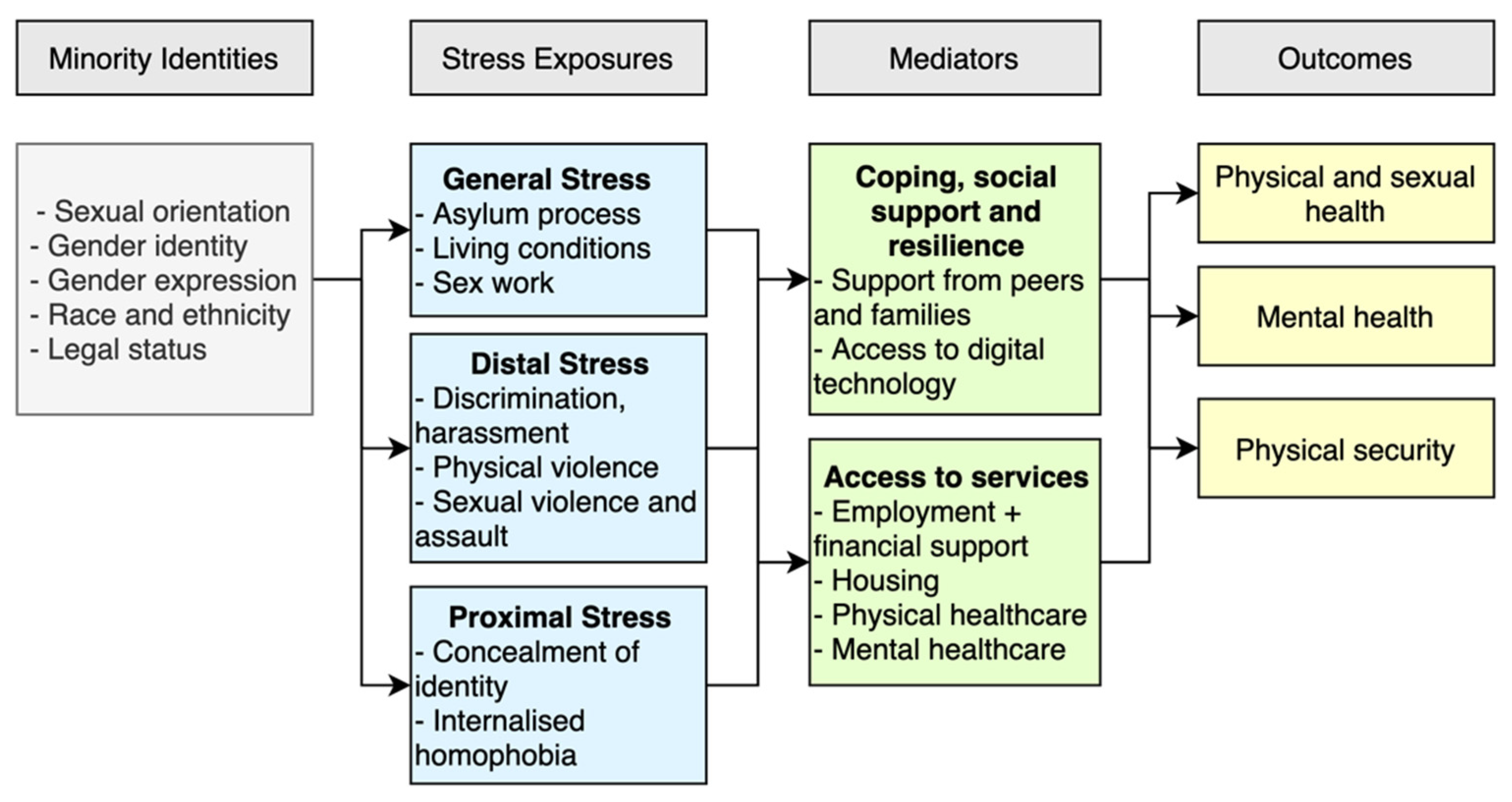
4.1. Conceptual Framework
4.1.1. Minority Identities
4.1.2. Stress Exposures
4.1.3. Mediators
4.1.4. Outcomes
4.2. Limitations
4.3. Policy, Program and Research Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNHCR. Global Trends: Forced Displacement in 2020. 2021. Available online: https://www.unhcr.org/60b638e37.pdf (accessed on 31 October 2021).
- Alessi, E.J.; Kahn, S.; Van Der Horn, R. A Qualitative Exploration of the Premigration Victimization Experiences of Sexual and Gender Minority Refugees and Asylees in the United States and Canada. J. Sex Res. 2017, 54, 936–948. [Google Scholar] [CrossRef] [PubMed]
- Piwowarczyk, L.; Fernandez, P.; Sharma, A. Seeking Asylum: Challenges Faced by the LGB Community. J. Immigr. Minor. Health 2017, 19, 723–732. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med14&NEWS=N&AN=26976005 (accessed on 31 October 2021). [CrossRef] [PubMed]
- International Lesbian Gay Bisexual Trans and Intersex Association State-Sponsored Homophobia. Global Legislation Overview Update. 2020. Available online: https://ilga.org/downloads/ILGA_World_State_Sponsored_Homophobia_report_global_legislation_overview_update_December_2020.pdf (accessed on 31 October 2021).
- Centre, R.S.; Centre, R.S. Sexual orientation and gender identity and the protection of forced migrants. Forced Migration Review 2013, 42, 1–64. Available online: http://www.refworld.org/docid/517eab7f4.html (accessed on 31 October 2021).
- United Nations Universal Declaration of Human Rights. 1948. Available online: https://www.un.org/sites/un2.un.org/files/udhr.pdf (accessed on 31 October 2021).
- UNHCR Resettlement Assessment Tool: Lesbian, Gay, Bisexual, Transgender and Intersex Refugees. 2013. Available online: https://www.unhcr.org/51de6e5f9.pdf (accessed on 31 October 2021).
- IOM World Migration Report 2020. 2020. Available online: https://www.un.org/sites/un2.un.org/files/wmr_2020.pdf (accessed on 31 October 2021).
- Correa, S.O.; Muntarbhorn, V. The Yogyakarta Principles. 2007. Available online: http://yogyakartaprinciples.org/wp-content/uploads/2016/08/principles_en.pdf (accessed on 31 October 2021).
- Grinspan, M.C.; Carpenter, M.; Ehrt, J.; Kara, S.; Narrain, A.; Patel, P.; Sidoti, C.; Tabengwa, M. The Yogyakarta Principles Plus 10. 2017. Available online: http://yogyakartaprinciples.org/wp-content/uploads/2017/11/A5_yogyakartaWEB-2.pdf (accessed on 31 October 2021).
- Kahn, S.; Alessi, E.J.; Kim, H.; Woolner, L.; Olivieri, C.J. Facilitating mental health support for LGBT forced migrants: A qualitative inquiry. J. Couns. Dev. 2018, 96, 316–326. [Google Scholar] [CrossRef]
- Kahn, S.; Alessi, E.; Woolner, L.; Kim, H.; Olivieri, C. Promoting the wellbeing of lesbian, gay, bisexual and transgender forced migrants in Canada: Providers’ perspectives. Cult. Health Sex. 2017, 19, 1165–1179. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S. Experiences of faith for gender role non-conforming Muslims in resettlement: Preliminary considerations for social work practitioners. Br. J. Soc. Work 2015, 45, 2038–2055. [Google Scholar] [CrossRef]
- Alessi, E.J.; Kahn, S.; Greenfield, B.; Woolner, L.; Manning, D.; Brett, M. A qualitative exploration of the integration experiences of lgbtq refugees who fled from the middle east, north africa, and central and south asia to austria and the netherlands. Sex. Res. Soc. Policy A J. NSRC 2018, 17, 13–26. [Google Scholar] [CrossRef]
- Alessi, E.J. Resilience in sexual and gender minority forced migrants: A qualitative exploration. Traumatology (Tallahass. Fla). 2016, 22, 203–213. [Google Scholar] [CrossRef]
- Logie, C.H.; James, L.L.; Tharao, W.; Loutfy, M.R. “We don’t exist”: A qualitative study of marginalization experienced by HIV-positive lesbian, bisexual, queer and transgender women in Toronto, Canada. J. Int. AIDS Soc. 2012, 15, 1–11. [Google Scholar] [CrossRef]
- Golembe, J.; Leyendecker, B.; Maalej, N.; Gundlach, A.; Busch, J. Experiences of minority stress and mental health burdens of newly arrived lgbtq* refugees in germany. Sex. Res. Soc. Policy A J. NSRC 2020. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=psyc17&NEWS=N&AN=2020-87750-001 (accessed on 31 October 2021).
- Paynter, E. The Liminal Lives of Europe’s Transit Migrants. Contexts 2018, 17, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Ansems De Vries, L.; Carrera, S.; Guild, E. Documenting the Migration Crisis in the Mediterranean. CEPS Pap. Lib. Secur. Eur. 2016, 1–10. Available online: www.ceps.eu (accessed on 31 October 2021).
- Duvell, F. Transit, Migration and Politics Trends and Constructions on the Fringes of Europe. 2008. Available online: http://www.compas.ox.ac.uk/2008/er-2008-transit_migration_trends_fringes_imiscoe/%0Apapers3://publication/uuid/B6031570-25A1-493F-8B9F-E4FC793F0403 (accessed on 31 October 2021).
- OHCHR The Situation of Migrants in Transit. 2015. Available online: http://www.ohchr.org/Documents/Issues/Migration/StudyMigrants/OHCHR_2016_Report-migrants-transit_EN.pdf (accessed on 31 October 2021).
- Council of Europe Parliamentary Assembly Countries of Transit: Meeting New Migration and Asylum Challenges. Available online: http://assembly.coe.int/nw/xml/XRef/Xref-XML2HTML-en.asp?fileid=22175&lang=en (accessed on 31 October 2021).
- De Massol de Rebetz, R. How useful is the concept of transit migration in an intra-Schengen mobility context? Diving into the migrant smuggling and human trafficking nexus in search for answers. Eur. J. Crim. Policy Res. 2021, 27, 41–63. [Google Scholar] [CrossRef]
- UNHCR Desperate Journeys. 2017. Available online: https://www.unhcr.org/uk/news/updates/2017/2/58b449f54/desperate-journeys-refugees-migrants-entering-crossing-europe-via-mediterranean.html (accessed on 31 October 2021).
- Campana, P. Out of Africa: The organization of migrant smuggling across the Mediterranean. Eur. J. Criminol. 2018, 15, 481–502. [Google Scholar] [CrossRef]
- IOM Missing Migrant Project. Available online: https://missingmigrants.iom.int (accessed on 31 October 2021).
- United Nations Human Rights Special Procedures; UNHCR 2021 Global Roundtable on Protection and Solutions for LGBTIQ+ People in Forced Displacement: Summary Conclusions. 2021. Available online: https://www.unhcr.org/en-us/611e48144.pdf (accessed on 31 October 2021).
- Lee, E.O.J.; Brotman, S. Identity, refugeeness, belonging: Experiences of sexual minority refugees in Canada. Can. Rev. Sociol. 2011, 48, 241–274. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med8&NEWS=N&AN=22214042 (accessed on 31 October 2021). [CrossRef]
- Bhugra, D.; Gupta, S.; Bhui, K.; Craig, T.; Dogra, N.; Ingleby, J.D.; Kirkbride, J.; Moussaoui, D.; Nazroo, J.; Qureshi, A.; et al. WPA guidance on mental health and mental health care in migrants. World Psychiatry 2011, 10, 2–10. [Google Scholar] [CrossRef]
- UNHCR Working with Bisexual, Transgender, Intersex and Queer (LGBTIQ+) Persons in Forced Displacement: Need to Know Guidance. Available online: https://www.refworld.org/cgi-bin/texis/vtx/rwmain?page=search&docid=4e6073972&skip=0&publisher=UNHCR&advsearch=y&process=y&allwords=&exactphrase=&atleastone=lgbsogi&without=&title=&monthfrom=01&yearfrom=2000&monthto=07&yearto=2021&coa=&language=EN&citati (accessed on 31 October 2021).
- Shidlo, A.; Ahola, J. Mental health challenges of LGBT forced migrants. Forced Migr. Rev. 2013, 42, 9–11. [Google Scholar]
- White, L.C.J.; Cooper, M.; Lawrence, D. Mental illness and resilience among sexual and gender minority refugees and asylum seekers. Br. J. Gen. Pract. 2019, 69, 10–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dwyer, E. The Only Way is Up: Monitoring and Encouraging Diverse SOGIESC Inclusion in the Humanitarian and DRR Sectors. 2021. Available online: https://www.edgeeffect.org/wp-content/uploads/2021/03/TheOnlyWayIsUp_Web.pdf (accessed on 31 October 2021).
- UNHCR Protecting Persons with Diverse Sexual Orientations and Gender Identities: A Global Report on UNHCR’s Efforts to Protect Lesbian, Gay, Bisexual, Transgender, and Intersex Asylum Seekers and Refugees. 2015. Available online: https://www.refworld.org/pdfid/566140454.pdf (accessed on 31 October 2021).
- Dolan, C. Addressing Sexual Violence against Men, Boys, and LGBTIQ+ Persons in Humanitarian Settings: A Field-Friendly Guidance Note by Sector. 2015. Available online: http://www.womensrefugeecommission.org/wp-content/uploads/2021/02/Addressing-Sexual-Violence-against-Men-Boys-LGBTIQ-Persons-Guidance-Note-022021-1.pdf (accessed on 31 October 2021).
- Organisation for Refuge Aslyum and Migration ORAM Toolkit. 2016. Available online: https://65cf986c-561b-404d-86c6-239bb71dad13.usrfiles.com/ugd/65cf98_05b1aee0de78423389295ae1f782a203.pdf (accessed on 31 October 2021).
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanford Law Rev. 1991, 43, 1241–1299. [Google Scholar] [CrossRef]
- McCauley, H.L.; Coulter, R.W.S.; Bogen, K.W.; Rothman, E.F. Chapter 14—Sexual Assault Risk and Prevention Among Sexual and Gender Minority Populations; Academic Press: San Diego, CA, USA, 2018; pp. 333–352. ISBN 978-0-12-805389-8. Available online: https://www.sciencedirect.com/science/article/pii/B9780128053898000141 (accessed on 31 October 2021).
- Meyer, I.H. Serving our youth 2015: The needs and experiences of lesbian, gay, bisexual, transgender, and questioning youth experiencing homelessness. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, I.; Aldridge, R.W.; Devakumar, D.; Orcutt, M.; Burns, R.; Barreto, M.L.; Dhavan, P.; Fouad, F.M.; Groce, N.; Guo, Y.; et al. The UCL–Lancet Commission on Migration and Health: The health of a world on the move. Lancet 2018, 392, 2606–2654. [Google Scholar] [CrossRef] [Green Version]
- Global Compact for Migration Global Compact for Safe, Orderly and Regular Migration. 2018. Available online: https://refugeesmigrants.un.org/sites/default/files/180713_agreed_outcome_global_compact_for_migration.pdf (accessed on 31 October 2021).
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- CASP. C.A.S.P. CASP Qualitative Checklist. CASP Online 2018, 1–6. Available online: https://casp-uk.net/%0Ahttp://www.casp-uk.net/casp-tools-checklists (accessed on 31 October 2021).
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pincock, K. UNHCR and LGBTI Refugees in Kenya: The Limits of “Protection”. Disasters 2020. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medp&NEWS=N&AN=32441384 (accessed on 31 October 2021).
- Bayramoğlu, Y.; Lünenborg, M. Queer Migration and Digital Affects: Refugees Navigating from the Middle East via Turkey to Germany. Sex. Cult. 2018, 22, 1019–1036. [Google Scholar] [CrossRef]
- Bhagat, A. Queer necropolitics of forced migration: Cyclical violence in the African context. Sexualities 2020, 23, 361–375. [Google Scholar] [CrossRef]
- Jafari, F. Silencing sexuality: LGBT refugees and the public-private divide in Iran and Turkey. Diss. Abstr. Int. Sect. A Humanit. Soc. Sci. 2014. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=psyc11&NEWS=N&AN=2014-99190-003 (accessed on 31 October 2021).
- Chynoweth, S. “More Than One Million Pains”: Sexual Violence Against Men and Boys on the Central Mediterranean Route to Italy. 2019. Available online: https://www.womensrefugeecommission.org/wp-content/uploads/2020/04/Libya-Italy-Report-03-2019.pdf (accessed on 31 October 2021).
- Chynoweth, S. “We Have a Broken Heart”: Sexual Violence against Refugees in Nairobi and Mombasa, Kenya. 2019. Available online: https://s33660.pcdn.co/wp-content/uploads/2020/04/SVMB-Kenya-Report-10-2019-FINAL.pdf (accessed on 31 October 2021).
- Gottlieb, N.; Puschmann, C.; Stenzinger, F.; Koelber, J.; Rasch, L.; Koppelow, M.; Al Munjid, R. Health and Healthcare Utilization among Asylum-Seekers from Berlin’s LGBTIQ Shelter: Preliminary Results of a Survey. Int. J. Environ. Res. Public Health 2020, 17, 4514. [Google Scholar] [CrossRef]
- Organization for Refugee Asylum & Migration, Refugee Law Project. Blind alleys PART II Country Findings: Uganda. 2013. Available online: https://www.refworld.org/pdfid/524d45e84.pdf (accessed on 31 October 2021).
- Alessi, E.J.; Kahn, S.; Woolner, L.; Van Der Horn, R. Traumatic Stress Among Sexual and Gender Minority Refugees From the Middle East, North Africa, and Asia Who Fled to the European Union. J. Trauma. Stress 2018, 31, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Broqua, C.; Laborde-Balen, G.; Menetrier, A.; Bangoura, D. Queer necropolitics of asylum: Senegalese refugees facing HIV in Mauritania. Glob. Public Health 2021, 16, 746–762. [Google Scholar] [CrossRef]
- Clark, K.; Pachankis, J.; Khoshnood, K.; Heimer, R.; Branstrom, R.; Seal, D.; Khoury, D.; Fouad, F.M.; Barbour, R. Stigma, displacement stressors and psychiatric morbidity among displaced Syrian men who have sex with men (MSM) and transgender women: A cross-sectional study in Lebanon. BMJ Open 2021, 11, e046996. [Google Scholar] [CrossRef]
- Fox, S.D.; Griffin, R.H.; Pachankis, J.E. Minority stress, social integration, and the mental health needs of LGBTQ asylum seekers in North America. Soc. Sci. Med. 2020, 246, 112727. [Google Scholar] [CrossRef]
- Tohme, J.; Egan, J.E.; Friedman, M.R.; Stall, R. Psycho-social Correlates of Condom Use and HIV Testing among MSM Refugees in Beirut, Lebanon. AIDS Behav. 2016, 20 (Suppl. 3), 417–425. [Google Scholar] [CrossRef]
- Amnesty International No Safe Place: Salvadorans, Guatemalans and Hondurans Seeking Asylum in Mexico Based on the Sexual Orientation and/or Gender Identity. 2017. Available online: https://www.amnesty.org/en/documents/amr01/7258/2017/en/ (accessed on 31 October 2021).
- Ghoshal, N. “Every Day I Live in Fear” Violence and Discrimination Against LGBT People in El Salvador, Guatemala, and Honduras, and Obstacles to Asylum in the United States. 2020. Available online: https://www.hrw.org/sites/default/files/media_2020/10/centralamerica_lgbt1020_web_0.pdf (accessed on 31 October 2021).
- Organization for Refuge Asylum & Migration Blind Alleys PART II Country Findings: Mexico. 2013. Available online: https://amrefugeeco-my.sharepoint.com/personal/bellas_oramrefugee_org/_layouts/15/onedrive.aspx?id=%2Fpersonal%2Fbellas_oramrefugee_org%2FDocuments%2FContentforWebsite%2FContentforWebsite%2FResources%2FORAM_BA_MexicoENG_HR.pdf&parent=%2Fpersonal%2Fbel (accessed on 31 October 2021).
- Organization for Refuge Asylum & Migration Blind Alleys PART II Country Findings: South Africa. 2013. Available online: https://amrefugeeco-my.sharepoint.com/personal/bellas_oramrefugee_org/_layouts/15/onedrive.aspx?id=%2Fpersonal%2Fbellas_oramrefugee_org%2FDocuments%2FContentforWebsite%2FContentforWebsite%2FResources%2F20130226-oram_ba_southafrica.pdf&parent=%2Fperson (accessed on 31 October 2021).
- Helsinki Citizens’ Assembly—Turkey Refugee Advocacy and Support Program; Organization for Refuge Asylum & Migration Unsafe Haven: The Security Challenges Facing Lesbian, Gay, Bisexual and Transgender Asylum Seekers and Refugees in Turkey. 2011, pp. 1–35. Available online: http://www.oraminternational.org/images/stories/PDFs/oram-unsafe-haven-2011.pdf (accessed on 31 October 2021).
- Morrissey, J. Environmental Change and Forced Migration: A State of the Art Review. Refug. Stud. Cent. 2009, 1–49. Available online: https://anyl4psd.org/wp-content/uploads/2019/01/dp-environmental-change-forced-migration-2009-1.pdf (accessed on 31 October 2021).
- Castles, S. Global perspectives on forced migration. Migr. Citizsh. Identity Sel. Essays 2017, 15, 269–290. [Google Scholar]
- United Nations High Commission for Refugees. UNHCR Trends at a Glance: Global Trends Forced Displacement in 2019. Unhcr 2020, 1–84. Available online: https://www.unhcr.org/5ee200e37.pdf (accessed on 31 October 2021).
- UNHCR Guidelines on Internation Protection No. 9. Claims to Refugee Status Based on Sexual Orientation and/or Gender Identity within the Context of Article 1A(2) of the 1951 Convention and/or its 1967 Protocol Relating to the Status of Refugees. 2012. Available online: https://www.unhcr.org/509136ca9.html (accessed on 31 October 2021).
- University of Oxford. Refugee Studies Centre Sexual orientation and gender identity and the protection of forced migrants. Forced Migr. Rev. 2013. Available online: https://www.fmreview.org/sites/fmr/files/FMRdownloads/en/fmr42full.pdf (accessed on 31 October 2021).
- Jakobsen, M.; Meyer Demott, M.A.; Wentzel-Larsen, T.; Heir, T. The impact of the asylum process on mental health: A longitudinal study of unaccompanied refugee minors in Norway. BMJ Open 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Werthern, M.; Robjant, K.; Chui, Z.; Schon, R.; Ottisova, L.; Mason, C.; Katona, C. The impact of immigration detention on mental health: A systematic review. BMC Psychiatry 2018, 18, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keygnaert, I.; Vettenburg, N.; Temmerman, M. Hidden violence is silent rape: Sexual and gender-based violence in refugees, asylum seekers and undocumented migrants in Belgium and the Netherlands. Cult. Health Sex. 2012, 14, 505–520. [Google Scholar] [CrossRef]
- Arsenijević, J.; Schillberg, E.; Ponthieu, A.; Malvisi, L.; Ahmed, W.A.E.; Argenziano, S.; Zamatto, F.; Burroughs, S.; Severy, N.; Hebting, C.; et al. A crisis of protection and safe passage: Violence experienced by migrants/refugees travelling along the Western Balkan corridor to Northern Europe. Confl. Health 2017, 11, 1–9. [Google Scholar] [CrossRef]
- Infante, C.; Idrovo, A.J.; Sánchez-Domínguez, M.S.; Vinhas, S.; González-Vázquez, T. Violence Committed Against Migrants in Transit: Experiences on the Northern Mexican Border. J. Immigr. Minor. Health 2012, 14, 449–459. [Google Scholar] [CrossRef]
- Cuneo, C.N.; Huselton, K.E.; Praschan, N.C.; Saadi, A.; Gartland, M.G. What Counts As “Safe?” Exposure To Trauma And Violence Among Asylum Seekers From The Northern Triangle. Health Aff. 2021, 40, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- ORAM. Country of Origin Report: Sexual and Gender Minorities Uganda. 2014. Available online: https://65cf986c-561b-404d-86c6-239bb71dad13.usrfiles.com/ugd/65cf98_e8e4601b836c4f8783b95ee3e67ecce0.pdf (accessed on 31 October 2021).
- Hall, W.J. Psychosocial Risk and Protective Factors for Depression among Lesbian, Gay, Bisexual, and Queer Youth: A Systematic Review. J. Homosex. 2018, 65, 263–316. [Google Scholar] [CrossRef]
- Rood, B.A.; Maroney, M.R.; Puckett, J.A.; Berman, A.K.; Reisner, S.L.; Pantalone, D.W. Identity concealment in transgender adults: A qualitative assessment of minority stress and gender affirmation. Am. J. Orthopsychiatry 2017, 87, 704–713. [Google Scholar] [CrossRef]
- Babatunde-Sowole, O.; Power, T.; Jackson, D.; Davidson, P.M.; DiGiacomo, M. Resilience of African migrants: An integrative review. Health Care Women Int. 2016, 37, 946–963. [Google Scholar] [CrossRef] [PubMed]
- OutRight Action International Activism and Resilence: LGBTQ Progress in the MIddle East and North Africa. 2018. Available online: https://outrightinternational.org/sites/default/files/MENAReport2018_100918_FINAL.pdf (accessed on 31 October 2021).
- Logie, C.H.; Lacombe-Duncan, A.; Lee-Foon, N.; Ryan, S.; Ramsay, H. “It’s for us -newcomers, LGBTQ persons, and HIV-positive persons. You feel free to be”: A qualitative study exploring social support group participation among African and Caribbean lesbian, gay, bisexual and transgender newcomers and refugees in Toronto. BMC Int. Health Hum. Rights 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, T.K.; Fantz, C.R. Barriers to quality health care for the transgender population. Clin. Biochem. 2014, 47, 983–987. [Google Scholar] [CrossRef]
- Baker, K.E.; Wilson, L.M.; Sharma, R.; Dukhanin, V.; McArthur, K.; Robinson, K.A. Hormone Therapy, Mental Health, and Quality of Life among Transgender People: A Systematic Review. J. Endocr. Soc. 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, B.A.; Peitzmeier, S.M.; Restar, A.; Adamson, T.; Howell, S.; Baral, S.; Beckham, S.W. Gender-affirming care, mental health, and economic stability in the time of COVID-19: A multi-national, cross-sectional study of transgender and nonbinary people. PLoS ONE 2021, 16, e0254215. [Google Scholar] [CrossRef] [PubMed]
- DasGupta, D. The Politics of Transgender Asylum and Detention. Hum. Geogr. 2019, 12, 1–16. [Google Scholar] [CrossRef]
- Tabak, S.; Levitan, R. LGBTI migrants in immigration detention. Forced Migr. Rev. 2013, 1, 47–49. [Google Scholar]
- Husakouskaya, N. Becoming a transgender/intersex internal migrant in Urban Gauteng: Challenges and Experiences of Transition while Seeking Access to Medical Services. Forsch—Stud. Online-J. Univ. Oldenbg. 2016, 1, 61–65. [Google Scholar]
- King, M.; Semlyen, J.; Tai, S.S.; Killaspy, H.; Osborn, D.; Popelyuk, D.; Nazareth, I. A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry 2008, 8, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, L.E.; Salway, T.; Tarasoff, L.A.; MacKay, J.M.; Hawkins, B.W.; Fehr, C.P. Prevalence of Depression and Anxiety Among Bisexual People Compared to Gay, Lesbian, and Heterosexual Individuals:A Systematic Review and Meta-Analysis. J. Sex Res. 2018, 55, 435–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz, R.M.; Ayala, G.; Bein, E.; Henne, J.; Marin, B.V. The impact of homophobia, poverty, and racism on the mental health of gay and bisexual Latino men: Findings from 3 US cities. Am. J. Public Health 2001, 91, 927–932. [Google Scholar] [PubMed] [Green Version]
- Suhaiban, H.A.; Grasser, L.R.; Javanbakht, A. Mental health of refugees and torture survivors: A critical review of prevalence, predictors, and integrated care. Int. J. Environ. Res. Public Health 2019, 16, 2309. [Google Scholar] [CrossRef] [Green Version]
- Logie, C.H.; Wang, Y.; Lacombe-Duncan, A.; Jones, N.; Ahmed, U.; Levermore, K.; Neil, A.; Ellis, T.; Bryan, N.; Marshall, A.; et al. Factors associated with sex work involvement among transgender women in Jamaica: A cross-sectional study: A. J. Int. AIDS Soc. 2017, 20, 21422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, M.; Chersich, M.; Temmerman, M.; Luchters, S. Characteristics, sexual behaviour and risk factors of female, male and transgender sex workers in South Africa. S. Afr. Med. J. 2013, 103, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baral, S.D.; Poteat, T.; Strömdahl, S.; Wirtz, A.L.; Guadamuz, T.E.; Beyrer, C. Worldwide burden of HIV in transgender women: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 214–222. [Google Scholar] [CrossRef]
- Logie, C.H.; Okumu, M.; Mwima, S.; Hakiza, R.; Abela, H.; Kyambadde, P. Gender, transactional sex, and HIV prevention cascade engagement among urban refugee and displaced adolescents and youth in Kampala, Uganda. AIDS Care-Psychol. Socio-Med. Asp. AIDS/HIV 2021, 33, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Spini, L. Ethics-based global health research for all, including women, children, indigenous people, LGBTQI, people with disabilities, refugees and other relevant stakeholders, especially in least developing countries and small island developing states in the Globa. Soc. Sci. Med. 2018, 214, 167–170. [Google Scholar] [CrossRef] [PubMed]
- The National Academies of Sciences Engineering Medicine Measuring Sex, Gender Identity, and Sexual Orientation for the National Institutes of Health. Available online: https://www.nationalacademies.org/our-work/measuring-sex-gender-identity-and-sexual-orientation-for-the-national-institutes-of-health#sectionContact (accessed on 31 October 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Included | Excluded | |
|---|---|---|
| Sample | People of all ages identifying as: (i) diverse SOGIE and (ii) refugees, asylum seekers, or forced irregular migrants Published after 1 January 2000 English language | Voluntary migrants Those with a traditional normative binary SOGIE Published prior to 1 January 2000 Non-English |
| Phenomenon of interest | Specific experiences during the migration journey that are related to SOGIE | Only pre-migration experiences |
| Design | Any study design that includes empirical evidence and not in exclusion list | Systematic reviews, reports, briefings, legal cases, commentaries, no empirical evidence |
| Evaluation | Mental and physical health during transit and immediately after arrival Services available and barriers to access | Integration experiences only |
| Research type | Peer-reviewed literature Grey literature Full text available | Full text not available |
| Author, Year | Objective | Setting | Study Design, Methods, Sampling | Study Population | Quality Appraisal Score |
|---|---|---|---|---|---|
| Alessi et al. 2018 [55] | To investigate how stress shapes migration experiences of LGBTQ refugees | Austria, Netherlands | Mixed methods: Cross-sectional survey, and qualitative interviews. Purposive sampling. | 38 LGBTQ adults in Europe from MENA 1 + Asia. Asylum seekers: accepted, pending or rejected | 100% CASP 80% AXIS High |
| Bayramoglu et al., 2018 [48] | To shed light on interaction of forced migration, sexuality, and media. | Germany | Qualitative ethnography, interviews and observation. Snowball sampling | 10 adults: Syrian + Egyptian. Queer as defined by author. Refugees. | 50% Medium |
| Bhagat et al., 2020 [49] | Explore queer forced displacement and how they survive and navigate spaces in Cape Town | South Africa | Qualitative interviews. Sampling unknown. | 6 adults: Kenya, Zimbabwe, and DRC 2. Queer as defined by author. Refugees and asylum seekers | 40% Medium |
| Broqua et al., 2021 [56] | To report on health and living conditions for Senegalese gay men in Mauritania applying for resettlement | Mauritania | Qualitative interviews. Snowball sampling | 10 Senegalese men self-identified as gay. Refugees, asylum seekers, or rejected asylum seekers | 30% Low |
| Clark et al., 2021 [57] | To assess and compare prevalence of psychiatric disorders among Lebanese and Syrian MSM and transgender women | Lebanon | Cross-sectional quantitative survey. Respondent driven, snowball sampling | 488 MSM and transgender women: 230 displaced Syrians and 258 Lebanese. Forcibly displaced due to war or identity | 65% Medium |
| Fox et al., 2020 [58] | To investigate how mental distress, social isolation, identity disclosure, and asylum procedures are interlinked for LGBTQ asylum seekers | US and Canada | Cross-sectional, quantitative online survey. Purposive sampling | 308 Adults. LGBTQ refugees and asylum seekers | 70% High |
| Golembe et al., 2020 [17] | To investigate how LGBTQ* refugees experience minority stress after migrating, including distal and proximal stress, and mental health | Germany | Qualitative FGDs 3, interviews, + demographic questionnaire. Convenience sampling | 26 adults from MENA, Middle East, Asia. Self-identified as LGBTQ*. Refugees, attempted or rejected asylum seekers | 100% High |
| Gottlieb et al., 2020 [53] | To provide insights into health and utilisation of services through comparison of LGBTIQ vs. non-LGBTIQ asylum seekers | Germany | Cross-sectional quantitative survey. Mix of non-random and weighted random sampling | 32 responses from refugees and asylum seekers in LGBTIQ shelter. | 85% High |
| Jafari F, 2014 [50] | To explore the impacts of race and sexual orientation on Iranian queer migrants | Turkey | Ethnographic+ qualitative interviews + participant observationUnknown sampling | 19 adult queer Iranian men. Asylum seekers or refugees | 30% Low |
| Pincock, 2020 [47] | To explore protection issues in communities among refugees in urban, camp, and settlement contexts in East Africa. | Kenya | Ethnographic + qualitative participant observation + interviews.Snowball sampling | LGBTI refugees. No sample size given | 40% Medium |
| Tohme et al., 2016 [59] | To determine prevalence of HIV and psychosocial correlates among Iraqi, Syrian, and Palestinian MSM refugees in Lebanon | Lebanon | Quantitative cross-sectional surveys Long chain peer referral method sampling | 150 adult refugees. Gay, bisexual, MSM | 70% High |
| Amnesty International, 2017 [60] | To document the path of flight from Honduras, Salvador and Guatemala to Mexico and the US | Mexico | Qualitative interviews. Sampling unknown | 20 refugees and asylum seekers identifying as gay men or trans women | 40% Medium |
| Chynoweth S, Women’s Refugee Commission, 2019 [51] | To examine sexual violence experiences by refugee men and boys traveling the central Mediterranean migration route | Italy | Qualitative. Key informant interviews + FGDs. Purposive sampling | 15 refugees and migrants with diverse SOGIESC 4. | 90% High |
| Chynoweth S, Women’s Refugee Commission, 2019 [52] | To examine sexual violence experienced by refugees with diverse SOGIESC and trans women in Kenya | Kenya | Qualitative interviews + FGDs. Purposive sampling. | 4 FGDs with refugees from the DRC, Somalia, and South Sudan with diverse SOGIESC | 90% High |
| Dwyer E, The Edge Effect, 2021 [33] | Reports on violence and exclusion experienced by people with diverse SOGIESC in humanitarian settings | Bangladesh | Qualitative, interviews Sampling unknown | 35 respondent: refugees with diverse SOGIESC | 60% Medium |
| Ghosal N, Human Rights Watch, 2020 [61] | To document violence and discrimination against LGBT asylum seekers in the US and Central America | El Salvador, Guatemala, Honduras, Mexico and US | Qualitative interviews Sampling unknown | 20 LGBT asylum seekers and refugees | 60% Medium |
| ORAM, 2013 [62] | To explore protection issues amongst SGN 5 refugees in Mexico | Mexico | Qualitative, Interviews. Likely purposive sampling. | 14 SGN refugees and asylum seekers | 60% Medium |
| ORAM, 2013 [63] | To identify protection issues for LGBTI asylum seekers and refugees in South Africa | Cape Town | Qualitative, interviews Purposive sampling | 14 SGN refugees and asylum seekers from Africa + Asia | 60% Medium |
| ORAM, 2011 [64] | To document protection gaps facing LGBT refugees in Turkey | Turkey | Qualitative, interviews Purposive sampling | 62 LGBT asylum seekers and refugees | 60% Medium |
| ORAM, Refugee Law Project, 2013 [54] | To explore protection issues for SGN refugees in Uganda | Uganda | Qualitative, interviews Purposive sampling | 25 SGN refugees from Africa | 80% High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yarwood, V.; Checchi, F.; Lau, K.; Zimmerman, C. LGBTQI + Migrants: A Systematic Review and Conceptual Framework of Health, Safety and Wellbeing during Migration. Int. J. Environ. Res. Public Health 2022, 19, 869. https://doi.org/10.3390/ijerph19020869
Yarwood V, Checchi F, Lau K, Zimmerman C. LGBTQI + Migrants: A Systematic Review and Conceptual Framework of Health, Safety and Wellbeing during Migration. International Journal of Environmental Research and Public Health. 2022; 19(2):869. https://doi.org/10.3390/ijerph19020869
Chicago/Turabian StyleYarwood, Vanessa, Francesco Checchi, Karen Lau, and Cathy Zimmerman. 2022. "LGBTQI + Migrants: A Systematic Review and Conceptual Framework of Health, Safety and Wellbeing during Migration" International Journal of Environmental Research and Public Health 19, no. 2: 869. https://doi.org/10.3390/ijerph19020869
APA StyleYarwood, V., Checchi, F., Lau, K., & Zimmerman, C. (2022). LGBTQI + Migrants: A Systematic Review and Conceptual Framework of Health, Safety and Wellbeing during Migration. International Journal of Environmental Research and Public Health, 19(2), 869. https://doi.org/10.3390/ijerph19020869