
A Multinational Longitudinal Study Incorporating Intensive Methods to Examine Caregiver Experiences in the Context of Chronic Health Conditions: Protocol of the ENTWINE-iCohort

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Primary Objective
1.2. Secondary Objectives
2. Materials and Methods
- (i)
- longitudinal data collection (Baseline + 6 months follow-up) using an electronic survey tool with measures and items addressing the project objectives, with a sample of informal caregivers;
- (ii)
- longitudinal data collection (Baseline + 6 months) using an electronic survey tool containing a subset of measures and items addressing the project objectives, with a sample of care recipients;
- (iii)
- a weekly assessment component to examine change over time using a subset of measures employed with caregivers and care recipients.
3. Recruitment Methods
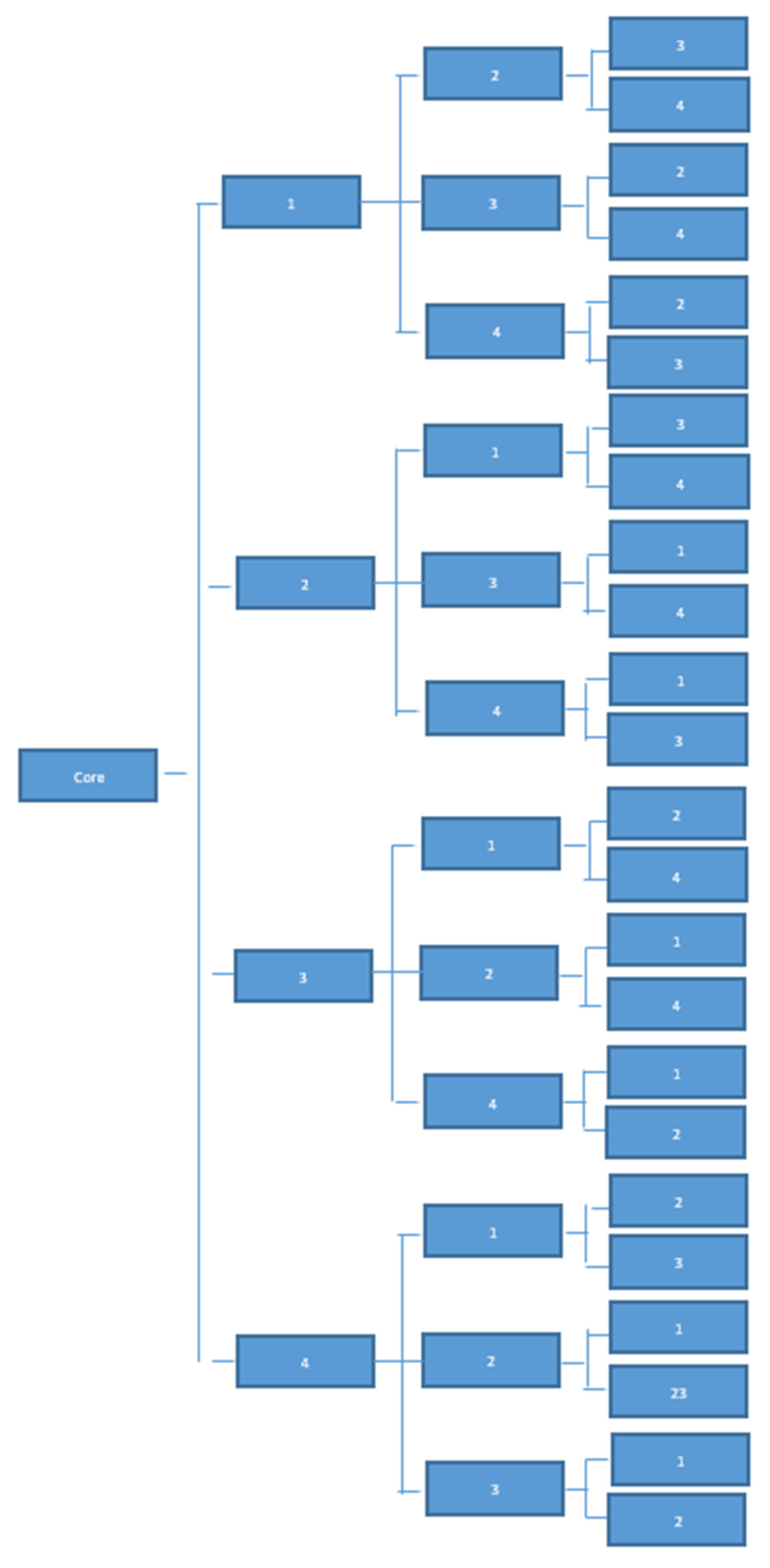
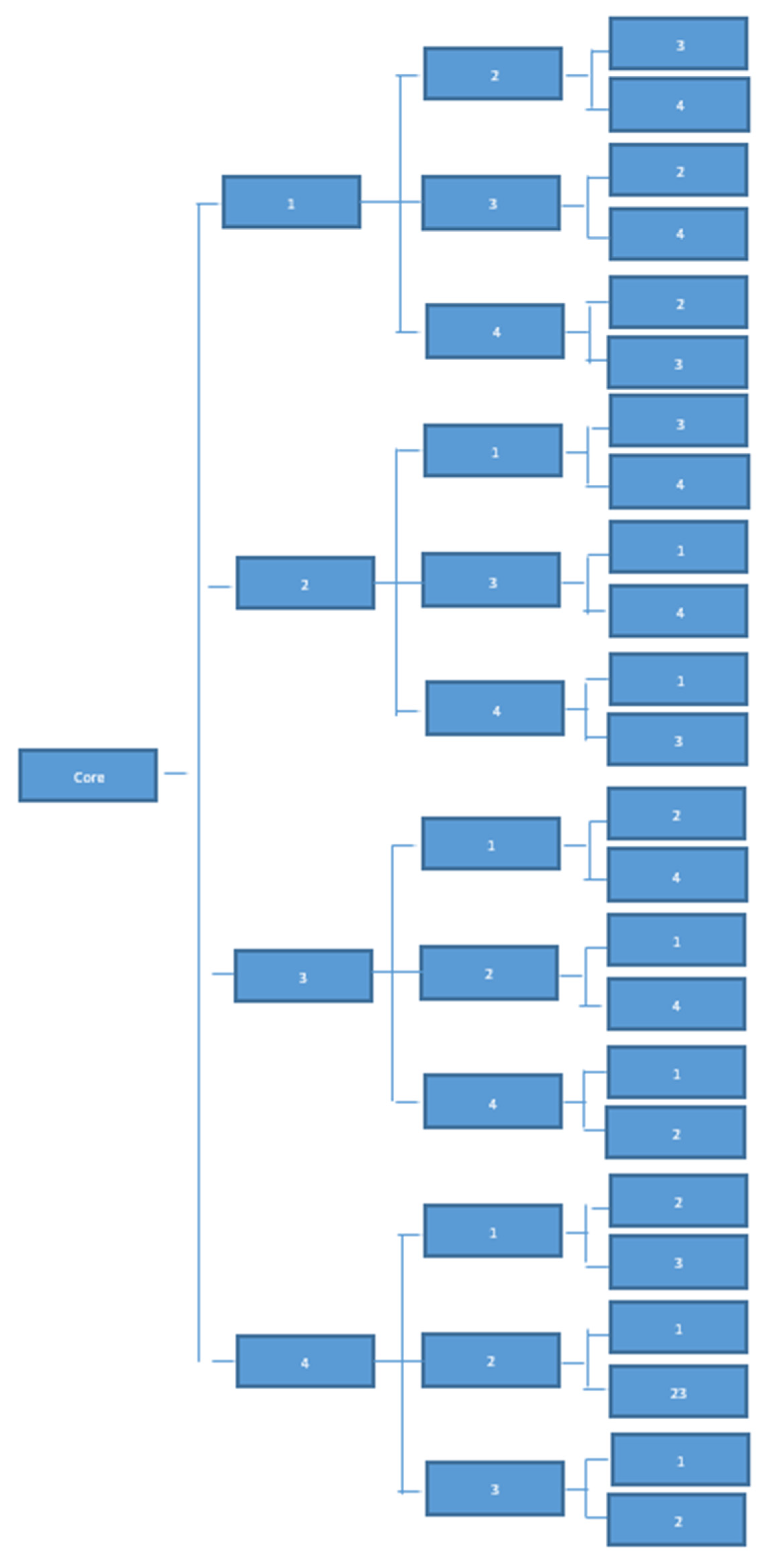
4. Questionnaire Randomisation
5. Sample Size Calculation
6. Measures
7. Analysis Plan
7.1. Modules 1-2-3 Plan Analyses
7.2. Module 4 Plan Analysis
8. Weekly Assessment Component
9. Dissemination
- Ireland 14/08/2020–31/05/2021
- UK 14/08/2020–31/05/2021
- Poland 14/08/2020–31/05/2021
- Italy 25/08/2020–31/05/2021
- Netherlands 16/10/2020–31/05/2021
- Sweden 23/10/2020–31/05/2021
- Greece 31/10/2020–31/05/2021
- Israel 16/02/2021–31/08/2021
- Germany 17/02/2021–31/08/2021
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Health Foundation. Health and Social Care Funding Explained; The Health Foundation: London, UK, 2017. [Google Scholar]
- Arcà, E.; Principe, F.; Van Doorslaer, E. Death by austerity? The impact of cost containment on avoidable mortality in Italy. Health Econ. 2020, 29, 1500–1516. [Google Scholar] [PubMed]
- Carers UK. State of Caring. A Snapshot of Unpaid Care in the UK; Carers UK: London, UK, 2019. [Google Scholar]
- Tur-Sinai, A.; Teti, A.; Rommel, A.; Hlebec, V.; Lamura, G. How many older informal caregivers are there in Europe? Comparison of estimates of their prevalence from three european surveys. Int. J. Environ. Res. Public Health 2020, 17, 9531. [Google Scholar]
- Rodrigues, R.; Huber, M.; Lamura, G. Facts and Figures on Healthy Ageing and Long-Term Care; Citeseer: Vienna, Austria, 2012. [Google Scholar]
- Ortiz-Ospina, E.; Tzvetkova, S.; Roser, M. Women’s Employment. Available online: https://ourworldindata.org/female-labor-supply (accessed on 15 October 2021).
- Greenwood, N.; Smith, R. Motivations for being informal carers of people living with dementia: A systematic review of qualitative literature. BMC Geriatr. 2019, 19, 1–18. [Google Scholar] [CrossRef]
- Morrison, V.; Williams, K. Gaining Longitudinal Accounts of Carers’ Experiences Using IPA and Photograph Elicitation. Front. Psychol. 2020, 11, 2429. [Google Scholar]
- Zarzycki, M.; Morrison, V. Getting back or giving back: Understanding caregiver motivations and willingness to provide informal care. Health Psychol. Behav. Med. 2021, 9, 636–661. [Google Scholar] [PubMed]
- Berg, C.A.; Upchurch, R. A developmental-contextual model of couples coping with chronic illness across the adult life span. Psychol. Bull. 2007, 133, 920. [Google Scholar]
- Dagan, M.; Sanderman, R.; Schokker, M.C.; Wiggers, T.; Baas, P.C.; Van Haastert, M.; Hagedoorn, M. Spousal support and changes in distress over time in couples coping with cancer: The role of personal control. J. Fam. Psychol. 2011, 25, 310. [Google Scholar]
- Falconier, M.K.; Kuhn, R. Dyadic coping in couples: A conceptual integration and a review of the empirical literature. Front. Psychol. 2019, 10, 571. [Google Scholar] [PubMed] [Green Version]
- Hagedoorn, M.; Puterman, E.; Sanderman, R.; Wiggers, T.; Baas, P.C.; van Haastert, M.; DeLongis, A. Is self-disclosure in couples coping with cancer associated with improvement in depressive symptoms? Health Psychol. 2011, 30, 753. [Google Scholar]
- Vilchinsky, N.; Dekel, R.; Revenson, T.A.; Liberman, G.; Mosseri, M. Caregivers’ burden and depressive symptoms: The moderational role of attachment orientations. Health Psychol. 2015, 34, 262. [Google Scholar]
- Parveen, S.; Morrison, V.; Robinson, C.A. Ethnic variations in the caregiver role: A qualitative study. J. Health Psychol. 2011, 16, 862–872. [Google Scholar] [CrossRef]
- Zarzycki, M.; Morrison, V.; Bei, E.; Seddon, D. Cultural and societal motivations for being informal caregivers: A qualitative systematic review and meta-synthesis. Health Psychol. Rev. 2021, in press. [Google Scholar]
- Casanova, G.; Di Rosa, M.; Fisher, O.; Lamura, G. Between migrant care work and new occupational welfare tools: Changing home care arrangements in Italy. Int. J. Environ. Res. Public Health 2020, 17, 5511. [Google Scholar]
- Baldassar, L.; Baldock, C.V.; Wilding, R. Families Caring across Borders: Migration, Ageing and Transnational Caregiving; Springer: Berlin/Heidelberg, Germany, 2006; ISBN 0230626262. [Google Scholar]
- Bei, E.; Zarzycki, M.; Morrison, V.; Vilchinsky, N. Motivations and willingness to provide care from a geographical distance, and the impact of distance care on caregivers’ mental and physical health: A mixed-method systematic review protocol. BMJ Open 2021, 11, 1–7. [Google Scholar] [CrossRef]
- Bei, E.; Rotem-Mindali, O.; Vilchinsky, N. Providing Care from Afar: A Growing Yet Understudied Phenomenon in the Caregiving Field. Front. Psychol. 2020, 11, 10–12. [Google Scholar] [CrossRef]
- Douglas, S.L.; Mazanec, P.; Lipson, A.; Leuchtag, M. Distance caregiving a family member with cancer: A review of the literature on distance caregiving and recommendations for future research. World J. Clin. Oncol. 2016, 7, 214. [Google Scholar]
- Li, M.; Mao, W.; Chi, I.; Lou, V.W.Q. Geographical proximity and depressive symptoms among adult child caregivers: Social support as a moderator. Aging Ment. Health 2019, 23, 205–213. [Google Scholar]
- Krol, M.; Papenburg, J.; van Exel, J. Does including informal care in economic evaluations matter? A systematic review of inclusion and impact of informal care in cost-effectiveness studies. Pharmacoeconomics 2015, 33, 123–135. [Google Scholar]
- Anderson, A. Europe’s care regimes and the role of migrant care workers within them. J. Popul. Ageing 2012, 5, 135–146. [Google Scholar] [PubMed] [Green Version]
- Pinquart, M.; Sorensen, S. Ethnic differences in stressors, resources, and psychological outcomes of family caregiving: A meta-analysis. Gerontologist 2005, 45, 90–106. [Google Scholar] [CrossRef] [PubMed]
- Verbakel, E. How to understand informal caregiving patterns in Europe? The role of formal long-term care provisions and family care norms. Scand. J. Public Health 2018, 46, 436–447. [Google Scholar] [PubMed] [Green Version]
- Bom, J.; Bakx, P.; Schut, F.; Van Doorslaer, E. Health effects of caring for and about parents and spouses. J. Econ. Ageing 2019, 14, 100196. [Google Scholar]
- Carmichael, F.; Charles, S.; Hulme, C. Who will care? Employment participation and willingness to supply informal care. J. Health Econ. 2010, 29, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Pickard, L. A growing care gap? The supply of unpaid care for older people by their adult children in England to 2032. Ageing Soc. 2015, 35, 96–123. [Google Scholar]
- Kooiker, S.; de Jong, A.; Verbeek-Oudijk, D.; de Boer, A. Toekomstverkenning Mantelzorg Aan Ouderen in 2040; SCP: London, UK, 2019. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar]
- Aron, A.; Aron, E.N.; Smollan, D. Inclusion of other in the self scale and the structure of interpersonal closeness. J. Pers. Soc. Psychol. 1992, 63, 596. [Google Scholar]
- Katz, S. Assessing Self-Maintenance: Activities of Daily Living, Mobility, and Instrumental Activities of Daily Living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar]
- Lyonette, C.; Yardley, L. The influence on carer wellbeing of motivations to care for older people and the relationship with the care recipient. Ageing Soc. 2003, 23, 487–506. [Google Scholar] [CrossRef] [Green Version]
- Lemay, E.P., Jr.; Neal, A.M. The wishful memory of interpersonal responsiveness. J. Pers. Soc. Psychol. 2013, 104, 653. [Google Scholar]
- Abell, N. Assessing Willingness to Care for Persons with AIDS: Validation of a New Measure. Res. Soc. Work Pract. 2001, 11, 118–130. [Google Scholar] [CrossRef]
- Hermanns, N. WHO-5-Well-Being-Index. Der Diabetol. 2007, 3, 464–465. [Google Scholar]
- Pearlin, L.I. Caregiver’s Stress and Coping Study; University of California: San Francisco, CA, USA, 1988. [Google Scholar]
- Bédard, M.; Molloy, D.W.; Squire, L.; Dubois, S.; Lever, J.A.; O’Donnell, M. The Zarit Burden Interview: A new short version and screening version. Gerontologist 2001, 41, 652–657. [Google Scholar] [PubMed] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. life Res. 2011, 20, 1727–1736. [Google Scholar] [PubMed] [Green Version]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar]
- Miller, W.C.; Anton, H.A.; Townson, A.F. Measurement properties of the CESD scale among individuals with spinal cord injury. Spinal Cord 2008, 46, 287–292. [Google Scholar] [PubMed]
- Sebern, M.D.; Whitlatch, C.J. Dyadic relationship scale: A measure of the impact of the provision and receipt of family care. Gerontologist 2007, 47, 741–751. [Google Scholar] [CrossRef] [PubMed]
- Hendrick, S.S.; Dicke, A.; Hendrick, C. The relationship assessment scale. J. Soc. Pers. Relat. 1998, 15, 137–142. [Google Scholar]
- Landfeldt, E.; Zethraeus, N.; Lindgren, P. Standardized questionnaire for the measurement, valuation, and estimation of costs of informal care based on the opportunity cost and proxy good method. Appl. Health Econ. Health Policy 2019, 17, 15–24. [Google Scholar]
- Losada, A.; Márquez-González, M.; Vara-García, C.; Barrera-Caballero, S.; Cabrera, I.; Gallego-Alberto, L.; Olmos, R.; Romero-Moreno, R. Measuring familism in dementia family caregivers: The revised familism scale. Aging Ment. Health 2019, 24, 784–788. [Google Scholar] [CrossRef]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The brief illness perception questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar]
- Steger, M.F.; Frazier, P.; Kaler, M.; Oishi, S. The meaning in life questionnaire: Assessing the presence of and search for meaning in life. J. Couns. Psychol. 2006, 53, 80–93. [Google Scholar] [CrossRef]
- Schwartz, S.H. A proposal for measuring value orientations across nations. Quest. Packag. Eur. Soc. Surv. 2003, 259, 261. [Google Scholar]
- Soto, C.J.; John, O.P. Short and extra-short forms of the Big Five Inventory–2: The BFI-2-S and BFI-2-XS. J. Res. Pers. 2017, 68, 69–81. [Google Scholar]
- Fraley, R.C.; Heffernan, M.E.; Vicary, A.M.; Brumbaugh, C.C. The experiences in close relationships—Relationship Structures Questionnaire: A method for assessing attachment orientations across relationships. Psychol. Assess. 2011, 23, 615. [Google Scholar] [PubMed] [Green Version]
- Spreng, R.N.; McKinnon, M.C.; Mar, R.A.; Levine, B. The Toronto Empathy Questionnaire: Scale Development and Initial Validation of a Factor-Analytic Solution to Multiple Empathy Measures. J. Pers. Assess. 2009, 91, 62–71. [Google Scholar] [PubMed] [Green Version]
- Pearlin, L.I.; Schooler, C. The structure of coping. J. Health Soc. Behav. 1978, 19, 2–21. [Google Scholar] [PubMed]
- Berg, C.A.; Schindler, I.; Maharajh, S. Adolescents’ and mothers’ perceptions of the cognitive and relational functions of collaboration and adjustment in dealing with type 1 diabetes. J. Fam. Psychol. 2008, 22, 865. [Google Scholar] [PubMed] [Green Version]
- Bodenmann, G. Stress und Coping Bei Paaren [Stress and Coping in Couples]; Hogrefe: Göttingen, Germany, 2000; ISBN 3801713520. [Google Scholar]
- Archbold, P.G.; Stewart, B.J.; Greenlick, M.R.; Harvath, T. Mutuality and preparedness as predictors of caregiver role strain. Res. Nurs. Health 1990, 13, 375–384. [Google Scholar] [PubMed]
- Perceived Partner Responsiveness Scale (PPRS) (Reis & Carmichael, 2006). Available online: https://onlinelibrary.wiley.com/doi/pdf/10.1002/9781119102991.ch57 (accessed on 15 August 2021).
- Kempen, G.; Van Eijk, L.M. The psychometric properties of the SSL12-I, a short scale for measuring social support in the elderly. Soc. Indic. Res. 1995, 35, 303–312. [Google Scholar]
- Fairclough, D.L. Design and Analysis of Quality of Life Studies in Clinical Trials; CRC Press: Boca Raton, FL, USA, 2010; ISBN 1420061186. [Google Scholar]
- Little, R.J.A. A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar]
- Van Buuren, S. Flexible Imputation of Missing Data; CRC Press: Boca Raton, FL, USA, 2018; ISBN 0429960352. [Google Scholar]
- Myers, T.A. Goodbye, listwise deletion: Presenting hot deck imputation as an easy and effective tool for handling missing data. Commun. Methods Meas. 2011, 5, 297–310. [Google Scholar]
- Rubin, D.B. Multiple Imputation for Non Response in Surveys; Wiley: New York, NY, USA, 1987. [Google Scholar]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [PubMed]
- Van den Berg, B.; Brouwer, W.B.F.; Koopmanschap, M.A. Economic valuation of informal care. Eur. J. Health Econ. Former. HEPAC 2004, 5, 36–45. [Google Scholar]
- Bolger, N.; Laurenceau, J.-P. Intensive Longitudinal Methods: An Introduction to Diary and Experience Sampling Research; Guilford Press: New York, NY, USA, 2013; ISBN 146250678X. [Google Scholar]

{kind=link}
| Section/Measure | Description and Max*N of Items | Scoring | IV, DV, Mod, Med | CG Baseline | CG Follow Up | CR BASELINE | CR Follow Up |
|---|---|---|---|---|---|---|---|
| Core | |||||||
| Caregiver Self-report Personal and Demographic Questionnaire | Seventy four (74) items addressing age, gender, home location, partnership status, relationship type, religion, ethnicity, household composition, highest level of attained education, employment status, income, other dependents, own health condition, health condition of care recipient, length of illness, distance from caregiver to care recipient, treatment or medication, | Categorical responses | IV, Mod, Med | ✔ | ✔ | ✘ | ✘ |
| Care Recipient Self-report Personal and Demographic Questionnaire | Fifty eight (58) items addressing age, gender, home location, partnership status, relationship type, religion, ethnicity, highest level of attained education, employment status, income, other dependents, own health condition, health condition of care recipient, length of illness, distance from caregiver to care recipient | Categorical responses | IV, Mo, Me | ✘ | ✘ | ✔ | ✔ |
| Inclusion of Other Self Scale (IOS) [32] | One item assesses the extent to which participants include another person in their sense of self | 7-point Likert scale in which participants choose a pair of circles from seven with different degrees of overlap (ranging from 1 = no overlap; to 7 = most overlap) Higher scores indicate greater inclusion of other in self | IV, Mod, Med | ✔ | ✔ | ✔ | ✔ |
| Katz ADL [33] | Six items assess functional status via measurement of the person’s ability to perform activities of daily living independently | Items address independence yes (1), no (0) in performing bathing, dressing, toileting, transferring, continence, and feeding. A score of 6 indicates full function, 4 indicates moderate impairment, and 2 or less indicates severe functional impairment. | IV | ✔ | ✔ | ✔ | ✔ |
| COVID-19 related questions | Ten (10) items address the impact of COVID-19 on employment, access to support services, willingness to care, provision of practical, emotional, personal care | Numerical and categorical | Med, Mod | ✔ | ✔ | ✘ | ✘ |
| Use of paid home care services and their characteristics | Thirty five (35) items in the caregiver baseline and follow up and 37 items in the care recipient baseline and follow up assess the self-reported use of paid home care services by the care recipient. Demographics of paid care workers i.e., gender, age, nationality, migration background, live-in or live-out | Numerical and categorical | IV, DV | ✔ | ✔ | ✔ | ✔ |
| Financial benefits | Six items regarding: cash benefits, financial compensation during care leave, tax benefits e.g., exemptions, deductions, credits, coverage of social or pension contributions, caregiver credits, and health insurance | Numerical and dichotomous questions | IV, Mod/Med | ✔ | ✔ | ✘ | ✘ |
| Motivations in Elder Care Scale (MECS) [34] | Two item sub-scales: Extrinsic Motivations to Care (EXMECS) and Intrinsic Motivations to Care (INMECS) | 5-point scale ranging from 1 (Strongly disagree) to 5 (Strongly agree). A higher score indicates greater motivations to provide care. | IV, DV, Med, Mod | ✔ | ✔ | ✘ | ✘ |
| Partner-Specific Communal Motivation Scale (CMS) [35] | Ten (10) items address communal motivation to care | 9-point scale ranging from 1 (Extremely disagree) to 9 (Extremely agree). A high score reflects greater CM. (items 2, 5 and 10 are reverse scored before summing) | IV | ✔ | ✔ | ✔ adapted | ✔ adapted |
| Willingness to Care Scale [36] | Thirty (30) items assess willingness to provide emotional, instrumental, and nursing care related tasks | 5-point Likert scale (1 = completely unwilling to complete the task, 5 = completely willing) | IV, DV, Med, Mod | ✔ | ✔ | ✘ | ✘ |
| Willingness to Receive Care, adapted from Abell [36] | Three items assess willingness to receive emotional, instrumental, and nursing care-related tasks | 5-point Likert scale (1 = completely unwilling to complete the task, 5 = completely willing) | IV, DV, Med, Mod | ✘ | ✘ | ✔ | ✔ |
| The World Health Organisation- Five Well-Being Index (WHO-5) [37] | Five items assess caregiver/care recipient well-being | 6-point scale ranging from 0 (at no time) to 5 (all of the time). High scores indicate greater wellbeing | DV | ✔ | ✔ | ✔ | ✔ |
| The GAINS Scale [38] | Ten (10) items assess perceived gains associated with caregiving | Items measured on a 4-point Likert scale from 0 = Not at all to 3= A lot, with a possible maximum score of 30. Higher scores indicate greater gains. | DV | ✔ | ✔ | ✘ | ✘ |
| Short Form Zarit Burden Interview (ZBI-12) [39] | Twelve (12) items assess caregiver burden | 5-point Likert scale ranging from 0 = Never to 4 = Always Total scores range from 0 to 48 with higher scores (>20) indicating high levels of burden | DV | ✔ | ✔ | ✘ | ✘ |
| EQ-5D-5L and EQ VAS [40] | Five dimensions of health state are assessed using 5 items: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The EQ VAS is a single item that records the patient’s self-rated health on a vertical “ladder” visual analogue scale. | Each dimension has 5 levels: no problems, slight problems, moderate problems, severe problems and extreme problems. The VAS endpoints are labelled ‘The best imaginable health state (100)’ and ‘The worst imaginable health state (0) | IV, DV | ✔ | ✔ | ✔ | ✔ |
| Centre for Epidemiological Studies Depression Scale (CESD-10) [41,42] | This 10-item screening tool assesses depressive symptoms in the past week | 4-point Likert scale ranging from 0 = Rarely or none of the time to 3 = All the time. (items 5 and 8 are reverse scored before summing) | IV, DV | ✔ | ✔ | ✔ | ✔ |
| Dyadic Relationship Scale (DRS) [43] | The 11-item scale for the caregiver baseline and follow up and the 10 item scale for the care recipient baseline and follow up assess positive dyadic interactions and negative dyadic strain experienced by caregivers and care recipients. | 5-point Likert scale ranging from 0 = strongly agree to 4 = strongly disagree. Reversed items: 3,4,5,8,11. Higher scores indicate higher levels of strain and positive interaction. | DV | ✔ | ✔ | ✔ | ✔ |
| Relationship satisfaction (RAS) [44] | A single item measure of relationship satisfaction | 5-point Likert scale ranging from 1 = not satisfied to 5 = very satisfied | DV | ✔ | ✔ | ✔ | ✔ |
| Caregiver Indirect and Informal Care Cost Assessment Questionnaire [45] | Twelve (12) items enable calculation of estimated indirect (productivity) and informal care costs as mutually exclusive subsets of total costs | DV, IV | ✔ | ✔ | ✘ | ✘ | |
| Module 1 | |||||||
| Revised Familism Scale (RFS) [46] | Twenty one (21) items across three sub-scales:
| 5-point Likert scale, with 0 indicating ‘very much in disagreement’ and 4 ‘very much in agreement.’ | IV | ✔ | ✔ | ✔ | ✔ |
| Brief Illness Perception Questionnaire (B-IPQ) [47] | Nine items, with a single item each assessing illness consequences, timeline, personal control, treatment control, identity, coherence, emotional representation, and illness concern | Each item assessed on a scale from 1 to 10 (modified response range). A summed score represents the degree to which the illness is perceived as threatening. | IV | ✔ | ✔ | ✔ | ✔ |
| Meaning in Life Questionnaire (MLQ) [48] | Five items each assess two dimensions of meaning in life: (1) Presence of Meaning (2) Search for Meaning. | 7-point Likert scale from 1 (‘absolutely untrue’) to 7 (‘absolutely true’). | IV | ✔ | ✔ | ✔ | ✔ |
| Portrait Values Questionnaire (PVQ-21) [49] | Nine items assess altogether two subscales of personal values: Self-transcendence and Self-enhancement. | 6-point Likert response scale from “very much like me” (1), to “not like me at all. (6).” The subscale score is obtained by calculating the mean of the relevant item scores. | IV | ✔ | ✔ | ✔ | ✔ |
| Perceived choice in assuming the caregiving role | Single item: Do you feel you had a choice in taking on this responsibility of caring for your loved one? | Yes/No | IV | ✔ | ✔ | ✔ | ✔ |
| The importance of religion | Single item: What is the importance of religion in your life? | 4-point response scale from 1 (“not important at all”) to 4 (“very important”) | IV | ✔ | ✔ | ✔ | ✔ |
| Module 2 | |||||||
| The geographies of care | Thirty (30) items for the CG survey and 8 for the CR identify two aspects of caregiving geographies; a) setting, access, characteristics; and b) perceived geographical barriers and facilitators to informal care provision. | Mixed format, Likert scale responses and dichotomous questions (Yes/No) | IV | ✔ | ✔ | ✔ | ✔ |
| Big-Five Inventory Extra Short Form (BFI-2-XS) [50] | 15 items measure the domains of Extraversion, Agreeableness, Conscientiousness, Neuroticism, Openness to Experience | 5-point Likert scale ranging from 1 = Disagree strongly to 5= Agree strongly. | IV | ✔ | ✔ | ✔ | ✔ |
| The Relationship Structures Questionnaire of the Experiences in Close Relationships-Revised (ECR-RS) [51] | Nine items assess (1) attachment-related anxiety and (2) attachment-related avoidance | 4-point Likert scale ranging from 1 = Strongly Disagree to 4 = Strongly Agree. Scores are computed for each of the two subscales by averaging item responses. | IV | ✔ | ✔ | ✔ | ✔ |
| Toronto Empathy Questionnaire (TEQ) [52] | Sixteen (16) items assess empathy as a primarily emotional process. | 5-point Likert scale ranging from 0 = Never to 4 = Always. Scores below 45 are indicative of below average empathy levels. | IV | ✔ | ✔ | ✔ | ✔ |
| The Pearlin Mastery Scale [53] | This seven-item scale assesses the extent to which an individual regards their life chances as being under their personal control | 4-point Likert scale ranging from 1 = Strongly Disagree to 4 = Strongly Agree | IV | ✔ | ✔ | ✔ | ✔ |
| Module 3 | |||||||
| Perception of Collaboration Questionnaire (PCQ) [54] | This nine-item scale assesses three dimensions of collaboration between caregiver and care recipient: (1) Cognitive Compensation (2) Interpersonal Enjoyment and (3) Frequency. | 5-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree with higher scores indicating stronger agreement. Items 5 and 9 are reverse scored. | IV, Me | ✔ | ✔ | ✔ | ✔ |
| Dyadic Coping Inventory (DCI)-communication subscale [55] | The eight-item DCI measures perceived communication and dyadic coping within a close relationship when one or both dyad members are stressed. | 5-point scale from 1 = very rarely to 5 = very often. Subscale scores include: (a) Stress communicated by oneself (SCO: items 1, 2, 3, and 4); (b) Stress communication of the partner (SCP: items 5, 6, 7 and 8). | IV, Me | ✔ | ✔ | ✔ | ✔ |
| Mutuality Scale (MS) [56] | Fifteen (15) items measure mutuality from either the caregiver or the care recipient perspective, across four dimensions: love and affection, shared pleasurable activities, shared values, and reciprocity. | 5-point Likert scale ranging from 1 = not at all to 4 = a great deal. A total scale score is computed by averaging all item scores. | IV, Me | ✔ | ✔ | ✔ | ✔ |
| The perceived partner responsiveness scale (PPRS) [57] | The 12-item PPRS measures the degree to which people feel that their significant others are responsive to them. | 9-point Likert scale ranging from 1 = not at all true to 9 = completely true. | IV, Me | ✔ | ✔ | ✔ | ✔ |
| Social Support List (SSL) [58] | Six items measure perceived supportive behaviours and seven items measure perceived unsupportive behaviour from the caregiver and the care recipient perspective. | 4-point Likert scale ranging from 1 = rarely or never to 4 = very often. The scores are summed into two indexes, with a higher score indicating a higher frequency of supportive and unsupportive behaviour. | IV, Me | ✔ | ✔ | ✔ | ✔ |
| Module 4 | |||||||
| The influence of informal care on employment and the associated costs. | Seven self-reported items address the influences of informal care on the employment situation of the caregiver, and the associated costs of this. | Categorical and numerical answers | IV, DV | ✔ | ✔ | ✘ | ✘ |
| Types of home care services provided by paid care workers | Eighteen (18) items assess which tasks and how many hours of care tasks (total and per type of care task) are provided by paid home care workers | Categorical and numerical answers. | IV, DV | ✔ | ✔ | ✘ | ✘ |
| Rationale for hiring of paid care workers | Twenty two (22) items assess the rationale for hiring paid home care workers and the decision to hire or not hire migrant care workers | Categorical answers, with each item treated separately | DV | ✔ | ✔ | ✔ | ✔ |
| Out-of-pocket expenses incurred by caregivers as a result of their caregiving role. | Twenty five (25) items measure out-of-pocket costs for caregivers (both in terms of overall total and per type of cost). These costs include expenditure on, e.g., caregiving support services, medical care, food, travel, home care services, aids, appliances and home modifications due to care recipient’s condition. | Categorical and numerical answers. | IV, DV | ✔ | ✔ | ✘ | ✘ |
| Care benefits received by the care recipient | Four self-reported items measure care benefits received (both in terms of overall total and per type of care benefit), e.g., tax benefits, cash benefits, care vouchers. | Categorical and numerical answers. | IV, DV | ✘ | ✘ | ✔ | ✔ |
| Self-reported questionnaire on the use of, and the out-of-pocket expenses for, care services, as well as assistive devices and aids used by the care recipient. | Twenty two (22) items detail which types of support services the care recipient receives in relation to their care and the out of pocket expenses spent in relation to their care. | Categorical and numerical answers | IV, DV | ✘ | ✘ | ✔ | ✔ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morrison, V.; Zarzycki, M.; Vilchinsky, N.; Sanderman, R.; Lamura, G.; Fisher, O.; Ferraris, G.; Elayan, S.; Buskens, E.; Bei, E.; et al. A Multinational Longitudinal Study Incorporating Intensive Methods to Examine Caregiver Experiences in the Context of Chronic Health Conditions: Protocol of the ENTWINE-iCohort. Int. J. Environ. Res. Public Health 2022, 19, 821. https://doi.org/10.3390/ijerph19020821
Morrison V, Zarzycki M, Vilchinsky N, Sanderman R, Lamura G, Fisher O, Ferraris G, Elayan S, Buskens E, Bei E, et al. A Multinational Longitudinal Study Incorporating Intensive Methods to Examine Caregiver Experiences in the Context of Chronic Health Conditions: Protocol of the ENTWINE-iCohort. International Journal of Environmental Research and Public Health. 2022; 19(2):821. https://doi.org/10.3390/ijerph19020821
Chicago/Turabian StyleMorrison, Val, Mikołaj Zarzycki, Noa Vilchinsky, Robbert Sanderman, Giovanni Lamura, Oliver Fisher, Giulia Ferraris, Saif Elayan, Erik Buskens, Eva Bei, and et al. 2022. "A Multinational Longitudinal Study Incorporating Intensive Methods to Examine Caregiver Experiences in the Context of Chronic Health Conditions: Protocol of the ENTWINE-iCohort" International Journal of Environmental Research and Public Health 19, no. 2: 821. https://doi.org/10.3390/ijerph19020821
APA StyleMorrison, V., Zarzycki, M., Vilchinsky, N., Sanderman, R., Lamura, G., Fisher, O., Ferraris, G., Elayan, S., Buskens, E., Bei, E., Looijmans, A., Angelini, V., & Hagedoorn, M. (2022). A Multinational Longitudinal Study Incorporating Intensive Methods to Examine Caregiver Experiences in the Context of Chronic Health Conditions: Protocol of the ENTWINE-iCohort. International Journal of Environmental Research and Public Health, 19(2), 821. https://doi.org/10.3390/ijerph19020821