
Hip Range of Motion and Strength in Male Athletes with Stage 1 Osteitis Pubis: A Cross-Sectional and Correlational Study

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Procedure
2.4. Reliability of the Measures
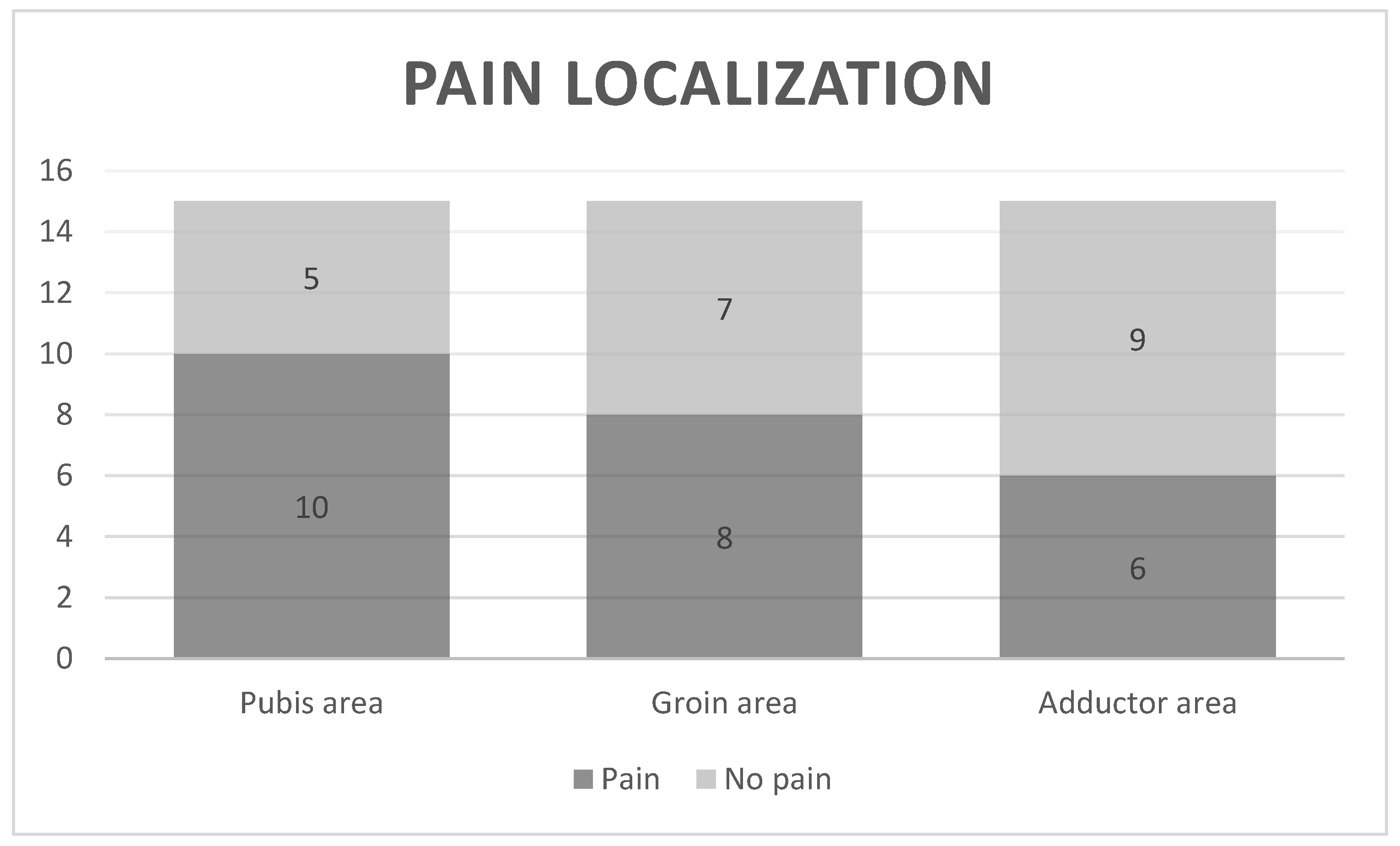
2.5. Pain Intensity and Localization
2.6. Physical Function
2.7. Range of Motion
2.8. Isometric Strength
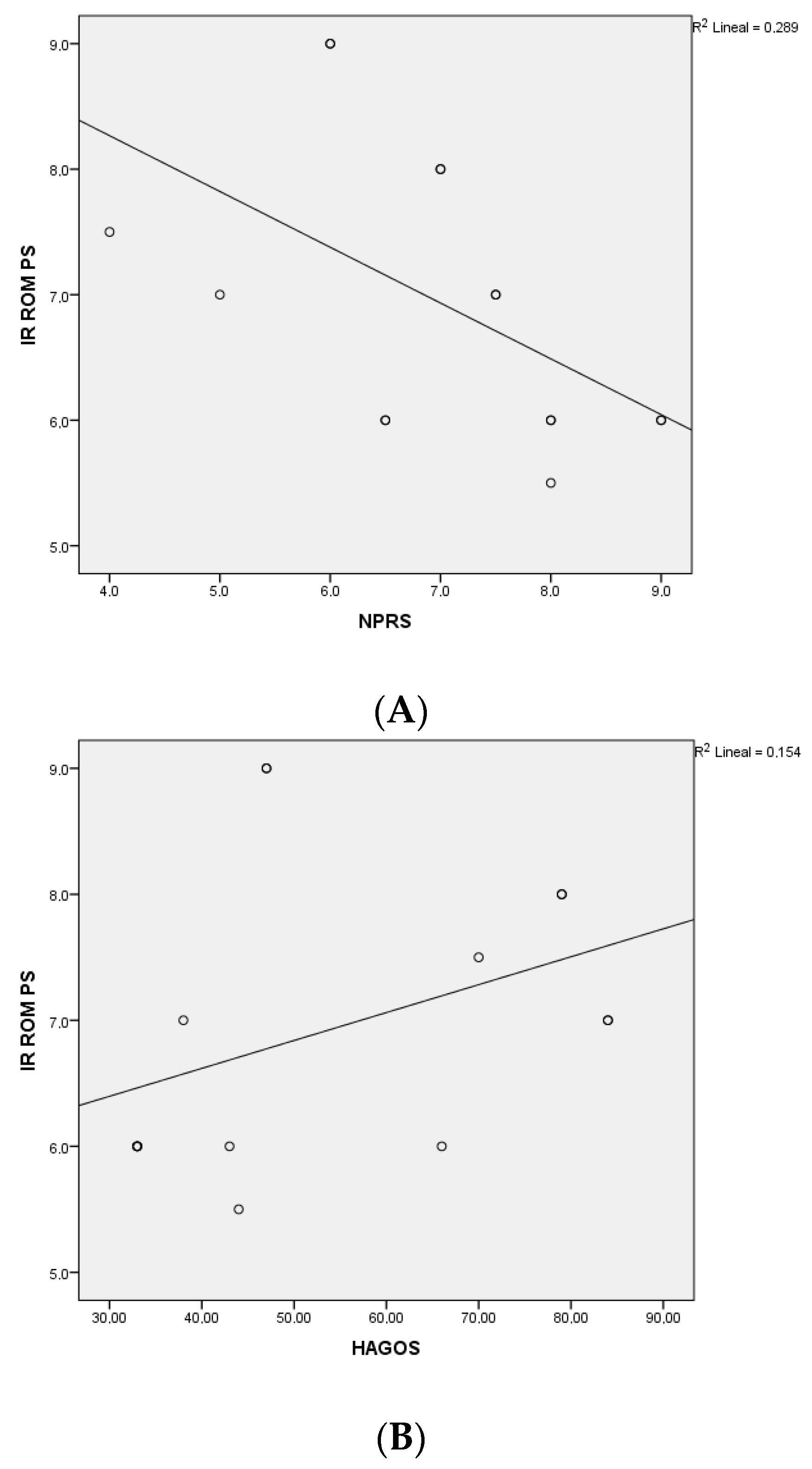
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verrall, G.M.; Henry, L.; Fazzalari, N.L.; Slavotinek, J.P.; Oakeshott, R.D. Bone Biopsy of the Parasymphyseal Pubic Bone Region in Athletes with Chronic Groin Injury Demonstrates New Woven Bone Formation Consistent with a Diagnosis of Pubic Bone Stress Injury. Am. J. Sports Med. 2008, 36, 2425–2431. [Google Scholar] [CrossRef] [PubMed]
- Cohen, B.; Kleinhenz, D.; Schiller, J.; Tabaddor, R. Understanding Athletic Pubalgia: A Review. Rhode Isl. Med. J. 2016, 99, 31. [Google Scholar]
- Sheen, A.J.; Stephenson, B.M.; Lloyd, D.M.; Robinson, P.; Fevre, D.; Paajanen, H.; de Beaux, A.; Kingsnorth, A.; Gilmore, O.J.; Bennett, D.; et al. ‘Treatment of the Sportsman’s groin’: British Hernia Society’s 2014 position statement based on the Manchester Consensus Conference. Br. J. Sports Med. 2013, 48, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Hiti, C.J.; Stevens, K.J.; Jamati, M.K.; Garza, D.; Matheson, G.O. Athletic Osteitis Pubis. Sports Med. 2011, 41, 361–376. [Google Scholar] [CrossRef] [PubMed]
- Orchard, J.; Seward, H. Epidemiology of injuries in the Australian Football League, seasons 1997–2000. Br. J. Sports Med. 2002, 36, 39–44. [Google Scholar] [CrossRef]
- Lovell, G. The diagnosis of chronic groin pain in athletes: A review of 189 cases. Aust. J. Sci. Med. Sport 1995, 27, 76–79. [Google Scholar] [PubMed]
- Gaudino, F.; Spira, D.; Bangert, Y.; Ott, H.; Zobel, B.B.; Kauczor, H.-U.; Weber, M.-A. Osteitis pubis in professional football players: MRI findings and correlation with clinical outcome. Eur. J. Radiol. 2017, 94, 46–52. [Google Scholar] [CrossRef]
- Phillips, E.; Khoury, V.; Wilmot, A.; Kelly, J.D. Correlation Between Cam-Type Femoroacetabular Impingement and Radiographic Osteitis Pubis. Orthopedics 2016, 39, e417–e422. [Google Scholar] [CrossRef][Green Version]
- Verrall, G.; Hamilton, I.; Slavotinek, J.; Oakeshott, R.; Spriggins, A.; Barnes, P.; Fon, G. Hip joint range of motion reduction in sports-related chronic groin injury diagnosed as pubic bone stress injury. J. Sci. Med. Sport 2005, 8, 77–84. [Google Scholar] [CrossRef]
- Giai Via, A.; Frizziero, A.; Finotti, P.; Oliva, F.; Randelli, F.; Maffulli, N. Management of osteitis pubis in athletes: Rehabilitation and return to training—A review of the most recent literature. Open Access J. Sport Med. 2018, 10, 1–10. [Google Scholar] [CrossRef]
- Rodriguez, C.; Miguel, A.; Lima, H.; Heinrichs, K. Osteitis Pubis Syndrome in the Professional Soccer Athlete: A Case Report. J. Athl. Train. 2001, 36, 437–440. [Google Scholar] [PubMed]
- Verrall, G.M.; Slavotinek, J.P.; Barnes, P.G.; Esterman, A.; Oakeshott, R.D.; Spriggins, A.J. Hip joint range of motion restriction precedes athletic chronic groin injury. J. Sci. Med. Sport 2007, 10, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, P.M.; Kelly, B.T.; Jacobs, R.; McGrady, L.; Wang, M. The effect of dynamic femoroacetabular impingement on pubic symphysis motion: A cadaveric study. Am J Sports Med. 2012, 40, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Rambani, R.; Hackney, R. Loss of range of motion of the hip joint: A hypothesis for etiology of sports hernia. Muscle Ligaments Tendons J. 2019, 05, 29–32. [Google Scholar] [CrossRef]
- Omar, I.M.; Zoga, A.C.; Kavanagh, E.C.; Franzcr, G.K.; Bergin, D.; Gopez, A.G.; Morrison, W.B.; Meyers, W.C. Athletic pubalgia and “sports hernia”: Optimal MR imaging technique and findings. Radiographics 2008, 28, 1415–1438. [Google Scholar] [CrossRef]
- Williams, P.R.; Thomas, D.P.; Downes, E.M. Osteitis pubis and instability of the pubic symphysis: When nonoperative measures fail. Am J Sports Med. 2000, 28, 350–355. [Google Scholar] [CrossRef]
- Garvey, J.F.W.; Read, J.W.; Turner, A. Sportsman hernia: What can we do? Hernia 2010, 14, 17–25. [Google Scholar] [CrossRef]
- Akgün, A.S.; Agirman, M. Association between cam-type femoroacetabular impingement and osteitis pubis in non-athletic population on magnetic resonance imaging. J. Orthop. Surg. Res. 2019, 14, 329. [Google Scholar] [CrossRef]
- Saito, M.; Utsunomiya, H.; Hatakeyama, A.; Nakashima, H.; Nishimura, H.; Matsuda, D.K.; Sakai, A.; Uchida, S. Hip Arthroscopic Management Can Improve Osteitis Pubis and Bone Marrow Edema in Competitive Soccer Players With Femoroacetabular Impingement. Am. J. Sports Med. 2019, 47, 408–419. [Google Scholar] [CrossRef]
- Krishnamoorthy, V.P.; Kunze, K.N.; Beck, E.C.; Cancienne, J.M.; O’Keefe, L.S.; Ayeni, O.R.; Nho, S.J. Radiographic Prevalence of Symphysis Pubis Abnormalities and Clinical Outcomes in Patients With Femoroacetabular Impingement Syndrome. Am. J. Sports Med. 2019, 47, 1467–1472. [Google Scholar] [CrossRef]
- Mohammad, W.S.; Abdelraouf, O.R.; Elhafez, S.M.; Abdel-Aziem, A.A.; Nassif, N.S. Isokinetic imbalance of hip muscles in soccer players with osteitis pubis. J. Sports Sci. 2014, 32, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, W.S.; Elsais, W.M. Deficits in eccentric antagonist/concentric agonist strength ratios: A comparative study of football players with and without osteitis pubis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1559–1564. [Google Scholar]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef]
- Thorborg, K.; Holmich, P.; Christensen, R.; Petersen, J.; Roos, E. The Copenhagen Hip and Groin Outcome Score (HAGOS): Development and validation according to the COSMIN checklist. Br. J. Sports Med. 2011, 45, 478–491. [Google Scholar] [CrossRef]
- Pua, Y.-H.; Wrigley, T.; Cowan, S.; Bennell, K. Intrarater Test-Retest Reliability of Hip Range of Motion and Hip Muscle Strength Measurements in Persons With Hip Osteoarthritis. Arch. Phys. Med. Rehabilitation 2008, 89, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.-H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of Lower Limb Muscle Strength and Power Using Hand-Held and Fixed Dynamometry: A Reliability and Validity Study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef]
- de Bruin, E.D.; Rozendal, R.H.; Stüssi, E. Reliability of phase-velocity measurements of tibial bone. Phys. Ther. 1998, 78, 1166–1174. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Roach, K.; Miles, T.P. Normal hip and knee active range of motion: The relationship to age. Phys Ther. 1991, 71, 656–665. [Google Scholar] [CrossRef]
- Tak, I.; Engelaar, L.; Gouttebarge, V.; Barendrecht, M.; Van Den Heuvel, S.; Kerkhoffs, G.; Langhout, R.; Stubbe, J.; Weir, A. Is lower hip range of motion a risk factor for groin pain in athletes? A systematic review with clinical applications. Br. J. Sports Med. 2017, 51, 1611–1621. [Google Scholar] [CrossRef] [PubMed]
- Tak, I.; Langhout, R.; Groters, S.; Weir, A.; Stubbe, J.; Kerkhoffs, G. A new clinical test for measurement of lower limb specific range of motion in football players: Design, reliability and reference findings in non-injured players and those with long-standing adductor-related groin pain. Phys. Ther. Sport 2016, 23, 67–74. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Outcome | ICC (95% CI) |
|---|---|
| ABD ROM (°) | 0.97 (0.96,0.98) |
| ADD ROM (°) | 0.98 (0.97,0.99) |
| ER ROM (°) | 0.92 (0.9, 0.94) |
| IR ROM (°) | 0.98 (0.96,0.99) |
| ABD Strength (kg) | 0.97 (0.95,0.98) |
| ADD Strength (kg) | 0.95 (0.9,0.97) |
| ER Strength (kg) | 0.98 (0.97,0.99) |
| IR Strength (kg) | 0.97 (0.94,0.98) |
| OP Group M (SD) | Control Group M (SD) | p-Value | |
|---|---|---|---|
| Age (years) | 25.30 (4.42) | 22.73 (2.68) | 0.123 |
| Weight (kg) | 77.68 (8.79) | 73.86 (8.62) | 0.294 |
| Height (cm) | 181.60 (8.15) | 178.33 (6.92) | 0.293 |
| BMI (kg/cm2) | 23.46 (1.45) | 23.15 (1.98) | 0.680 |
| Weekly practice (hours) | 10.01 (4.34) | 10.52 (5.66) | 0.809 |
| Frequency (days/week) | 4.20 (0.81) | 3.80 (1.27) | 0.637 |
| OP Group (n = 15) | Control Group (n = 15) | ||||
|---|---|---|---|---|---|
| Outcomes | Differences (p-Value) | Differences (p-Value) | Between-Groups Differences p-Value | ||
| IR ROM (°) | |||||
| PS | 6.80 (1.11) | −4.45 (−6.93; −1.96) 0.003 | 18.10 (6.43) | −0.40 (−4.13; 3.33) 0.822 | −11.30 (−15.58; −7.01) <0.001 |
| Non-PS | 11.25 (3.51) | 18.50 (9.43) | −7.25 (−13.73; −0.76) 0.014 | ||
| ER ROM (°) | |||||
| PS | 16.40 (5.58) | −7.20 (−11.67; −2.72) 0.005 | 22.10 (7.79) | −0.86 (−3.46; 1.73) 0.486 | −5.70 (−11.24; −0.15) 0.044 |
| Non-PS | 23.60 (8.84) | 22.96 (1.52) | 0.63 (−6.27; 7.54) 0.851 | ||
| ABD ROM (°) | |||||
| PS | 9.80 (4.51) | −1.20 (−3.87; 1.47) 0.336 | 11.47 (2.92) | 0.66 (−3.15; 4.48) 0.714 | −1.67 (−4.73; 1.40) 0.273 |
| Non-PS | 11.00 (7.36) | 10.80 (6.71) | 0.20 (−5.68; 6.08) 0.945 | ||
| ADD ROM (°) | |||||
| PS | 0.30 (0.48) | −3.70 (−4.71; −2.68) < 0.001 | 5.93 (2.12) | 0.13 (−1.72; 2.03) 0.883 | −5.63 (−7.05; −4.21) < 0.001 |
| Non-PS | 4.00 (1.05) | 5.80 (3.46) | −1.80 (−4.15; 0.55) 0.076 |
| OP Group (n = 15) | Control Group (n = 15) | ||||
|---|---|---|---|---|---|
| Outcomes | Differences (p-Value) | Differences (p-Value) | Between-Groups Differences p-Value | ||
| IR Strength (kg) | |||||
| PS | 7.58 (2.97) | 0.93 (−1.79; 3.66) 0.458 | 6.96 (1.52) | 0.44 (−0.12; 1.00) 0.116 | 0.61 (−1.25; 2.47) 0.503 |
| Non-PS | 6.64 (1.78) | 6.52 (1.41) | 0.11 (−1.20;1.44) 0.855 | ||
| ER Strength (kg) | |||||
| PS | 7.23 (2.28) | −1.24 (−1.96; −0.52) 0.004 | 7.79 (2.59) | 0.26 (−0.61; 1.13) 0.533 | −0.56 (−2.65; 1.52) 0.584 |
| Non-PS | 8.48 (2.89) | 7.53 (1.82) | 0.94 (−1.00; 2.88) 0.326 | ||
| ABD Strength (kg) | |||||
| PS | 10.01 (3.41) | 0.07 (−0,86; 1.00) 0.869 | 10.80 (3.99) | 0.22 (−0.76; 1.20) 0.638 | −0.79 (−3.98; 2.39) 0.610 |
| Non-PS | 9.94(1.59) | 10.58 (3.05) | −0.64 (−3.29; 2.00) 0.618 | ||
| ADD Strength (kg) | |||||
| PS | 9.01 (4.15) | 1.18 (−2.33; 4.70) 0.466 | 9.82 (2.47) | −0.02 (−0.72; 0.67) 0.936 | −0.81 (−3.54; 1.92) 0.545 |
| Non-PS | 7.83 (2.05) | 9.85 (2.75) | −2–20 (−4.13; 0.09) 0.060 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceballos-Laita, L.; Hernando-Garijo, I.; Medrano-de-la-Fuente, R.; Mingo-Gómez, M.T.; Carrasco-Uribarren, A.; Jiménez-del-Barrio, S. Hip Range of Motion and Strength in Male Athletes with Stage 1 Osteitis Pubis: A Cross-Sectional and Correlational Study. Int. J. Environ. Res. Public Health 2022, 19, 12824. https://doi.org/10.3390/ijerph191912824
Ceballos-Laita L, Hernando-Garijo I, Medrano-de-la-Fuente R, Mingo-Gómez MT, Carrasco-Uribarren A, Jiménez-del-Barrio S. Hip Range of Motion and Strength in Male Athletes with Stage 1 Osteitis Pubis: A Cross-Sectional and Correlational Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12824. https://doi.org/10.3390/ijerph191912824
Chicago/Turabian StyleCeballos-Laita, Luis, Ignacio Hernando-Garijo, Ricardo Medrano-de-la-Fuente, María Teresa Mingo-Gómez, Andoni Carrasco-Uribarren, and Sandra Jiménez-del-Barrio. 2022. "Hip Range of Motion and Strength in Male Athletes with Stage 1 Osteitis Pubis: A Cross-Sectional and Correlational Study" International Journal of Environmental Research and Public Health 19, no. 19: 12824. https://doi.org/10.3390/ijerph191912824
APA StyleCeballos-Laita, L., Hernando-Garijo, I., Medrano-de-la-Fuente, R., Mingo-Gómez, M. T., Carrasco-Uribarren, A., & Jiménez-del-Barrio, S. (2022). Hip Range of Motion and Strength in Male Athletes with Stage 1 Osteitis Pubis: A Cross-Sectional and Correlational Study. International Journal of Environmental Research and Public Health, 19(19), 12824. https://doi.org/10.3390/ijerph191912824