
Exploring the Nexus of Healthcare Employees’ Professional Quality, Health Psychology and Service Value: A Qualitative Study

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Grounded Theory
2.2. Research Design
2.3. Theoretical Sampling
3. Results
3.1. Open Coding
3.2. Axial Coding
3.3. Selective Coding
3.4. Theoretical Saturation Test
- (1)
- We will regularly visit the homes of rural residents, mainly to do some basic health management tasks, such as helping the elderly to regularly measure blood sugar and blood pressure, etc. For postoperative patients, we will also be responsible for rehabilitation training and guidance; I also observe the living conditions of the elderly and do a good job in disease prevention. (28-1-2 “door-to-door service”).
- (2)
- Develop long-term management plans for patients with chronic diseases such as diabetes, hypertension, and heart disease. For frequently occurring patients with neck, shoulder, back, and leg pain, endocrine disorders, and disease control. For common colds, fevers, and gastritis, the sick patient has the ability to deal with the disease in time. (25-1-1 “outpatient”)
- (3)
- Our regular prescriptions for chronic diseases are prescribed on a monthly basis, and he will come to you to prescribe them before he finishes his medicine. In this situation, we also try to explain patiently to patients. (9-3-2 “patience explain”)
- (4)
- Our own unit will also organize some training, and there will be more training in general business. (9-4-1 “community hospital autonomous training”)
- (5)
- After the training, you can indeed learn knowledge, gain some new knowledge, and use some new drugs. After all, you have graduated many years ago, and your knowledge is updated quickly. If you do not study, you will not be able to master it. (15-5-1 “theoretical knowledge”)
- (6)
- After training, there will be a certain impact on the patient’s satisfaction. Because the patient is selective, he thinks that he will trust you after he has asked you a few times to solve the problem. I will come to you, may leave a phone call, and call you when I have something to do. (15-6-1 “patient satisfaction”)
4. Analysis of Coding Results
- (1)
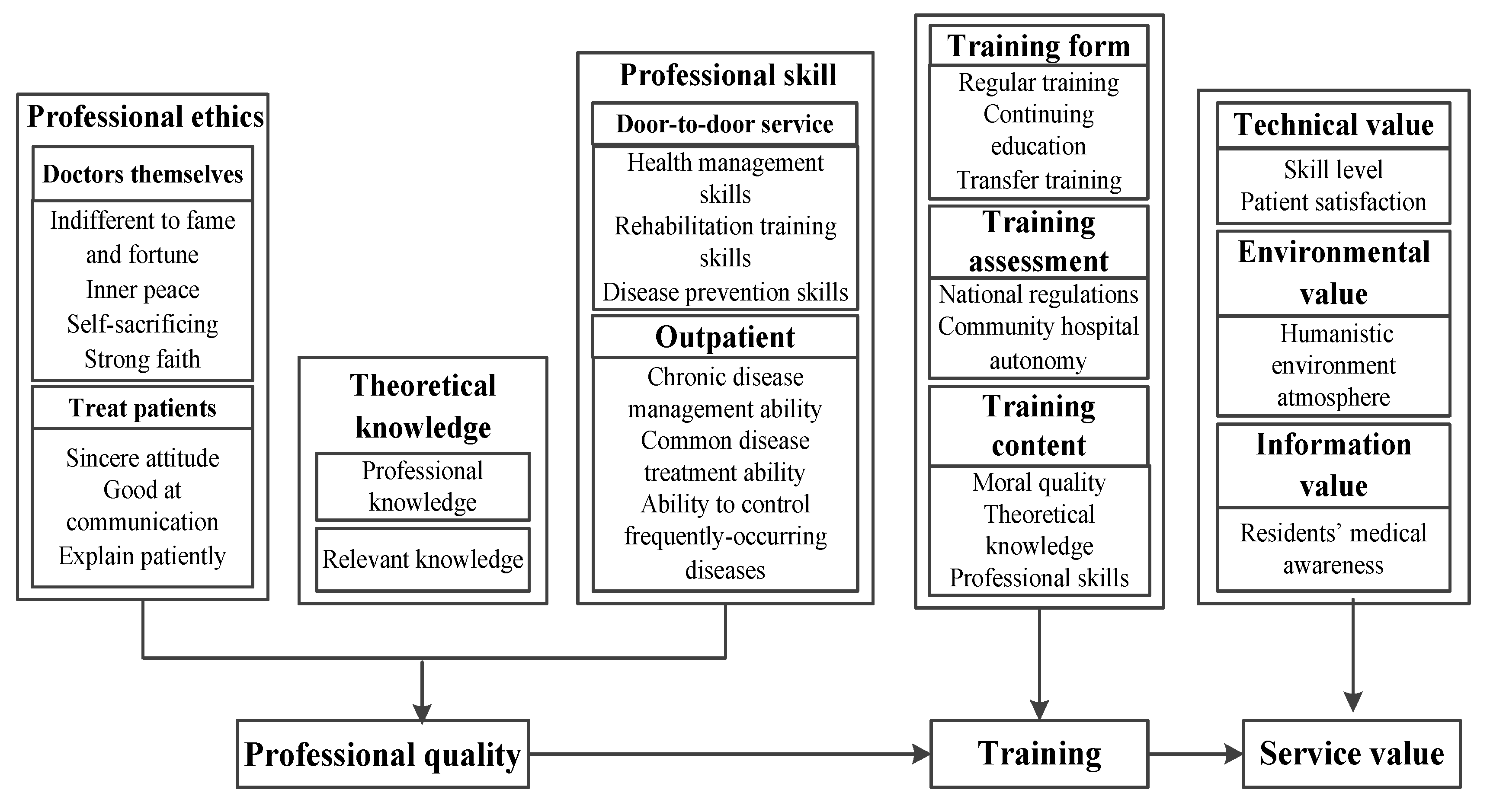
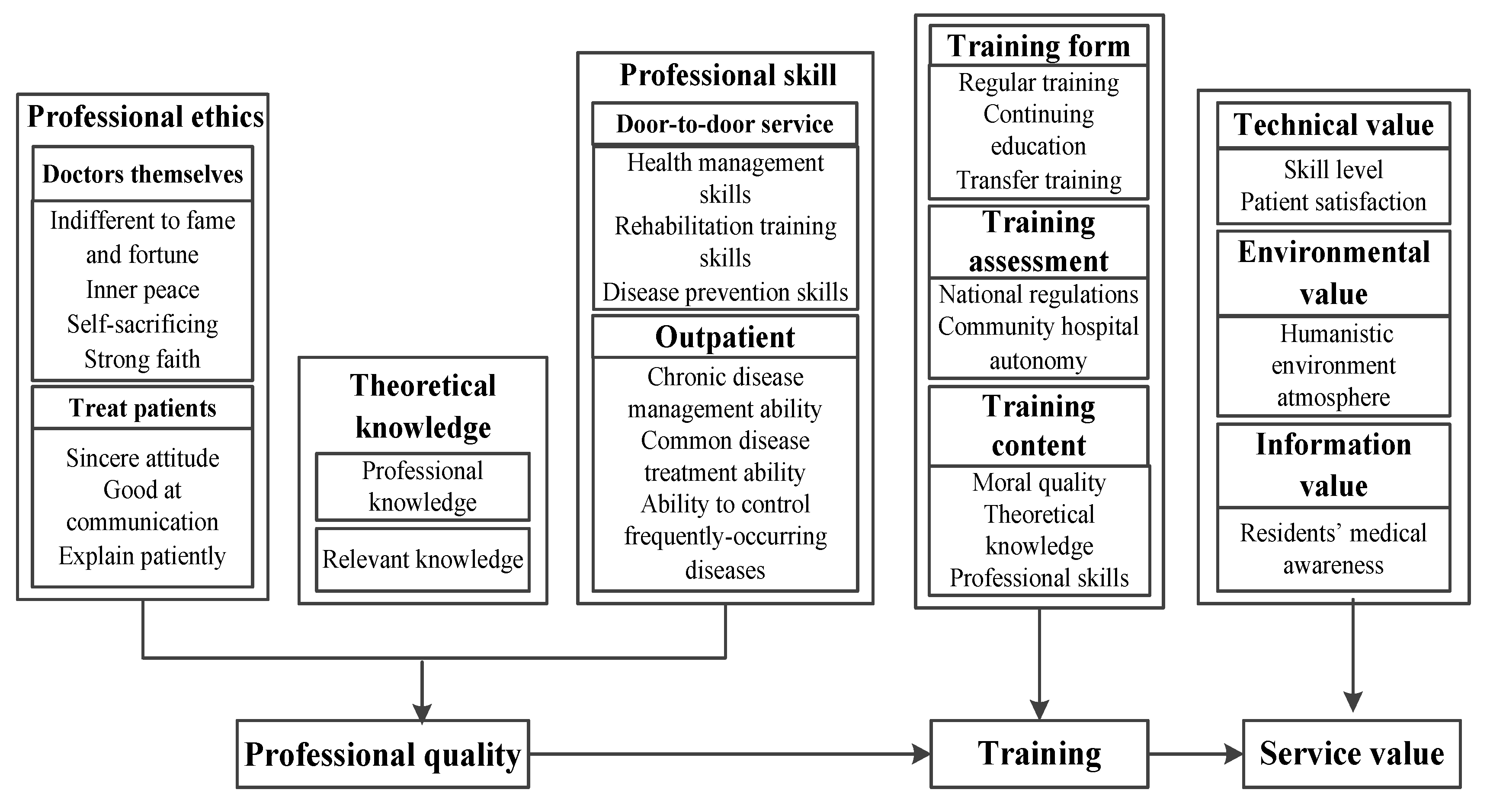
- It has formed a three-dimensional dimension of the professional quality of general practitioners, that is, the quality of professional ethics, theoretical knowledge, and professional skills.First of all, noble professional ethics is the premise of being a qualified general practitioner and the soul of this profession. As a code of conduct, professional ethics are formed in the long-term medical practice of medical staff. It is the moral concept and moral behavior that every medical staff should have. Especially for general practitioners with strong service, it highlights the importance of their professional ethics. The biggest difference between general practitioners and specialists is that specialists manage diseases, while general practitioners manage people, and people-centered is the core concept of their practice. General practitioners mainly take the family as the unit, take the maintenance and promotion of overall health as the direction, and participate in the long-term physical and psychological life cycle responsible care process of individuals from birth to death. In this process, they play a variety of roles, such as educators, consultants, and health guardians. They are medical talents with a high degree of integration. It can be seen that it is extremely important to maintain long-term and effective communication with patients and always understand their needs, which puts forward higher requirements for the internal cultivation and noble professional ethics of general practitioners [41]. From the personal perspective of general practitioners, the reality of lower income and fewer promotion opportunities require them to have the noble character of weak fame and wealth, maintain inner peace for the complex nature of work, and have firm faith in the face of difficulties. Only general practitioners with these noble characteristics can contribute to their work. The formation of high professional ethics quality of general practitioners is a process of continuous accumulation and perception. It is a very key psychological dimension of professional quality. When general practitioners work and live in a high-intensity and stressful environment for a long time, they are prone to form negative emotions, such as anxiety and depression, and their mental health status will change to varying degrees. Especially in the recent outbreak of the new coronavirus epidemic, the general practitioner’s psychological endurance capacity has put forward higher requirements. It requires not only the general practitioner’s psychological state of self-sacrifice and firm belief, but also the need to consider the patient’s mood, communicate effectively and understand the importance of empathy.Secondly, in addition to mastering basic professional knowledge, such as internal medicine, surgery, gynecology, and pediatrics, general practitioners should also understand and learn other theoretical knowledge, such as psychology and interpersonal science, because the main feature of general practice is to serve patients with an overall medical view and a systematic way of thinking. For example, general practitioners should not only pay attention to the patient’s disease, but also observe the changes in the patient’s mood and the factors that may lead to the disease, such as the surrounding environment; they should even predict the possible diseases in the future according to the current patient’s physical condition—all of this to prevent the occurrence of diseases, prevent or shorten the time of future diseases in advance, or transfer patients in time according to the patient’s physical condition, and share the pressure of medical treatment for large hospitals [42,43]. This requires general practitioners to have a comprehensive reserve of theoretical knowledge in order to improve the accuracy of judging diseases and reduce the risk of miscalculation. In the process of growing up, general practitioners should also pay attention to their in-depth research on a certain aspect of professional knowledge. In this way, while training general practitioners to have the overall concept, they will also establish unique thinking required for hard research.Finally, the professional skills of general practitioners are not only the core component of professional quality, but also the embodiment of the practical workability of general practitioners. The professional skill quality of general practitioners mainly includes door-to-door service and outpatient service. In recent years, the state has gradually attached importance to door-to-door service, mainly because the aging population has led to the gradual increase of disabled, elderly people in China. In order to meet the medical needs of these patients, higher requirements are put forward for general practitioners’ health management skills, rehabilitation training skills, and disease prevention skills [44]. At present, there are many elderly people in community clinics. Chronic diseases (such as diabetes, hypertension, and heart disease) are very common diseases in the elderly. Therefore, general practitioners should have the ability to manage chronic diseases and control the development of patients’ diseases as much as possible. The other group is the residents near the community. Generally, people with common diseases (such as colds, headaches, etc.) will choose the community hospital close to home for treatment, which requires the general practitioner to have the ability to deal with common diseases. In addition, some patients suffer from frequently occurring diseases all year round (such as neck, shoulder, waist, and leg pain, endocrine disorders, etc.), and will also choose a more convenient community hospital to regulate their bodies. Therefore, general practitioners should have the ability to control the frequently occurring diseases of patients.
- (2)
- The internal relationship model among general practitioners’ professional quality, training, and service value is established.Specifically, professional ethics, theoretical knowledge, and professional skills, as the dimensions of general practitioners’ professional quality, can be improved and improved through training, so as to further realize their technical value, environmental value, and information value. At present, the most important way to improve doctors’ professional quality and skills is to improve doctors’ theoretical and practical skills through training; therefore, the state should pay attention to vigorously carrying out the standardized training of general practitioners and strengthening the construction of grassroots health personnel.Training mainly includes standardized training, job transfer training, and continuing education. The standardized training is aimed at medical students. The training focuses on basic theories, clinical skills, and basic medical and health practice. Through training, most of the trainees reported that their professional knowledge level and skills, teamwork, and learning ability had been significantly improved, further promoting the realization of the technical value of general practitioners. The job transfer training is aimed at qualified grassroots on-the-job professional doctors or professional assistant doctors. The content of job transfer training is also carried out around the professional quality of general practitioners, mainly including knowledge, skills, and other training. The emphasis on mental health and communication skills has also increased. After the training, appropriate adjustments should be made according to the service effect. The training is gradually strengthening the application of general practice medicine and the content of knowledge and skills in the field of preventive medicine. As the types of trainees for job transfer training are complex, it is necessary to implement targeted training for trainees at different levels. Therefore, trained general practitioners are conducive to realizing their environmental value, technical value, and functional value. The improvement of general practitioners’ medical knowledge, medical experience, and ability to quickly handle emergencies is conducive to the further realization of technical value, and the improvement of family planning technical guidance, disease prevention, health care, and health management services is conducive to the further realization of functional value.The cultivation of humanistic quality needs long-term accumulation and precipitation. For general practitioners, the cultivation of humanistic quality is gradually concerned in training. Through the establishment of an assessment mechanism suitable for the innovative teaching model, more subjective training content is added, and students’ noble humanistic feelings, such as fraternity and empathy, are improved. In order to guide students to apply theory to practice, use the form of case analysis to simulate and restore the authenticity of real events, so as to constantly adjust and deepen the humanistic concept, which plays an important role in realizing good environmental values for general practitioners.
5. Conclusions
6. Theoretical Contribution and Practical Value
6.1. Theoretical Contribution
6.2. Practical Value
7. Managerial Implications
8. Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chou, S.; Cole, G.; McLaughlin, K.; Lockyer, J. CanMEDS evaluation in Canadian postgraduate training programmes: Tools used and programme director satisfaction. Med. Educ. 2008, 42, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.R.; White, J.S.; Poth, C.; Rogers, W.T. Learning the CanMEDS roles in a near-peer shadowing program: A mixed methods randomized control trial. Med. Teach. 2012, 34, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Nie, H.Y.; Zhang, D.D.; Wang, S.L.; Gang, B.U.; Cao, Y.X. Study on the problems and thoughts about general practitioner training in pain department under the background of “Healthy China 2030”. Med. Educ. Res. Pract. 2019, 27, 197–199. [Google Scholar]
- Gan, R.; Zhu, Y. Exploratory study on the consultation competence of community general practitioners in Guiyang city. Chin. Gen. Pract. 2019, 22, 3825–3829. [Google Scholar]
- Xie, B.Y.; Chen, J.; Long, J.J. Analysis of reform measures and effect of humanistic quality education in the standardized train-ing of general practitioners. China Health Ind. 2017, 14, 67–69. [Google Scholar]
- Hei, Y.H. Thoughts on the cultivation of professional quality of medical personnel. Chin. Med. Rec. 2015, 16, 48–50. [Google Scholar] [CrossRef]
- Li, X.; Krumholz, H.M.; Yip, W.; Cheng, K.K.; De Maeseneer, J.; Meng, Q.; Mossialos, E.; Li, C.; Lu, J.; Su, M.; et al. Quality of primary health care in China: Challenges and recommendations. Lancet 2020, 395, 1802–1812. [Google Scholar] [CrossRef]
- Liu, Y.; Jiang, G.; Ren, J. Current Status and Development Strategies of General Practitioner Training in China. Chin. J. Eng. Sci. 2019, 21, 74–78. [Google Scholar] [CrossRef]
- Wang, X.H.; Feng, W.; Qian, Y.; Fang, W.F.; Zheng, G.G.; Wang, H.; Li, P. Study of the formation mechanism and governance logic of the service motivation for community doctors’ first contact. Chin. J. Health Policy 2017, 10, 57–64. [Google Scholar] [CrossRef]
- Yang, H.; Han, J.J.; Xu, Y.L. The development, challenge and prospect of general practitioner team construction in China. Chin. Gen. Pract. 2019, 22, 2267–2279. [Google Scholar] [CrossRef]
- Rong, F.J. On the dual action mechanism of human capital and social capital on the career growth of university administrators. Hum. Resour. Manag. 2014, 241–244. [Google Scholar]
- Chen, X.P.; Sun, Y.M. Research and construction of professional competency model for master of engineering. Res. High. Eng. Educ. 2017, 5, 60–65. [Google Scholar]
- Zhao, S.; Hospital, F.P. Measures and achievements of standardized training of general practitioners in Chinese medicine based on competency model. Clin. Res. 2019, 27, 15–16. [Google Scholar]
- Wei, Y.; Wang, F.; Pan, Z.; Wang, M.; Jin, G.; Liu, Y.; Lu, X. Development of a competency model for general practitioners after standardized residency training in China by a modified Delphi method. BMC Fam. Pract. 2021, 22, 171. [Google Scholar] [CrossRef]
- Hu, J.H. Cultivation of professional quality of clinical pharmacists. Pharm. Care Res. 2013, 13, 161–165. [Google Scholar] [CrossRef]
- Liu, Y.J.; Liu, N.; Zhang, Q.; Wang, C.; Gu, Y.L.; Li, Z.Y. Salary incentive policy for general practitioners in Britain and its reference significance. Chin. Gen. Pract. 2018, 21, 3033–3037. [Google Scholar]
- Campion, M.A.; Fink, A.A.; Ruggeberg, B.J.; Carr, L.; Phillips, G.M.; Odman, R.B. Doing competencies well: Best practices in competency modeling. Pers. Psychol. 2011, 64, 225–262. [Google Scholar] [CrossRef]
- Meng, X.M.; Pan, X.Y. Digital learning resources and general practitioner training under network environment. Hebei Med. 2013, 19, 1277–1280. [Google Scholar] [CrossRef]
- Sun, C.; Liu, Y.L.; Lu, X.Q.; Du, J.; Liu, X.P.; Zhao, Y.L. Effects of “3+2” assistant general practitioners training program implemented in Beijing: A qualitative study. Chin. Gen. Pract. 2017, 20, 2393–2395. [Google Scholar]
- Wang, S.; Xie, X.J.; Jin, D.J.; Yu-Long, L.I.; Chen, W.M.; Wei-Hua, J.; Zhan, D.M. Analysis of teaching effect at colleges education stage of “3+2” assistant general practitioner training mode in clinical medicine. Clin. Res. Pract. 2019, 4, 192–194. [Google Scholar]
- Jiang, H.L.; Zhou, L.Q. Exploration on the cultivation of humanistic quality in the standardized training of general practitioners. China’s Health Ind. 2019, 16, 154–155. [Google Scholar] [CrossRef]
- Luo, Q. Analysis of humanistic quality education strategy in the training process of general practitioners. Theory Pract. Innov. Entrep. 2019, 2, 74–75. [Google Scholar]
- Zhao, W.; Wang, R.; Wang, Y.; Zhang, M.; Yin, T. The Necessity of Medical Humanities Education to General Practitioners: A Brief Review. Iran. J. Public Health 2020, 49, 2054–2059. [Google Scholar] [CrossRef]
- Zhao, B.J. Evaluation of community health service ability of standardized training general practitioners in Hubei Province. Chin. Community Physician 2017, 33, 163–164. [Google Scholar]
- Ye, T.F.; Pan, X.Y. Construction of evaluating index system based on the AHP on the competence of urban general practitioner in Guangxi. Chin. Gen. Pract. 2014, 17, 752–755. [Google Scholar]
- Harris, S.M.; Binder, P.-E.; Sandal, G.M. General Practitioners’ Experiences of Clinical Consultations With Refugees Suffering From Mental Health Problems. Front. Psychol. 2020, 11, 412. [Google Scholar] [CrossRef]
- Laurence, C.O.; Eley, D.S.; Walters, L.; Elliott, T.; Cloninger, C.R. Personality characteristics and attributes of international medical graduates in general practice training: Implications for supporting this valued Australian workforce. Aust. J. Rural Health 2016, 24, 333–339. [Google Scholar] [CrossRef]
- Li, W.M.; Shu, Q.Q.; Huang, Q.Y.; Jiang, Y.L.; Yuan, D.; Zhao, H.H.; Liu, J.L.; Zi, R. Study on practice registration intention and influencing factors of general practitioners in Yunnan Province. Chin. Gen. Med. 2018, 16, 863–865. [Google Scholar]
- Liu, L.x.; Liao, X.Y.; Wu, J.; Deng, L.L.; Xiong, M.; Zhuang, L.X. Research progress of general-specialty joint outpatient service. Chin. J. Hosp. Adm. 2019, 35, 915–918. [Google Scholar] [CrossRef]
- Zheng, X.L.; Liu, D.Y.; Zhao, C.M.; Jian, Y.J. Investigation and analysis on the current situation and demand of continuing medical education for general practitioners in Tianjin. Contin. Med. Educ. 2018, 32, 8–9. [Google Scholar]
- Yang, H.M.; Yin, D.L.; Xin, Q.Q.; Yin, T.; Ding, X.Y.; Wang, L.H.; Chen, B.W. Analysis on the current situation of grass-roots general practitioners and the content demand of continuing medical education in China. Chin. Gen. Med. 2018, 16, 1591–1594. [Google Scholar] [CrossRef]
- Liu, Z.R.; Li, Z.; Deng, S.G. Investigation and effect evaluation of general practitioners’ job transfer training in Ethnic Minority areas. Youjiang Med. 2019, 47, 56–59. [Google Scholar]
- Berkhof, M.; van Rijssen, J.; Schellart, A.J.; Anema, J.R.; van der Beek, A.J. Effective training strategies for teaching communication skills to physicians: An overview of systematic reviews. Patient Educ. Couns. 2011, 84, 152–162. [Google Scholar] [CrossRef]
- Clayton, J.M.; Butow, P.N.; Waters, A.; Laidsaar-Powell, R.C.; O’Brien, A.; Boyle, F.; Back, A.L.; Arnold, R.M.; A Tulsky, J.; Tattersall, M.H. Evaluation of a novel individualised communication-skills training intervention to improve doctors’ confidence and skills in end-of-life communication. Palliat. Med. 2013, 27, 236–243. [Google Scholar] [CrossRef]
- Ellis, V.; Tully, K.; Gill, N.; McLewin, A.; Clift, S. ‘Creating health’: Evaluation of three arts for health training events for GP trainees. Perspect. Public Health 2020, 141, 287–294. [Google Scholar] [CrossRef]
- Sadeh, E.; Mousavi, L.; Garkaz, M.; Sadeh, S. The structural model of e-service quality, e-customer satisfaction, trust, customer perceived value and e-loyalty. Aust. J. Basic Appl. Sci. 2011, 5, 532–538. [Google Scholar]
- Mokhtaran, M.; Fakharyan, M.; Jalilvand, M.R.; Mohebi, M. The Effect of Service Climate on Perceived Service Value and Behavioral Intentions: The Mediating Role of Service Quality. Asia Pac. J. Tour. Res. 2015, 20, 472–486. [Google Scholar] [CrossRef]
- Wang, X.Y. Construction of Community Health Service Value Evaluation Model and Empirical Study; Shanxi Medical University: Taiyuan, China, 2018. [Google Scholar]
- Wang, C.Y.; Zhao, S.M.; Qin, W.P.; Ding, M.Z. Research on the influence mechanism of college students’ entrepreneurial team cohesion based on grounded theory. Sci. Technol. Prog. Policy 2022, 39, 152–160. [Google Scholar] [CrossRef]
- Li, J.; Sun, Q.; Fu, L.P. Qualitative research on influencing factors of elderly care service in Tangshan medical and nursing institutions based on grounded theory. Med. Soc. 2022, 35, 37–42. [Google Scholar]
- Wu, Z.M.; Zhang, Q.F.; Luo, Y.; Gui, P.G. Research on humanistic quality education in the training of general practitioners. China’s Health Ind. 2018, 15, 125–126. [Google Scholar] [CrossRef]
- Li, W.M.; Yuan, D.; Zi, R.; Shu, Q.Q.; Huang, Q.Y.; Zhang, M.; Chen, Y.C.; Huang, X.L. Willingness and influencing factors of clinical medical students in Yunnan Province to participate in the training of assistant general practitioners. Chin. J. Gen. Pract. 2018, 17, 784–788. [Google Scholar] [CrossRef]
- Liu, J.Y.; Hui, J.F.; Sun, M.Y.; Liu, X.S.; Lu, W.H.; Ma, C.H.; Zhang, Q.B. Effects of phosphorus application level, inoculation of AMF and Phosphorus Solubilizing Bacteria on Alfalfa Yield and phosphorus utilization efficiency. J. Agric. Eng. 2020, 36, 142–149. [Google Scholar] [CrossRef]
- Zhang, W.; Sun, R.L. Research on the construction of evaluation index system of standardized training for general practitioners based on koch model. Chin. Gen. Pract. 2020, 23, 4371–4376. [Google Scholar]
- Pan, Y.; Yu, D.H.; Lu, Y.; Liu, X.Y.; Zhang, H.Z.; Fan, H.Q. Research on the construction of general practitioners’ comprehensive ability evaluation index system based on literature analysis. Chin. J. Gen. Pract. 2016, 19, 248–250. [Google Scholar]
- Egerer, M.; Kuth, N.; Koch, A.; Schmitz, S.M.-T.; Kroh, A.; Neumann, U.P.; Ulmer, T.F.; Alizai, P.H. General Practitioner’s Knowledge about Bariatric Surgery Is Associated with Referral Practice to Bariatric Surgery Centers. Int. J. Environ. Res. Public Health 2021, 18, 10055. [Google Scholar] [CrossRef] [PubMed]
- McGrail, M.R.; O’Sullivan, B.G. Faculties to Support General Practitioners Working Rurally at Broader Scope: A National Cross-Sectional Study of Their Value. Int. J. Environ. Res. Public Health 2020, 17, 4652. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No | Main Category | Concept |
|---|---|---|
| 1 | Door-to-door service | Generally speaking, the interviewees said: Door-to-door service should have three aspects of skills and qualities: First, health management skills, including basic medical service capabilities such as blood pressure measurement, blood sugar measurement, and dressing change. The second is the rehabilitation training skills, the functional guidance to help disabled elderly, and the management of the condition of long-term bedridden patients. The third is disease prevention skills. Through long-term observation of the patient’s physical state and emotional changes, once an abnormal situation is found, the ability to guide the patient to accurately seek medical treatment in a timely manner. |
| 2 | Outpatient clinic | Disease types include: First, the ability to manage chronic diseases such as diabetes, hypertension, and heart disease. The second is the ability to control frequently occurring diseases such as neck, shoulder, waist, and leg pain and endocrine disorders. The third is the ability to deal with common diseases such as colds, fever, and gastritis. |
| 3 | Books | Generally, interviewees will choose to read books on basic medicine, such as general practitioner manuals, general medicine introductions, and also read books on psychology and doctor–patient communication to enrich their theoretical knowledge. |
| 4 | Internet | Download online resources such as Good Doctors.com and Dingxiang.com through the mobile APP to learn theoretical knowledge and broaden the ways of acquiring knowledge. |
| 5 | Treatment patients | The moral qualities that doctors need to treat patients: sincere attitude (2) *, good at communication (8), patient explanation (11), and empathy (3). |
| 6 | Doctors themselves | The doctor’s moral cultivation: indifferent to fame and fortune (1), inner peace (4), self-sacrifice (1), firm belief (2). |
| 7 | Regulation training | The regulation training time is three years, and content includes internal, external, women, children, health care, etc. During the study period, each department rotates to cultivate operational skills. |
| 8 | Continuous education | Participate in continuing education in the form of lectures and conferences every year. |
| 9 | Transfer of training | Learn theoretical knowledge in the form of class; you can choose a few basic courses, and rotate in the selected department about once every three months. |
| 10 | National mandatory training assessment | It is stipulated that the required credits can be completed before the assessment can be completed. |
| 11 | Autonomous training and assessment of community hospitals | Community hospitals regularly organize general practitioners to study or participate in lectures in major hospitals, and experts from major hospitals also regularly attend classes in community hospitals, forming an interactive training model. |
| 12 | Moral quality | General interviewees said: The professional ethics during the training period mainly involves communication skills, attitudes, people-oriented, belief-building, and other ideological content. |
| 13 | Theoretical knowledge | During the training, the professional knowledge learning mainly focuses on basic medical theory learning and the explanation of the latest development of chronic diseases in the community (such as diabetes, hypertension, etc.). |
| 14 | Practical skills | Skills and operation training mainly focuses on the mastery of basic operation skills and new technologies. The center is about lung rejuvenation, cardiovascular and cerebrovascular, and other first-aid operations. |
| 15 | Humanistic environment | The personal impact of the training on the general practitioner: The training is a summary explanation, with a deep memory point. In the work, I will often remind myself of the attitude and tone of communication with the patient to reduce misunderstandings and contradictions. |
| 16 | Skill levels | The personal impact of training on general practitioners: First, the knowledge level has enriched theoretical literacy and improved understanding of diseases. The second is the skill level, with a good understanding of new skills, especially in emergency training such as cardiopulmonary resuscitation. The improvement of doctors’ personal operating ability is beneficial to accurately determine the patient’s disease and provide effective treatment. |
| 17 | Patient satisfaction | Training effect: Increasing patients’ trust and recognition of general practitioners. Most interviewees said that they have fixed “fans” and come to see doctors regularly. As the quality of general practitioners in community hospitals has been improved through training, the number of outpatient clinics has shown an increasing trend year by year. |
| 18 | Residents’ medical awareness | Training effect: General practitioners have improved their own quality through training, mastered new knowledge and skills, and increased their awareness of general medical care in the process of communicating with patients. |
| No | Main Category | Concept |
|---|---|---|
| 1 | Professional ethics quality | It summarizes the professional ethics quality of general practitioners from two aspects: treating patients and doctors themselves. |
| 2 | Theoretical knowledge | Theoretical knowledge is a necessary professional quality for general practitioners, and books and the Internet are important ways for them to obtain basic content. |
| 3 | Professional skills quality | The form of outpatient service requires general practitioners to have the ability to manage chronic diseases, control frequently occurring diseases, and handle common diseases. The form of door-to-door service requires general practitioners to have health management skills, rehabilitation training skills, and disease prevention skills. |
| 4 | Training form | The training forms mainly include regular training, continuing education, and transfer training. |
| 5 | Evaluate training | The assessment units are national training assessment and community hospital independent training assessment |
| 6 | Training content | The training content is related to the professional quality of general practitioners, including three aspects: ethics, theoretical knowledge, and skills. |
| 7 | Technical value | The training enriches the theoretical knowledge of general practitioners and effectively improves their practical skills, especially the improvement of operating skills for handling emergencies. At the same time, the increase in patient satisfaction has prompted a continuous increase in the number of outpatient services. |
| 8 | Environmental value | Through the humanistic qualities formed by the exchanges and communication between doctors and patients after training, a good environmental atmosphere is created for community residents. |
| 9 | Information value | In the training process, general practitioners accept advanced knowledge and can provide general medical service information and medical progress in time, so that they can effectively answer questions raised by residents. |
| No | Relationship Category | Concept of Influence Relationship (Corresponding Code) | Relationship Connotation |
|---|---|---|---|
| 1 | Professional quality | Professional ethics quality: Doctors themselves ① indifferent to fame and fortune (1-3-1) ② inner peace (1-3-2, 10-3-2, 4-3-2, 24-3-2) ③ self-sacrificing (1-3-4) ④ strong faith (24-3-1, 22-3-1); Treat patients ① sincere attitude (3-3-1, 6-3-2) ② good at communication (1-3-4, 2-3-2, 6-3-3, 11-3-1, 16-3-1, 18-3-2, 22-3-2, 33-3-2) ③ explain patiently (1-3-3, 5-3-3, 10-3-1, 12-3-4, 13-3-3, 23-3-1, 24-3-3, 28-3-2, 32-3-1, 35-3-5, 36-3-2) ④ empathy (2-3-1, 3-3-2, 28-3-1) | The most fundamental thing for a doctor is to have a heart of “the benevolent loves others”, and a good professional ethics is the inner soul of the spiritual level of a doctor. From the doctor’s point of view, indifference to fame and fortune, inner peace, self-sacrifice, and firm conviction are the basic characteristics of personal charm. A sincere attitude, good communication, patient explanation, and empathy are the good moral qualities that general practitioners need to have when facing patients. In addition to internal literacy, general practitioners also need to have profound theoretical knowledge, professional skills, and other external qualities. |
| Theoretical knowledge: books (5-4-2, 20-4-2, 26-4-4, 35-4-4); network (8-4-3, 26-4-5, 4-4-3, 35-4-2, 31-4-3) | |||
| Professional skill quality: Outpatient ① chronic disease management ability (1-1-1, 8-1-1, 10-1-1, 12-1-1, 13-1-1, 22-1-1, 23-1-1, 24-1-1, 26-1-1, 28-1-1, 33-1-1, 34-1-1, 35-1-1) ② common disease treatment ability (2-1-1, 3-1-1, 5-1-1, 6-1-1, 11-1-1, 16-1-1, 18-1-1, 24-1-1, 26-1-1, 31-1-1, 32-1-1, 35-1-1, 36-1-1) ③ ability to control frequently occurring diseases (4-1-1); Door-to-door service ① health management skills (2-1-2, 5-1-2, 12-1-4, 23-1-2, 28-1-2, 31-1-2, 32-1-2, 36-1-2) ② rehabilitation training skills (1-1-3, 4-1-2, 11-1-2, 28-1-2) ③ disease prevention skills (28-1-2) | |||
| 2 | Training | Training form: regular training (8-4-3, 10-4-1, 12-4-1, 36-4-2); continuing education (6-4-2, 12-4-4, 16-4-2, 24-4-1, 32-4-1, 33-4-2); transfer training (13-4-1, 18-4-1, 33-4-1) | The professional quality of general practitioners determines the trust and satisfaction of patients. Training is an effective way to improve one’s own professional quality, mainly involving three aspects of training form, assessment, and content. The main forms of training are planned training, continuing education, and transfer training. The assessment is organized by both the state and community hospitals. The training content is mainly set according to the basic quality of general practitioners. |
| Training assessment: National regulations (1-4-4, 4-4-1, 5-4-1, 8-4-1); community hospital autonomy (1-4-5, 4-4-2, 5-4-3, 10-4-2, 11-4-2, 16-4-4, 22-4-2, 34-4-2) | |||
| Training content: moral quality (1-4-2, 2-4-2, 5-4-4, 26-4-3, 28-4-2, 31-4-1, 35-4-5, 36-4-3); theoretical knowledge (13-4-5, 23-4-2, 26-4-2, 32-4-2, 34-4-3); skills (1-4-3, 2-4-1, 8-4-2, 10-4-3, 11-4-1, 26-4-1, 28-4-1, 35-4-3) | |||
| 3 | Service value | Technical value: skill level (11-5-3, 13-5-3, 16-5-1, 26-5-1, 35-5-1, 34-5-2, 32-5-1, 31- 5-1, 2-5-1, 3-5-1, 6-5-1, 10-5-1, 11-5-1, 24-5-1, 34-5-1, 31-5-2, 6-5-2); patient satisfaction (11-6-4, 12-6-2, 24-6-3, 26-6-3, 2-6-1, 3-6-1, 22 -6-1, 28-6-2, 31-6-3, 36-6-2) | Through training, the technical value, environmental value, and information value of general practitioners have been realized. The realization of technical value is due to the improvement of skill level, which increases patient satisfaction. The realization of environmental value is the promotion of moral quality, which has shaped a good humanistic environment. The realization of the value of information is the acceptance and learning of new knowledge and advanced technology in the training process, which has a certain positive effect on the improvement of residents’ medical awareness. |
| Environmental value: humanistic environment atmosphere (2-5-2, 11-5-2, 35-5-3, 36-5-1) | |||
| Information value: residents’ medical awareness (1-6-1, 10-6-2, 13-6-1, 33-6-1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ge, B.; Ma, Z.; Li, M.; Chi, X.; Khan, H.S.u.d.; Yang, L. Exploring the Nexus of Healthcare Employees’ Professional Quality, Health Psychology and Service Value: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 12462. https://doi.org/10.3390/ijerph191912462
Ge B, Ma Z, Li M, Chi X, Khan HSud, Yang L. Exploring the Nexus of Healthcare Employees’ Professional Quality, Health Psychology and Service Value: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12462. https://doi.org/10.3390/ijerph191912462
Chicago/Turabian StyleGe, Bailin, Zhiqiang Ma, Mingxing Li, Xiaomeng Chi, Hira Salah ud din Khan, and Ling Yang. 2022. "Exploring the Nexus of Healthcare Employees’ Professional Quality, Health Psychology and Service Value: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 19: 12462. https://doi.org/10.3390/ijerph191912462
APA StyleGe, B., Ma, Z., Li, M., Chi, X., Khan, H. S. u. d., & Yang, L. (2022). Exploring the Nexus of Healthcare Employees’ Professional Quality, Health Psychology and Service Value: A Qualitative Study. International Journal of Environmental Research and Public Health, 19(19), 12462. https://doi.org/10.3390/ijerph191912462