
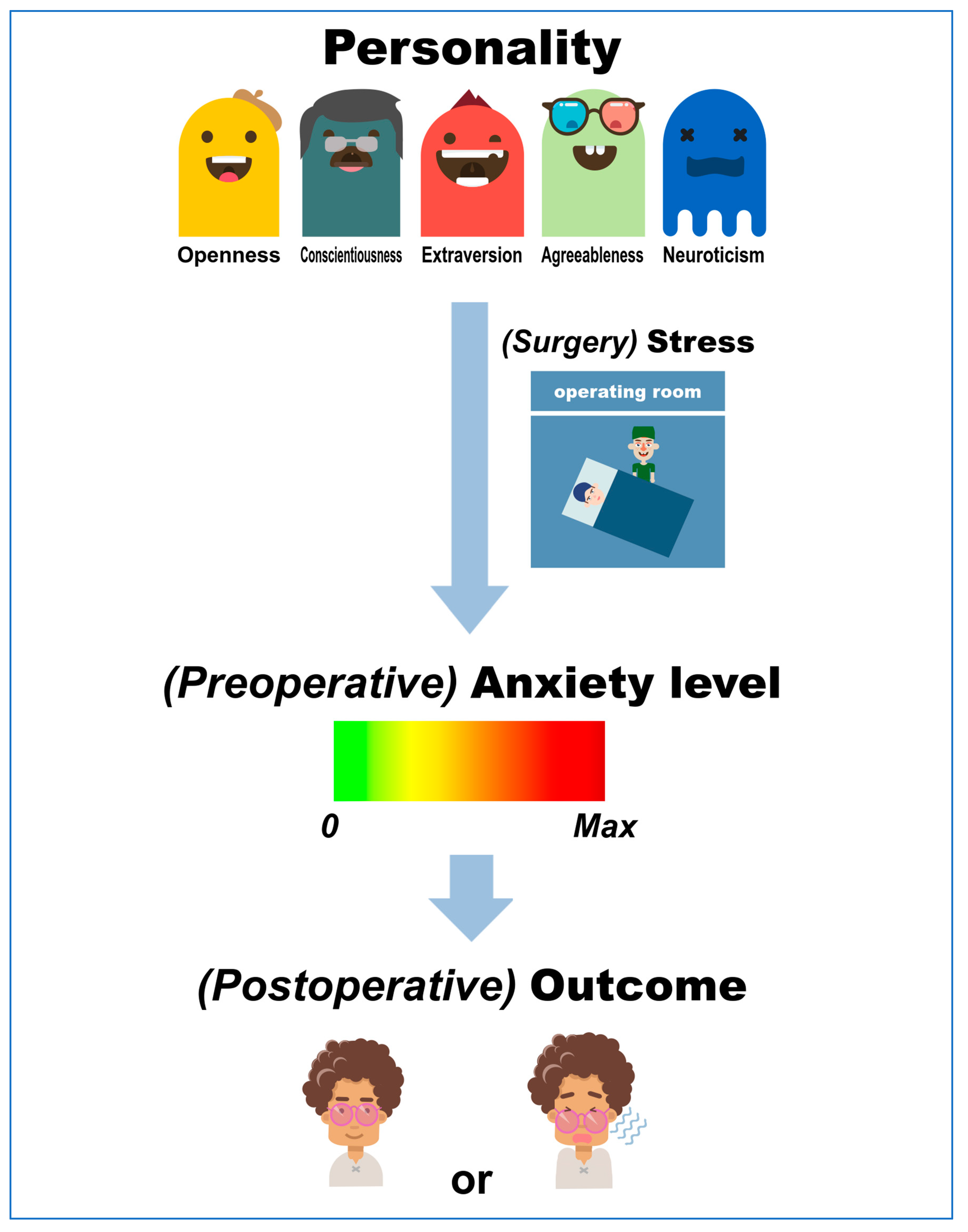
Personality, Preoperative Anxiety, and Postoperative Outcomes: A Review



{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
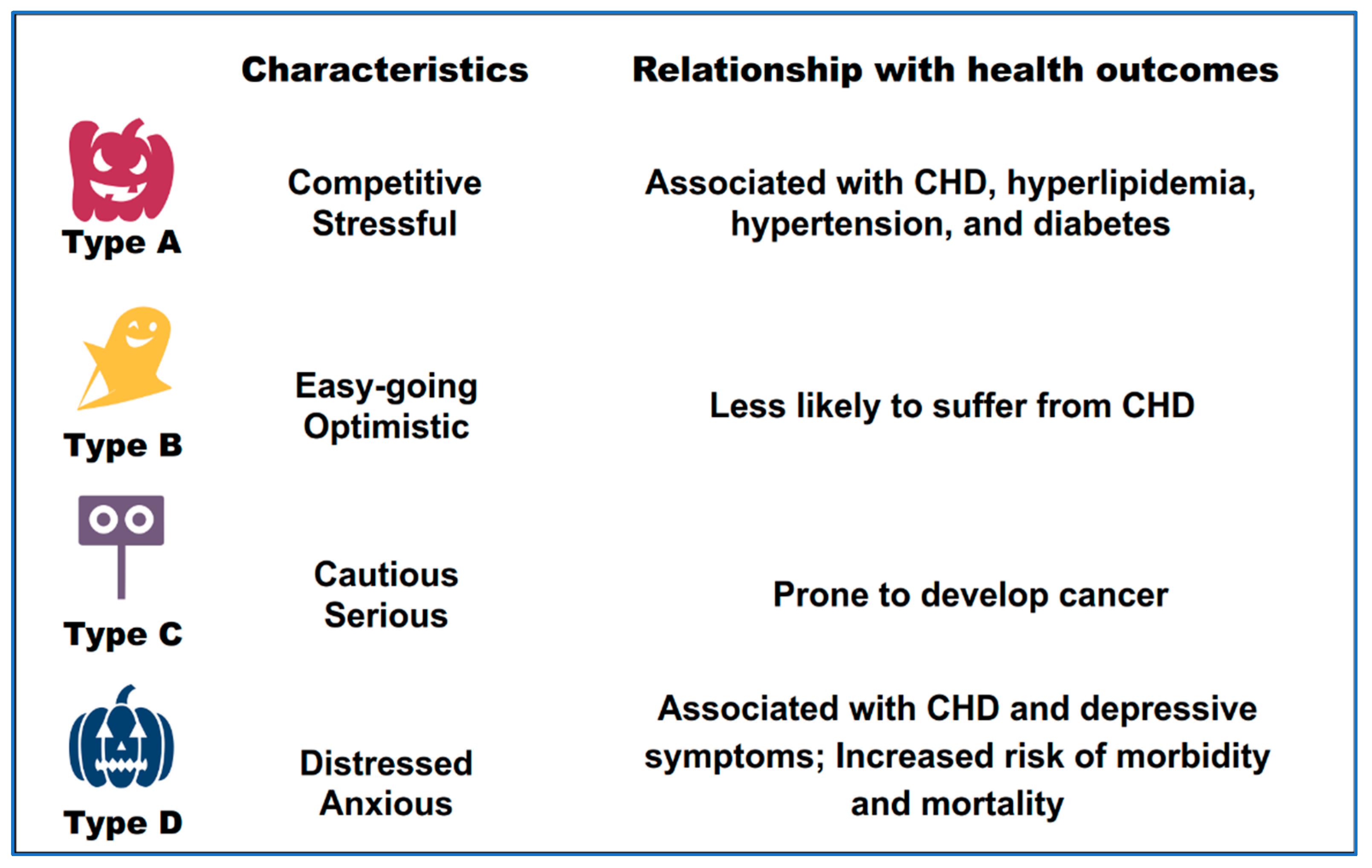
3. Personality, Health, and Patient Outcomes
4. Personality and Preoperative Anxiety
5. Preoperative Anxiety and Postoperative Outcomes
5.1. Epidemiology of Preoperative Anxiety
5.2. The Influence of Preoperative Anxiety on Postoperative Outcomes
5.3. Strategies to Mitigate Preoperative Anxiety and Improve Postoperative Outcomes
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldberg, L.R.; Kilkowski, J.M. The prediction of semantic consistency in self-descriptions: Characteristics of persons and of terms that affect the consistency of responses to synonym and antonym pairs. J. Personal. Soc. Psychol. 1985, 48, 82–98. [Google Scholar] [CrossRef]
- Buss, A.H.J.A.P. Personality as traits. Am. Psychol. 1989, 44, 1378–1388. [Google Scholar] [CrossRef]
- Pervin, L.A. A Critical Analysis of Current Trait Theory. Psychol. Inq. 1994, 5, 103–113. [Google Scholar] [CrossRef]
- Grillon, C. Models and mechanisms of anxiety: Evidence from startle studies. Psychopharmacology 2008, 199, 421–437. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Belfiore, M.P.; Urraro, F.; Grassi, R.; Giacobbe, G.; Patelli, G.; Cappabianca, S.; Reginelli, A. Artificial intelligence to codify lung CT in COVID-19 patients. La Radiol. Med. 2020, 125, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Vagg, P.R. Test Anxiety: Theory, Assessment, and Treatment; Taylor & Francis: Abingdon, UK, 1995. [Google Scholar]
- Kil, H.K.; Kim, W.O.; Chung, W.Y.; Kim, G.H.; Seo, H.; Hong, J.Y. Preoperative anxiety and pain sensitivity are independent predictors of propofol and sevoflurane requirements in general anaesthesia. Br. J. Anaesth. 2012, 108, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.-S.; Byeon, G.-J.; Song, B.-J.; Lee, H.J. Availability of preoperative anxiety scale as a predictive factor for hemodynamic changes during induction of anesthesia. Korean J. Anesthesiol. 2010, 58, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Kassahun, W.T.; Mehdorn, M.; Wagner, T.C.; Babel, J.; Danker, H.; Gockel, I. The effect of preoperative patient-reported anxiety on morbidity and mortality outcomes in patients undergoing major general surgery. Sci. Rep. 2022, 12, 6312. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, A. Personality traits, patient-centered health status and prognosis of brain tumor patients. J. Neuro-Oncol. 2018, 137, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Matsuishi, Y.; Shimojo, N.; Unoki, T.; Sakuramoto, H.; Tokunaga, C.; Yoshino, Y.; Hoshino, H.; Ouchi, A.; Kawano, S.; Sakamoto, H.; et al. Type D personality is a predictor of prolonged acute brain dysfunction (delirium/coma) after cardiovascular surgery. BMC Psychol. 2019, 7, 27. [Google Scholar] [CrossRef]
- Srivastava, K.; Das, R.C. Personality and health: Road to well-being. Ind. Psychiatry J. 2015, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ray, J.J.; Bozek, R. Dissecting the A-B personality type. Br. J. Med. Psychol. 1980, 53, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, A.A.; Pedersen, S.S.; Widdershoven, J.W.; Hendriks, E.H.; Winter, J.B.; Denollet, J. The distressed (type D) personality is independently associated with impaired health status and increased depressive symptoms in chronic heart failure. Eur. J. Cardiovasc. Prev. Rehabil. Off. J. Eur. Soc. Cardiol. Work. Groups Epidemiol. Prev. Card. Rehabil. Exerc. Physiol. 2005, 12, 341–346. [Google Scholar] [CrossRef]
- Eysenck, H.J. Cancer, personality and stress: Prediction and prevention. Adv. Behav. Res. Ther. 1994, 16, 167–215. [Google Scholar] [CrossRef]
- Ross, G.F. Work stress and personality measures among hospitality industry employees. Int. J. Contemp. Hosp. Manag. 1995, 7, 9–13. [Google Scholar] [CrossRef]
- John, O.P.; Srivastava, S. The Big Five Trait taxonomy: History, measurement, and theoretical perspectives. In Handbook of Personality: Theory and Research, 2nd ed.; Guilford Press: New York, NY, USA, 1999; pp. 102–138. [Google Scholar]
- Schmitt, D.P.; Allik, J.; McCrae, R.R.; Benet-Martínez, V. The Geographic Distribution of Big Five Personality Traits:Patterns and Profiles of Human Self-Description across 56 Nations. J. Cross-Cult. Psychol. 2007, 38, 173–212. [Google Scholar] [CrossRef]
- Ferguson, E.; Bibby, P.A. Openness to experience and all-cause mortality: A meta-analysis and r(equivalent) from risk ratios and odds ratios. Br. J. Health Psychol. 2012, 17, 85–102. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Dong, J.Y. Patient’s personality predicts recovery after total knee arthroplasty: A retrospective study. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2014, 19, 263–269. [Google Scholar] [CrossRef]
- Chen, C.; Shi, Y.Y.; An, X.; Gong, L.; Tan, M.S.; Fang, Z.Y. Personality Traits Affect the Cost-Effectiveness of Total Knee Arthroplasty. Orthop. Surg. 2021, 13, 1026–1035. [Google Scholar] [CrossRef]
- Bozo, Ö.; Tathan, E.; Yılmaz, T. Does Perceived Social Support Buffer the Negative Effects of Type C Personality on Quality of Life of Breast Cancer Patients? Soc. Indic. Res. 2014, 119, 791–801. [Google Scholar] [CrossRef]
- Chida, Y.; Hamer, M.; Wardle, J.; Steptoe, A. Do stress-related psychosocial factors contribute to cancer incidence and survival? Nat. Clin. Pract. Oncol. 2008, 5, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Dahl, A.A. Link between personality and cancer. Future Oncol. 2010, 6, 691–707. [Google Scholar] [CrossRef]
- Morag, M.; Morag, A.; Reichenberg, A.; Lerer, B.; Yirmiya, R. Psychological variables as predictors of rubella antibody titers and fatigue--a prospective, double blind study. J. Psychiatr. Res. 1999, 33, 389–395. [Google Scholar] [CrossRef]
- Grande, G.; Romppel, M.; Barth, J. Association between type D personality and prognosis in patients with cardiovascular diseases: A systematic review and meta-analysis. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2012, 43, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [PubMed]
- Denollet, J.; Sys, S.U.; Stroobant, N.; Rombouts, H.; Gillebert, T.C.; Brutsaert, D.L. Personality as independent predictor of long-term mortality in patients with coronary heart disease. Lancet 1996, 347, 417–421. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D. Temperament: A new paradigm for trait psychology. In Handbook of Personality: Theory and Research, 2nd ed.; Guilford Press: New York, NY, USA, 1999; pp. 399–423. [Google Scholar]
- Maher, B.A.; Maher, W.B. Personality and psychopathology: A historical perspective. J. Abnorm. Psychol. 1994, 103, 72–77. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D. Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. J. Abnorm. Psychol. 1991, 100, 316–336. [Google Scholar] [CrossRef]
- Watson, D.B.; Wiese, D.; Vaidya, J.G.; Tellegen, A.J.J. The two general activation systems of affect: Structural findings, evolutionary considerations, and psychobiological evidence. J. Personal. Soc. Psychol. 1999, 76, 820–838. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D.; Mineka, S. Temperament, personality, and the mood and anxiety disorders. J. Abnorm. Psychol. 1994, 103, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Kotov, R.; Watson, D.; Robles, J.P.; Schmidt, N.B. Personality traits and anxiety symptoms: The multilevel trait predictor model. Behav. Res. Ther. 2007, 45, 1485–1503. [Google Scholar] [CrossRef]
- Brandes, M.; Bienvenu, O.J. Personality and anxiety disorders. Curr. Psychiatry Rep. 2006, 8, 263–269. [Google Scholar] [CrossRef]
- İzci, F.; Sarsanov, D.; Erdogan, Z.; İlgün, A.S.; Çelebi, E.; Alço, G.; Kocaman, N.; Ordu, Ç.; Öztürk, A.; Duymaz, T.; et al. Impact of Personality Traits, Anxiety, Depression and Hopelessness Levels on Quality of Life in the Patients with Breast Cancer. Eur. J. Breast Health 2018, 14, 105–111. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Arlington, V.A., Ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Katsohiraki, M.; Poulopoulou, S.; Fyrfiris, N.; Koutelekos, I.; Tsiotinou, P.; Adam, O.; Vasilopoulou, E.; Kapritsou, M. Evaluating Preoperative Anxiety Levels in Patients Undergoing Breast Cancer Surgery. Asia-Pac. J. Oncol. Nurs. 2020, 7, 361–364. [Google Scholar] [CrossRef]
- Kotov, R.; Gamez, W.; Schmidt, F.; Watson, D. Linking “big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychol. Bull. 2010, 136, 768–821. [Google Scholar] [CrossRef]
- Bienvenu, O.J.; Stein, M.B. Personality and anxiety disorders: A review. J. Personal. Disord. 2003, 17, 139–151. [Google Scholar] [CrossRef]
- Krueger, R.F. Personality traits in late adolescence predict mental disorders in early adulthood: A prospective-epidemiological study. J. Personal. 1999, 67, 39–65. [Google Scholar] [CrossRef]
- Rettew, D.C.; Vink, J.M.; Willemsen, G.; Doyle, A.; Hudziak, J.J.; Boomsma, D.I. The genetic architecture of neuroticism in 3301 Dutch adolescent twins as a function of age and sex: A study from the Dutch twin register. Twin Res. Hum. Genet. Off. J. Int. Soc. Twin Stud. 2006, 9, 24–29. [Google Scholar] [CrossRef][Green Version]
- Jardine, R.; Martin, N.G.; Henderson, A.S. Genetic covariation between neuroticism and the symptoms of anxiety and depression. Genet. Epidemiol. 1984, 1, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Hettema, J.M.; Prescott, C.A.; Kendler, K.S. Genetic and environmental sources of covariation between generalized anxiety disorder and neuroticism. Am. J. Psychiatry 2004, 161, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Samuels, J.; Nestadt, G.; Bienvenu, O.J.; Costa, P.T., Jr.; Riddle, M.A.; Liang, K.Y.; Hoehn-Saric, R.; Grados, M.A.; Cullen, B.A. Personality disorders and normal personality dimensions in obsessive-compulsive disorder. Br. J. Psychiatry J. Ment. Sci. 2000, 177, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Chartier, M.J.; Lizak, M.V.; Jang, K.L. Familial aggregation of anxiety-related quantitative traits in generalized social phobia: Clues to understanding “disorder” heritability? Am. J. Med. Genet. 2001, 105, 79–83. [Google Scholar] [CrossRef]
- Jiang, N.; Sato, T.; Hara, T.; Takedomi, Y.; Ozaki, I.; Yamada, S. Correlations between trait anxiety, personality and fatigue: Study based on the Temperament and Character Inventory. J. Psychosom. Res. 2003, 55, 493–500. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Schmid-Büchi, S.; Halfens, R.J.; Dassen, T.; van den Borne, B. A review of psychosocial needs of breast-cancer patients and their relatives. J. Clin. Nurs. 2008, 17, 2895–2909. [Google Scholar] [CrossRef]
- Ganz, P.A. Psychological and social aspects of breast cancer. Oncology 2008, 22, 642–646, 650; discussion 650, 653. [Google Scholar]
- Steel, P.; Schmidt, J.; Shultz, J. Refining the relationship between personality and subjective well-being. Psychol. Bull. 2008, 134, 138–161. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E.; Fujita, F. Extraversion and happiness. Personal. Individ. Differ. 1990, 11, 1299–1306. [Google Scholar] [CrossRef]
- Middeldorp, C.; Cath, D.; Berg, M.; Beem, A.; van Dyck, R.; Boomsma, D. The association of personality with anxious and depressive psychopathology. Biol. Pers. Indiv. Diff. 2006, 12, 251–272. [Google Scholar]
- Widiger, T.A.; Oltmanns, J.R. Neuroticism is a fundamental domain of personality with enormous public health implications. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2017, 16, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Lahey, B.B. Public health significance of neuroticism. Am. Psychol. 2009, 64, 241–256. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Jacobson, K.C.; Gardner, C.O.; Prescott, C.A.; Kendler, K.S. Personality and comorbidity of common psychiatric disorders. Br. J. Psychiatry J. Ment. Sci. 2005, 186, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Eysenck, S.B.; Eysenck, H.J. An improved short questionnaire for the measurement of extraversion and neuroticism. Life Sci. 1964, 3, 1103–1109. [Google Scholar] [CrossRef]
- Schneider, T.; Jackson, S. Extraversion and Stress; Nova Science Publishers: New York, NY, USA, 2014. [Google Scholar]
- Rosenman, R.H.; Brand, R.J.; Sholtz, R.I.; Friedman, M. Multivariate prediction of coronary heart disease during 8.5 year follow-up in the Western Collaborative Group Study. Am. J. Cardiol. 1976, 37, 903–910. [Google Scholar] [CrossRef]
- Taylor-Loughran, A.E.; O’Brien, M.E.; LaChapelle, R.; Rangel, S. Defining characteristics of the nursing diagnoses Fear and Anxiety: A validation study. Appl. Nurs. Res. 1989, 2, 178–186. [Google Scholar] [CrossRef]
- Mitchell, M. Patient anxiety and conscious surgery. J. Perioper. Pract. 2009, 19, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Van den Bosch, J.E.; Moons, K.G.; Bonsel, G.J.; Kalkman, C.J. Does measurement of preoperative anxiety have added value for predicting postoperative nausea and vomiting? Anesth. Analg. 2005, 100, 1525–1532. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Ando, T.; Umemoto, T. Perioperative depression or anxiety and postoperative mortality in cardiac surgery: A systematic review and meta-analysis. Heart Vessel. 2017, 32, 1458–1468. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.S. Anxiety, signal anxiety, and unconscious anticipation: Neuroscientific evidence for an unconscious signal function in humans. J. Am. Psychoanal. Assoc. 1999, 47, 817–841. [Google Scholar] [CrossRef]
- Ali, A.; Altun, D.; Oguz, B.H.; Ilhan, M.; Demircan, F.; Koltka, K. The effect of preoperative anxiety on postoperative analgesia and anesthesia recovery in patients undergoing laparascopic cholecystectomy. J. Anesth. 2014, 28, 222–227. [Google Scholar] [CrossRef]
- Norris, W.; Baird, W.L. Pre-operative anxiety: A study of the incidence and aetiology. Br. J. Anaesth. 1967, 39, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, M.J. Identifying and assessing anxiety in pre-operative patients. Nurs. Stand. (R. Coll. Nurs. (Great Br.) 1987) 2009, 23, 35–40. [Google Scholar] [CrossRef]
- Almalki, M.S.; Hakami, O.A.O.; Al-Amri, A.M. Assessment of Preoperative Anxiety among Patients Undergoing Elective Surgery. Egypt. J. Hosp. Med. 2017, 69, 2329–2333. [Google Scholar] [CrossRef]
- Ramsay, M.A. A survey of pre-operative fear. Anaesthesia 1972, 27, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Abate, S.M.; Chekol, Y.A.; Basu, B. Global prevalence and determinants of preoperative anxiety among surgical patients: A systematic review and meta-analysis. Int. J. Surg. Open 2020, 25, 6–16. [Google Scholar] [CrossRef]
- Maheshwari, D.; Ismail, S. Preoperative anxiety in patients selecting either general or regional anesthesia for elective cesarean section. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Hellstadius, Y.; Lagergren, J.; Zylstra, J.; Gossage, J.; Davies, A.; Hultman, C.M.; Lagergren, P.; Wikman, A. Prevalence and predictors of anxiety and depression among esophageal cancer patients prior to surgery. Dis. Esophagus 2017, 30, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Prado-Olivares, J.; Chover-Sierra, E. Preoperatory Anxiety in Patients Undergoing Cardiac Surgery. Diseases 2019, 7, 46. [Google Scholar] [CrossRef]
- Shafer, A.; Fish, M.P.; Gregg, K.M.; Seavello, J.; Kosek, P. Preoperative anxiety and fear: A comparison of assessments by patients and anesthesia and surgery residents. Anesth. Analg. 1996, 83, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Mavridou, P.; Dimitriou, V.; Manataki, A.; Arnaoutoglou, E.; Papadopoulos, G. Patient’s anxiety and fear of anesthesia: Effect of gender, age, education, and previous experience of anesthesia. A survey of 400 patients. J. Anesth. 2013, 27, 104–108. [Google Scholar] [CrossRef]
- Forlani, M.; Morri, M.; Belvederi Murri, M.; Bernabei, V.; Moretti, F.; Attili, T.; Biondini, A.; De Ronchi, D.; Atti, A.R. Anxiety symptoms in 74+ community-dwelling elderly: Associations with physical morbidity, depression and alcohol consumption. PLoS ONE 2014, 9, e89859. [Google Scholar] [CrossRef] [PubMed]
- Domar, A.D.; Everett, L.L.; Keller, M.G. Preoperative anxiety: Is it a predictable entity? Anesth. Analg. 1989, 69, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Perks, A.; Chakravarti, S.; Manninen, P. Preoperative anxiety in neurosurgical patients. J. Neurosurg. Anesthesiol. 2009, 21, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wang, H.; Zhang, L.; Wang, K.; Jiang, L.; Li, S.; Xiang, W.; Song, L.; Hu, S.; Yang, C.; et al. Clinical study of preoperative psychological distress and its related factors in the primary caregivers of patients with glioma. Clin. Neurol. Neurosurg. 2021, 200, 106364. [Google Scholar] [CrossRef]
- Li, X.R.; Zhang, W.H.; Williams, J.P.; Li, T.; Yuan, J.H.; Du, Y.; Liu, J.D.; Wu, Z.; Xiao, Z.Y.; Zhang, R.; et al. A multicenter survey of perioperative anxiety in China: Pre- and postoperative associations. J. Psychosom. Res. 2021, 147, 110528. [Google Scholar] [CrossRef] [PubMed]
- Riddle, D.L.; Wade, J.B.; Jiranek, W.A. Major depression, generalized anxiety disorder, and panic disorder in patients scheduled for knee arthroplasty. J. Arthroplast. 2010, 25, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Duivenvoorden, T.; Vissers, M.M.; Verhaar, J.A.; Busschbach, J.J.; Gosens, T.; Bloem, R.M.; Bierma-Zeinstra, S.M.; Reijman, M. Anxiety and depressive symptoms before and after total hip and knee arthroplasty: A prospective multicentre study. Osteoarthr. Cartil. 2013, 21, 1834–1840. [Google Scholar] [CrossRef] [PubMed]
- Matthias, A.T.; Samarasekera, D.N. Preoperative anxiety in surgical patients-experience of a single unit. Acta Anaesthesiol. Taiwanica 2012, 50, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Fu, P.; Yuan, S.; Zhou, Y.; Wu, Y.; Wu, H. Effects of preoperative anxiety on early postoperative pain and anesthesia recovery in total knee arthroplasty. Chin. J. Jt. Surg. (Electron. Version) 2015, 2, 165–169. [Google Scholar]
- Jawaid, M.; Mushtaq, A.; Mukhtar, S.; Khan, Z. Preoperative anxiety before elective surgery. Neurosciences 2007, 12, 145–148. [Google Scholar] [PubMed]
- Ferede, Y.A.; Bizuneh, Y.B.; Workie, M.M.; Admass, B.A. “Prevalence and associated factors of preoperative anxiety among obstetric patients who underwent cesarean section”: A cross-sectional study. Ann. Med. Surg. 2022, 74, 103272. [Google Scholar] [CrossRef]
- Boker, A.; Brownell, L.; Donen, N. The Amsterdam preoperative anxiety and information scale provides a simple and reliable measure of preoperative anxiety. Can. J. Anaesth. J. Can. D’anesthesie 2002, 49, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Haugen, A.S.; Eide, G.E.; Olsen, M.V.; Haukeland, B.; Remme, A.R.; Wahl, A.K. Anxiety in the operating theatre: A study of frequency and environmental impact in patients having local, plexus or regional anaesthesia. J. Clin. Nurs. 2009, 18, 2301–2310. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Mok, H.-P.; Zhang, H.-Y.; Qiu, H.-L.; Liu, J.; Chen, Z.-R.; Teng, Y.; Li, X.-H.; Cen, J.-Z.; Chen, J.-M.; et al. Inflammatory indicator levels in patients undergoing aortic valve replacement via median sternotomy with preoperative anxiety and postoperative complications: A prospective cohort study. J. Int. Med. Res. 2021, 49, 0300060520977417. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, S.M.H.; Janis, I.L. Psychological Stress: Psychoanalytic and Behavioral Studies of Surgical Patients; John Wiley & Sons: New York, NY, USA, 1958; p. 439. [Google Scholar]
- Grupe, D.W.; Nitschke, J.B. Uncertainty and anticipation in anxiety: An integrated neurobiological and psychological perspective. Nat. Rev. Neurosci. 2013, 14, 488–501. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Colditz, G.A.; Ascherio, A.; Rimm, E.B.; Giovannucci, E.; Stampfer, M.J.; Willett, W.C. Prospective study of phobic anxiety and risk of coronary heart disease in men. Circulation 1994, 89, 1992–1997. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.B.; Alexander, K.P.; Morin, J.F.; Langlois, Y.; Noiseux, N.; Perrault, L.P.; Smolderen, K.; Arnold, S.V.; Eisenberg, M.J.; Pilote, L.; et al. Preoperative anxiety as a predictor of mortality and major morbidity in patients aged >70 years undergoing cardiac surgery. Am. J. Cardiol. 2013, 111, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Granot, M. Can we predict persistent postoperative pain by testing preoperative experimental pain? Curr. Opin. Anaesthesiol. 2009, 22, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Nelson, F.V.; Zimmerman, L.; Barnason, S.; Nieveen, J.; Schmaderer, M. The relationship and influence of anxiety on postoperative pain in the coronary artery bypass graft patient. J. Pain Symptom Manag. 1998, 15, 102–109. [Google Scholar] [CrossRef]
- Ziętek, P.; Ziętek, J.; Szczypiór, K. Anxiety in patients undergoing fast-track knee arthroplasty in the light of recent literature. Psychiatr. Pol. 2014, 48, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Charmandari, E.; Tsigos, C.; Chrousos, G. Endocrinology of the stress response. Annu. Rev. Physiol. 2005, 67, 259–284. [Google Scholar] [CrossRef] [PubMed]
- Kiecolt-Glaser, J.K.; Page, G.G.; Marucha, P.T.; MacCallum, R.C.; Glaser, R. Psychological influences on surgical recovery. Perspectives from psychoneuroimmunology. Am. Psychol. 1998, 53, 1209–1218. [Google Scholar] [CrossRef]
- Wong, E.M.; Chan, S.W.; Chair, S.Y. Effectiveness of an educational intervention on levels of pain, anxiety and self-efficacy for patients with musculoskeletal trauma. J. Adv. Nurs. 2010, 66, 1120–1131. [Google Scholar] [CrossRef]
- Chapman, C.R. Psychological aspects of pain patient treatment. Arch. Surg. 1977, 112, 767–772. [Google Scholar] [CrossRef]
- Rhudy, J.L.; Meagher, M.W. Fear and anxiety: Divergent effects on human pain thresholds. Pain 2000, 84, 65–75. [Google Scholar] [CrossRef]
- Al Absi, M.; Rokke, P.D. Can anxiety help us tolerate pain? Pain 1991, 46, 43–51. [Google Scholar] [CrossRef]
- Cook, C.; Baxendale, S. Preoperative predictors of postoperative satisfaction with surgery. Epilepsy Behav. EB 2022, 129, 108612. [Google Scholar] [CrossRef]
- Karakoyun-Celik, O.; Gorken, I.; Sahin, S.; Orcin, E.; Alanyali, H.; Kinay, M. Depression and anxiety levels in woman under follow-up for breast cancer: Relationship to coping with cancer and quality of life. Med. Oncol. 2010, 27, 108–113. [Google Scholar] [CrossRef]
- Stirling, L.; Raab, G.; Alder, E.M.; Robertson, F. Randomized trial of essential oils to reduce perioperative patient anxiety: Feasibility study. J. Adv. Nurs. 2007, 60, 494–501. [Google Scholar] [CrossRef]
- Pinto, P.R.; McIntyre, T.; Nogueira-Silva, C.; Almeida, A.; Araújo-Soares, V. Risk factors for persistent postsurgical pain in women undergoing hysterectomy due to benign causes: A prospective predictive study. J. Pain 2012, 13, 1045–1057. [Google Scholar] [CrossRef]
- Grieve, R.J. Day surgery preoperative anxiety reduction and coping strategies. Br. J. Nurs. 2002, 11, 670–678. [Google Scholar] [CrossRef]
- Starkweather, A.R.; Witek-Janusek, L.; Nockels, R.P.; Peterson, J.; Mathews, H.L. Immune function, pain, and psychological stress in patients undergoing spinal surgery. Spine 2006, 31, E641–E647. [Google Scholar] [CrossRef]
- Ayyadhah Alanazi, A. Reducing anxiety in preoperative patients: A systematic review. Br. J. Nurs. 2014, 23, 387–393. [Google Scholar] [CrossRef]
- Phyomaung, P.P.; Dubowitz, J.; Cicuttini, F.M.; Fernando, S.; Wluka, A.E.; Raaijmaakers, P.; Wang, Y.; Urquhart, D.M. Are depression, anxiety and poor mental health risk factors for knee pain? A systematic review. BMC Musculoskelet. Disord. 2014, 15, 10. [Google Scholar] [CrossRef]
- Peacock, J.C.; Zizzi, S.J. An assessment of patient behavioral requirements pre- and post-surgery at accredited weight loss surgical centers. Obes. Surg. 2011, 21, 1950–1957. [Google Scholar] [CrossRef]
- Bailey, L. Strategies for decreasing patient anxiety in the perioperative setting. AORN J. 2010, 92, 445–457, quiz 458–460. [Google Scholar] [CrossRef]
- Jangland, E.; Gunningberg, L.; Carlsson, M. Patients’ and relatives’ complaints about encounters and communication in health care: Evidence for quality improvement. Patient Educ. Couns. 2009, 75, 199–204. [Google Scholar] [CrossRef]
- Lassen, K.; Soop, M.; Nygren, J.; Cox, P.B.; Hendry, P.O.; Spies, C.; von Meyenfeldt, M.F.; Fearon, K.C.; Revhaug, A.; Norderval, S.; et al. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch. Surg. 2009, 144, 961–969. [Google Scholar] [CrossRef]
- Mishra, P.K.; Mathias, H.; Millar, K.; Nagrajan, K.; Murday, A. A randomized controlled trial to assess the effect of audiotaped consultations on the quality of informed consent in cardiac surgery. Arch. Surg. 2010, 145, 383–388. [Google Scholar] [CrossRef]
- Guo, P. Preoperative education interventions to reduce anxiety and improve recovery among cardiac surgery patients: A review of randomised controlled trials. J. Clin. Nurs. 2015, 24, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Deyirmenjian, M.; Karam, N.; Salameh, P. Preoperative patient education for open-heart patients: A source of anxiety? Patient Educ. Couns. 2006, 62, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.J.A.; Polascik, B.A.; Kee, H.M.; Hui Lee, A.C.; Sultana, R.; Kwan, M.; Raghunathan, K.; Belden, C.M.; Sng, B.L. The Effect of Perioperative Music Listening on Patient Satisfaction, Anxiety, and Depression: A Quasiexperimental Study. Anesthesiol. Res. Pract. 2020, 2020, 3761398. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, É.V.; Haas, V.J.; de Faria, M.F.; Dos Santos Felix, M.M.; Ferreira, M.B.G.; Barichello, E.; da Silva Pires, P.; Barbosa, M.H. Effect of listening to music on anxiety, pain, and cardiorespiratory parameters in cardiac surgery: Study protocol for a randomized clinical trial. Trials 2022, 23, 278. [Google Scholar] [CrossRef]
- Muddana, S.K.; Hess, O.M.; Sundar, S.; Venkatesh, R. Preoperative and perioperative music to reduce anxiety during first-time phacoemulsification cataract surgery in the high-volume setting: Randomized controlled trial. J. Cataract. Refract. Surg. 2021, 47, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Jia, T.; Ogawa, Y.; Miura, M.; Ito, O.; Kohzuki, M. Music Attenuated a Decrease in Parasympathetic Nervous System Activity after Exercise. PLoS ONE 2016, 11, e0148648. [Google Scholar] [CrossRef] [PubMed]
- Aitken, J.C.; Wilson, S.; Coury, D.; Moursi, A.M. The effect of music distraction on pain, anxiety and behavior in pediatric dental patients. Pediatric Dent. 2002, 24, 114–118. [Google Scholar]
- Koch, M.E.; Kain, Z.N.; Ayoub, C.; Rosenbaum, S.H. The sedative and analgesic sparing effect of music. Anesthesiology 1998, 89, 300–306. [Google Scholar] [CrossRef]
- Kavak Akelma, F.; Altınsoy, S.; Arslan, M.T.; Ergil, J. Effect of favorite music on postoperative anxiety and pain. Der Anaesthesist 2020, 69, 198–204. [Google Scholar] [CrossRef]
- Kupeli, I.; Gülnahar, Y. Comparing Different Music Genres in Decreasing Dental Anxiety in Young Adults Who Underwent Third Molar Surgery in Turkey: Randomized Controlled Trial. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2020, 78, 546.e1–546.e7. [Google Scholar] [CrossRef]
- Azizoddin, D.R.; Zamora-Racaza, G.; Ormseth, S.R.; Sumner, L.A.; Cost, C.; Ayeroff, J.R.; Weisman, M.H.; Nicassio, P.M. Psychological Factors that Link Socioeconomic Status to Depression/Anxiety in Patients with Systemic Lupus Erythematosus. J. Clin. Psychol. Med. Settings 2017, 24, 302–315. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, W.; Sang, C.; Zhang, X.; Zhu, K.; Bo, L. Personality, Preoperative Anxiety, and Postoperative Outcomes: A Review. Int. J. Environ. Res. Public Health 2022, 19, 12162. https://doi.org/10.3390/ijerph191912162
Ji W, Sang C, Zhang X, Zhu K, Bo L. Personality, Preoperative Anxiety, and Postoperative Outcomes: A Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12162. https://doi.org/10.3390/ijerph191912162
Chicago/Turabian StyleJi, Wentao, Chao Sang, Xiaoting Zhang, Keming Zhu, and Lulong Bo. 2022. "Personality, Preoperative Anxiety, and Postoperative Outcomes: A Review" International Journal of Environmental Research and Public Health 19, no. 19: 12162. https://doi.org/10.3390/ijerph191912162
APA StyleJi, W., Sang, C., Zhang, X., Zhu, K., & Bo, L. (2022). Personality, Preoperative Anxiety, and Postoperative Outcomes: A Review. International Journal of Environmental Research and Public Health, 19(19), 12162. https://doi.org/10.3390/ijerph191912162