
Diagnostic Performance Evaluation of the Novel Index Combining Urinary Cotinine and 4-(Methylnitrosamino)-1-(3-pyridyl)-1-butanol in Smoking Status Verification and Usefulness for Trend Monitoring of Tobacco Smoking Exposure


Abstract
:1. Introduction
2. Materials and Methods
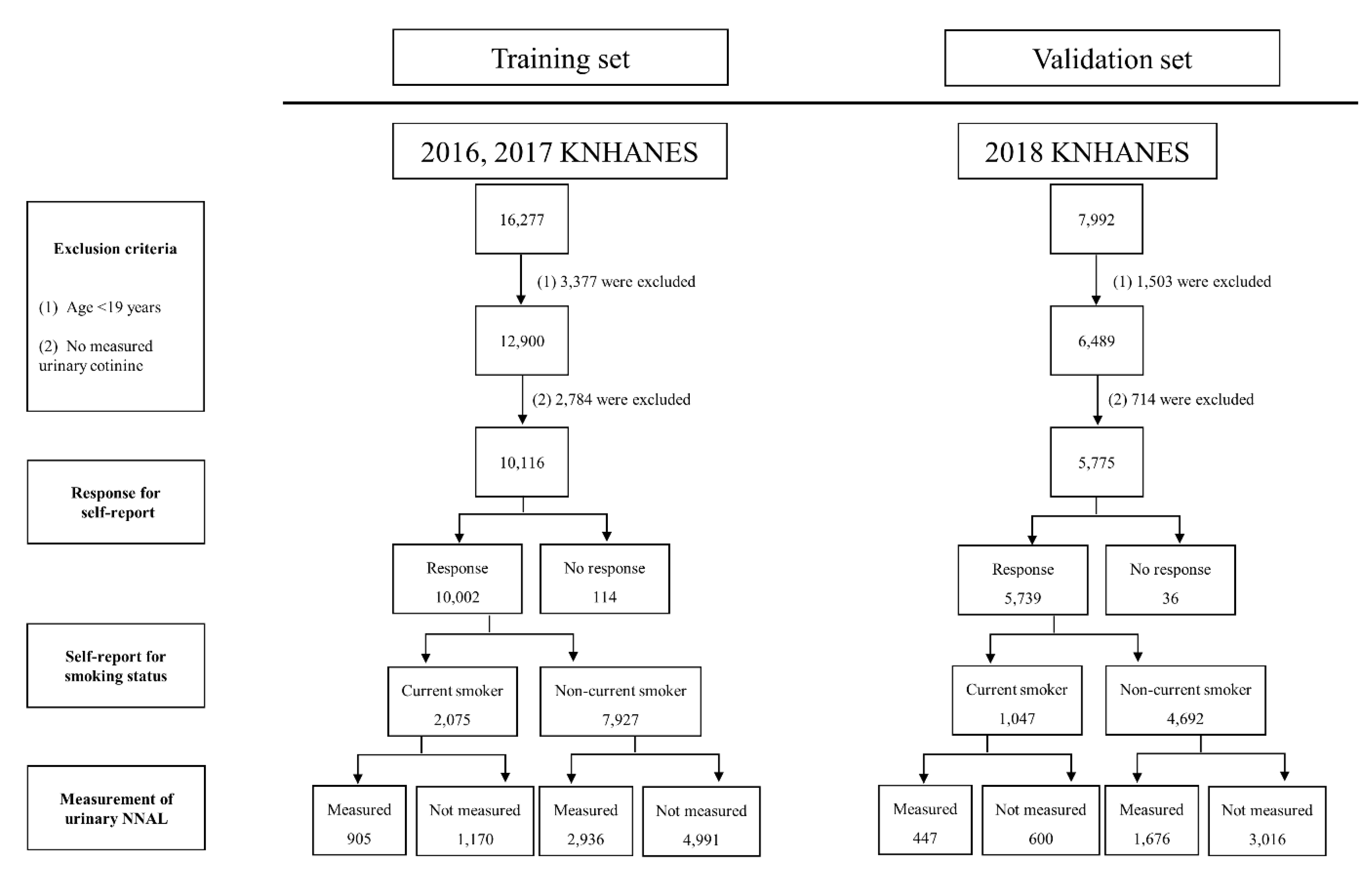
2.1. Study Participants
2.2. Self-Report for Smoking Status
2.3. Self-Report for SHS Exposure
2.4. Measurement of Urinary Cotinine and NNAL
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Study Participants
3.2. Results of the Self-Reported Smoking Status
3.3. Results of the Self-Reported SHS Exposure
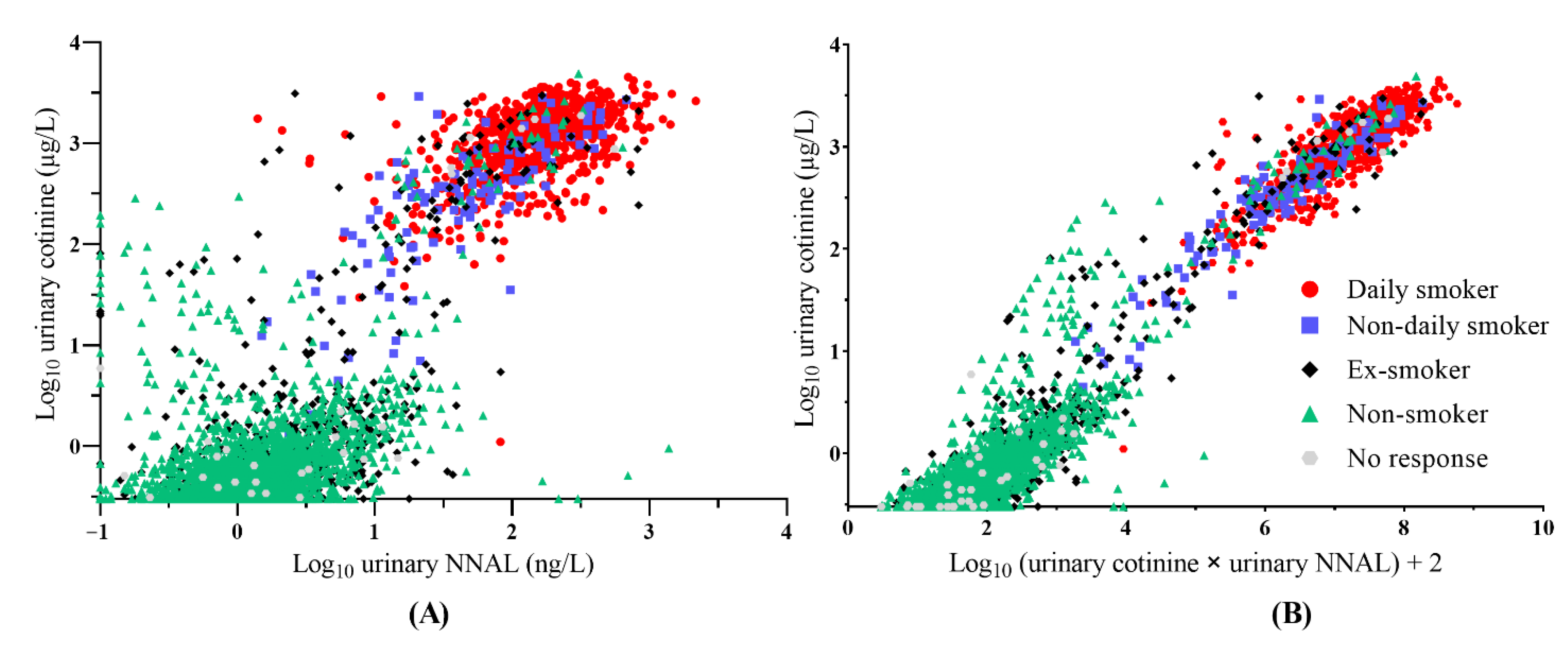
3.4. Scatter Plot of Urinary Cotinine and NNAL in the Training Set
3.5. Scatter Plot of Urinary Cotinine and a Novel Index Multiplying Urinary Cotinine and NNAL in the Training Set
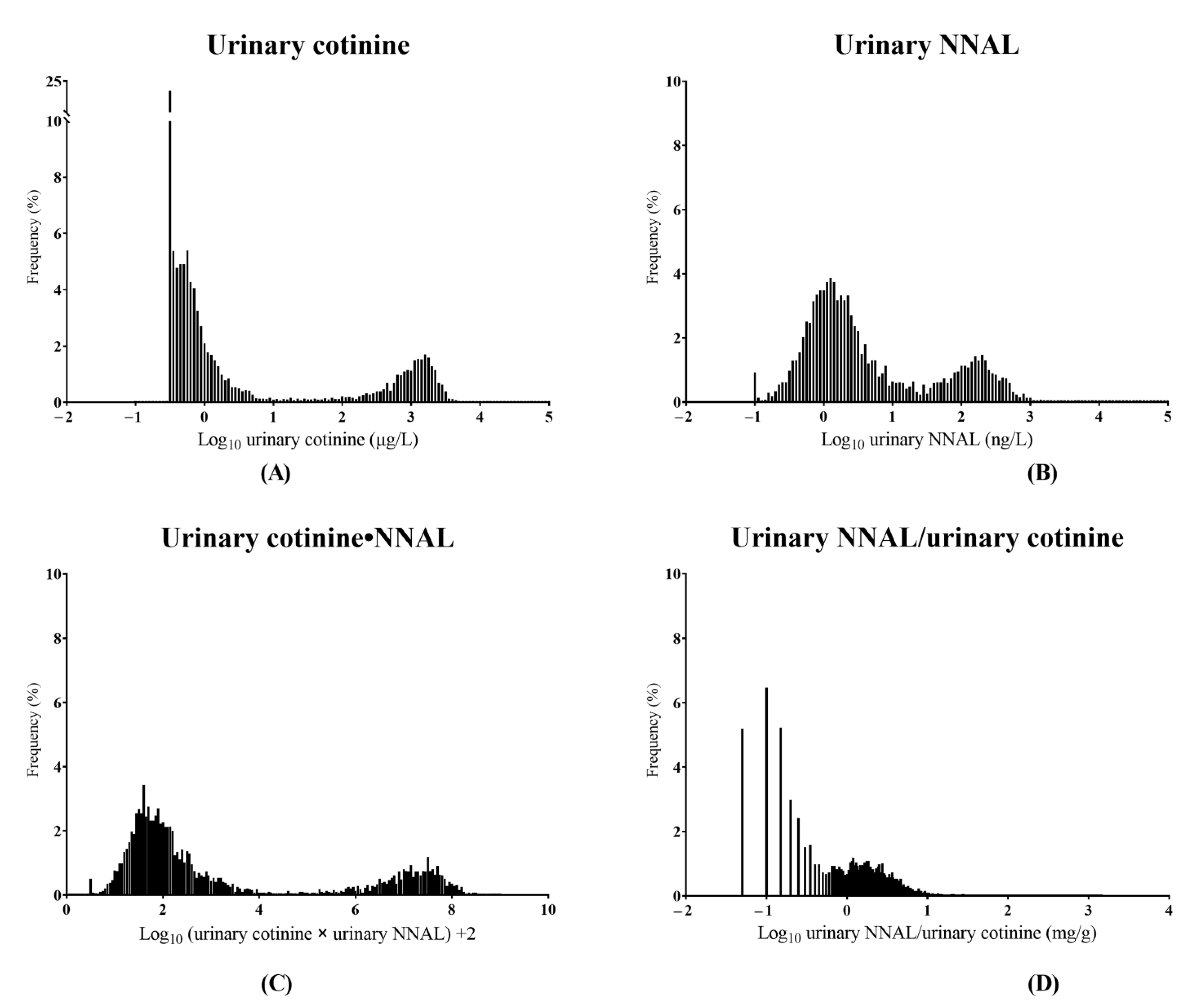
3.6. Distributions of Urinary Biomarkers from All Participants
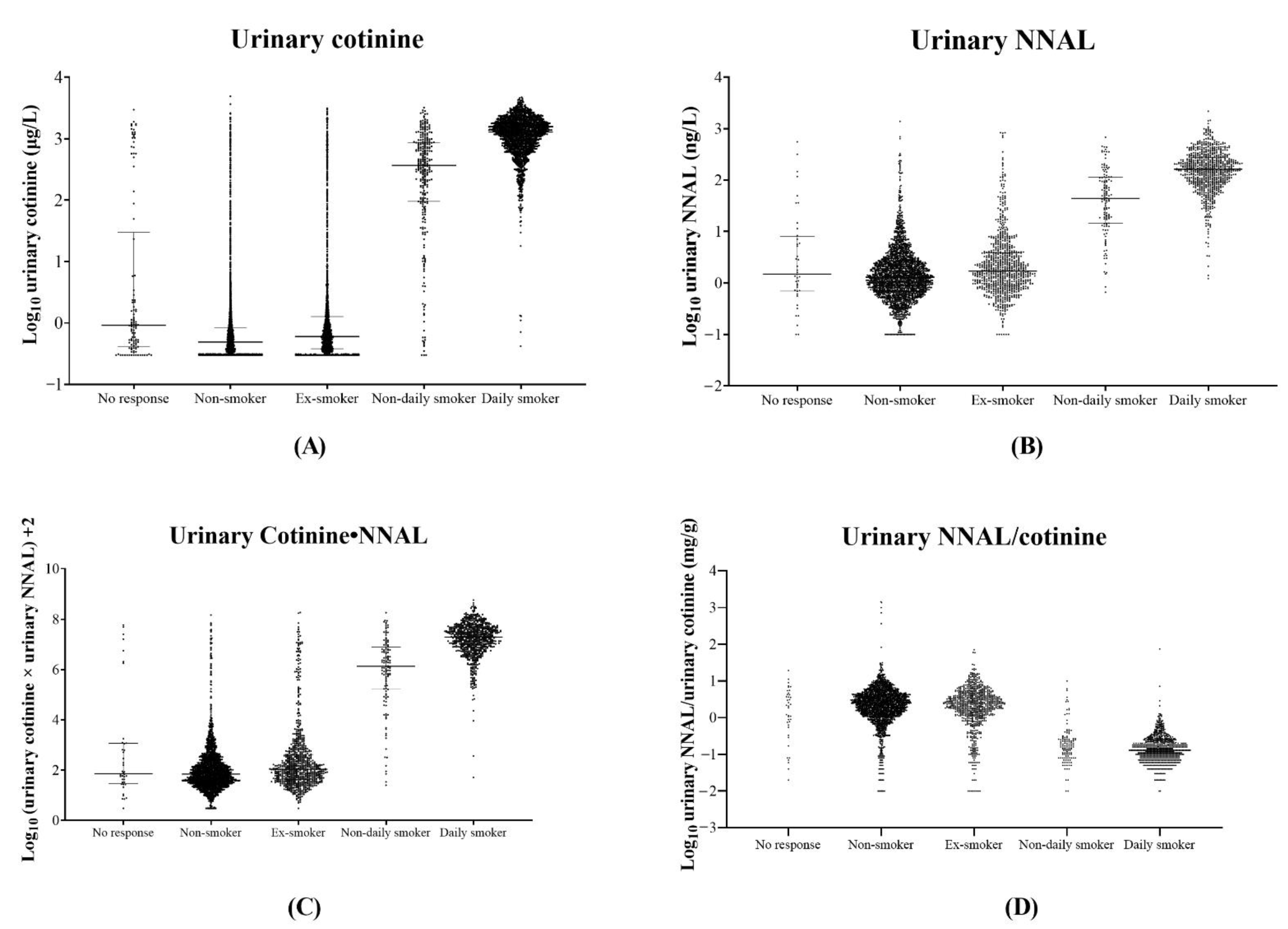
3.7. Established Optimal Cut-Off Values of Urinary Biomarkers Using the Training Set and Diagnostic Performance Evaluation for Smoking Status Classification
3.8. Comparison of the Diagnostic Performance of Urinary Biomarkers in E-Cigarette Users and NRP Users
3.9. Comparison of Diagnostic Performance in Non-Current Smokers according to SHS Exposure
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Samet, J.M. Tobacco Smoking. The leading cause of preventable disease worldwide. Thorac. Surg. Clin. 2013, 23, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Polosa, R.; Thomson, N. Smoking and asthma: Dangerous liaisons. Eur. Respir. J. 2013, 41, 716–726. [Google Scholar] [CrossRef] [PubMed]
- Ebbert, J.O.; Croghan, I.T.; Schroeder, D.R.; Murawski, J.; Hurt, R.D. Association between respiratory tract diseases and secondhand smoke exposure among never smoking flight attendants: A cross-sectional survey. Environ. Health 2007, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Sasco, A.J.; Secretan, M.B.; Straif, K. Tobacco smoking and cancer: A brief review of recent epidemiological evidence. Lung Cancer 2004, 45, S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Scherübl, H. Smoking tobacco and cancer risk. Dtsch. Med. Wochenschr. 2021, 146, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Al-Delaimy, W.K.; Willett, W.C. Measurement of Tobacco Smoke Exposure: Comparison of Toenail Nicotine Biomarkers and Self-Reports. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.; McCullough, L.; Devries, K.; Jategaonkar, N.; Greaves, L.; Richardson, L. Location Restrictions on Smoking: Assessing their Differential Impacts and Consequences in the Workplace. Can. J. Public Health 2009, 100, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P., III. Nicotine chemistry, metabolism, kinetics and biomarkers. Handb. Exp. Pharmacol. 2009, 192, 29–60. [Google Scholar] [CrossRef]
- Kim, B. Workplace smoking ban policy and smoking behavior. J. Prev. Med. Public Health 2009, 42, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Sim, B.; Park, M.-B. Exposure to Secondhand Smoke: Inconsistency between Self-Response and Urine Cotinine Biomarker Based on Korean National Data during 2009–2018. Int. J. Environ. Res. Public Health 2021, 18, 9284. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, D.A.; Sambol, N.C.; Jacob, P.; Hoffmann, E.; Tyndale, R.F.; Fuentes-Afflick, E.; Benowitz, N.L. CYP2A6 genotype but not age determines cotinine half-life in infants and children. Clin. Pharmacol. Ther. 2013, 94, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Matsuki, H.; Hashimoto, K.; Arashidani, K.; Akiyama, Y.; Amagai, T.; Ishizu, Y.; Matsushita, H. Studies on a simultaneous analytical method of urinary nicotine and its metabolites, and their half-lives in urine. J. UOEH 2008, 30, 235–252. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.M.; Edwards, S.H.; Arab, A.; Del Valle-Pinero, A.Y.; Yang, L.; Hatsukami, D.K. Biomarkers of Tobacco Exposure: Summary of an FDA-Sponsored Public Workshop. Cancer Epidemiol. Biomark. Prev. 2017, 26, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Hecht, S.S. Biochemistry, Biology, and Carcinogenicity of Tobacco-Specific N-Nitrosamines. Chem. Res. Toxicol. 1998, 11, 559–603. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Eisner, M.D.; Lazcano-Ponce, E.; Zielinska-Danch, W.; Koszowski, B.; Sobczak, A.; Havel, C.; Jacob, P.; Benowitz, N.L. Comparison of Urine Cotinine and the Tobacco-Specific Nitrosamine Metabolite 4-(Methylnitrosamino)-1-(3-Pyridyl)-1-Butanol (NNAL) and Their Ratio to Discriminate Active from Passive Smoking. Nicotine Tob. Res. 2011, 13, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Nardone, N.; Jain, S.; Dempsey, D.A.; Addo, N.; Helen, G.S.; Jacob, P. Comparison of Urine 4-(Methylnitrosamino)-1-(3)Pyridyl-1-Butanol and Cotinine for Assessment of Active and Passive Smoke Exposure in Urban Adolescents. Cancer Epidemiol. Biomark. Prev. 2018, 27, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Shahab, L.; Goniewicz, M.; Alwis, U.; Xia, Y.; Feng, J.; Blount, B. Exposure to selected toxicants and carcinogens as a function of smoking status and long-term use of nicotine replacement therapy or electronic cigarettes. In Proceedings of the Society for Research on Nicotine and Tobacco 21st Annual Meeting, Philadelphia, PA, USA, 25–28 February 2015. [Google Scholar]
- Selleck, M.J.; Senthil, M.; Wall, N.R. Making Meaningful Clinical Use of Biomarkers. Biomark. Insights 2017, 12, 1177271917715236. [Google Scholar] [CrossRef] [PubMed]
- Vogel, R.I.; Carmella, S.G.; Stepanov, I.; Hatsukami, D.K.; Hecht, S.S. The ratio of a urinary tobacco-specific lung carcinogen metabolite to cotinine is significantly higher in passive than in active smokers. Biomarkers 2011, 16, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-S.; Cho, J.-H.; Lee, Y.-J.; Park, D.-S. Effect of Second-Hand Smoke Exposure on Establishing Urinary Cotinine-Based Optimal Cut-Off Values for Smoking Status Classification in Korean Adults. Int. J. Environ. Res. Public Health 2022, 19, 7971. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Characteristics | KNHANES (2016–2018) | |
|---|---|---|
| Training Set | Validation Set | |
| 2016, 2017 | 2018 | |
| Number | 10,116 | 5775 |
| Age, year (mean ± SD) | 51.1 ± 16.5 | 49.1 ± 16.8 |
| Sex, female (n, %) | 5397 (53.5%) | 3179 (55.0%) |
| Urinary cotinine (μg/L) | 286.8 ± 648.0 | 300.0 ± 682.2 |
| Subjects with measured NNAL concentration | 3841 (37.9%) | 2148 (37.2%) |
| Urinary NNAL (ng/L) | 52.5 ± 131.7 | 45.9 ± 121.2 |
| Response for self-report (n, %) | 10,002 (98.9%) | 5739 (99.4%) |
| Non-current smoker, self-report (n, %) | 7927 (79.3%) | 4692 (81.8%) |
| Non-smoker (n, %) | 5803 (73.2%) | 3428 (73.1%) |
| Ex-smoker (n, %) | 2124 (26.8%) | 1264 (26.9%) |
| Current smoker, self-report (n, %) | 2075 (20.7%) | 1047 (18.2%) |
| Daily smoker (n, %) | 1796 (86.6%) | 906 (86.5%) |
| Non-daily smoker (n, %) | 279 (13.4%) | 141 (13.5%) |
| Usage of nicotine replacement product (NRP) | ||
| Current NRP user (n, %) | 22 (0.2%) | 10 (0.2%) |
| Non-current NRP user (n, %) | 9980 (99.8%) | 5729 (99.8%) |
| Usage of electronic cigarette (e-cigarette) | ||
| Current e-cigarette user (n, %) | 182 (1.8%) | 163 (2.8%) |
| Non-current e-cigarette user (n, %) | 9820 (98.2%) | 5576 (97.2%) |
| Subjects with less or equal to LoD of urinary cotinine (n, %) | 1225 (12.1%) | 1216 (21.1%) |
| Subjects with less or equal to LoD of urinary NNAL (n, %) | 9 (0.2%) | 13 (0.6%) |
| Urinary Biomarker | Dataset | Optimal Cut-Off (95% CI) | Sensitivity (%) | Specificity (%) | Youden’s Index | AUC | 95% CI | p Value |
|---|---|---|---|---|---|---|---|---|
| Cotinine (µg/L) | Training set | 26.9 | 97.93 | 95.07 | 0.930 | 0.983 | 0.981–0.986 | <0.0001 |
| Validation set | (9.3–33.9) | 98.19 | 96.01 | 0.980 | 0.978–0.986 | <0.0001 | ||
| NNAL (ng/L) | Training set | 12.3 | 96.24 | 94.18 | 0.904 | 0.980 | 0.975–0.984 | <0.0001 |
| Validation set | (12.0–18.6) | 96.87 | 92.72 | 0.975 | 0.971–0.984 | <0.0001 | ||
| Cotinine∙NNAL | Training set | 4.0 | 98.45 | 95.33 | 0.938 | 0.985 | 0.981–0.989 | <0.0001 |
| Validation set | (3.9–4.6) | 98.66 | 94.62 | 0.987 | 0.980–0.991 | <0.0001 | ||
| NNAL/cotinine (mg/g) | Training set | 0.6 | 94.70 | 88.15 | 0.828 | 0.937 | 0.929–0.945 | <0.0001 |
| Validation set | (0.6–0.8) | 96.20 | 89.35 | 0.942 | 0.930–0.952 | <0.0001 |
| Urinary Biomarker | Dataset | Optimal Cut-Off (95% CI) | NRP Users | E-Cigarette Users | Current Smokers | Non-Current Smokers | ||
|---|---|---|---|---|---|---|---|---|
| Median (IQR) | Misclassification | Median (IQR) | Misclassification | Median (IQR) | Median (IQR) | |||
| Cotinine (µg/L) | Training set | 26.9 | 1230 (433–2220) | 81.8% (18/22) | 1180 (650–2030) | 2.7% (5/182) | 1150 (608–1716) | 0.54 (0.34–0.95) |
| Validation set | (9.3–33.9) | 767 (246–1676) | 90.0% (9/10) | 1332 (752.5–1884) | 3.0% (5/163) | 1312 (754–1900) | 0.50 (0.31–0.85) | |
| NNAL (ng/L) | Training set | 12.3 | 93.4 (42.1–402) | 90.0% (9/10) | 112 (54.7–271) | 10.1% (8/77) a | 149 (74.6–253) | 1.39 (0.76–2.81) |
| Validation set | (12.0–18.6) | N.T. | 0/0 | 77.9 (16.8–195.3) | 21.4% (15/70) b | 158 (68.1–273) | 1.16 (0.67–2.25) | |
| Cotinine∙NNAL | Training set | 4.0 | 7.46 (6.78–7.55) | 90.0% (9/10) | 7.11 (6.66–7.59) | 2.5% (2/77) | 7.21 (6.71–7.61) | 1.88 (1.47–2.39) |
| Validation set | (3.9–4.6) | N.T. | 0/0 | 6.98 (6.25–7.57) | 2.9% (2/70) c | 7.28 (6.75–7.68) | 1.78 (1.44–2.21) | |
| NNAL/cotinine (mg/g) | Training set | 0.6 | 0.19 (0.07–0.19) | 90.0% (9/10) | 0.13 (0.06–0.21) | 6.3% (5/77) | 0.14 (0.09–0.24) | 2.55 (1.31–4.69) |
| Validation set | (0.6–0.8) | N.T. | 0/0 | 0.07 (0.03–0.16) | 2.9% (2/70) c | 0.13 (0.07–0.22) | 2.08 (1.13–3.53) | |
| Urinary Biomarker | SHS Exposure | No SHS Exposure | Unclear SHS Exposure | |||
|---|---|---|---|---|---|---|
| Median | Less Than LoD | Median | Less Than LoD | Median | Less Than LoD | |
| Cotinine (µg/L) | 0.85 (0.59–1.70) | 10.2% (33/320) | 0.57 (0.40–0.94) | 22.6% (956/4236) | 1.26 (0.59–2.15) | 3.0% (4/136) |
| NNAL (ng/L) | 2.55 (1.32–4.99) | 0.0% (0/49) | 1.24 (0.72–2.38) | 1.1% (13/1191) | 3.02 (0.94–11.30) | 0.0% (0/112) |
| Cotinine∙NNAL | 2.40 (2.04–2.85) | 1.87 (1.54–2.26) | 2.55 (1.94–3.37) | |||
| NNAL/cotinine (mg/g) | 2.34 (1.20–4.01) | 2.00 (1.08–3.45) | 2.19 (1.16–4.52) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-S. Diagnostic Performance Evaluation of the Novel Index Combining Urinary Cotinine and 4-(Methylnitrosamino)-1-(3-pyridyl)-1-butanol in Smoking Status Verification and Usefulness for Trend Monitoring of Tobacco Smoking Exposure. Int. J. Environ. Res. Public Health 2022, 19, 12147. https://doi.org/10.3390/ijerph191912147
Lee H-S. Diagnostic Performance Evaluation of the Novel Index Combining Urinary Cotinine and 4-(Methylnitrosamino)-1-(3-pyridyl)-1-butanol in Smoking Status Verification and Usefulness for Trend Monitoring of Tobacco Smoking Exposure. International Journal of Environmental Research and Public Health. 2022; 19(19):12147. https://doi.org/10.3390/ijerph191912147
Chicago/Turabian StyleLee, Hyun-Seung. 2022. "Diagnostic Performance Evaluation of the Novel Index Combining Urinary Cotinine and 4-(Methylnitrosamino)-1-(3-pyridyl)-1-butanol in Smoking Status Verification and Usefulness for Trend Monitoring of Tobacco Smoking Exposure" International Journal of Environmental Research and Public Health 19, no. 19: 12147. https://doi.org/10.3390/ijerph191912147