
Effects of the Developing and Using a Model to Predict Dengue Risk Villages Based on Subdistrict Administrative Organization in Southern Thailand

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Development Step
2.2.1. Preparation Step
2.2.2. Assessment Step
- (1)
- Houses’ Environment Assessment
- (2)
- UDS and ULISS Assessment
2.2.3. Development Step
- (1)
- Predicting High- and Low-Risk Dengue Villages
- (2)
- Setting Larval Indices Surveillance System
- (3)
- The UDS and ULISS Training Program
- (4)
- Develop the Local Wisdom Innovation (LWI) with Herbs for Mosquito Repellant
2.2.4. Implementation Step
2.2.5. Evaluation Step
2.3. Questionnaires for Assessment and Evaluation
2.4. Data Analysis
3. Results
3.1. Keawsan SAO Dengue Model
3.1.1. Setting Team Leader’s Responsibility
3.1.2. Situation Assessment
- (1)
- Houses’ Environment Assessment
3.1.3. Village Dengue Risk Prediction Criteria
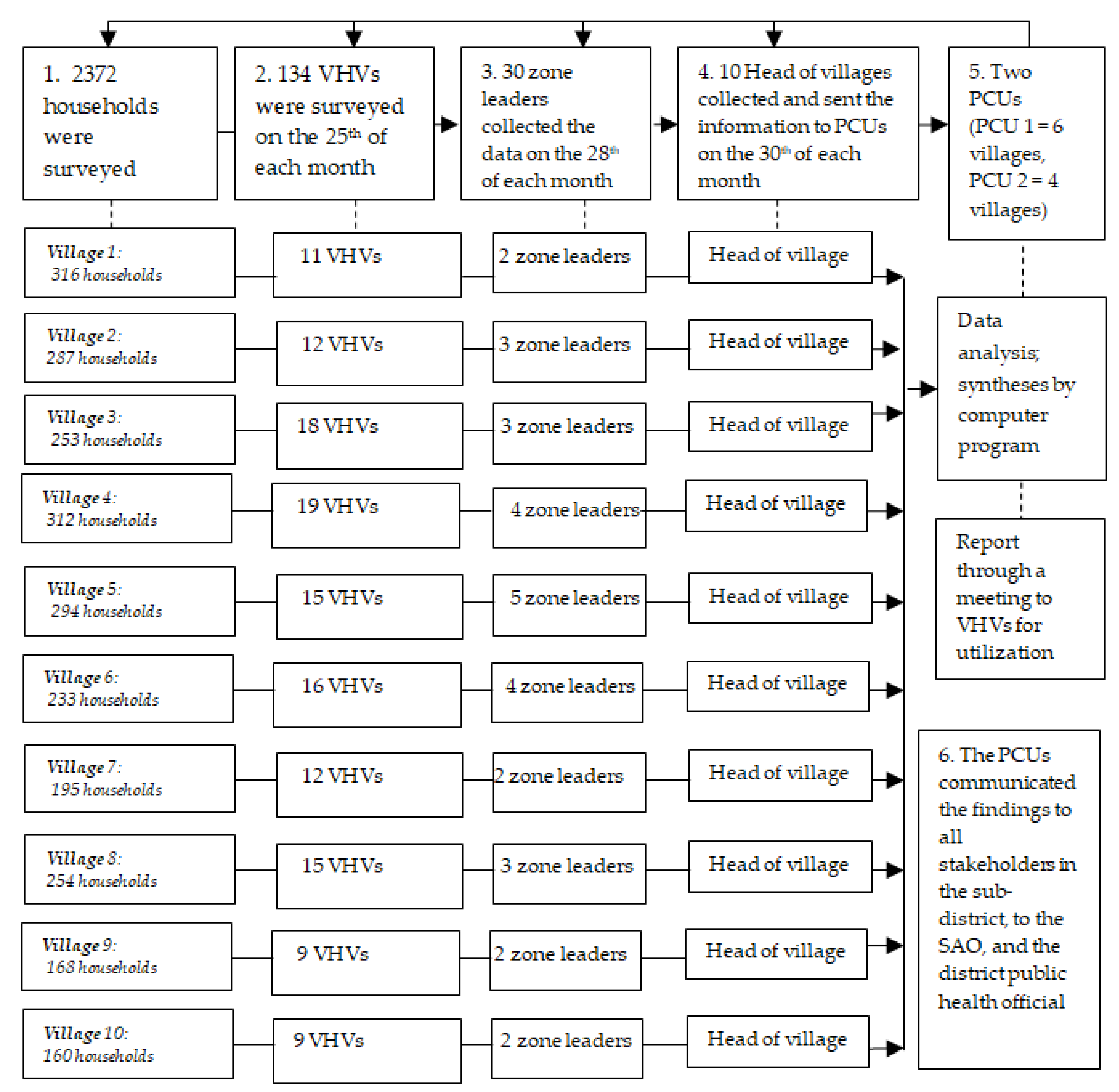
3.1.4. The Larval Indices Surveillance System
- (1)
- In total, 2372 family leaders were surveyed using the larval indices and were helped in the elimination of the breeding sites of mosquitos in their houses and within the surrounding 100 meters of their houses every seven days.
- (2)
- The 134 VHVs and family leaders underwent surveys on the larval indices of 10 to 15 households, 5 schools, 4 child development centers, and 4 four temples. Their data were inserted in their “violet books”—notebooks for recording the results of the household larval data from the 10 to 15 houses surveyed per a VHV on 25th of each month—and the books were sent to the 30 zone leaders.
- (3)
- The 30 zone leaders collected the survey data from their VHVs, inserted them in their “blue books”, and sent the books to the community leader on the 28th of each month.
- (4)
- The 10 community leaders collected the data from each zone leader, inserted them in their “yellow books” on the 30th of each month, and sent those to the two primary care units.
- (5)
- Two primary care units gathered and entered the data from all villages into the website http://nakhonsi.denguelim.com. The levels of the larval indices (BI, HI, and CI) were reported in a VHV meeting on the 9th of each next month. All the stakeholders were then used to construct a local wisdom innovation.
- (6)
- The primary care units communicated the findings to all the stakeholders, to the SAO, and to the district public health official.
3.1.5. The UDS and ULISS Training Programs
- (1)
- The UDS and ULISS training programs were applied to 50 stakeholders in the community and the SAO. At the program’s onset, the UDS training was applied; the SAO devised the training for all the stakeholders regarding the objectives of the methods to tackle dengue, as well as the meaning, causes, signs, symptoms, and treatment for dengue illness. Thereafter, the ULISS training was applied, focusing on explaining the seven steps of the LISS and the roles of the stakeholders who participated in and supported the initiative.
- (2)
- The UDS and ULISS training programs were applied to all 134 participating VHVs; this is because the VHVs were the key stakeholders for tackling dengue in villages where the UDS and ULISS training programs were conducted. They underwent workshops for six months and completed the 15-item UDS and ULISS questionnaires pre- and post-training (in June and August 2020). After the village health volunteers’ training, they were requested to share their understanding of dengue solutions and the larval indices surveillance system with the family leader during the larval indices survey on every 25th day of each month from June to August 2020.
- (3)
- The UDS and ULISS training programs were also applied to 59 student leaders who represented five schools. They also completed the questionnaires before the test, in June 2020, and post-test, after training for 3 months.
3.1.6. Local Wisdom Innovation
3.2. Effects after Using Keawsan SAO Dengue Model
3.2.1. VHVs’ UDS and ULISS
3.2.2. Family Leaders’ UDS and ULISS
3.2.3. Student Leaders’ UDS and ULISS
3.2.4. Larval Indices Level before and after Using the Model
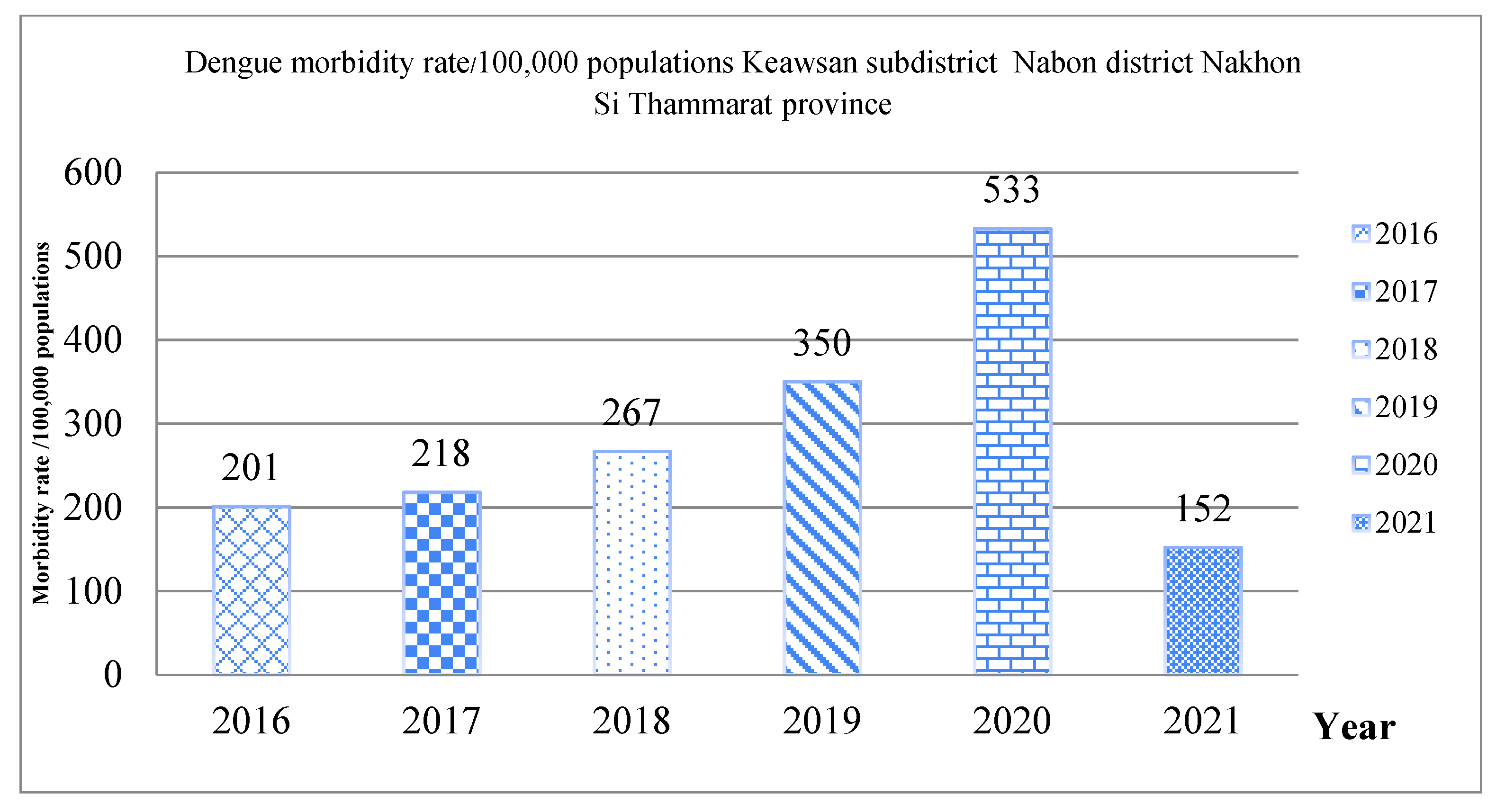
3.2.5. Dengue Morbidity Rate
3.2.6. Satisfaction of Stakeholders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control; WHO Library Cataloguing-in-Publication Data: Geneva, Switzerland, 2009.
- WHO. Handbook for Clinical Management of Dengue; WHO Library Catagologulng-in-Publication Data: Geneva, Switzerland, 2012.
- Vector Borne Diseases Division, Diseases Control Department, Thai Ministry of Public Health. Academic Manual Disease of Dengue Infection and Dengue Heamorrhagic Fever: Perspective of Medical and Public Health, 2nd ed.; Vector Borne Diseases Division, Diseases Control Department: Bangkok, Thailand, 2015.
- Bhumiratana, A.; Intarapuk, A.; Chujun, S.; Kaewwaen, W.; Sorosjinda-Nunthawarasilp, P.; Koyadun, S. Thailand momentum on policy and practice in local legislation on dengue vector control. Interdiscip. Perspect. Infect. Dis. 2014, 2014, 217237. [Google Scholar] [CrossRef]
- Aumaung, B.; Sevana, J.; Amatchaiyaku, K. Assessment of local ordinance related to mosquito control by local administrative organizations in 2014. Dis. Control J. 2017, 43, 76–84. (In Thai) [Google Scholar]
- Bongjaporn, N.; Suwonkerd, W.; Sriwongpun, T. The achievement of driving for the use of local ordinances of the sub-district administrative organization according to the public health act BE 2535 to reduce the source of dengue vectors. The Office of Disease Prevention and Control 9th. Nakhon Ratchasima J. 2020, 26, 25–35. [Google Scholar]
- Vector Borne Diseases Division, Dengue Situation. 2019: Vector Borne Diseases Division, Diseases Control Department: Thai Ministry of Public Health. Available online: https://ddc.moph.go.th/en/details.php?topic=high (accessed on 10 July 2020).
- Kusuma, Y.S.; Burman, D.; Kumari, R.; Lamkang, A.S.; Babu, B.V. Impact of health education based intervention on community’s awareness of dengue and its prevention in Delhi, India. Glob. Health Promot. 2019, 26, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Suwanbamrung, C.; Kusol, K.; Tantraseneerate, K.; Promsupa, S.; Doungsin, T.; Tongian, S. Developing the participatory education program for dengue prevention and control in the primary school, southern region, Thailand. Health 2015, 7, 1255–1267. [Google Scholar] [CrossRef]
- Suwanbamrung, C.; Thoutong, C.; Eksirinimit, T.; Tongjan, S.; Thongkew, K. The use of the “Lansaka Model” as the larval indices surveillance system for a sustainable solution to the dengue problem in southern Thailand. PLoS ONE 2018, 13, e0201107. [Google Scholar] [CrossRef]
- Suwanbamrung, C. Developing the active larval indices surveillance system for dengue solution in low and high dengue risk primary care units, Southern Thailand. J. Health Res. 2018, 32, 408–420. [Google Scholar] [CrossRef]
- Suwanbamrung, C.; Le, C.N.; Kaewsawat, S.; Chutipattana, N.; Khammaneechan, P.; Thongchan, S.; Nontapet, O.; Thongsuk, C.; Laopram, S.; Niyomchit, C.; et al. Developing risk assessment criteria and predicting high- and low-dengue risk villages for strengthening dengue prevention activities: Community participatory action research, Thailand. J. Prim. Care Community Health 2021, 12, 1–14. [Google Scholar] [CrossRef]
- Saré, D.; Pérez, D.; Somé, P.-A.; Kafando, Y.; Barro, A.; Ridde, V. Community-based dengue control intervention in Ouagadougou: Intervention theory and implementation fidelity. Glob. Health Res. Policy 2018, 3, 2–11. [Google Scholar] [CrossRef]
- Ouédraogo, S.; Benmarhnia, T.; Bonnet, E.; Somé, P.-A.; Barro, A.S.; Kafando, Y.; Soma, D.D.; Dabiré, R.K.; Saré, D.; Fournet, F.; et al. Evaluation of effectiveness of a community-based intervention for control of dengue virus vector, Ouagadougou, Burkina Faso. Emerg. Infect. Dis. J. 2018, 24, 1859–1867. [Google Scholar] [CrossRef]
- Xue, Q.; Xie, X.; Liu, Q.; Zhou, Z.; Zhu, K.; Wu, H.; Wan, Z.; Feng, Y.; Meng, H.; Zhang, J.; et al. Knowledge, attitudes, and practices towards COVID-19 among primary school students in Hubei Province, China. Child. Youth Serv. Rev. 2021, 120, 105735. [Google Scholar] [CrossRef] [PubMed]
- Suwanbamrung, C. Reflections of health leaders’ experiences related dengue solutions from transmitting a technology of larval indices surveillance system in Southern Thailand. Trends Med. 2019, 19, 1–6. [Google Scholar] [CrossRef]
- Selvarajoo, S.; Liew, J.W.K.; Tan, W.; Lim, X.Y.; Refai, W.F.; Zaki, R.A.; Sethi, N.; Sulaiman, W.Y.W.; Lim, Y.A.L.; Vadivelu, J.; et al. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: A cross-sectional study. Sci. Rep. 2020, 10, 9534. [Google Scholar] [CrossRef] [PubMed]
- Víctor Alvarado-Castro, V.; Paredes-Solís, S.; Nava-Aguilera, E.; Morales-Pérez, A.; Alarcón-Morales, L.; Balderas-Vargas, N.A.; Andersson, N. Assessing the effects of interventions for Aedes aegypti control: Systematic review and meta-analysis of cluster randomised controlled trials. BMC Public Health 2017, 17 (Suppl. 1), 384–407. [Google Scholar] [CrossRef] [PubMed]
- WHO. Monograph on Dengue/Dengue Haemorrhagic Fever; Regional Office for South-East Asia: New Delhi, India, 1993; Available online: https://apps.who.int/iris/handle/10665/205538 (accessed on 20 October 2019).
- Thai Ministry of Public Health. Manual of Assessment District for Sustainable Disease Control. Nontaburi Province: Department of Disease Control; Ministry of Public Health: Bangkok, Thailand, 2013. Available online: http://data.ptho.moph.go.th/cdc/files/news/f01_20121219085230_93010000.pdf (accessed on 20 October 2019). (In Thai)
- WHO Regional Office for South-East Asia. Comprehensive Guidelines for Prevention and Control of Dengue and Dengue Haemorrhagic Fever; Revised and Expanded Edition; SEARO Technical Publication Series No. 60; WHO: New Delhi, India, 2011.
- Vanlerberghe, V.; Toledo, M.E.; Rodríguez, M.; Gómez, D.; Baly, A.; Benítez, J.R.; Stuyft, P.V. Community involvement in dengue vector control: Cluster randomised trial. MEDICC Rev. 2010, 12, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Suwanbamrung, C. Larval Indices Surveillance System and Dengue Risk Prediction for Dengue Solution from Household to Province: A Case "SURAT Dengue Model"; Kponkanpim Publishing: Nakhon Si Thammmarat Province, Thailand, 2019; p. 292. [Google Scholar]
- Marcos-Marcos, J.; Labry-Lima, A.O.; Toro-Cardenas, S.; Lacasaña, M.; Degroote, S.; Ridde, V.; Bermudez-Tamayo, C. Impact, economic evaluation, and sustainability of integrated vector management in urban settings to prevent vector-borne diseases: A scoping review. Infect. Dis. Poverty 2018, 7, 1–14. [Google Scholar] [CrossRef]
- Anderson, L.W.; Krathwohl, D.R. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives; Addison Wesley Longman, Inc.: New York, NY, USA, 2001. [Google Scholar]
- Harvey, K.; Horton, L. Bloom’s human characteristics and school learning. Phi Delta Kappan 1977, 59, 189–193. [Google Scholar]
- Imsawat, T.; Oowichit, Y.; Saybun, S. Understanding Dengue and Larval Indices of Village Health Volunteer in Lansaka District, Nakhon Si Thammarat Province, in School of Public Health. Bachelor’s Thesis, Walailak University, Nakhon Si Thammmarat Province, Thailand, September 2018. (In Thai). [Google Scholar]
- Bolarinwa, O. Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger. Postgrad. Med. J. 2015, 22, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, A.M.; Ibrahim, N.A. Knowledge, attitude and practice towards dengue fever prevention and associated factors among public health sector health-care professionals: In Dire Dawa, eastern Ethiopia. Risk Manag. Healthc. Policy 2019, 12, 91–104. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic Analysis. In APA Handbook of Research Methods in Psychology, Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological; Cooper, H., Camic, P.M., Long, D.L., Panter, A.T., Rindskopf, D., Sher, K.J., Eds.; American Psychological Association: Washington, DC, USA, 2012; Volume 2, pp. 57–71. [Google Scholar]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Limpavitthayakul, M.; Srihawong, W.; Deogchan, T. Local legislation development model on dengue vector control in subdistrict administrative organization of Dangmor, Khueang Nai District, Ubon Ratchathani Province. J. Ratchathani Innov. Health Sci. 2017, 1, 99–113. (In Thai) [Google Scholar]
- Schmidt, W.P.; Suzuki, M.; Thiem, V.D.; White, R.G.; Tsuzuki, A.; Yoshida, L.M.; Yanai, H.; Haque, U.; Tho, L.H.; Anh, D.D.; et al. Population density, water supply, and the risk of dengue fever in Vietnam: Cohort study and spatial analysis. PLoS Med. 2011, 8, e1001082. [Google Scholar] [CrossRef] [PubMed]
- Shuaib, F.; Todd, D.; Campbell-Stennett, D.; Ehiri, J.; Jolly, P.E. Knowledge, attitudes and practices regarding dengue infection in Westmoreland, Jamaica. West Indian Med. J. 2010, 59, 139–146. [Google Scholar] [PubMed]
- Farich, A.; Lipoeto, N.I.; Bachtiar, H.; Hardisman, H. The effects of community empowerment on preventing dengue fever in lampung province, Indonesia. Open Access Maced. J. Sci. 2020, 8, 194–197. [Google Scholar] [CrossRef]
- Hanklang, S.; Ratanasiripong, P.; Sivasan, S. Effectiveness of the intervention program for dengue hemorrhagic fever prevention among rural communities in Thailand. J. Health Res. 2018, 32, 352–363. [Google Scholar] [CrossRef]
- Lachyan, A.S.; Mabood, A.K.; Zaki, R.A.; Bratati, B. Effect of community-based intervention on awareness of dengue and its prevention among urban poor community in India: A systematic review approach. Int. J. Community Med. Public Health 2020, 7, 5182–5189. [Google Scholar] [CrossRef]
- Tang, B.; Xiao, Y.; Sander, B.; Kulkarni, M.A.; RADAM-LAC Research Team; Wu, J. Modelling the impact of antibody-dependent enhancement on disease severity of Zika virus and dengue virus sequential and co-infection. R. Soc. Open Sci. 2020, 7, 191749. [Google Scholar] [CrossRef]
- Bureau of Knowledge Management DoDC, Thai Ministry of Public Health. Manual of Assessment for Center of disease Control: District Health System and Disease Control in 2016–2017; Bureau of Knowledge Management DoDC, Thai Ministry of Public Health: Nonthaburi, Thailand, 2017. (In Thai)
- Jain, R.; Sontisirikit, S.; Iamsirithaworn, S.; Prendinger, H. Prediction of dengue outbreaks based on disease surveillance, meteorological and socio-economic data. BMC Infect. Dis. 2019, 19, 272. [Google Scholar] [CrossRef]
- Sánchez-González, G.; Condé, R.; Noguez Moreno, R.; López Vázquez, P.C. Prediction of dengue outbreaks in Mexico based on entomological, meteorological and demographic data. PLoS ONE 2018, 13, e0196047. [Google Scholar] [CrossRef]
- Piedrahita, L.D.; Agudelo Salas, I.Y.; Marin, K.; Trujillo, A.I.; Osorio, J.E.; Arboleda-Sanchez, S.O.; Restrepo, B.N. Risk factors associated with dengue transmission and spatial distribution of high seroprevalence in schoolchildren from the urban area of Medellin, Colombia. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 2308095. [Google Scholar] [CrossRef]
- Sirisena, P.; Noordeen, F.; Kurukulasuriya, H.; Romesh, T.A.; Fernando, L. Effect of climatic factors and population density on the distribution of dengue in Sri Lanka: A GIS based evaluation for prediction of outbreaks. PLoS ONE 2017, 12, e0166806. [Google Scholar] [CrossRef]
- Banerjee, S.; Aditya, G.; Saha, G.K. Household Wastes as Larval Habitats of Dengue Vectors: Comparison between Urban and Rural Areas of Kolkata, India. PLoS ONE 2015, 10, e0138082. [Google Scholar] [CrossRef]
- Bowman, L.R.; Runge-Ranzinger, S.; McCall, P.J. Assessing the Relationship between Vector Indices and Dengue Transmission: A Systematic Review of the Evidence. PLoS Negl. Trop. Dis. 2014, 8, e2848. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.C.; Luo, L.; Li, L.; Jing, Q.L.; Ou, C.Q.; Yang, Z.C.; Chen, X.G. The impacts of mosquito density and meteorological factors on dengue fever epidemics in Guangzhou, China, 2006–2014: A time-series analysis. Biomed. Environ. Sci. 2015, 28, 321–329. [Google Scholar] [PubMed]
- Suwanbamrung, C.; Dumpan, A.; Thammapalo, S.; Sumrongtong, R.; Phedkeang, P. A model of community capacity building for sustainable dengue problem solution in Southern Thailand. Health 2011, 3, 584–601. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Stakeholder/Representative of Stakeholder of the Subdistrict | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CPAR Step | Family Leader (N = 2372) | VHV (N = 134) | Student Leader (N = 59) | Teacher of 5 Schools (N = 5) | Staff of CDC (N = 4) | Community Leader (N = 10) | Temple (N = 3) | SAO Committee (N = 10) | PCU (N = 2) | PHOD (N = 2) | |
| Preparation step | 3 | 20 | 5 | 4 | 10 | 3 | 10 | 2 | 2 | ||
| Houses’ environment assessment | 824 * | ||||||||||
| Development step: LISS | 134 ** | 10 | 2 | ||||||||
| Development step: LWI | 134 ** | 4 | 2 | 2 | |||||||
| Implementation step | 2372 | 134 ** | 5 | 4 | 10 | 2 | 10 | 2 | 2 | ||
| Evaluation: UDS, ULISS | 824 * | 134 ** | 59 | ||||||||
| Stakeholders | Responsibility |
|---|---|
| Family leaders /community leaders (N = 2372) | Responsible for conducting the survey on the household larval indices every 7 days. They were supposed to collaborate with VHVs in activities related to dengue prevention and control by learning through the UDS and ULISS training programs, which provided them with methods for achieving local wisdom innovation. |
| VHVs (N = 134) | Responsible for conducting the larval indices surveillance system, the assessment of the risk of dengue in the village, and monitoring community innovation. They were also supposed to communicate about the UDS and ULISS to every household via survey activities and stickers of dengue prevention guidelines for the householders. |
| PCUs (N = 2) | Responsible for coordinating VHVs and to enter data into http://nakhoni.denguelim.com (accessed on 8 October 2020) Responsible for communicating about dengue information and the risk level to all stakeholders, as well as for supporting dengue prevention/control activities. |
| SAO | Responsible for setting up plans and strategies; supporting with budget; monitoring project processes; using information to support local wisdom innovation; and promoting a continued dengue prevention/control plan. |
| The district public health official | Responsible for communicating to all stakeholders and supporting the SAO. |
| 59 Student leaders in 5 schools 4 Child development centers 3 Temples | Responsible for collaborating with VHVs, PCUs, households, and the SAO for dengue prevention/control initiatives, and for providing data on larval indices through surveys at least every 7 days; they were also supposed to make good use of the initiatives of other parties to promote local wisdom innovation. |
| Village Dengue Risk Prediction Criteria (RDVPC) | Point | Village | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 a | 2 a | 3 b | 4 b | 5 a | 6 b | 7 a | 8 b | 9 a | 10 a | ||
| 1.Dengue severity aspect | |||||||||||
| 1.1. Endemic village factor | 5 | 5 | 2 | 5 | 5 | 5 | 5 | 3 | 3 | 3 | 3 |
| 1.2. Dengue herd immunity factor | 5 | 2 | 4 | 5 | 5 | 1 | 5 | 1 | 5 | 1 | 1 |
| 1.3. Current morbidity rate factor | 5 | 1 | 1 | 1 | 1 | 1 | 1 | 5 | 1 | 1 | 1 |
| Total dengue severity | 15 | 8 | 7 | 11 | 11 | 7 | 11 | 9 | 9 | 5 | 5 |
| 2.Dengue outbreak opportunity aspect | |||||||||||
| 2.1. Population movement factor | 3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 2.2. Population density in village | 5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 2.3. Strengthening village for dengue prevention activities | 10 | ||||||||||
| (1) Larval indices surveillance system | 1 | 1 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 1 | |
| (2) Garbage management | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| (3) Larval indices level of the village | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| (4) Community capacity activities | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| (5) School-based dengue prevention activities | 1 | 1 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 1 | |
| Total dengue outbreak opportunity aspect | 18 | 7 | 7 | 9 | 9 | 7 | 9 | 7 | 9 | 7 | 7 |
| Total full score | 33 | 15 * | 14 * | 20 ** | 20 ** | 14 * | 20 ** | 14 * | 18 ** | 12 * | 12 * |
| VHVs’ UDS | Correct Response n (%) | |||
|---|---|---|---|---|
| Before (n = 109) | After (n = 90) | |||
| 1. If a patient has a high fever for 2 to 7 days, petechiae, and a painful enlargement of the liver, the patient is showing signs of dengue infection. | 94 (51.4) | 89 (48.6) | 10.67 *** | |
| 2. If the patient presents signs and symptoms of dengue, then the patient is showing signs of a dengue viral infection. | 84 (48.6) | 89 (51.4) | 20.67 *** | |
| 3. If a person living in a high dengue risk area is infected with one dengue serotype, they may have lifelong immunity to that strain. However, they would still be vulnerable to other serotypes and could, thus, be infected with the other dengue serotypes later in life. | 17 (16.8) | 84 (83.2) | 119.19 *** | |
| 4. If a patient is protected from female Aedes aegypti bites, they will be safe from dengue. | 77 (48.4) | 82 (51.6) | 16.03 *** | |
| 5. If a patient has a high fever for 2 to 7 days, nausea, vomiting, and possible abdominal pain, the patient is in the fever stage. | 58 (39.5) | 89 (60.5) | 46.15 *** | |
| 6. If a patient with dengue hemorrhagic fever presents pain at the right lower costal margin, they are showing signs of hepatomegaly. | 59 (39.6) | 90 (60.4) | 55.14 *** | |
| 7. If a patient with dengue hemorrhagic fever presents signs of shock from leakage of plasma, they will have poor tissue perfusion, weak pulse, and narrowed pulse pressure. | 61 (40.4) | 90 (59.6) | 52.23 *** | |
| 8. If your neighbor presents signs of poor tissue perfusion, weak pulse, and clammy skin, you need to send them to hospital. | 82 (48.2) | 88 (51.8) | 20.13 *** | |
| 9. Dengue patients should avoid consuming aspirin or non-steroidal anti-inflammatory drugs because they may cause gastritis and subsequent massive gastrointestinal or hepatic injury. | 43 (33.1) | 87 (66.9) | 71.25 *** | |
| 10. If your neighbor presents high fever on day 1, you give one paracetamol every 6 h and a tepid sponge bath. | 74 (46.3) | 86 (53.8) | 23.95 *** | |
| 11. You suggest for your neighbor to prevent mosquito bites by using skin lotion. | 56 (39.2) | 87 (60.8) | 50.01 *** | |
| 12. If a village has a dengue disease index above the threshold, you suggest a dengue prevention strategy that will destroy the mosquito breeding grounds and larva around the houses. | 93 (51.7) | 87 (48.3) | 7.45 ** | |
| 13. Tiliacora leaves do not serve as a natural herbal remedy for concocting a mosquito repellent. | 61 (42.1) | 84 (57.9) | 0.06 ns | |
| 14. Temephos sand granulates may be used to eliminate larval mosquitos, but not to eliminate mosquito eggs. | 7 (8.0) | 81 (92.0) | 72.76 *** | |
| 15. Household members must complete larval surveys and eliminate contaminated water containers in their house every 7 days. | 34 (54.8) | 87 (45.2) | 88.67 *** | |
| Total | Poor level (cut-off point < 12) | 103 (100.0) | 0 (0.0) | 0.000 ***, a |
| Good level (cut-off point ≥ 12) | 6 (6.3) | 90 (93.8) | ||
| VHVs’ ULISS | Correct Responses, n (%) | |||
|---|---|---|---|---|
| Before (n = 109) | After (n = 90) | |||
| 1. VHVs are surveyed on the 25th of each month. They are supposed to send data to the zone leader on the 28th of each month, to head of the village on the 30th, to the PCU for analysis, and to report to all stakeholders to prepare a dengue solution program. This process is called the larval indices surveillance system. | 29 (25.7) | 84 (74.3) | 89.45 *** | |
| 2. The objective of the VHVs’ larval survey is to reduce dengue outbreaks. | 93 (51.1) | 89 (48.9) | 11.62 *** | |
| 3. Larval indices formula = Breteau index (BI) | 26 (22.8) | 88 (77.2) | 110.10 *** | |
| 4. Larval indices formula = House index (HI) | 19 (18.8) | 82 (81.2) | 107.07 *** | |
| 5. Larval indices formula = Container index (CI) | 14 (14.9) | 80 (85.1) | 114.38 *** | |
| 6. The standard number for positive containers per 100 houses inspected is <50 | 7 (7.4) | 88 (92.6) | 164.91 *** | |
| 7. The standard level for percentage of houses infested with larva and/or pupae is <10 | 34 (29.1) | 83 (70.9) | 75.79 *** | |
| 8. The standard percentage of water-holding infested containers with larva is <1 | 12 (12.1) | 87 (87.9) | 144.68 *** | |
| 9. If the survey finds that among 20 houses there are 4 that are infested or that among 1000 water containers there are 200 that are infested, BI = 1000. | 0 (0) | 87 (100) | 187.21 ***, a | |
| 10. If the survey finds that among 20 houses there are 4 that are infested or that among 1000 water containers there are 200 that are infested, HI = 20. | 36 (31.6) | 78 (68.4) | 57.96 *** | |
| 11. If the survey finds that among 20 houses there are 4 that are infested or that among 1000 water containers there are 200 that are infested, CI = 20. | 25 (23.4) | 82 (76.6) | 5.03 * | |
| 12. If the water container capacity is 100 L, we can use red lime in the container. | 6 (6.3) | 89 (93.7) | 172.31 *** | |
| 13. The larval indices survey needs to be conducted every 7 days because the life cycle of Aedes aegypti ranges from 7 to 11 days. | 5 (5.6) | 84 (94.4) | 157.05 *** | |
| 14. The results of the larval indices surveillance system must be documented every 25th of the month in the “violet book”. | 27 (23.3) | 89 (76.7) | 111.39 *** | |
| 15. VHVs who are community leaders should collect data from zone leaders and send to PCUs every 30th of the month. | 12 (11.9) | 89 (88.1) | 152.32 *** | |
| Total | Poor level (cut-off point < 12) | 109 (97.3) | 3 (2.7) | 0.000 ***, a |
| Good level (cut-off point ≥ 12) | 0 (0.0) | 87 (100) | ||
| Family Leaders’ UDS | Correct Responses n (%) | |||
|---|---|---|---|---|
| Before (n = 932) | After (n = 856) | |||
| 1. If a patient has a high fever for 2 to 7 days, petechiae, and a painful enlargement of the liver, the patient is showing signs of dengue infection. | 794 (49.3) | 817 (50.7) | 52.57 *** | |
| 2. If the patient presents signs and symptoms of dengue, then the patient is showing signs of a dengue viral infection. | 586 (44.5) | 731 (55.5) | 116.64 *** | |
| 3. If a person living in a high dengue risk area is infected with one dengue serotype, they may have lifelong immunity to that strain. However, they would still be vulnerable to other serotypes and could, thus, be infected with the other dengue serotypes later in life. | 383 (37.6) | 635 (62.4) | 199.23 *** | |
| 4. If a patient is protected from female Aedes aegypti bites, they will be safe from dengue. | 715 (48.2) | 768 (51.8) | 53.32 *** | |
| 5. If a patient has a high fever for 2–7 days, nausea, vomiting, and possible abdominal pain, the patient is in the fever stage. | 555 (45.8) | 657 (54.2) | 60.47 *** | |
| 6. If a patient with dengue hemorrhagic fever presents pain at the right lower costal margin, they are showing signs of hepatomegaly. | 442 (38.4) | 709 (61.6) | 234.84 *** | |
| 7. If a patient with dengue hemorrhagic fever presents signs of shock from leakage of plasma, they will have poor tissue perfusion, weak pulse, and narrowed pulse pressure. | 648 (47.4) | 719 (52.6) | 51.88 *** | |
| 8. If your neighbor presents signs of poor tissue perfusion, weak pulse, and clammy skin, you need to send them to hospital. | 720 (49.5) | 735 (50.5) | 21.83 *** | |
| 9. Dengue patients should avoid consuming aspirin or non-steroidal anti-inflammatory drugs because they may cause gastritis and subsequent massive gastrointestinal or hepatic injury. | 331 (38.4) | 530 (61.6) | 124.57 *** | |
| 10. If your neighbor presents high fever on day 1, you give one paracetamol every 6 h and a tepid sponge bath. | 585 (47.2) | 655 (52.8) | 39.69 *** | |
| Total | Poor level (cut-off point < 8) | 628 (70.4) | 268 (29.6) | 0.000 *** |
| Good level (cut-off point ≥ 8) | 304 (33.9) | 592 (66.1) | ||
| Family Leaders’ ULISS | Correct Response n (%) | |||
|---|---|---|---|---|
| Before (n = 932) | After (n = 856) | |||
| 1. The number of larvae of female Aedes Aegypti in the area is indicated by larval indices. | 386 (42.3) | 527 (57.7) | 72.49 *** | |
| 2. Through the container index (CI), the value for identifying a dengue outbreak is calculated. Then, the number of water containers and the number of water containers infested with larvae are surveyed. | 274 (40.8) | 398 (59.2) | 55.59 *** | |
| 3. The participation of family leaders in the survey for larval indices in and out of the household every 7 days is key. | 546 (44.5) | 680 (55.5) | 90.05 *** | |
| 4. Insecticide Temephos sand granulates may be used to eliminate larvae but not to eliminate mosquito eggs. | 41 (9.6) | 388 (90.4) | 409.85 *** | |
| 5. You suggest the use of lotion in the neighborhood as a prevention of mosquito bites. | 465 (41.5) | 656 (58.5) | 136.44 *** | |
| 6. If people in the village have dengue, you suggest for all to prevent dengue by eliminating mosquito breeding sites and endeavoring to diminish the scores for the larval indices around the house. | 739 (49.6) | 752 (50.4) | 23.60 *** | |
| 7. You suggest eliminating mosquito larvae by cleansing and scrubbing the edge of the container over the area that used to have water. | 192 (30.8) | 431 (69.2) | 173.94 *** | |
| 8. You suggest putting the water container upside down until the larvae can be seen. You also check the container again, considering that the lifespan of a mosquito egg is 1–5 years. | 195 (27.3) | 520 (72.7) | 294.89 *** | |
| 9. If the water container capacity is 100 L, we can use red lime in the container. | 180 (23.9) | 574 (76.1) | 417.04 *** | |
| 10. The larval indices surveillance system must be documented on the 25th of every month in the “Violet book”. | 548 (42.8) | 732 (57.2) | 157.79 *** | |
| Total | Poor level (cut-off point < 8) | 916 (64.2) | 511 (35.8) | 0.000 *** |
| Good level (cut-off point ≥ 8) | 16 (4.4) | 345 (95.6) | ||
| Student Leaders’ UDS | Correct Response n (%) | |||
|---|---|---|---|---|
| Before (n = 59) | After (n = 59) | |||
| 1. If a patient has a high fever for 2 to 7 days, petechiae, and a painful enlargement of the liver, the patient is showing signs of dengue infection. | 54 (48.6) | 57 (51.4) | 1.37 ns | |
| 2. If the patient presents signs and symptoms of dengue, then the patient is showing signs of a dengue viral infection. | 50 (49.5) | 51 (50.5) | 0.07 ns | |
| 3. If a person living in a high dengue risk area is infected with one dengue serotype, they may have lifelong immunity to that strain. However, they would still be vulnerable to other serotypes and could, thus, be infected with the other dengue serotypes later in life. | 32 (38.6) | 51 (61.4) | 14.66 *** | |
| 4. If a patient is protected from female Aedes aegypti bites, they will be safe from dengue. | 58 (50.0) | 58 (50.0) | 0.00 ns | |
| 5. If a patient has a high fever for 2–7 days, nausea, vomiting, and possible abdominal pain, the patient is in the fever stage. | 35 (42.7) | 47 (57.3) | 5.76 * | |
| 6. If a patient with dengue hemorrhagic fever presents pain at the right lower costal margin, they are showing signs of hepatomegaly. | 32 (38.1) | 52 (61.9) | 16.53 *** | |
| 7. If a patient with dengue hemorrhagic fever presents signs of shock from leakage of plasma, they will have poor tissue perfusion, weak pulse, and narrowed pulse pressure. | 35 (40.2) | 52 (59.8) | 12.64 *** | |
| 8. If your neighbor presents signs of poor tissue perfusion, weak pulse, and clammy skin, you need to send them to hospital. | 44 (44.0) | 56 (56.0) | 9.44 ** | |
| 9. Dengue patients should avoid consuming aspirin or non-steroidal anti-inflammatory drugs because they may cause gastritis and subsequent massive gastrointestinal or hepatic injury. | 16 (26.7) | 44 (73.3) | 26.58 *** | |
| 10. If your neighbor presents high fever on day 1, you give one paracetamol every 6 hr and a tepid sponge bath. | 24 (33.8) | 47 (66.2) | 18.71 *** | |
| Total | Poor level (cut-off point < 8) | 45 (77.6) | 13 (22.4) | 0.000 *** |
| Good level (cut-off point ≥ 8) | 14 (23.3) | 46 (76.7) | ||
| Student Leaders’ ULISS | Correct Response n (%) (n = 59) | |||
|---|---|---|---|---|
| Before | After | |||
| 1. The number of larvae of female Aedes aegypti in the areas are indicated by the larval indices. | 24 (44.4) | 30 (55.6) | 1.23 ns | |
| 2. Through the container index (CI), the value for identifying a dengue outbreak is calculated. Then, the number of water containers and the number of water containers infested with larvae are surveyed. | 18 (37.5) | 30 (62.5) | 5.06 * | |
| 3. The participation of family leaders in the survey for larval indices in and out of the household every 7 days is key. | 20 (26.0) | 57 (74.0) | 51.17 *** | |
| 4. Insecticide temephos sand granulates may be used to eliminate larvae, but not to eliminate mosquito eggs. | 8 (17.8) | 37 (82.2) | 30.21 *** | |
| 5. You suggest the use of lotion in the neighborhood as a prevention of mosquito bites. | 31 (38.8) | 49 (61.3) | 12.58 *** | |
| 6. If people in the village have dengue, you suggest for all to prevent dengue by eliminating mosquito breeding sites and endeavoring to diminish the scores for the larval indices around the house. | 44 (47.8) | 48 (52.2) | 0.79 ns | |
| 7. You suggest eliminating mosquito larvae by cleansing and scrubbing the edge of the container over the area that used to have water. | 3 (6.0) | 47 (94.0) | 67.19 *** | |
| 8. You suggest putting the water container upside down until the larvae can be seen. You also check the container again, considering that the lifespan of a mosquito is 1–5 years. | 7 (13.2) | 46 (86.8) | 52.10 *** | |
| 9. If the water container capacity is 100 L, we can use red lime in the container. | 4 (6.8) | 55 (93.2) | 88.17 *** | |
| 10. The larval indices surveillance system must be documented on the 25th of every month in the “Violet book”. | 20 (27.4) | 53 (72.6) | 39.12 *** | |
| Total | Poor level (cut-off point < 8) | 59 (73.8) | 21 (26.3) | 0.000 ***, a |
| Good level (cut-off point ≥ 8) | 0 (0.0) | 38 (100.0) | ||
| Village | RDV Scores | Total Stakeholders | Before (June 2020) | After (August 2020) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Household (N = 2372) | People (N = 7068) | VHVs (N = 134) | Head of Zone (N = 30) | Head of Village (N = 10) | ||||||||
| BI | HI | CI | BI | HI | CI | |||||||
| V1 | 15 * | 316 | 891 | 11 | 2 | 1 | 54.21 | 24.77 | 7.93 | 14.88 | 0.93 | 2.15 |
| V2 | 14 * | 287 | 795 | 12 | 3 | 1 | 82.45 | 40.43 | 8.47 | 30.27 | 24.32 | 3.71 |
| V3 | 20 ** | 253 | 751 | 18 | 3 | 1 | 37.18 | 41.67 | 11.94 | 53.21 | 28.85 | 6.06 |
| V4 | 20 ** | 312 | 1069 | 19 | 4 | 1 | 154.37 | 49.5 | 15.27 | 52.94 | 22.17 | 5.63 |
| V5 | 14 * | 294 | 715 | 15 | 5 | 1 | 112.46 | 48.15 | 12.93 | 25.82 | 1.1 | 3.61 |
| V6 | 20 ** | 233 | 756 | 16 | 4 | 1 | 49.71 | 25.73 | 6.15 | 8.77 | 21.64 | 1 |
| V7 | 16 * | 195 | 673 | 12 | 2 | 1 | 340.13 | 77.71 | 25.09 | 85.44 | 40.51 | 6.59 |
| V8 | 18 ** | 154 | 482 | 13 | 3 | 1 | 70.43 | 34.78 | 5.93 | 3.48 | 3.48 | 0.35 |
| V9 | 12 * | 168 | 442 | 9 | 2 | 1 | 103.42 | 41.88 | 8.28 | 29.06 | 23.93 | 2.8 |
| V10 | 12 * | 160 | 494 | 9 | 2 | 1 | 134.21 | 51.75 | 13.73 | 39.66 | 20.69 | 4.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nontapet, O.; Jaroenpool, J.; Maneerattanasa, S.; Thongchan, S.; Ponprasert, C.; Khammaneechan, P.; Le, C.N.; Chutipattana, N.; Suwanbamrung, C. Effects of the Developing and Using a Model to Predict Dengue Risk Villages Based on Subdistrict Administrative Organization in Southern Thailand. Int. J. Environ. Res. Public Health 2022, 19, 11989. https://doi.org/10.3390/ijerph191911989
Nontapet O, Jaroenpool J, Maneerattanasa S, Thongchan S, Ponprasert C, Khammaneechan P, Le CN, Chutipattana N, Suwanbamrung C. Effects of the Developing and Using a Model to Predict Dengue Risk Villages Based on Subdistrict Administrative Organization in Southern Thailand. International Journal of Environmental Research and Public Health. 2022; 19(19):11989. https://doi.org/10.3390/ijerph191911989
Chicago/Turabian StyleNontapet, Orratai, Jiraporn Jaroenpool, Sarunya Maneerattanasa, Supaporn Thongchan, Chumpron Ponprasert, Patthanasak Khammaneechan, Cua Ngoc Le, Nirachon Chutipattana, and Charuai Suwanbamrung. 2022. "Effects of the Developing and Using a Model to Predict Dengue Risk Villages Based on Subdistrict Administrative Organization in Southern Thailand" International Journal of Environmental Research and Public Health 19, no. 19: 11989. https://doi.org/10.3390/ijerph191911989
APA StyleNontapet, O., Jaroenpool, J., Maneerattanasa, S., Thongchan, S., Ponprasert, C., Khammaneechan, P., Le, C. N., Chutipattana, N., & Suwanbamrung, C. (2022). Effects of the Developing and Using a Model to Predict Dengue Risk Villages Based on Subdistrict Administrative Organization in Southern Thailand. International Journal of Environmental Research and Public Health, 19(19), 11989. https://doi.org/10.3390/ijerph191911989