
Exploration of Multilevel Barriers and Strategies That Affected Early COVID-19 Vaccination and Testing in Rural Latino Communities in Southwest Florida

 , , and
, , and 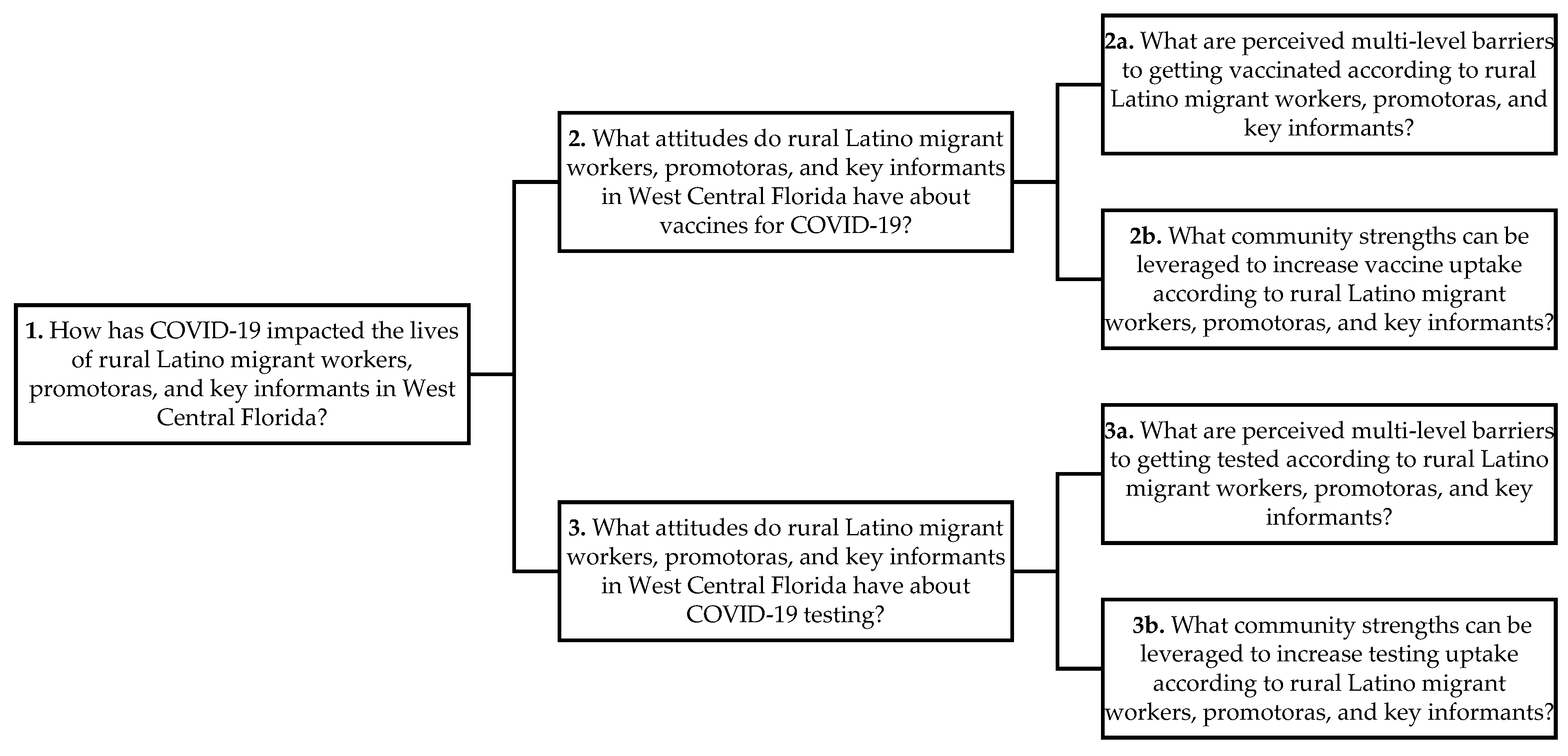{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Questions, Study Design, Setting, and Participants
2.2. Analysis
3. Results
3.1. Barriers
People believe, as [she] says, that when they go to a hospital, when they see the doctor, they’re too afraid. They’ve called me and said, “I’m very ill. I’m breathing badly”. I’ve said, “Please go see a doctor. This is an emergency. Call 911”. They say, “No, no, because if I go to the hospital, I’m going to die, and my family won’t even be able to say goodbye to me”.—Promotora
That’s the number one concern that they’re not going to have anyone there. That they’re going to die alone and that the only thing their families are going to be given are their remains. People have that fear. That’s their fear when they get COVID. These are the concerns that I’ve seen and that they’ve called me about. Because unfortunately, every day, more and more people die of COVID. It’s dramatic not to say goodbye to your family. That’s the worst thing that can happen.—Promotora
Because there are so many rumors, so many things that have been said. Lately, some people were saying that they were giving them water, that they weren’t giving them anything. All that caused a little bit of fear. Another thing is, sometimes, you don’t know. Since they’re just coming out, we don’t know exactly what the consequences of the vaccine will be. Well, right now, they came out with a new dose. Everything is news and news, and honestly, you never know what’s true. They took it off the market because of what was happening, and that’s why sometimes, you have a little fear. When I went to get the vaccine, when I saw that the man already had the syringes ready. I didn’t see where he got it from, whether he really took it from the vaccine, or I don’t know what he put in me. Do you understand my fear? Because they’re not showing you, “Look, this is where I’m taking it from”.—Community member
Well, they wanted to go out and because they needed it at work. There were entire trailer communities with the virus. It was very sad because they didn’t know where to get it done. They were a little afraid and didn’t want to know they had the virus. They felt that rejection of, “If I say I have the virus, I’ll be rejected”. They didn’t want to say it.—Promotora
So, I think, in our population, it’s more the fear of having to present documentation to get their vaccination. So, am I going to be asked to have an ID, or a birth certificate, or something like that? So, that’s the same reason they’re—they don’t come to schools and want to enroll their children is because they don’t have that documentation.—Community member
They’re afraid immigration will find out. That’s why they don’t even want to register the kids in school because they’re fearful that immigration will get the information. They don’t want to register their information for the vaccinations. That’s what (name redacted) said at the very beginning.—Key Informant
I mean, they don’t have access to the technology, so you have to do that face to face, and you have to go and meet them in their home, so you have to help them. And if there was—we were being told we couldn’t go anywhere, yet we were asking the parents to have this technology available. So, it was very frustrating, and to this day, it still is very frustrating because we make a lot of assumptions that our parents are ready to handle all this, and they’re not. Through no fault of their own. It’s just it’s kind of like a vicious circle, but going back to the positive, it’s at least now we know what we didn’t know. So, how we handle it in the future is a game-changer, and we can’t just sit and cross our arms and do nothing. It’s everybody’s responsibility to fix it.—Community member
If a child is sick or showing any symptoms of anything, they go down to the clinic; parents have to pick them up. They cannot come back to school until they’ve had this COVID test, right? So, you’re hoping for a fast COVID test that the parent has access to, but not all the parents have access to these fast COVID tests because the idea is if the child comes up positive, then you’ve got to quarantine every child that that child’s been in contact with, which has been—had a huge impact this school year on the days of school that children have missed all across the whole school, and teachers, and everything.—Key informant
Restaurants were closed. Bars were closed. Whereas essential work, such as farm work, which I also do, is essential. You couldn’t stop working. You had to continue. Construction work, which I also do, also couldn’t be stopped. There was social distancing and everything, but you had to continue. Those types of jobs were essential. Government work, or work in the state health department, wasn’t considered essential. Unfortunately, those people didn’t have any form of income, so it affected them very hard.—Key informant
At work, I never saw a case like that. In the case of my daughter, who works at Amazon, they told her that, since she tested positive, she had to stay home for a month. They only paid her for one week. The other weeks, she didn’t get paid.—Community member
I worked with a family, and the wife was giving me their details, and the husband had a horrible cough. People also told me, “I was cooped up in my home for a month and a half. I have no job”. Someone else told me, “Look, I don’t have the same phone number because I was very sick for three months. I’m better now, but I don’t have anything. I had to start again from scratch.”—Promotora
So, when you’re living day to day and every single paycheck is what you need in order to survive, taking a day off to get your vaccine, and then taking another day off to get your vaccine, and then thinking, “Maybe I’ll get sick, I might need another day off to get the vaccine”, is complicated. It’s not something that they can take lightly. And so, if the vaccines were offered closer to their homes because maybe they don’t even have transportation and they have to get to the source of the vaccine.—Key informant
That’s why they’re giving (vaccines) first to 65-year-olds. That’s what they say. Because they want to exterminate old people, so that they will no longer be in the way. What did a lady tell me? Oh yes, that it’s so that they will no longer have to pay their Social Security or their pensions. That they need to renew the race.—Promotora
The other thing is that everybody will be sterilized because, of course, they don’t want certain populations to keep growing. Matter of fact—and other people they just—they just die, and that’s not being publicized. So, there is quite a bit of bad information out in the different communities, especially the ones that are more isolated than others.—Community member
But yes, what I see mostly, it’s because of fear. When we call them, they are scared. Even the last time we had a gentleman that went in, he was very ill. He didn’t want to get tested because he said that his little boy told him that if he gets tested, they were going to put a chip on his nose. So, I guess it’s miscommunication, the education, and the fear.—Community member
Because they’re afraid due to misinformation, I think. They have to be educated on it to get rid of all those myths that they have and all the beliefs. As [she] says, technology is overtaking us, so everything you see on Facebook, everything you see is that they’re going to steal our DNA, and this, and that.—Promotora
Access, access, access because whether it is exactly what you say, and yes, I have family, and I know how much they struggle to get their own, and that’s why every single time I’m like, “And we expect our farmworkers to go online and have on their little phone, and they put in a program or something so that you can eventually get it”. It is very unrealistic, so the access to the vaccines was a total failure in Florida, period.—Community member
But for our families, to expect them to be able to access, to register, and get in, is very complicated for them. And to set up those appointments. It’s not simple. And it’s time-consuming. And it’s just what they don’t have. They need a more ease of access. So, that’s one more thing that has prevented them from getting their vaccination.—Community member
…It was not easy to find a place and find an appointment. We wanted the rapid test because I wanted to be able to come back to work. It was right around Christmas time, and to find the rapid test was—I mean, I had to get up at like three in the morning and go stand in line or wait in my car and just pray to God that I got a test, and I didn’t want to wait for three days, so I was very—I and my entire family, we were very frustrated because I’m very tech-savvy. I can find anything on the internet, but it was not easy for me. So, it’s hard. It’s not easy.—Community member
They don’t have transportation, so I think that would be good. For the country or the state to do something like have healthcare workers go from house to house, knocking on doors.—Promotora
Only people over 65 who are residents of Florida have been able to get it. For those who are here, for example, and who stayed because they couldn’t travel due to COVID, they don’t have an ID, or they’re not Florida residents, or they don’t have a phone bill, electric bill, anything. They lack proof that they’re Florida residents. They haven’t been able to get it. Immigrants haven’t been able to get it because I’ve called. Those who don’t have papers.—Promotora
It’s very hard for them to do anything, and they do not. Their employers are not willing to give them check stubs. They’re here undocumented. They don’t have social security numbers. They’re working under the table. So, most of our Mexican families are moving along, but this huge population that’s coming in, and I mean it’s big, and it’s growing. It is really a place where we need to provide a lot of support.—Community member
And national guard soldiers. They’re not holding guns or anything like that, but they’re—it’s a big presence. So, they’re not—so, when you do these community events, I understand you have to have law enforcement, but do they have to be in full-fledged uniform because my families will shy away from that. I’m hoping that changes with the changes with what’s kind of changing right now. We’re going—I don’t want to get political, but that’s where I’m going.—Community member
What’s the business, then? The fact that the free places where they’re being done make you go somewhere else, where they charge you 150 dollars. Then, it turns out that your test is negative. That’s a huge point because here, everything is a business, in my opinion”.—Promotora
Whatever or whoever they are, and I met with every person that I could with the CEOs, and the this, and the that, and they all had their good excuses. And all across the state, I’m not going to say just here, I’m saying all across the state was the same resources, resources, resources. And I’m like, “But hey, you’re getting federal dollars for migrants”, and but they still were never on their list.—Community member
3.2. Strategies
Injection, and for many, I think it’s a light at the end of the tunnel, right? To hear about a vaccine for this disease, it’s a light at the end of the tunnel for many. Also, for many, I think that the community is among those who fear side effects from the vaccine and everything. There’s rumors, and a lot of people don’t want to be vaccinated, but in terms of the vaccine itself, it’s a light at the end of the tunnel.—Key informant
There’s a lot of pain, but we’re here, and we have hope with the vaccine. We say that even if we’re vaccinated, we’ll still wear our masks and everything. I hope we’ll be a little calmer now, though, because we believe that now, we’re a little more protected.—Promotora
It’s very hard to hear all that because we’re used to working with our people. We feel for them and their situations, and it’s very hard for us to give them what we used to give them. Sometimes, that’s so important. She and I used to work together a lot, and sometimes, people came to us crying, and we would hug them. Now, we can’t have that contact where they’re crying, and we hug them and tell them that we’ll pray for them.—Promotora
…There’s very little, let’s say, culture in terms of self-care. COVID has taught us through that vulnerability that infections, diseases, obesity, a lot of problems that humanity faces, will never be addressed or treated. Now, with the emergence of COVID, people are worrying more so about themselves, taking care of themselves, protecting themselves. How many infections are around us? It’s not the first time that it exists. There have been a lot of types of diseases, even when H1N1 came out, there was a controversy that was maybe the closest thing we’ve had to face.—Promotora
I can’t tell you that I saw them doing anything. A lot of people that I saw in the community made food to sell in the office or on street corners. Maybe to take it to the farm workers. They cleaned houses. Anything. Garage sales. No one wanted to be close to anyone else because of hygiene, but they created their own source of work. Whatever they could do.—Key informant
Older people who decided not to go to the hospital and spent time at home looking for herbs. I’m telling you, they ran out of all the herbs that people use. You couldn’t find them in any store. People were practically trafficking those little herbs and ginger. All that had run out. There wasn’t any in any store.—Promotora
COVID has caused for a lot of different agencies and communities to come together and really start figuring out or start voicing our concerns and really focusing on what are our rights as—not even as citizens, as human beings.—Community member
Families went, and they didn’t have the ID; they were not tested. And this is when they were in some of those locations that were safe places for them to go, so which is why, and, again, I do plan to go and—because I want to know what it is they’re requiring or not.—Community member
COVID has a lot of negative impacts, but it also has—it’s like the slingshot that has pushed us in the right direction. So, I love hearing all this conversation because we all represent different communities or different agencies, and I’m—I think we’re going to start seeing some changes, and people really noticing that, yes, our essential workers, even the most marginalized of populations, we really get—they got tossed aside.—Community member
In my eyes, COVID has put a very strong light on the inequities that our Latinos and especially our migrant population is going—so, it’s not—to me, it’s a positive because I am getting more traction with even within our school system. I’m getting more traction on issues that have plagued our families for forever. I’ve been an educator for [decades] all here in Hillsborough County, and I’ve always been with the migrant—supporting the migrant population in one way or form, but—so, COVID has really provided a venue for our voices to be heard.—Community member
We have taken on finding vaccinations for our families because that has been a nightmare in this state. I’m sure everybody knows that. But we have been able to, a trickle at a time, get some of those vaccines out into the rural communities and some out into the fields. And, as of today, hopefully, with this new change that, they will not be requiring certain information. We are really hoping that more families can be vaccinated. If somebody chooses not to do it, that’s okay, but we just want to make sure that the opportunity is there, and so far, most of our families have been wide open.—Community member
I, personally, have helped several senior citizens make appointments because they don’t know how to really speak up for themselves. I’ve helped them, and some of them, I haven’t been able to get an appointment for. I register them. I call a line. I register them. I give them my phone number. They call me, and then they’re registered. Well, they call me and ask me for all the information.—Promotora
It’s been very rough. No one expected this. Everything completely collapsed in a very bad way. At the same time, there were also beautiful things. More family time. Being closer to my family and children. Maybe before, we’d leave for work, and we didn’t see each other. We didn’t sit down at the table or anything. Now, with COVID, we became closer as a family.—Key informant
I see the positive side of COVID. It’s brought a lot of bad things, but it’s also generated positive things. Family time let’s say. We also have an approach to information technology, and that has allowed us to spend more time with our family. We’ve also started working from home because a lot of mothers need to work from home to take care of their children. Fathers, too. We have to see the positive side as well, I think.—Promotora
I had two jobs. I worked in a church. I worked at a restaurant, and on Wednesdays, I worked in a church. Then, I lost that job during the pandemic. Now, I don’t know when they’re going to open again. I said, “Wow, how am I going to make it?” I have three children. My husband doesn’t work. I said, “No.” I started doing what I had to do.—Key informant
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Spencer, H.; Rusek, M.; Anderson, J.; Veazie, S.; et al. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths: A Systematic Review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef] [PubMed]
- E Hayward, S.; Deal, A.; Cheng, C.; Crawshaw, A.; Orcutt, M.; Vandrevala, T.F.; Norredam, M.; Carballo, M.; Ciftci, Y.; Requena-Méndez, A.; et al. Clinical outcomes and risk factors for COVID-19 among migrant populations in high-income countries: A systematic review. J. Migr. Health 2021, 3, 100041. [Google Scholar] [CrossRef] [PubMed]
- Gil, R.M.; Marcelin, J.R.; Zuniga-Blanco, B.; Marquez, C.; Mathew, T.; A Piggott, D. COVID-19 Pandemic: Disparate Health Impact on the Hispanic/Latinx Population in the United States. J. Infect. Dis. 2020, 222, 1592–1595. [Google Scholar]
- Hawkins, D. Differential occupational risk for COVID-19 and other infection exposure according to race and ethnicity. Am. J. Ind. Med. 2020, 63, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Pathak, E.B.; Menard, J.M.; Garcia, R.B.; Salemi, J.L. Joint Effects of Socioeconomic Position, Race/Ethnicity, and Gender on COVID-19 Mortality among Working-Age Adults in the United States. Int. J. Environ. Res. Public Health 2022, 19, 5479. [Google Scholar] [CrossRef] [PubMed]
- Thakur, N.; Lovinsky-Desir, S.; Bime, C.; Wisnivesky, J.P.; Celedón, J.C. The Structural and Social Determinants of the Racial/Ethnic Disparities in the U.S. COVID-19 Pandemic. What’s Our Role? Am. J. Respir. Crit. Care Med. 2020, 202, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Long, A.S.; Hanlon, A.L.; Pellegrin, K.L. Socioeconomic variables explain rural disparities in US mortality rates: Implications for rural health research and policy. SSM Popul. Health 2018, 6, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- McFadden, S.M.; Demeke, J.; Dada, D.; Wilton, L.; Wang, M.; Vlahov, D.; Nelson, L.E. Confidence and Hesitancy During the Early Roll-out of COVID-19 Vaccines Among Black, Hispanic, and Undocumented Immigrant Communities: A Review. J. Urban Health 2022, 99, 3–14. [Google Scholar] [CrossRef]
- Garcini, L.M.; Pham, T.T.; Bs, A.M.A.; Lill, S.; Tsevat, J.; Garcini, M.L.M.; Ma, S.L.; Tsevat, M.J. COVID-19 diagnostic testing among underserved Latino communities: Barriers and facilitators. Health Soc. Care Community 2021, 30, e1907–e1916. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Risk for COVID-19 Infection, Hospitalization, and Death By Race/Ethnicity. 17 June 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 13 June 2022).
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Balasuriya, L.; Santilli, A.; Morone, J.; Ainooson, J.; Roy, B.; Njoku, A.; Mendiola-Iparraguirre, A.; Duffany, K.O.; Macklin, B.; Higginbottom, J.; et al. COVID-19 Vaccine Acceptance and Access Among Black and Latinx Communities. JAMA Netw. Open 2021, 4, e2128575. [Google Scholar] [CrossRef]
- United States Census Bureau. QuickFacts: Florida. 2021. Available online: https://www.census.gov/quickfacts/fact/table/FL/BZA210219 (accessed on 24 May 2022).
- The COVID Tracking Project. Florida: All Race & Ethnicity Data. 2021. Available online: https://covidtracking.com/data/state/florida/race-ethnicity (accessed on 24 May 2022).
- Florida Department of Health. Latest Vaccine Updates. 2022. Available online: https://floridahealthcovid19.gov/latest-vaccine-updates/ (accessed on 24 May 2022).
- Florida Department of Health, Public Health Advisory. Rescission of Prior COVID-19 Public Health Advisories, Eligibility for COVID-19 Vaccines, Resuming in-Person Government Services; Florida Department of Health: Tallahassee, FL, USA, 2021.
- Cáceres, N.A.; Shirazipour, C.H.; Herrera, E.; Figueiredo, J.C.; Salvy, S.-J. Exploring Latino Promotores/a de Salud (Community Health Workers) knowledge, attitudes, and perceptions of COVID-19 vaccines. SSM Qual. Res. Health 2022, 2, 100033. [Google Scholar] [CrossRef] [PubMed]
- Krueger, R.A.C.M.A. Focus Groups: A Practical Guide for Applied Research; SAGE: Los Angeles, CA, USA, 2009. [Google Scholar]
- Messias, D.K.H.; Parra-Medina, D.; Sharpe, P.A.; Treviño, L.; Koskan, A.M.; Morales-Campos, D. Promotoras de Salud: Roles, responsibilities, and contributions in a multisite community-based randomized controlled trial. Hisp. Health Care Int. 2013, 11, 62–71. [Google Scholar] [CrossRef]
- Stokols, D. Establishing and maintaining healthy environments: Toward a social ecology of health promotion. Am. Psychol. 1992, 47, 6–22. [Google Scholar] [CrossRef] [PubMed]
- Moyce, S.; Velazquez, M.; Claudio, D.; Thompson, S.; Metcalf, M.; Aghbashian, E.; Vanderwood, K.; Sisson, N. Exploring a rural Latino community’s perception of the COVID-19 pandemic. Ethn. Health 2021, 26, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Burke, P.F.; Masters, D.; Massey, G. Enablers and barriers to COVID-19 vaccine uptake: An international study of perceptions and intentions. Vaccine 2021, 39, 5116–5128. [Google Scholar] [CrossRef] [PubMed]
- Salinas, J.; Salinas, M. Systemic Racism and Undocumented Latino Migrant Laborers during COVID-19: A Narrative Review and Implications for Improving Occupational Health. J. Migr. Health 2022, 5, 100106. [Google Scholar] [CrossRef]
- Demeke, J.; McFadden, S.M.; Dada, D.; Djiometio, J.N.; Vlahov, D.; Wilton, L.; Wang, M.; Nelson, L.E. Strategies that Promote Equity in COVID-19 Vaccine Uptake for Undocumented Immigrants: A Review. J. Community Health 2022, 47, 554–562. [Google Scholar] [CrossRef]
- Rothe, E.M.; Fortuna, L.R.; Tobon, A.L.; Postlethwaite, A.; Sanchez-Lacay, J.A.; Anglero-Diaz, Y.L. Structural Inequities and the Impact of COVID-19 on Latinx Children: Implications for Child and Adolescent Mental Health Practice. J. Am. Acad. Child. Adolesc. Psychiatry 2021, 60, 669–671. [Google Scholar] [CrossRef]
- DeHaven, M.J.; Hunter, I.B.; Wilder, L.; Walton, J.W.; Berry, J. Health programs in faith-based organizations: Are they effective? Am. J. Public Health 2004, 94, 1030–1036. [Google Scholar] [CrossRef]
- Alsan, M.; Stanford, F.C.; Banerjee, A.; Breza, E.; Chandrasekhar, A.G.; Eichmeyer, S.; Goldsmith-Pinkham, P.; Ogbu-Nwobodo, L.; Olken, B.A.; Torres, C.; et al. Comparison of Knowledge and Information-Seeking Behavior After General COVID-19 Public Health Messages and Messages Tailored for Black and Latinx Communities: A Randomized Controlled Trial. Ann. Intern. Med. 2021, 174, 484–492. [Google Scholar] [CrossRef]
- Figueroa, C.M.; Medvin, A.; Phrathep, B.D.; Thomas, C.W.; Ortiz, J.; Bushy, A. Healthcare Needs of U.S. Rural Latinos: A Growing, Multicultural Population. Online J. Rural. Nurs. Health Care Off. J. Rural. Nurse Organ. 2021, 21, 24–48. [Google Scholar] [CrossRef] [PubMed]
- Boen, C.E.; Hummer, R.A. Longer-but Harder-Lives?: The Hispanic Health Paradox and the Social Determinants of Racial, Ethnic, and Immigrant-Native Health Disparities from Midlife through Late Life. J. Health Soc. Behav. 2019, 60, 434–452. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buro, A.W.; Roman Candelaria, K.; Bailey, R.; Luna, F.; Albizu-Jacob, A.; Stern, M.; Redwine, L. Exploration of Multilevel Barriers and Strategies That Affected Early COVID-19 Vaccination and Testing in Rural Latino Communities in Southwest Florida. Int. J. Environ. Res. Public Health 2022, 19, 11785. https://doi.org/10.3390/ijerph191811785
Buro AW, Roman Candelaria K, Bailey R, Luna F, Albizu-Jacob A, Stern M, Redwine L. Exploration of Multilevel Barriers and Strategies That Affected Early COVID-19 Vaccination and Testing in Rural Latino Communities in Southwest Florida. International Journal of Environmental Research and Public Health. 2022; 19(18):11785. https://doi.org/10.3390/ijerph191811785
Chicago/Turabian StyleBuro, Acadia W., Kevin Roman Candelaria, Rocio Bailey, Frances Luna, Alexandra Albizu-Jacob, Marilyn Stern, and Laura Redwine. 2022. "Exploration of Multilevel Barriers and Strategies That Affected Early COVID-19 Vaccination and Testing in Rural Latino Communities in Southwest Florida" International Journal of Environmental Research and Public Health 19, no. 18: 11785. https://doi.org/10.3390/ijerph191811785
APA StyleBuro, A. W., Roman Candelaria, K., Bailey, R., Luna, F., Albizu-Jacob, A., Stern, M., & Redwine, L. (2022). Exploration of Multilevel Barriers and Strategies That Affected Early COVID-19 Vaccination and Testing in Rural Latino Communities in Southwest Florida. International Journal of Environmental Research and Public Health, 19(18), 11785. https://doi.org/10.3390/ijerph191811785