

Oral-Health-Related Quality of Life in Patients with Medication-Related Osteonecrosis of the Jaw: A Prospective Clinical Study

 , , ,
, , , 
Abstract
:1. Introduction
- (I)
- Stages I and II MRONJ and its successful therapy predict no improvement of OHRQoL
- (II)
- MRONJ-associated parameters do not affect OHRQoL.
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
- (I)
- Total: included the entire patient sample
- (II)
- Stage: clinical stages I and II
- (III)
- Pain: presence (yes) or absence (no) of pain
- (IV)
- Primary disease: the disease for which MRONJ-related drugs were used. These were divided into two groups: osteoporosis and malignoma. Malignoma included multiple myeloma and breast, lung, prostate, renal cell, thyroid, and gastric carcinomas.
- (V)
- Risk evaluation: risk was evaluated according to drug intake. A low-risk group (Prolia/denosumab, 60 mg, subcutaneous administration every 6 months and alendronate, 70 mg, oral application once a week) was compared with a high-risk group (Xgeva/denosumab, 120 mg, subcutaneous application every 4 weeks and zoledronate, 4 mg, intravenous administration every 4 weeks)
- (VI)
- Duration of intake: was categorized into short (≤36 months) and long (>36 months) duration of drug intake
- (VII)
- Defect size: MRONJ-related defects were categorized into small (<2 cm2), medium (≥2 to <4 cm2), and large (≥4 cm2) defects
- (VIII)
- Need for prosthodontics: Patients who needed prosthetic care (yes) were compared with patients who did not need prosthetic treatment (no).
2.3. Questionnaires
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
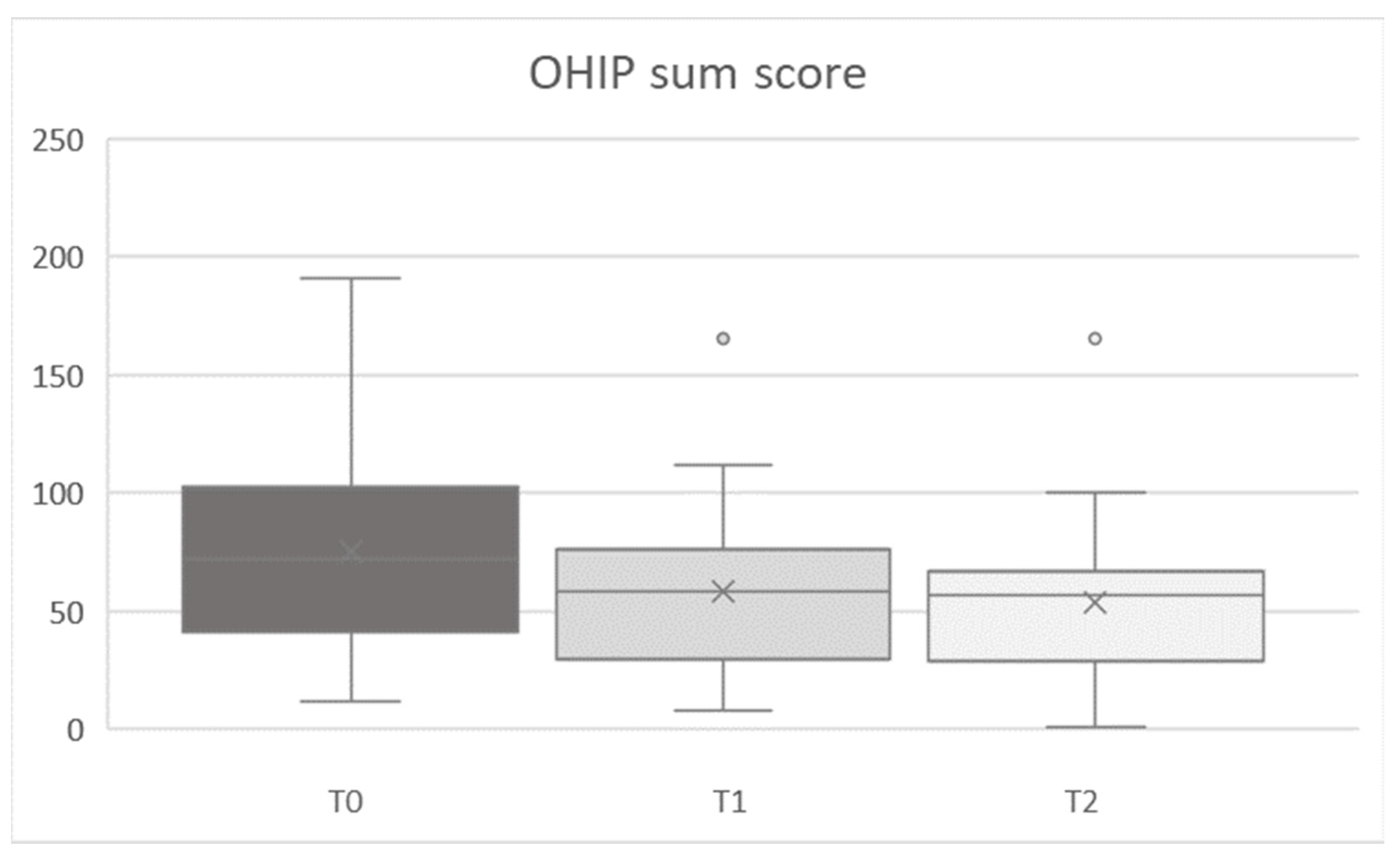
3.2. OHIP Evaluations
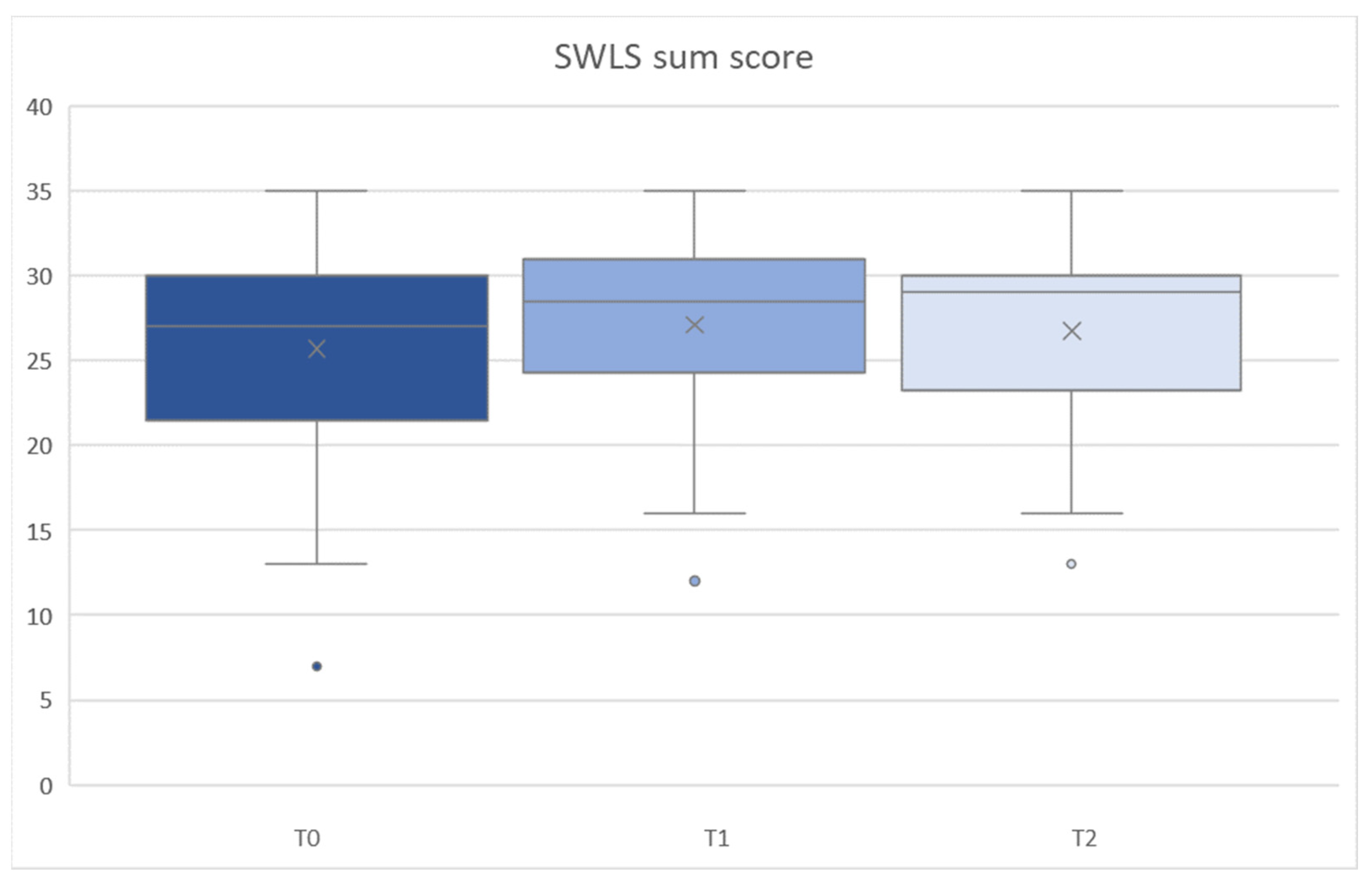
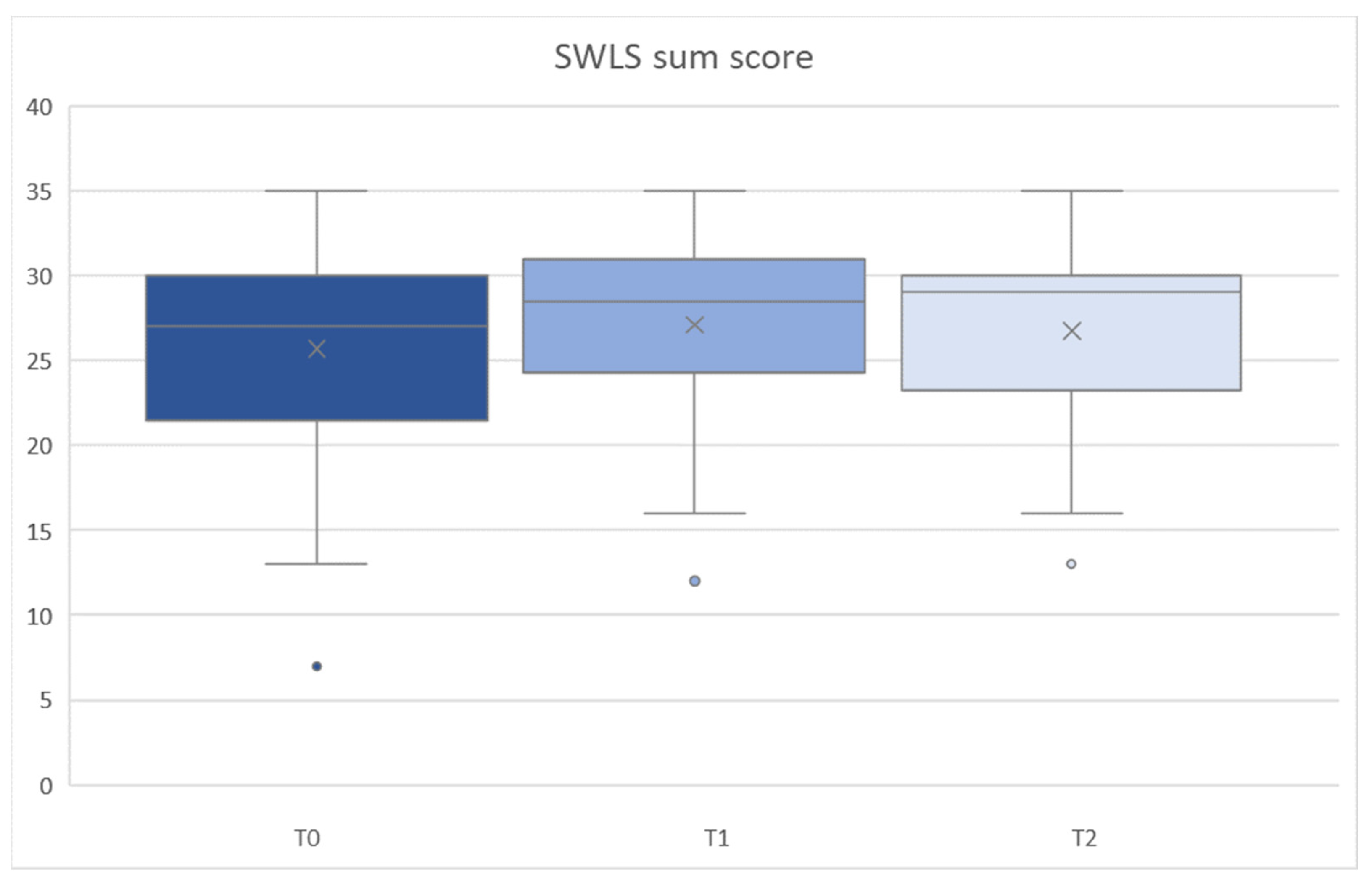
3.3. SWLS Assessment
3.4. VAS 1
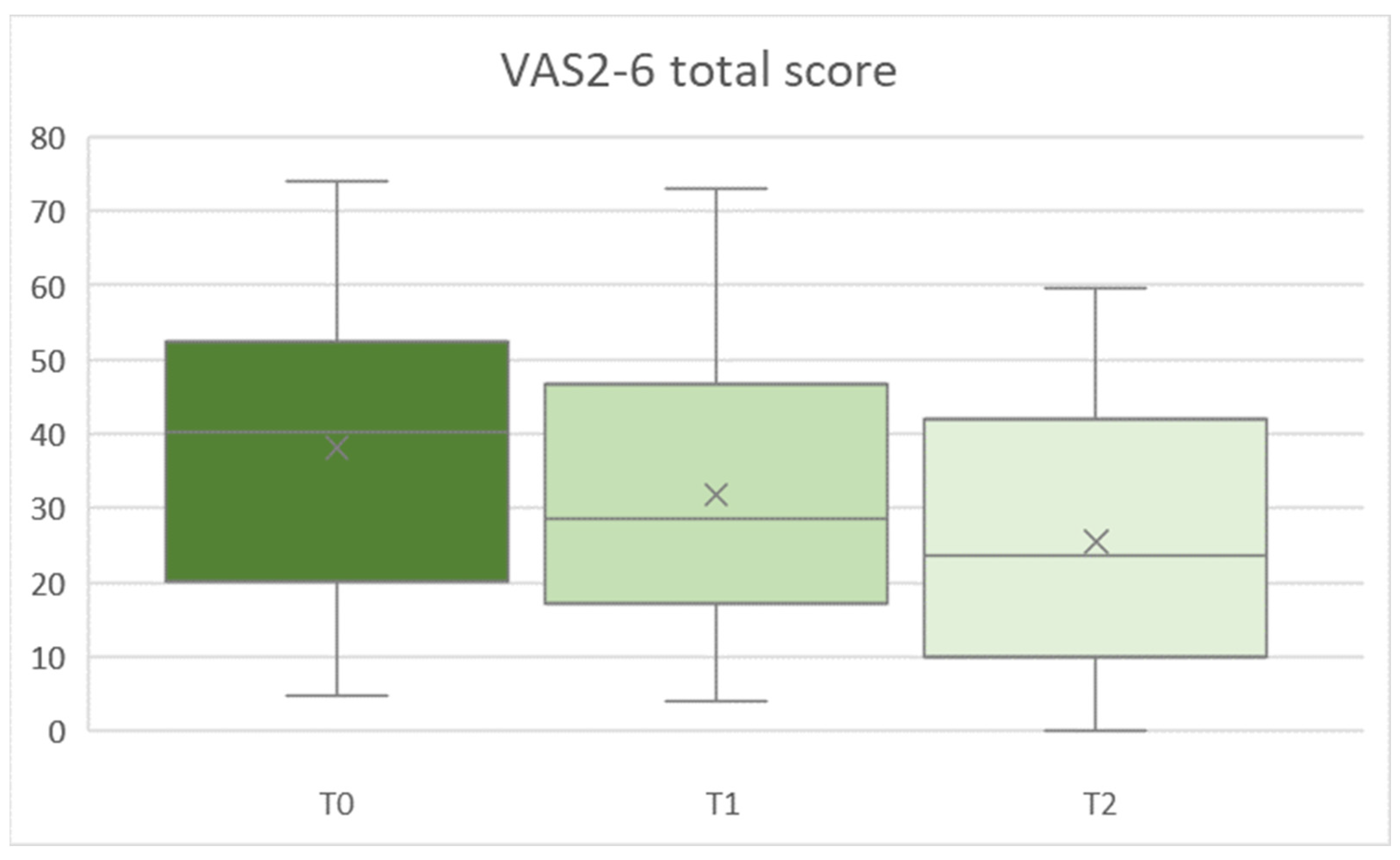
3.5. VAS2-6
3.6. Analysis of Linear Regression
3.7. Internal Consistency
4. Discussion
5. Conclusions
- Considering the impaired OHRQoL due to MRONJ, awareness of MRONJ in dentists and patients should be increased, in order to improve patient compliance, especially in the MRONJ stage “at risk”.
- The present OHIP, SWLS, and VAS findings demonstrated that patients with stage II MRONJ, pain, and larger defects who have taken drugs for a longer time and need prosthetic treatment have greater changes in OHRQoL between baseline and follow-up. This could demonstrate a greater benefit of therapy in these patients. In general, the surgical treatment improved OHRQoL and related parameters. This underscores the benefit of surgical intervention, not only limited to effects on bone and mucosal healing but also in terms of quality of life.
- The impairment of MRONJ patients indicated that prevention, early diagnosis, early therapy, and interdisciplinary treatment might improve outcomes in patients with MRONJ, both in terms of their somatic health and subjective experiences such as OHRQoL.
- The effects of MRONJ treatment affected the seven-domain and four-dimensional scales. In addition, the new four-dimensional OHIP scale revealed additional information about the standard seven-domain structure.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cavalcante, R.C.; Tomasetti, G. Pentoxifylline and tocopherol protocol to treat medication-related osteonecrosis of the jaw: A systematic literature review. J. Craniomaxillofac. Surg. 2020, 48, 1080–1086. [Google Scholar] [CrossRef]
- Hata, H.; Imamachi, K.; Ueda, M.; Matsuzaka, M.; Hiraga, H.; Osanai, T.; Harabayashi, T.; Fujimoto, K.; Oizumi, S.; Takahashi, M.; et al. Prognosis by cancer type and incidence of zoledronic acid-related osteonecrosis of the jaw: A single-center retrospective study. Support. Care Cancer 2022, 30, 4505–4514. [Google Scholar] [CrossRef]
- De Faria, L.P.; Sueyoshi, G.; De Oliveira, T.C.; Holliday, L.S.; Arana-Chavez, V.E. Effects of Alendronate and Dexamethasone on Osteoclast Gene Expression and Bone Resorption in Mouse Marrow Cultures. J. Histochem. Cytochem. 2022, 70, 169–179. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Hirsh, V.; Siena, S.; Henry, D.H.; Woll, P.J.; Manegold, C.; Solal-Celigny, P.; Rodriguez, G.; Krzakowski, M.; Mehta, N.D.; et al. Overall survival improvement in patients with lung cancer and bone metastases treated with denosumab versus zoledronic acid: Subgroup analysis from a randomized phase 3 study. J. Thorac. Oncol. 2012, 7, 1823–1829. [Google Scholar] [CrossRef]
- Dearnaley, D.P.; Mason, M.D.; Parmar, M.K.; Sanders, K.; Sydes, M.R. Adjuvant therapy with oral sodium clodronate in locally advanced and metastatic prostate cancer: Long-term overall survival results from the MRC PR04 and PR05 randomised controlled trials. Lancet Oncol. 2009, 10, 872–876. [Google Scholar] [CrossRef]
- Jakob, T.; Tesfamariam, Y.M.; Macherey, S.; Kuhr, K.; Adams, A.; Monsef, I.; Heidenreich, A.; Skoetz, N. Bisphosphonates or RANK-ligand-inhibitors for men with prostate cancer and bone metastases: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 12, CD013020. [Google Scholar]
- Ali, I.E.; Sumita, Y. Medication-related osteonecrosis of the jaw: Prosthodontic considerations. Jpn. Dent. Sci. Rev. 2022, 58, 9–12. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw--2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- Schoenhof, R.; Munz, A.; Yuan, A.; ElAyouti, A.; Boesmueller, H.; Blumenstock, G.; Reinert, S.; Hoefert, S. Microarchitecture of medication-related osteonecrosis of the jaw (MRONJ); a retrospective micro-CT and morphometric analysis. J. Craniomaxillofac. Surg. 2021, 49, 508–517. [Google Scholar] [CrossRef]
- Diniz-Freitas, M.; Fernández-Feijoo, J.; Diz Dios, P.; Pousa, X.; Limeres, J. Denosumab-related osteonecrosis of the jaw following non-surgical periodontal therapy: A case report. J. Clin. Periodontol. 2018, 45, 570–577. [Google Scholar] [CrossRef]
- Boff, R.C.; Salum, F.G.; Figueiredo, M.A.; Cherubini, K. Important aspects regarding the role of microorganisms in bisphosphonate-related osteonecrosis of the jaws. Arch. Oral Biol. 2014, 59, 790–799. [Google Scholar] [CrossRef]
- Ewald, F.; Wuesthoff, F.; Koehnke, R.; Friedrich, R.E.; Gosau, M.; Smeets, R.; Rohde, H.; Assaf, A.T. Retrospective analysis of bacterial colonization of necrotic bone and antibiotic resistance in 98 patients with medication-related osteonecrosis of the jaw (MRONJ). Clin. Oral Investig. 2021, 25, 2801–2809. [Google Scholar] [CrossRef]
- Kawahara, M.; Kuroshima, S.; Sawase, T. Clinical considerations for medication-related osteonecrosis of the jaw: A comprehensive literature review. Int. J. Implant. Dent. 2021, 7, 47. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Fantasia, J.; Carlson, E. Bisphosphonate-related osteonecrosis of the jaw: Background and guidelines for diagnosis, staging and management. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 433–441. [Google Scholar] [CrossRef]
- Preidl, R.H.M.; Amann, K.; Weber, M.; Schiller, M.; Ringler, M.; Ries, J.; Neukam, F.W.; Kesting, M.; Geppert, C.I.; Wehrhan, F. Lineage-associated connexin 43 expression in bisphosphonate-exposed rat bones. J. Craniomaxillofac. Surg. 2021, 49, 738–747. [Google Scholar] [CrossRef]
- Oteri, G.; Trifirò, G.; Peditto, M.; Lo Presti, L.; Marcianò, I.; Giorgianni, F.; Sultana, J.; Marcianò, A. Treatment of Medication-Related Osteonecrosis of the Jaw and its Impact on a Patient’s Quality of Life: A Single-Center, 10-Year Experience from Southern Italy. Drug Saf. 2018, 41, 111–123. [Google Scholar] [CrossRef]
- Ristow, O.; Rückschloß, T.; Müller, M.; Berger, M.; Kargus, S.; Pautke, C.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Is the conservative non-surgical management of medication-related osteonecrosis of the jaw an appropriate treatment option for early stages? A long-term single-center cohort study. J. Craniomaxillofac. Surg. 2019, 47, 491–499. [Google Scholar] [CrossRef]
- Bacci, C.; Cerrato, A.; Bardhi, E.; Frigo, A.C.; Djaballah, S.A.; Sivolella, S. A retrospective study on the incidence of medication-related osteonecrosis of the jaws (MRONJ) associated with different preventive dental care modalities. Support. Care Cancer 2022, 30, 1723–1729. [Google Scholar] [CrossRef]
- Sischo, L.; Broder, H.L. Oral health-related quality of life: What, why, how, and future implications. J. Dent. Res. 2011, 90, 1264–1270. [Google Scholar] [CrossRef]
- Winter, A.; Rasche, E.; Hartmann, S.; Schmitter, M.; Kübler, A.; Manuel, K.; Schulz, S.M. Validation of the German-language version of the Liverpool Oral Rehabilitation Questionnaire version 3 and evaluation of oral-health-related quality of life among patients with squamous cell carcinoma of the head and neck. J. Craniomaxillofac. Surg. 2021, 49, 1081–1087. [Google Scholar] [CrossRef]
- Tenore, G.; Mohsen, A.; Rossi, A.F.; Palaia, G.; Rocchetti, F.; Cassoni, A.; Valentini, V.; Ottolenghi, L.; Polimeni, A.; Romeo, U. Does Medication-Related Osteonecrosis of the Jaw Influence the Quality of Life of Cancer Patients? Biomedicines 2020, 8, 95. [Google Scholar] [CrossRef]
- John, M.T.; Patrick, D.L.; Slade, G.D. The German version of the Oral Health Impact Profile--translation and psychometric properties. Eur. J. Oral Sci. 2002, 110, 425–433. [Google Scholar] [CrossRef]
- John, M.T.; Omara, M.; Su, N.; List, T.; Sekulic, S.; Häggman-Henrikson, B.; Visscher, C.M.; Bekes, K.; Reissmann, D.R.; Baba, K.; et al. Recommendations for Use and Scoring of Oral Health Impact Profile Versions. J. Evid. Based Dent. Pract. 2022, 22, 101619. [Google Scholar] [CrossRef]
- Campisi, G.; Mauceri, R.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; Fede, O.D.; Favia, G.; Fusco, V.; et al. Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020. Int. J. Environ. Res. Public Health 2020, 17, 5998. [Google Scholar] [CrossRef]
- Mijiritsky, E.; Lerman, Y.; Mijiritsky, O.; Shely, A.; Meyerson, J.; Shacham, M. Development and Validation of a Questionnaire Evaluating the Impact of Prosthetic Dental Treatments on Patients’ Oral Health Quality of Life: A Prospective Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 5037. [Google Scholar] [CrossRef]
- Winter, A.; Erdelt, K.; Rasche, E.; Schmitter, M.; Edelhoff, D.; Liebermann, A. Impact of Missing Teeth on Oral-Health-Related Quality of Life: A Prospective Bicenter Clinical Trial. Int. J. Prosthodont. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Wolfart, S.; Wolf, K.; Brunzel, S.; Wolfart, M.; Caliebe, A.; Kern, M. Implant placement under existing removable dental prostheses and its effect on masticatory performance. Clin. Oral Investig. 2016, 20, 2447–2455. [Google Scholar] [CrossRef]
- Glaesmer, H.; Grande, G.; Braehler, E.; Roth, M. The German version of the Satisfaction with Life Scale (SWLS): Psychometric properties, validity, and population-based norms. Eur. J. Psychol. Assess. 2011, 27, 127–132. [Google Scholar] [CrossRef]
- Miksad, R.A.; Lai, K.C.; Dodson, T.B.; Woo, S.B.; Treister, N.S.; Akinyemi, O.; Bihrle, M.; Maytal, G.; August, M.; Gazelle, G.S.; et al. Quality of life implications of bisphosphonate-associated osteonecrosis of the jaw. Oncologist 2011, 16, 121–132. [Google Scholar] [CrossRef]
- Caminha, R.D.; Alcantara, P.L.; Carvalho, C.G.; Reia, V.C.; Capelozza, A.L.; Santos, P.S. The impact of medication-related osteonecrosis of the jaws on the quality of life in cancer patients. J. Clin. Exp. Dent. 2020, 12, e725–e729. [Google Scholar] [CrossRef]
- de Cassia Tornier, S.; Macedo, F.J.; Sassi, L.M.; Schussel, J.L. Quality of life in cancer patients with or without medication-related osteonecrosis of the jaw. Support. Care Cancer 2021, 29, 6713–6719. [Google Scholar] [CrossRef] [PubMed]
- El-Rabbany, M.; Blanas, N.; Sutherland, S.; Lam, D.K.; Shah, P.S.; Azarpazhooh, A. Surgical Therapy in Patients With Medication-Related Osteonecrosis of the Jaw Is Associated With Disease Resolution and Improved Quality of Life: A Prospective Cohort Study. J. Oral Maxillofac. Surg. 2022, 80, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Kusumoto, J.; Takeda, D.; Kishimoto, M.; Kashin, M.; Furudoi, S.; Akashi, M. Which symptoms negatively affect the oral health-related quality of life in patients with osteonecrosis of the jaw? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Di Fede, O.; Canepa, F.; Panzarella, V.; Mauceri, R.; Del Gaizo, C.; Bedogni, A.; Fusco, V.; Tozzo, P.; Pizzo, G.; Campisi, G.; et al. The Treatment of Medication-Related Osteonecrosis of the Jaw (MRONJ): A Systematic Review with a Pooled Analysis of Only Surgery versus Combined Protocols. Int. J. Environ. Res. Public Health 2021, 18, 8432. [Google Scholar] [CrossRef]
- Kojima, Y.; Soutome, S.; Otsuru, M.; Hayashida, S.; Sakamoto, Y.; Sawada, S.; Umeda, M. Factors Exacerbating Clinical Symptoms and CT Findings in Patients with Medication-Related Osteonecrosis of the Jaw Receiving Conservative Therapy: A Multicenter Retrospective Study of 53 Cases. Int. J. Environ. Res. Public Health 2022, 19, 7854. [Google Scholar] [CrossRef]
- Drixler, K.; Morfeld, M.; Glaesmer, H.; Brähler, E.; Wirtz, M.A. Validation of the Short-Form-Health-Survey-12 (SF-12 Version 2.0) assessing health-related quality of life in a normative German sample. Z. Psychosom. Med. Psychother. 2020, 66, 272–286. [Google Scholar]
- Capocci, M.; Romeo, U.; Guerra, F.; Mannocci, A.; Tenore, G.; Annibali, S.; Ottolenghi, L. Medication-related osteonecrosis of the jaws (MRONJ) and quality of life evaluation: A pilot study. Clin. Ter. 2017, 168, e253–e257. [Google Scholar]
- Chan, B.H.; Yee, R.; Puvanendran, R.; Ang, S.B. Medication-related osteonecrosis of the jaw in osteoporotic patients: Prevention and management. Singap. Med. J. 2018, 59, 70–75. [Google Scholar] [CrossRef]
- Ohrn, K.E.; Wahlin, Y.B.; Sjödén, P.O. Oral status during radiotherapy and chemotherapy: A descriptive study of patient experiences and the occurrence of oral complications. Support. Care Cancer 2001, 9, 247–257. [Google Scholar]
- Oteri, G.; De Ponte, F.S.; Runci, M.; Peditto, M.; Marcianò, A.; Cicciù, M. Oral-Health-Related Quality of Life After Surgical Treatment of Osteonecrosis of the Jaws. J. Craniofac. Surg. 2018, 29, 403–408. [Google Scholar] [CrossRef]
- Winter, A.; Erdelt, K.; Giannakopoulos, N.N.; Schmitter, M.; Edelhoff, D.; Liebermann, A. Impact of different types of dental prostheses on oral-health-related quality of life: A prospective bicenter study of definitive and interim restorations. Int. J. Prosthodont. 2021, 34, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Rodakowska, E.; Jamiolkowski, J.; Baginska, J.; Kaminska, I.; Gabiec, K.; Stachurska, Z.; Kondraciuk, M.; Dubatowka, M.; Kaminski, K.A. Oral Health-Related Quality of Life and Missing Teeth in an Adult Population: A Cross-Sectional Study from Poland. Int. J. Environ. Res. Public Health 2022, 19, 1626. [Google Scholar] [CrossRef] [PubMed]
- Buchbender, M.; Bauerschmitz, C.; Pirkl, S.; Kesting, M.R.; Schmitt, C.M. A Retrospective Data Analysis for the Risk Evaluation of the Development of Drug-Associated Jaw Necrosis through Dentoalveolar Interventions. Int. J. Environ. Res. Public Health 2022, 19, 4339. [Google Scholar] [CrossRef] [PubMed]
- Kuroshima, S.; Sasaki, M.; Sawase, T. Medication-related osteonecrosis of the jaw: A literature review. J. Oral Biosci. 2019, 61, 99–104. [Google Scholar] [CrossRef]
- Kuo, H.C.; Chen, J.H.; Wu, J.H.; Chou, T.M.; Yang, Y.H. Application of the Oral Health Impact Profile (OHIP) among Taiwanese elderly. Qual. Life Res. 2011, 20, 1707–1713. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Classification |
|---|---|
| At risk | patients who are being or have been treated with antiangiogenetic or antiresorptive therapy |
| Stage 0 | prodromal symptoms without bone exposure |
| Stage I | bone necrotic and exposed, fistula, no signs of infection |
| Stage II | signs of infection additional to symptoms in stage I |
| Stage III | symptoms of stage II combined with pathologic fractures, extraoral fistula, or extensive osteolysis |
| Parameter | Groups | n |
|---|---|---|
| Total | - | 36 |
| Stage | I | 25 |
| II | 11 | |
| Pain | no | 15 |
| yes | 21 | |
| Primary disease | osteoporosis | 8 |
| malignoma | 28 | |
| Risk evaluation | low risk | 12 |
| high risk | 24 | |
| Duration of intake | short | 15 |
| long | 21 | |
| Defect size | small | 11 |
| medium | 11 | |
| large | 14 | |
| Need for prosthodontics | yes | 17 |
| no | 19 |
| Time of Assessment | T0 | T1 | T2 | ||||
|---|---|---|---|---|---|---|---|
| Parameter | Groups | Mean | SD | Mean | SD | Mean | SD |
| Total | - | 75.4 | 40.5 | 58.1 | 33.1 | 53.6 | 32.4 |
| Stage | I | 78.4 | 38.8 | 59.9 | 32.7 | 57.3 | 34.0 |
| II | 68.6 | 43.2 | 54.1 | 35.2 | 45.3 | 28.1 | |
| Pain | no | 67.6 | 29.6 | 53.8 | 29.1 | 48.5 | 26.7 |
| yes | 81.0 | 46.7 | 61.2 | 36.1 | 57.3 | 36.1 | |
| Primary disease | osteoporosis | 96.6 | 30.1 | 61.9 | 23.7 | 53.8 | 32.3 |
| malignoma | 69.3 | 41.5 | 57.0 | 35.6 | 53.6 | 33.0 | |
| Risk evaluation | low risk | 92.5 | 28.3 | 54.8 | 23.8 | 51.1 | 30.5 |
| high risk | 66.8 | 43.4 | 59.9 | 37.3 | 54.9 | 33.8 | |
| Duration of intake | short | 61.6 | 29.8 | 56.3 | 31.9 | 56.1 | 16.5 |
| long | 85.2 | 44.8 | 59.4 | 34.7 | 51.9 | 40.4 | |
| Defect size | small | 77.3 | 33.1 | 67.1 | 23.8 | 63.6 | 24.5 |
| medium | 76.9 | 46.6 | 62.0 | 42.3 | 50.0 | 43.2 | |
| large | 72.7 | 43.5 | 48.0 | 30.8 | 48.7 | 28.3 | |
| Need for prostho- dontics | yes | 89.9 | 41.1 | 67.7 | 36.2 | 61.3 | 36.4 |
| no | 62.4 | 36.2 | 49.6 | 28.4 | 46.8 | 27.5 | |
| Time of Assessment | T0 | T1 | T2 | ||||
|---|---|---|---|---|---|---|---|
| Parameter | Groups | Mean | SD | Mean | SD | Mean | SD |
| Total | - | 25.7 | 6.4 | 27.1 | 6.2 | 26.7 | 5.5 |
| Stage | I | 25.0 | 6.3 | 25.7 | 6.7 | 25.6 | 5.9 |
| II | 27.2 | 6.7 | 30.3 | 3.3 | 29.4 | 3.3 | |
| Pain | no | 24.8 | 7.7 | 25.1 | 8.0 | 24.8 | 6.9 |
| yes | 26.3 | 5.4 | 28.6 | 4.0 | 28.1 | 3.9 | |
| Primary disease | osteoporosis | 26.1 | 5.9 | 23.3 | 8.3 | 26.1 | 5.0 |
| malignoma | 25.6 | 6.6 | 28.2 | 5.1 | 26.9 | 5.7 | |
| Risk evaluation | low risk | 26.7 | 6.3 | 26.3 | 8.2 | 27.3 | 4.9 |
| high risk | 25.2 | 6.6 | 27.5 | 5.0 | 26.5 | 5.9 | |
| Duration of intake | short | 25.5 | 7.4 | 27.8 | 5.8 | 27.0 | 5.7 |
| long | 25.8 | 5.8 | 26.6 | 6.5 | 26.5 | 5.5 | |
| Defect size | small | 26.9 | 6.2 | 28.0 | 5.6 | 27.9 | 4.4 |
| medium | 22.1 | 7.5 | 23.4 | 6.5 | 23.5 | 5.7 | |
| large | 27.6 | 4.6 | 29.4 | 5.3 | 28.4 | 5.4 | |
| Need for prostho-dontics | yes | 25.7 | 5.4 | 26.5 | 5.7 | 25.8 | 6.1 |
| no | 25.7 | 7.3 | 27.6 | 6.7 | 27.6 | 4.9 | |
| Time of Assessment | T0 | T1 | T2 | ||||
|---|---|---|---|---|---|---|---|
| Parameter | Groups | Mean | SD | Mean | SD | Mean | SD |
| Total | - | 61.0 | 29.5 | 43.8 | 33.0 | 33.1 | 33.3 |
| Stage | I | 66.5 | 30.0 | 42.9 | 31.5 | 31.0 | 32.2 |
| II | 48.3 | 25.3 | 45.7 | 37.7 | 37.9 | 36.9 | |
| Pain | no | 61.7 | 28.7 | 46.2 | 29.0 | 33.1 | 32.7 |
| yes | 60.4 | 30.9 | 42.1 | 36.2 | 33.2 | 34.6 | |
| Primary disease | osteoporosis | 63.5 | 34.3 | 42.3 | 39.0 | 37.5 | 39.3 |
| malignoma | 60.2 | 28.7 | 44.5 | 31.9 | 31.9 | 32.1 | |
| Risk evaluation | low risk | 67.8 | 30.6 | 38.3 | 36.1 | 33.5 | 37.2 |
| high risk | 57.5 | 29.0 | 46.5 | 31.8 | 33.0 | 32.1 | |
| Duration of intake | short | 60.4 | 28.7 | 45.9 | 31.0 | 32.5 | 33.3 |
| long | 61.3 | 30.8 | 42.3 | 35.1 | 33.6 | 34.2 | |
| Defect size | small | 60.0 | 33.8 | 48.9 | 32.3 | 37.4 | 35.9 |
| medium | 58.5 | 25.9 | 46.8 | 35.7 | 33.6 | 36.4 | |
| large | 63.6 | 30.7 | 37.4 | 32.8 | 29.4 | 30.9 | |
| Need for prostho-dontics | yes | 75.1 | 25.0 | 47.4 | 35.3 | 41.0 | 36.9 |
| no | 48.4 | 28.3 | 40.6 | 31.4 | 26.1 | 29.0 | |
| Time of Assessment | T0 | T1 | T2 | ||||
|---|---|---|---|---|---|---|---|
| Parameter | Groups | Mean | SD | Mean | SD | Mean | SD |
| Total | - | 38.1 | 19.4 | 31.8 | 17.1 | 25.4 | 17.5 |
| Stage | I | 38.4 | 19.5 | 28.9 | 15.3 | 24.2 | 18.0 |
| II | 37.5 | 20.1 | 38.4 | 20.0 | 28.3 | 16.6 | |
| Pain | no | 38.7 | 20.5 | 35.4 | 15.4 | 28.0 | 19.3 |
| yes | 37.6 | 19.1 | 29.2 | 18.2 | 23.6 | 16.3 | |
| Primary disease | osteoporosis | 32.6 | 16.0 | 26.1 | 16.2 | 15.6 | 14.1 |
| malignoma | 39.7 | 20.2 | 33.4 | 17.3 | 28.2 | 17.5 | |
| Risk evaluation | low risk | 34.5 | 15.9 | 25.3 | 16.0 | 17.4 | 15.5 |
| high risk | 39.9 | 21.0 | 35.0 | 17.1 | 29.4 | 17.3 | |
| Duration of intake | short | 38.7 | 19.7 | 35.1 | 18.4 | 28.5 | 16.4 |
| long | 37.6 | 19.6 | 29.4 | 16.2 | 23.3 | 18.3 | |
| Defect size | small | 29.6 | 19.2 | 29.8 | 18.7 | 24.7 | 18.1 |
| medium | 42.7 | 16.7 | 37.3 | 17.2 | 27.4 | 19.4 | |
| large | 41.2 | 20.6 | 29.0 | 16.1 | 24.5 | 16.7 | |
| Need for prostho-dontics | yes | 44.1 | 20.6 | 35.4 | 16.7 | 29.8 | 18.7 |
| no | 32.7 | 17.0 | 28.6 | 17.4 | 21.5 | 15.8 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winter, A.; Schulz, S.M.; Schmitter, M.; Brands, R.C.; Straub, A.; Kübler, A.; Borgmann, A.; Hartmann, S. Oral-Health-Related Quality of Life in Patients with Medication-Related Osteonecrosis of the Jaw: A Prospective Clinical Study. Int. J. Environ. Res. Public Health 2022, 19, 11709. https://doi.org/10.3390/ijerph191811709
Winter A, Schulz SM, Schmitter M, Brands RC, Straub A, Kübler A, Borgmann A, Hartmann S. Oral-Health-Related Quality of Life in Patients with Medication-Related Osteonecrosis of the Jaw: A Prospective Clinical Study. International Journal of Environmental Research and Public Health. 2022; 19(18):11709. https://doi.org/10.3390/ijerph191811709
Chicago/Turabian StyleWinter, Anna, Stefan M. Schulz, Marc Schmitter, Roman C. Brands, Anton Straub, Alexander Kübler, Anna Borgmann, and Stefan Hartmann. 2022. "Oral-Health-Related Quality of Life in Patients with Medication-Related Osteonecrosis of the Jaw: A Prospective Clinical Study" International Journal of Environmental Research and Public Health 19, no. 18: 11709. https://doi.org/10.3390/ijerph191811709
APA StyleWinter, A., Schulz, S. M., Schmitter, M., Brands, R. C., Straub, A., Kübler, A., Borgmann, A., & Hartmann, S. (2022). Oral-Health-Related Quality of Life in Patients with Medication-Related Osteonecrosis of the Jaw: A Prospective Clinical Study. International Journal of Environmental Research and Public Health, 19(18), 11709. https://doi.org/10.3390/ijerph191811709