
Freedive Training Gives Additional Physiological Effect Compared to Pulmonary Rehabilitation in COPD

 , , ,
, , ,
Abstract
1. Introduction
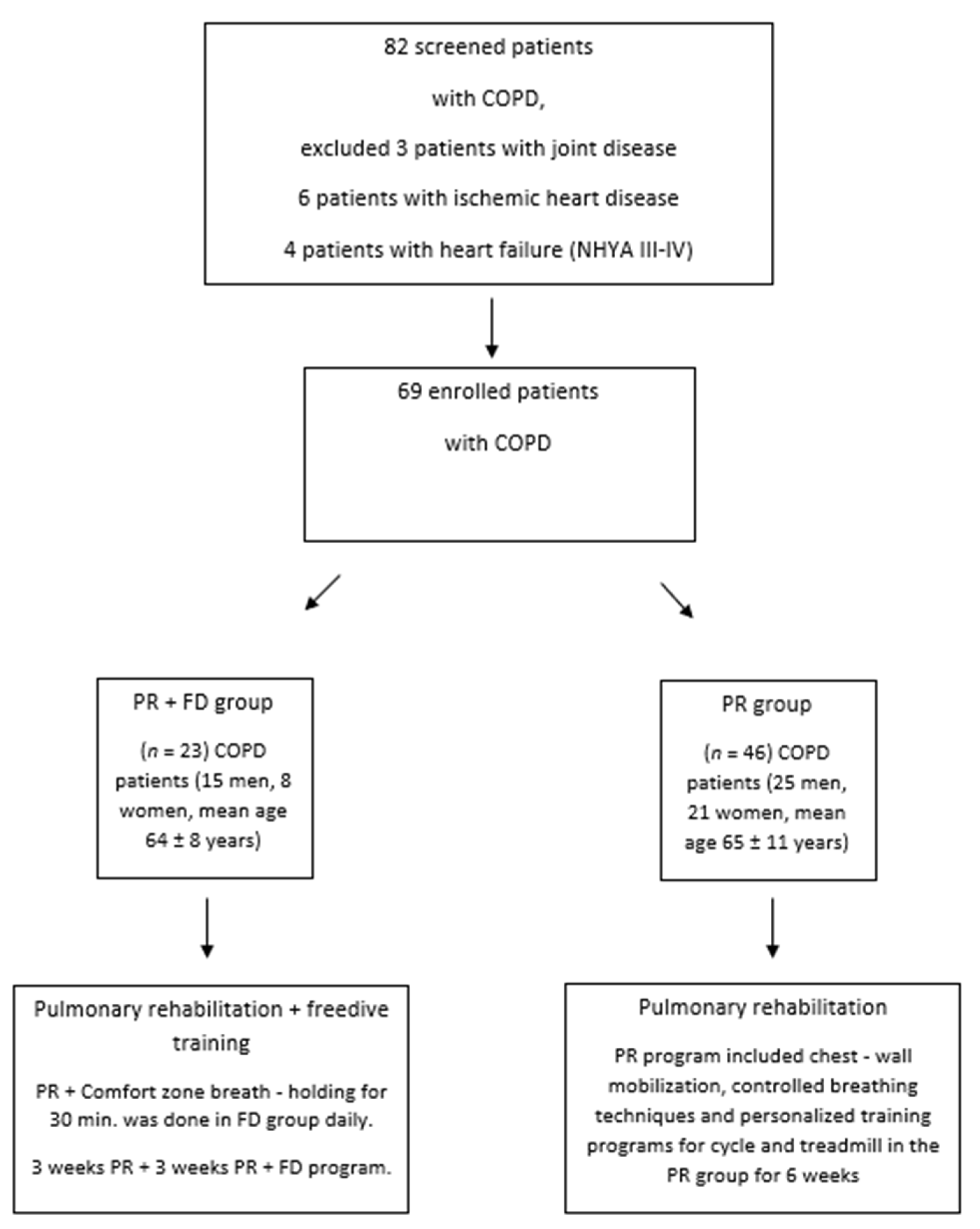
2. Patients and Methods
3. Measurements
3.1. Pulmonary Function
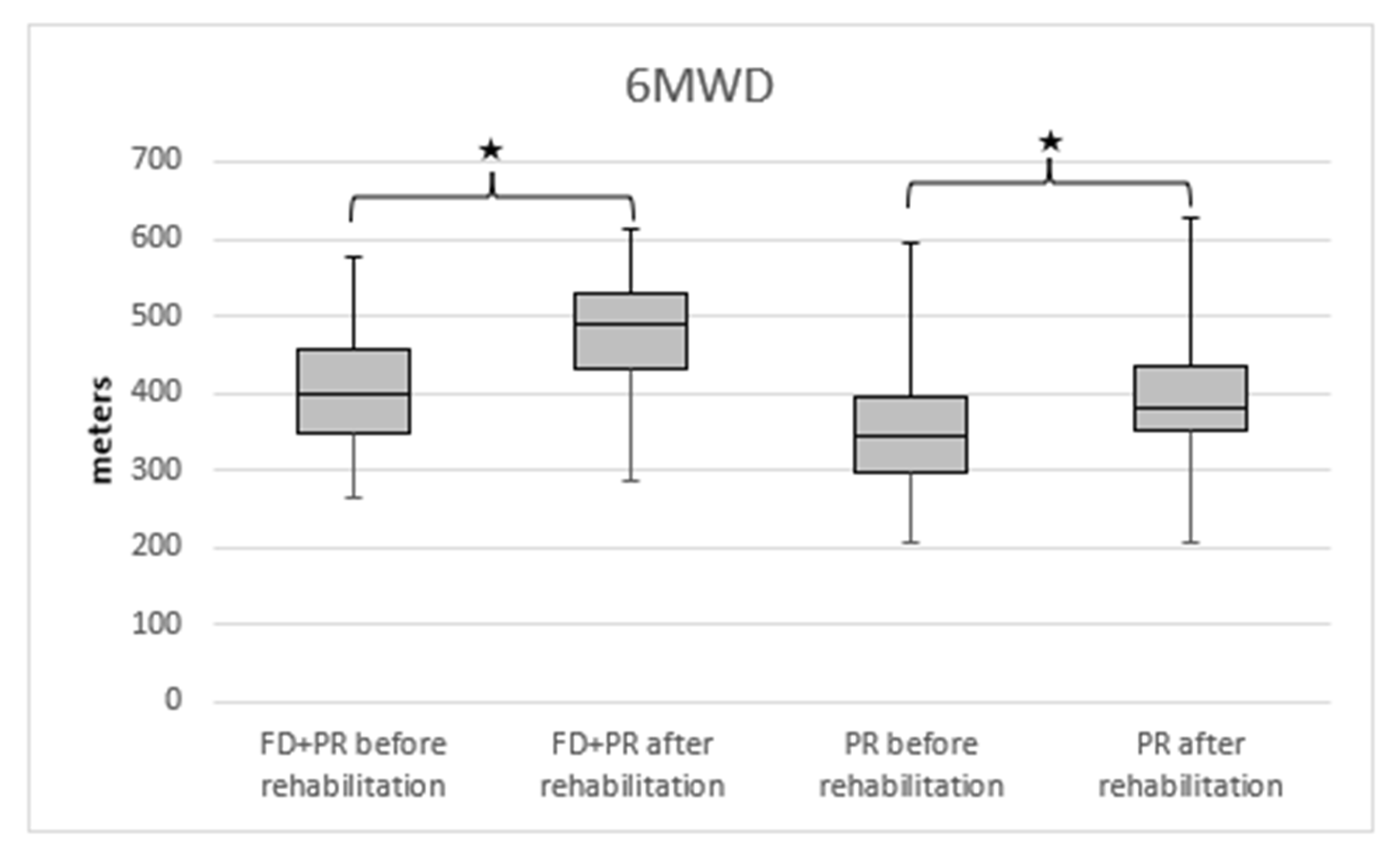
3.1.1. Six-Minute Walking Distance
3.1.2. Chest Wall Expansion
3.1.3. Maximal Inspiratory Pressure
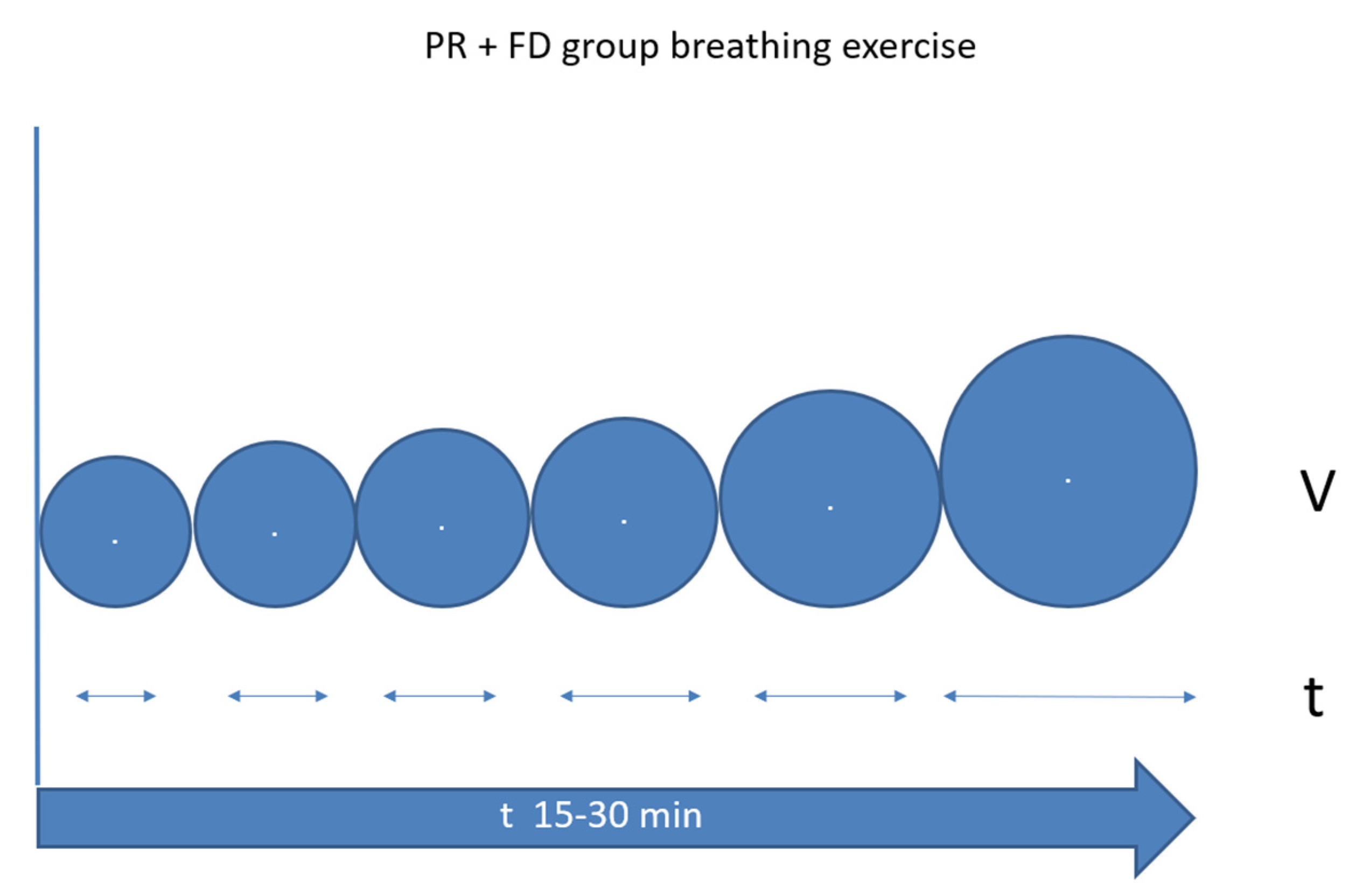
3.1.4. Breath-Holding Time
3.1.5. Grip Strength Measurement
3.1.6. Quality of Life and DYSPNEA Questionnaires
3.2. Severity of the Disease
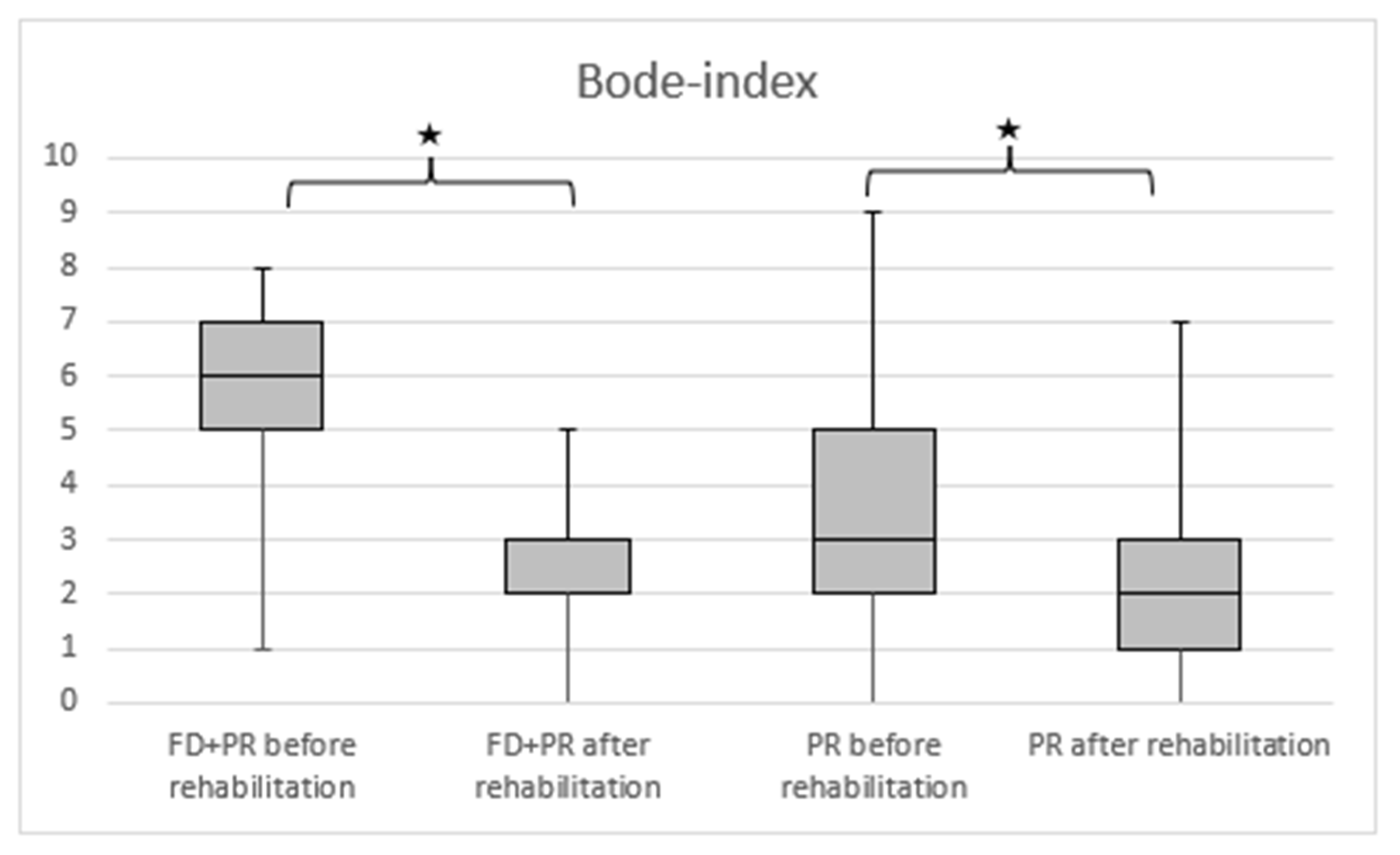
3.2.1. BODE Index
3.2.2. Alternative Scale
3.3. Statistical Methods
4. Results
5. Discussion
Elements of Conventional Rehabilitation
6. Limitations of the Study
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AS | Alternative Scale |
| BHT | Breath-Holding Time |
| BMI | Body Mass Index |
| CAT | COPD Assessment Test |
| CBT | Comfort Zone Breath Hold Training |
| COPD | Chronic Obstructive Pulmonary Disease |
| C | Continuous |
| CT | Continuous Training |
| CWE | Chest Wall Extension |
| DH | Dynamic Hyperinflation |
| FD | Freediving Training |
| FEV1 | Forced Expiratory Volume in the first second |
| FVC | Forced Vital Capacity |
| GS | Grip Strength |
| I | Interval |
| IVC | Inspiratory Vital Capacity |
| MIP | Maximal Inspiratory Pressure |
| mMRC | Modified Medical Research Council Dyspnea Scale |
| PLB | Pursed Lip Breathing |
| PH | Pulmonary Hypertension |
| PR | Pulmonary Rehabilitation |
| S | Self-paced |
| 6MWD | Six-Minute Walking Distance |
| VAS | Visual Analogue Scale |
| VC | Vital Capacity |
References
- Kerti, M.; Balogh, Z.; Kelemen, K.; Varga, J.T. The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 717–724. [Google Scholar] [CrossRef]
- Varga, J.; Casaburi, R.; Ma, S.; Hecht, A.; Hsia, D.; Somfay, A.; Porszasz, J. Relation of concavity in the expiratory flow-volume loop to dynamic hyperinflation during exercise in COPD. Respir. Physiol. Neurobiol. 2016, 234, 79–84. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Laveneziana, P. Physiology and consequences of lung hyperinflation in COPD. Eur. Resp. Rev. 2006, 15, 61–67. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Revill, S.M.; Webb, K.A. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 164, 770–777. [Google Scholar] [CrossRef]
- Csizmadia, Z. Improvement of respiratory effectiveness in connection with new functional markers. In Proceedings of the International Conference on Pulmonology, Allergology and Immunology, Debrecen, Hungary, 29 August 2019. [Google Scholar]
- Varga, J.; Porszasz, J.; Boda, K.; Casaburi, R.; Somfay, A. Supervised high intensity continuous and interval training vs. self-paced training in COPD. Respir Med. 2007, 101, 2297–2304. [Google Scholar] [CrossRef]
- de Sá, R.B.; Pessoa, M.F.; Cavalcanti, A.G.L.; Campos, S.L.; Amorim, C.; Dornelas de Andrade, A. Immediate effects of respiratory muscle stretching on chest wall kinematics and electromyography in COPD patients. Respir Physiol. Neurobiol. 2017, 242, 1–7. [Google Scholar] [CrossRef]
- Jones, P.W.; Agusti, A.G. Outcomes and markers in the assessment of chronic obstructive pulmonary disease. Eur. Respir J. 2006, 27, 822–832. [Google Scholar] [CrossRef]
- Cote, C.G.; Celli, B.R. Pulmonary rehabilitation and the BODE index in COPD. Eur. Respir J. 2005, 26, 630–636. [Google Scholar] [CrossRef]
- Kerti, M.; Balogh, Z.S.; Halasz, A.; Kelemen, K.; Varga, J. COPD Assessment for Symptoms and Functional Condition in Pulmonary Rehabilitation; ERS Annual Congress: Amsterdam, The Amsterdam, 2015; p. P2218. [Google Scholar]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests, European community for steel and coal. Official statement of the European Respiratory Society. Eur. Respir J. 1993, 16, 5–40. [Google Scholar] [CrossRef]
- Balke, B. A Simple Field Test for the Assessment of Physical Fitness; Rep 63-6; Civil Aeromedical Research Institute: Oklahoma City, Oklahoma, 1963; pp. 1–8. [Google Scholar]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Debouche, S.; Pitance, L.; Robert, A.; Liistro, G.; Reychler, G. Reliability and reproducibility of chest wall expansion measurement in young healthy adults. J. Manip. Physiol. Ther. 2016, 39, 443–449. [Google Scholar] [CrossRef]
- Neumeister, W.; Rasche, K.; Maas, P.; Monnerjahn, C.; Singh, B.; Schultze-Werninghaus, G. Reproduzierbarkeit der EDV-gestützte Mund Okklusion Druckmessungen [Reproducibility of computer-assisted mouth occlusion pressure measurements]. Med. Klin. 1996, 91 (Suppl. 2), 73–75. (In German) [Google Scholar]
- Mirsky, I.A.; Lipman, E.; Grinker, R.R. Breath holding time in anxiety states. Fed. Proc. 1946, 5 Pt 2, 74. [Google Scholar]
- Shingai, K.; Kanezaki, M. Effect of dyspnea induced by breath-holding on maximal muscular strength of patients with COPD. J. Phys. Ther. Sci. 2014, 26, 255–258. [Google Scholar] [CrossRef][Green Version]
- An, K.N.; Chao, N.Y.; Askew, L.J. Hand strength measurement instruments. Arch. Phys. Med. Rehabil. 1980, 61, 366–368. [Google Scholar]
- Jeong, M.; Kang, H.K.; Song, P.; Park, H.K.; Jung, H.; Lee, S.S.; Koo, H.K. Hand grip strength in patients with chronicobstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 2385–2390. [Google Scholar] [CrossRef]
- Launois, C.; Barbe, C.; Bertin, E.; Nardi, J.; Perotin, J.-M.; Dury, S.; Lebargy, F.; Deslee, G. The modified Medical Research Council scale for the assessment of dyspnea in daily living in obesity: A pilot study. BMC Pulm. Med. 2012, 12, 61. [Google Scholar] [CrossRef]
- Braun, S.R. Respiratory Rate and Pattern. In Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Butterworths: Boston, MA, USA, 1990; Chapter 43. [Google Scholar]
- Brown, S.J.; Bryant, M.; Mundel, T.; Stannard, S.R. Human ventilatory efficiency and respiratory sinus arrhythmia during head-up tilt. J. Physiol. Pharmacol. 2008, 59, 771–780. [Google Scholar]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The physiological effects of slow breathing in the healthy human. Breathe 2017, 13, 298–309. [Google Scholar] [CrossRef]
- Pako, J.; Barta, I.; Balogh, Z.; Kerti, M.; Drozdovszky, O.; Bikov, A.; Antus, B.; Horvath, I.; Varga, J. Assessment of the Anti-Aging Klotho Protein in Patients with COPD Undergoing Pulmonary Rehabilitation. J. COPD 2017, 14, 176–180. [Google Scholar] [CrossRef][Green Version]
- Vagvolgyi, A.; Rozgonyi, Z.; Kerti, M.; Agathou, G.; Vadasz, P.; Varga, J. Effectiveness of pulmonary rehabilitation and correlations in between functional parameters, extent of thoracic surgery and severity of post-operative complications: Randomized clinical trial. J. Thor. Dis. 2018, 10, 3519–3531. [Google Scholar] [CrossRef]
- Vágvölgyi, A.; Rozgonyi, Z.; Vadász, P.; Varga, J.T. A mellkassebészeti műtéti teherbíróképesség megítélése, perioperatív légzésrehabilitáció. Orv. Hetil. 2017, 158, 1989–1997. [Google Scholar] [CrossRef]
- Varga, J.; Porszasz, J.; Boda, K.; Casaburi, R.; Somfay, A. Felügyelt magas intenzitású folyamatos és intervallum, valamint otthoni tréning hatásának vizsgálata krónikus obstruktív tüdőbetegek rehabilitációjában. Med. Thor. 2008, 61, 135–143. [Google Scholar]
- Varga, J.; Pálinkás, A.; Lajkó, I.; Horvath, I.; Boda, K.; Somfay, A. Pulmonary arterial pressure response during exercise in COPD: A correlation with C-reactive protein (hsCRP). Open Resp. J. 2016, 10, 1–11. [Google Scholar] [CrossRef]
- Hegedus, B.; Varga, J.; Somfay, A. Az interdiszciplináris rehabilitáció hatása spondylitis ankylopoeticában szenvedő betegeknél [Interdisciplinary rehabilitation in patients with ankylosing spondylitis]. Orv. Hetil. 2016, 157, 1126–1132. [Google Scholar] [CrossRef]
- Ács, P.; Stocker, M.; Füge, K.; Paár, D.; Oláh, A.; Kovács, A. Economic and public health benefits: The result of increased regular physical activity. Eur. J. Integr Med. 2016, 8, 8–12. [Google Scholar] [CrossRef]
- Ács, P.; Veress, R.; Rocha, P.; Dóczi, T.; László, R.B.; Baumann, P.; Ostojic, S.; Prémusz, V.; Makai, A. Criterion validity and reliability of the International Physical Activity Questionnaire–Hungarian short form against the RM42 accelerometer. BMC Public Health 2021, 21, 381. [Google Scholar] [CrossRef]
- Ács, P.; Betlehem, J.; Oláh, A.; Barbara, B.; Morvay-Sey, K.; Alexandra, M.; Viktória, P. Cross-cultural adaptation and validation of the Global Physical Activity Questionnaire among healthy Hungarian adults. BMC Public Health 2020, 20, 1056. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Group PR (n = 46) | Group PR + FD (n = 23) | p-Value |
|---|---|---|---|
| Age (years) | 66 ± 11 | 63 ± 12 | 0.435 |
| Male/Female | 24/22 | 12/11 | 0.600 |
| BMI (kg/m2) | 27 ± 9 | 28 ± 8 | 0.529 |
| FEV1 (%pred) | 43 ± 36 | 41 ± 19 | 0.862 |
| Hypertension | 35 (76%) | 18 (78%) | 0.547 |
| Diabetes | 11 (24%) | 6 (26%) | 0.532 |
| Pulmonary hypertension | 12 (26%) | 6 (26%) | 0.608 |
| Emphysema | 14 (30%) | 7 (30%) | 0.605 |
| Quitting of smoking | 33 (72%) | 17 (74%) | 0.544 |
| PR Group Before Rehabilitation | PR Group | p-Value | PR + FD Group | PR + FD Group | p-Value | Comparison of PR + FD and PR p-Value | |
|---|---|---|---|---|---|---|---|
| After Rehabilitation | Before Rehabilitation | After Rehabilitation | |||||
| FEV1 % pred | 43 (36) | 50 (27) | 0.002 | 40.5 (19) | 50 (24) | <0.001 | 0.101 |
| FVC % pred | 73 (28) | 80 (36) | 0.002 | 75 (19) | 75 (15) | 0.871 | 0.035 |
| IVC (L) | 2.23 (1.32) | 2.25 (1.35) | 0.011 | 2.51 (1.01) | 2.78 (1.08) | <0.001 | 0.127 |
| Chest expansion (cm) | 3.5 (3.5) | 5 (4) | <0.001 | 3 (2.5) | 6.25 (2.5) | <0.001 | <0.001 |
| Breath-holding time (s) | 20 (10) | 24 (16) | 0.002 | 24 (18) | 41 (30) | <0.001 | <0.001 |
| MIP (H2Ocm) | 64 (27) | 69 (36) | <0.001 | 65 (27) | 79 (25) | <0.001 | 0.009 |
| Grip strength (kg) | 27.2 (12) | 27.8 (13.5) | <0.001 | 27.3 (15.2) | 31.3 (18.1) | <0.001 | 0.059 |
| CAT | 18 (14) | 12 (13) | <0.001 | 17 (8) | 7 (7) | <0.001 | 0.006 |
| mMRC | 2 (0) | 2 (1) | 0.011 | 2 (1) | 2 (1) | 0.002 | 0.010 |
| Alternative scale | 4 (3) | 3 (3) | <0.001 | 6 (2) | 2 (2) | <0.001 | <0.001 |
| 6MWD (m) | 345 (99) | 382 (86) | <0.001 | 399.5 (116) | 490 (96) | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Csizmadia, Z.; Ács, P.; Szőllősi, G.J.; Tóth, B.; Kerti, M.; Kovács, A.; Varga, J.T. Freedive Training Gives Additional Physiological Effect Compared to Pulmonary Rehabilitation in COPD. Int. J. Environ. Res. Public Health 2022, 19, 11549. https://doi.org/10.3390/ijerph191811549
Csizmadia Z, Ács P, Szőllősi GJ, Tóth B, Kerti M, Kovács A, Varga JT. Freedive Training Gives Additional Physiological Effect Compared to Pulmonary Rehabilitation in COPD. International Journal of Environmental Research and Public Health. 2022; 19(18):11549. https://doi.org/10.3390/ijerph191811549
Chicago/Turabian StyleCsizmadia, Zoltán, Pongrác Ács, Gergő József Szőllősi, Blanka Tóth, Mária Kerti, Antal Kovács, and János Tamás Varga. 2022. "Freedive Training Gives Additional Physiological Effect Compared to Pulmonary Rehabilitation in COPD" International Journal of Environmental Research and Public Health 19, no. 18: 11549. https://doi.org/10.3390/ijerph191811549
APA StyleCsizmadia, Z., Ács, P., Szőllősi, G. J., Tóth, B., Kerti, M., Kovács, A., & Varga, J. T. (2022). Freedive Training Gives Additional Physiological Effect Compared to Pulmonary Rehabilitation in COPD. International Journal of Environmental Research and Public Health, 19(18), 11549. https://doi.org/10.3390/ijerph191811549