

Determining Trends and Factors Associated with Self-Reported Physical Activity among Adolescents in Rural North Carolina



Abstract
:1. Introduction
2. Methods
2.1. Study Setting and Participants
2.2. Measures
2.2.1. Dependent Variable—Self-Reported PA
2.2.2. Independent Variables
2.2.3. Access to Exercise Opportunities
2.2.4. Physical Education and Activity
2.2.5. PACER
2.2.6. Body Mass Index
2.3. Data Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Physical Activity Plan Alliance. The 2018 United States Report Card on Physical Activity for Children and Youth; National Physical Activity Plan Alliance: Washington, DC, USA, 2018. [Google Scholar]
- Child and Adolescent Health Measurement Initiative. 2016 National Survey of Children’s Health (NSCH) Data Query. Data Resource Center for Child and Adolescent Health supported by the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB). Available online: www.childhealthdata.org (accessed on 2 February 2022).
- Nelson, M.C.; Gordon-Larsen, P.; Song, Y.; Popkin, B. Built and Social Environments: Associations with Adolescent Overweight and Activity. Am. J. Prev. Med. 2006, 31, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.B.; Bocarro, J.; Kanters, M.A. Place Disparities in Supportive Environments for Extracurricular Physical Activity in North Carolina Middle Schools. Youth Soc. 2012, 45, 265–285. [Google Scholar] [CrossRef]
- Gray, H.L.; Buro, A.W.; Ikan, J.B.; Wang, W.; Stern, M. School-level factors associated with obesity: A systematic review of longitudinal studies. Obes. Rev. 2019, 20, 1016–1032. [Google Scholar] [CrossRef] [PubMed]
- Ploeg, K.A.V.; McGavock, J.; Maximova, K.; Veugelers, P.J. School-Based Health Promotion and Physical Activity During and After School Hours. Pediatrics 2014, 133, e371–e378. [Google Scholar] [CrossRef] [PubMed]
- Abi Nader, P.; Hilberg, E.; Schuna, J.M.; John, D.H.; Gunter, K.B. Teacher-Level Factors, Classroom Physical Activity Opportunities, and Children’s Physical Activity Levels. J. Phys. Act. Health 2018, 15, 637–643. [Google Scholar] [CrossRef]
- Eather, N.; Morgan, P.; Lubans, D. Improving the fitness and physical activity levels of primary school children: Results of the Fit-4-Fun group randomized controlled trial. Prev. Med. 2013, 56, 12–19. [Google Scholar] [CrossRef]
- Eather, N.; Morgan, P.J.; Lubans, D.R. Feasibility and preliminary efficacy of the Fit4Fun intervention for improving physical fitness in a sample of primary school children: A pilot study. Phys. Educ. Sport Pedagog. 2013, 18, 389–411. [Google Scholar] [CrossRef]
- Li, X.-H.; Lin, S.; Guo, H.; Huang, Y.; Wu, L.; Zhang, Z.; Ma, J.; Wang, H.-J. Effectiveness of a school-based physical activity intervention on obesity in school children: A nonrandomized controlled trial. BMC Public Health 2014, 14, 1282. [Google Scholar] [CrossRef]
- Yen, H.-Y.; Li, C. Correction: Determinants of physical activity: A path model based on an ecological model of active living. PLoS ONE 2019, 14, e0222625. [Google Scholar] [CrossRef]
- Lazorick, S.; Crawford, Y.; Gilbird, A.; Fang, X.; Burr, V.; Moore, V.; Hardison, G.T. Long-Term Obesity Prevention and the Motivating Adolescents with Technology to CHOOSE Health™ Program. Child. Obes. 2014, 10, 25–33. [Google Scholar] [CrossRef]
- Lazorick, S.; Fang, X.; Crawford, Y. The match program: Long-term obe- sity prevention through a middle school based inter-vention. Child Obes. 2016, 12, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Lazorick, S.; Hardison, G.T.; Esserman, D.A.; Perrin, E.M. Sustained Body Mass Index Changes One and Two Years Post MATCH: A School-Based Wellness Intervention in Adolescents. Child. Obes. 2011, 7, 372–378. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. 2018 Youth Risk Behavior Survey Questionnaire. Available online: www.cdc.gov/yrbs (accessed on 3 February 2021).
- Opper, C.; Collier, C.; Fang, X.; Lazorick, S. Measuring Determinants of Health for a School-based Obesity Intervention. Health Behav. Policy Rev. 2020, 7, 248–262. [Google Scholar]
- County Health Rankings. Access to Exercise Opportunities. Available online: http://www.countyhealthrankings.org/app/north-carolina-2018/measures/factors/132/data (accessed on 1 December 2021).
- The Cooper Institute. FitnessGram. Available online: https://fitnessgram.net/assessment/ (accessed on 1 December 2021).
- Eastern Upper Peninsula Intermediate School District. The PACER. Available online: https://www.eupschools.org/cms/lib/MI17000134/Centricity/Domain/127/pacer%20directions.pdf (accessed on 24 August 2022).
- CDC. Defining Childhood Weight Status. Available online: https://www.cdc.gov/obesity/childhood/defining.html (accessed on 1 December 2021).
- Muth, N. American Academy of Pediatrics. New Report Guides Physical Activity Counseling in Pediatric Clinical Settings. Available online: https://publications.aap.org/aapnews/news/12302 (accessed on 1 March 2022).
- Saunders, R.P.; Dowda, M.; McIver, K.; McDonald, S.M.; Pate, R.R. Physical and Social Contexts of Physical Activity Behaviors of Fifth and Seventh Grade Youth. J. Sch. Health 2018, 88, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Rosselli, M.; Ermini, E.; Tosi, B.; Boddi, M.; Stefani, L.; Toncelli, L.; Modesti, P.A. Gender differences in barriers to physical activity among adolescents. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Robbins, L.B.; Pender, N.J.; Kazanis, A. Barriers to Physical Activity Perceived by Adolescent Girls. J. Midwifery Women’s Health 2003, 48, 206–212. [Google Scholar] [CrossRef]
- Kimm, S.Y.S.; Glynn, N.W.; Mcmahon, R.P.; Voorhees, C.C.; Striegel-Moore, R.H.; Daniels, S.R. Self-Perceived Barriers to Activity Participation among Sedentary Adolescent Girls. Med. Sci. Sports Exerc. 2006, 38, 534–540. [Google Scholar] [CrossRef]
- Basch, C.E. Physical Activity and the Achievement Gap Among Urban Minority Youth. J. Sch. Health 2011, 81, 626–634. [Google Scholar] [CrossRef]
- World Health Organization. New WHO-Led Study Says Majority of Adolescents Worldwide are not Sufficiently Physically Active, Putting Their Current and Future Health at Risk. Available online: https://www.who.int/news/item/22-11-2019-new-who-led-study-says-majority-of-adolescents-worldwide-are-not-sufficiently-physically-active-putting-their-current-and-future-health-at-risk (accessed on 1 March 2022).
- Gordon-Larsen, P.; McMurray, R.G.; Popkin, B.M. Adolescent physical activity and inactivity vary by ethnicity: The National Longitudinal Study of Adolescent Health. J. Pediatr. 1999, 135, 301–306. [Google Scholar] [CrossRef]
- Gordon-Larsen, P.; Nelson, M.C.; Page, P.; Popkin, B.M. Inequality in the Built Environment Underlies Key Health Disparities in Physical Activity and Obesity. Pediatrics 2006, 117, 417–424. [Google Scholar] [CrossRef]
- Mak, K.-K.; Tan, S.H. Underweight problems in Asian children and adolescents. Eur. J. Pediatr. 2012, 171, 779–785. [Google Scholar] [CrossRef]
- Ochiai, H.; Shirasawa, T.; Nanri, H.; Nishimura, R.; Nomoto, S.; Hoshino, H.; Kokaze, A. Lifestyle factors associated with underweight among Japanese adolescents: A cross-sectional study. Arch. Public Health 2017, 75, 45. [Google Scholar] [CrossRef]
- Levin, S.; Lowry, R.; Brown, D.R.; Dietz, W.H. Physical Activity and Body Mass Index Among US Adolescents: Youth risk behavior survey, 1999. Arch. Pediatr. Adolesc. Med. 2003, 157, 816–820. [Google Scholar] [CrossRef]
- Kohl, H.W., III; Cook, H.D. Committee on Physical Activity and Physical Education in the School Environment. In Food and Nutrition Board; Educating the Student Body: Taking Physical Activity and Physical Education to School; Institute of Medicine, Ed.; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- McKenzie, T.L.; Lounsbery, M.A.F. The Pill Not Taken: Revisiting Physical Education Teacher Effectiveness in a Public Health Context. Res. Q. Exerc. Sport 2014, 85, 287–292. [Google Scholar] [CrossRef]
- NCLD. Learn The Law ESEA/NCLB. Available online: https://www.ncld.org/get-involved/learn-the-law/esea-nclb/ (accessed on 1 December 2021).
- Siedentop, D.L. National Plan for Physical Activity: Education Sector. J. Phys. Act. Health 2009, 6, S168–S180. [Google Scholar] [CrossRef]
- Cooper, K.H.; Greenberg, J.D.; Castelli, D.M.; Barton, M.; Martin, S.B.; Morrow, J.R., Jr. Implementing Policies to Enhance Physical Education and Physical Activity in Schools. Res. Q. Exerc. Sport 2016, 87, 133–140. [Google Scholar] [CrossRef]
- Mayra, S.T.; Kandiah, J.; McIntosh, C.E. COVID-19 and health in children and adolescents in the US: A narrative systematic review. Psychol. Sch. 2022. [Google Scholar] [CrossRef]
- Beck, A.L.; Huang, J.C.; Lendzion, L.; Fernandez, A.; Martinez, S. Impact of the Coronavirus Disease 2019 Pandemic on Parents’ Perception of Health Behaviors in Children With Overweight and Obesity. Acad. Pediatr. 2021, 21, 1434–1440. [Google Scholar] [CrossRef]
- Tulchin-Francis, K.; Stevens, W., Jr.; Gu, X.; Zhang, T.; Roberts, H.; Keller, J.; Dempsey, D.; Borchard, J.; Jeans, K.; VanPelt, J. The impact of the coronavirus disease 2019 pandemic on physical activity in U.S. children. J. Sport Health Sci. 2021, 10, 323–332. [Google Scholar] [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef]
- Pavlovic, A.; DeFina, L.F.; Natale, B.L.; Thiele, S.E.; Walker, T.J.; Craig, D.W.; Vint, G.R.; Leonard, D.; Haskell, W.L.; Kohl, H.W. Keeping children healthy during and after COVID-19 pandemic: Meeting youth physical activity needs. BMC Public Health 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Dayton, J.D.; Ford, K.; Carroll, S.J.; Flynn, P.A.; Kourtidou, S.; Holzer, R.J. The Deconditioning Effect of the COVID-19 Pandemic on Unaffected Healthy Children. Pediatr. Cardiol. 2021, 42, 554–559. [Google Scholar] [CrossRef]
- Dorn, E.; Hancock, B.; Sarakatsannis, J.; Viruleg, E. McKinsey & Company. COVID-19 and Education: An Emerging K-Shaped Recovery. Available online: https://www.mckinsey.com/industries/education/our-insights/covid-19-and-education-an-emerging-k-shaped-recovery# (accessed on 15 June 2022).
- Council of Chief State School Officers. CCSSO Fact Sheet: COVID-19 Relief Funding For K-12 Education (Updated with ARP). Available online: https://753a0706.flowpaper.com/CCSSOCovidReliefFactSheet/#page=1 (accessed on 15 June 2022).
- Achieve The Core. 2020–21 Priority Instructional Content in English Language Arts/Literacy and Mathematics. Available online: https://achievethecore.org/page/3267/priority-instructional-content-in-english-language-arts-literacy-and-mathematics (accessed on 15 June 2022).
- Council of the Great City Schools. Addressing Unfinished Learning After COVID-19 School Closures. Available online: https://www.cgcs.org/cms/lib/DC00001581/Centricity/Domain/313/CGCS_Unfinished%20Learning.pdf (accessed on 15 June 2021).

{kind=link}
| Determinant | Description | Level | Scale | Description | Source |
|---|---|---|---|---|---|
| County-level Determinant | |||||
| Exercise Opportunities | Adequate access to locations for physical activity | County | 1–5 | “Access to Exercise Opportunities measures the percentage of individuals in a county who live reasonably close to a location for physical activity. Locations for physical activity are defined as parks or recreational facilities. Individuals are considered to have access to exercise opportunities if they: reside in a census block that is within a half mile of a park, reside in an urban census block that is within one mile of a recreational facility, or reside in a rural census block that is within 3 miles of a recreational facility” [17] | County Health Rankings and Roadmaps |
| School-level Determinants | |||||
| Physical Education (PE) | How health/PE is provided for 7th grade students | School | 1–5 | 1 = Not provided in 7th grade 2 = Provided for a subset of students in one semester or block schedule 3 = Provided for a subset of students throughout the year 4 = On a semester or block schedule for all students 5 = Provided for both semesters or throughout the school year for all students | School Administrator Survey |
| School Physical Activity (PA) Opportunities | PA opportunities available at school outside of regular PE time | School | 1, 3, 5 | 1 = No 3 = Yes, but how this occurs varies by teacher or class 5 = Yes, there is time set aside with organized, appropriate activities and/or places for activity (such as playground, gym, all purpose room, game field, or a place to walk) | School Administrator Survey |
| Characteristics of 2018–2019 MATCH Participants | ||
|---|---|---|
| Sample Size, N | Participants | 3799 |
| Schools | 40 | |
| N (%) | ||
| Sex | Male | 1942(51.1%) |
| Female | 1857 (48.9%) | |
| Ethnicity | Black | 942 (24.8%) |
| White | 1871 (49.3%) | |
| Other | 986 (26.0%) | |
| Weight Status (Based on BMI Percentile) | Underweight (<5%) | 108 (2.8%) |
| Healthy weight (5–84.9%) | 1925 (50.7%) | |
| Overweight (85–94.9%) | 709 (18.7%) | |
| Obese (≥95%) | 1057 (27.8%) | |
| Body Mass Index, Fitness Testing, and Self-Reported PA | ||
| Mean (SD) | ||
| BMI z-score | 0.8 (1.2) | |
| PACER test result, # of laps | 28.7 (20.6) | |
| Baseline # of days with 60 min PA | 3.7 (2.2) | |
| Variable | N | ≥1 Day * | ≥5 Days * | 7 Days * |
|---|---|---|---|---|
| School PE | ||||
| 2 | 607 | 542 (89.3%) | 209 (34.4%) | 74 (12.2%) |
| 3 | 439 | 386 (87.9%) | 174 (39.6%) | 63 (14.4%) |
| 4 | 1147 | 1033 (90.1%) | 435 (37.9%) | 175 (15.3%) |
| 5 | 1604 | 1470 (91.7%) | 726 (45.2%) | 275 (17.1%) |
| p-value | 0.1618 | <0.0001 | 0.0307 | |
| School PA | ||||
| 1 | 1631 | 1454 (89.2%) | 637 (39.1%) | 231 (14.2%) |
| 3 | 1336 | 1224 (91.6%) | 596 (44.6%) | 233 (17.4%) |
| 5 | 830 | 753 (90.7%) | 311 (37.5%) | 123 (14.8%) |
| p-value | 0.0707 | 0.001 | 0.0414 | |
| Access to PA | ||||
| 1 | 309 | 295 (95.5%) | 164 (53.1%) | 56 (18.1%) |
| 2 | 703 | 634 (90.2%) | 263 (37.4%) | 112 (15.9%) |
| 3 | 711 | 642 (90.3%) | 277 (39.0%) | 101 (14.2%) |
| 4 | 1428 | 1261 (88.3%) | 519 (36.3%) | 206 (14.4%) |
| 5 | 646 | 599 (92.72) | 321 (49.7%) | 112 (17.3%) |
| p-value | 0.0004 | <0.0001 | 0.2342 | |
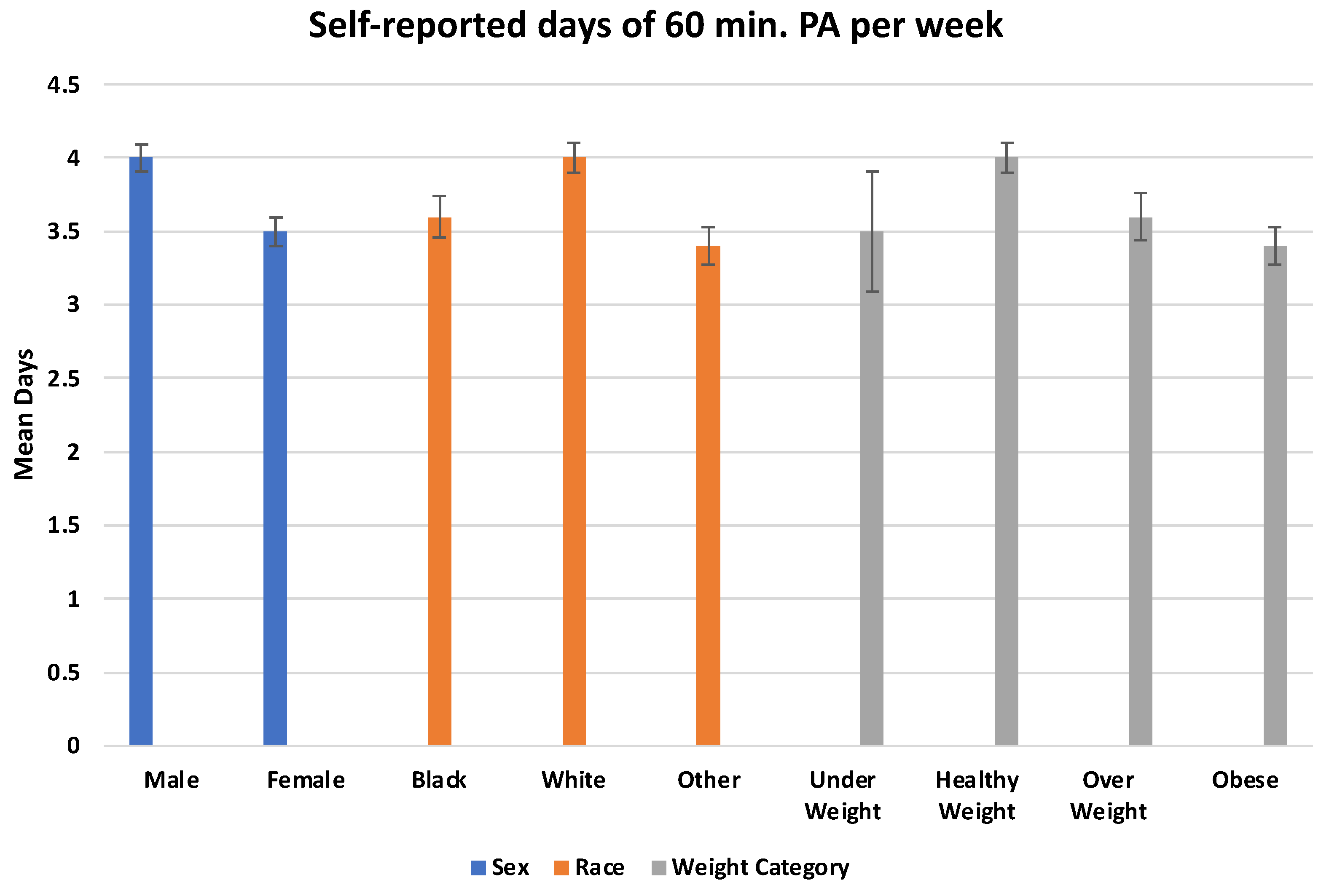
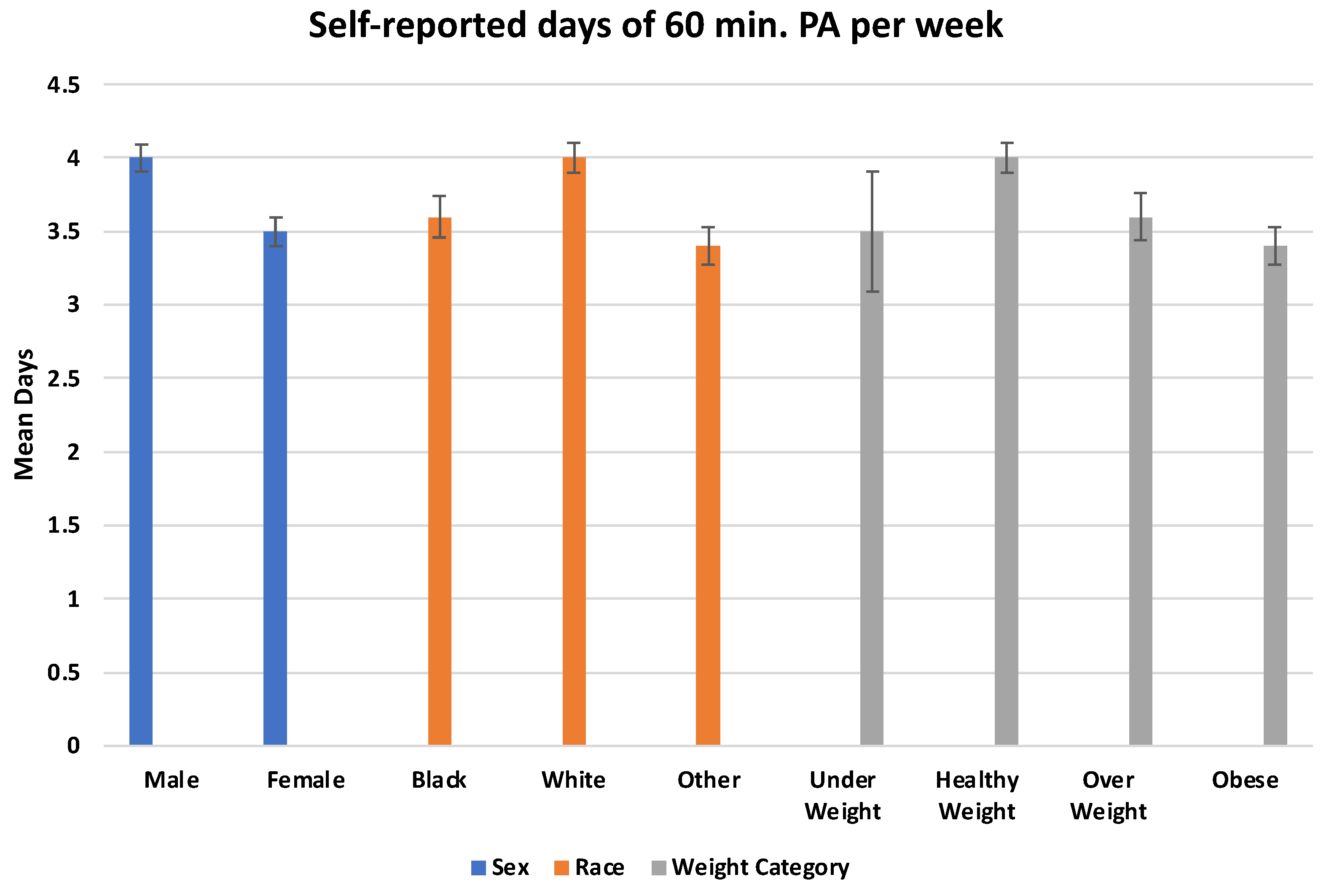
| Sex | ||||
| Female | 1857 | 1643 (88.5%) | 667 (36.0%) | 232 (12.5%) |
| Male | 1940 | 1788 (92.2%) | 877 (45.2%) | 355 (18.3%) |
| p-value | 0.0001 | <0.0001 | <0.0001 | |
| Race | ||||
| Black | 942 | 823 (87.4%) | 357 (37.9%) | 149 (15.8%) |
| White | 1871 | 1720 (92.0%) | 874 (46.7%) | 327 (17.5%) |
| Other | 984 | 888 (90.2%) | 313 (31.8%) | 111 (11.3%) |
| p-value | 0.0006 | <0.0001 | <0.0001 | |
| Weight Category | ||||
| Under Weight | 108 | 94 (87.0%) | 33 (30.6%) | 15 (13.9%) |
| Healthy Weight | 1924 | 1756 (91.3%) | 884 (46.0%) | 344 (17.9%) |
| Overweight | 709 | 630 (88.9%) | 273 (38.5%) | 101 (14.3%) |
| Obese | 1056 | 951 (90.1%) | 354 (33.5%) | 127 (12.03%) |
| p-value | 0.1618 | <0.0001 | 0.0003 |
| Variable | Estimate (B) | Standard Error | p-Value |
|---|---|---|---|
| School PE | 0.108 | 0.033 | 0.0011 |
| Sex | <0.0001 | ||
| Female | −0.526 | 0.070 | <0.0001 |
| Male | - | - | - |
| Race | <0.0001 | ||
| Black | −0.306 | 0.088 | 0.0005 |
| Other | −0.542 | 0.086 | <0.0001 |
| White | - | - | - |
| Weight Category | <0.0001 | ||
| Under Weight | −0.638 | 0.213 | 0.0028 |
| Overweight | −0.281 | 0.095 | 0.0030 |
| Obese | −0.477 | 0.083 | <0.0001 |
| Healthy Weight | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazemzadeh, S.; Opper, C.E.; Fang, X.; Lazorick, S. Determining Trends and Factors Associated with Self-Reported Physical Activity among Adolescents in Rural North Carolina. Int. J. Environ. Res. Public Health 2022, 19, 11417. https://doi.org/10.3390/ijerph191811417
Kazemzadeh S, Opper CE, Fang X, Lazorick S. Determining Trends and Factors Associated with Self-Reported Physical Activity among Adolescents in Rural North Carolina. International Journal of Environmental Research and Public Health. 2022; 19(18):11417. https://doi.org/10.3390/ijerph191811417
Chicago/Turabian StyleKazemzadeh, Sina, Chloe E. Opper, Xiangming Fang, and Suzanne Lazorick. 2022. "Determining Trends and Factors Associated with Self-Reported Physical Activity among Adolescents in Rural North Carolina" International Journal of Environmental Research and Public Health 19, no. 18: 11417. https://doi.org/10.3390/ijerph191811417
APA StyleKazemzadeh, S., Opper, C. E., Fang, X., & Lazorick, S. (2022). Determining Trends and Factors Associated with Self-Reported Physical Activity among Adolescents in Rural North Carolina. International Journal of Environmental Research and Public Health, 19(18), 11417. https://doi.org/10.3390/ijerph191811417