1. Introduction
Stress is a complex response to psychological (e.g., emotional abuse) or biological (e.g., threatening stimuli) challenges. Although reactions to stressors can be adaptive, chronic exposure to stress has been associated with maladaptive long-term changes in emotional, physiological, immune, and behavioural responses [
1,
2]. For example, stress has been proposed as a possible pathogenic mechanism for depression and anxiety [
3,
4,
5]. There is a consistent body of research showing that mindfulness-based interventions (MBIs) are efficacious in reducing symptoms of stress [
6], but little is known about their therapeutic mechanisms [
7]. Monitor and acceptance theory (MAT) [
8,
9] is a recent psychobiological model that aims at explaining the therapeutic mechanisms of mindfulness-based interventions (MBIs) for stress. The theory proposes that MBIs reduce stress by training monitoring and acceptance skills.
Monitoring may be defined as the ability to maintain awareness of present-moment experience and may rely on the attentional neurocognitive subsystems of executive attention and orienting [
9,
10]. Existing research provides preliminary evidence supporting the role of mindfulness training in improving the performance and altering the neurophysiology of these two subsystems of attention [
11,
12,
13,
14]. Acceptance is an attitude of nonjudgement and equanimity toward any experience that may enter the field of awareness [
9]. It is a form of emotion regulation strategy and is the opposite of avoiding or engaging in (stressful) thoughts or experiences. Instead, it consists in welcoming any experience into awareness until it eventually fades, as it is replaced by subsequent experiences. MBIs have consistently been shown to increase self-reported measures of acceptance [
15]. Neuroimaging studies have also shown changes in brain activity in emotion-regulatory areas following mindfulness training (e.g., dorsolateral prefrontal cortex) [
16].
MAT theorises that the practice of mindfulness trains the ability to monitor (i.e., notice, be aware of) present moment experiences and to regulate (distressing/emotional) experiences with acceptance. The interaction between monitoring and acceptance should drive stress reduction. This may imply that these functions are impaired in chronically stressed people and that “improvements” of these functions may underlie the positive effect of MBIs for stress reduction [
8]. However, only preliminary evidence directly supports the idea that monitoring or acceptance are impaired in chronically stressed groups [
17,
18,
19,
20], or that the interaction between these two skills is associated with reduced chronic stress (or other health benefits) [
21]. However, a vast literature shows that stress can generally impact cognition (e.g., working memory, interference inhibition) and emotion regulation, and vice-versa. Specifically, chronically released cortisol (i.e., a hormone secreted during the stress response) is known to bind several brain areas implicated in cognition and emotion and cause impairments in these functions [
22,
23]. Moreover, these brain areas are implicated in the regulation of the stress response and their impairment could contribute to maintaining a maladaptive chronic stress response [
23,
24,
25]. Given this preliminary evidence, it is plausible to hypothesise that monitoring and acceptance are impaired in chronic stress groups compared to controls.
1.1. The Present Study
This theory-driven cross-sectional study aimed primarily at investigating the association of monitoring and acceptance measures with chronic stress. We hypothesised that self-reported measures of chronic stress are correlated with reduced attention monitoring efficiency (i.e., orienting and executive attention) and acceptance skills. We speculated that MBIs are effective in reducing stress in chronically stressed cohorts precisely because their monitoring and acceptance skills are impaired. Secondarily, this study aimed at exploring which specific acceptance variables show stronger correlations with chronic stress, as multiple self-reported measures of trait mindful acceptance exist. Although MAT broadly defines and operationalises acceptance [
9], an acceptance measure showing a stronger correlation with chronic stress might be better suited to test MAT in the context of chronic stress studies compared to other scales. Moreover, we conducted these exploratory analyses to a priori identify a single measure of acceptance for our moderation analyses. Thirdly, this study aimed at exploring whether the interaction between monitoring and acceptance is associated with chronic stress. A significant moderation effect might provide preliminary support to MAT’s hypothesis that the interaction between monitoring and acceptance can drive stress reduction. We assessed self-reported levels of chronic stress using the perceived stress scale (PSS) [
26] and assessed efficiency (i.e., reaction times) in orienting and executive control (i.e., monitoring) using the attentional network test (ANT) [
27]. Finally, we measured acceptance skills with the five facets of mindfulness questionnaire (FFMQ—nonreactivity and nonjudgement subscales) [
15] and Philadelphia mindfulness scale (PHLMS—acceptance subscale) [
28]. To investigate the associations between variables (i.e., main hypothesis), we conducted correlational analyses between our chronic stress measure (i.e., PSS) and each monitoring and acceptance measure. To compare the magnitude of the correlations between our chronic stress measure and our acceptance measures (i.e., exploratory analysis 2), we statistically compared the correlation coefficients associating chronic stress with each of our acceptance measures. Measures showing stronger correlations with chronic stress might be employed in future studies testing MAT. To investigate the association between chronic stress and the interaction between monitoring and acceptance (i.e., exploratory analysis 2), we built two moderation models predicting chronic stress from acceptance, monitoring (i.e., orienting and target detection separately), and their interaction.
1.2. Novelty
This is a theory-driven study of specific hypotheses derived from MAT. Little theoretical research is generally conducted in psychology [
29] and specifically on MAT [
30], and, to our knowledge, only one other published study investigated theory-driven research questions similar to ours [
21]. However, this research employed self-reported measures of monitoring, while we operationalised this variable with a behavioural task. The results of our study are complementary to existing MAT research and studies that serendipitously tested similar hypotheses with similar methods in other areas of psychology (e.g., [
19]).
2. Materials and Methods
2.1. Design
This is a cross-sectional association study. The study was conceptualised, and this report written, according to the Strengthening the Reporting of Observational studies in Epidemiology guidelines for cross-sectional studies (STROBE) [
31]. This study was pre-registered on the AsPredicted website (
https://credlab.wharton.upenn.edu/ (accessed on 6 April 2021); see
Supporting Information S1 for more details).
2.2. Participants
We invited 85 individuals from the general population to complete our questionnaires and behavioural measures. Advertisements and word of mouth were used to recruit participants from the University of Surrey and local area. Participants were included in the study if they were between 18 and 65 years old and had normal or corrected to normal vision. All participants were fluent in English. Participants provided written informed consent and received a GBP 7 shopping voucher or two university credits (if eligible) for their participation. The procedure was approved by the University of Surrey Ethics Committee and The Research Integrity and Governance Office (FHMS 20-21 159 EGA).
The sample size was determined a priori, with a power analysis conducted with the “pwr” package on R [
32,
33]. To compute sample size, we assumed a power of 0.8, and a significance level of
p = 0.05 (two-tailed). Effect size was set at r = 0.3, as this should indicate a medium effect size. We defined r = 0.3 as the smallest effect size of interest, in the context of this study. We determined our effect size of interest based on Cohen’s heuristic, which defines a medium effect size as something visible to the naked eye of the careful observer [
34,
35] and the guidelines proposed by Lakens [
36] who suggest calculating an experimental sample size based on the minimum effect size of interest. The results of our power analysis suggested a sample of 85 participants.
2.3. Procedure
Advertisements and word of mouth were used to recruit participants from the University of Surrey and local area. The advertisement campaign started in September 2021 and ended in March 2022. Potential volunteers contacted the experimenter via email, were screened according to our inclusion criteria, and then invited to participate in the study. On the day of the study, participants read an information sheet explaining the experimental procedure and signed a consent form. Volunteers who gave consent provided demographic data and completed three self-reported questionnaires and a behavioural task (see “
Section 2.4” for more information). The order of the questionnaires (including demographics) and experimental task were randomised to prevent order-effect bias [
37]. After completing the experiment, participants read a debriefing document containing additional information about the experiment, received compensation for their participation, and had the chance to ask for additional information. The entire procedure took approximately 50 min per participant to complete.
2.4. Measures and Variables
Demographics: Age (years), sex assigned at birth (male vs. female), education (years), and ethnicity (White, Black, Asian, Mixed, or Other (please specify)).
Covariate: Subjective level of current sleepiness was measured with the Karolinska Sleepiness Scale (KSS) [
38]. This is a 9-point scale (1 = extremely alert, 2 = very alert, 3 = alert, 4 = rather alert, 5 = neither alert nor sleepy, 6 = some signs of sleepiness, 7 = sleepy—but no difficulty remaining awake, 8 = very sleepy—great effort to keep awake—fighting sleep, and 9 = extremely sleepy—fighting sleep). This sleepiness variable was used to control for sleepiness in our statistical analyses of the data obtained during the experimental tasks. We chose to control for sleepiness because performance in experimental tasks is known to deteriorate as a function of sleepiness [
38]. The KSS is a valid measure of sleepiness [
39].
Chronic stress: We obtained chronic stress measures using the perceived stress scale (PSS) [
26], which was modified to assess perceived stress over the past 3 months [
40]. Participants answered 14 questions on a Likert scale from 1 to 5, where 0 = never and 4 = very often. The PSS was designed to measure chronic stress in the general population along the dimensions of unpredictability, uncontrollability, and overload that relate to the risk for developing adverse health outcomes. It has strong construct validity and reliability across gender, socioeconomic status, age groups, ethnicity, and other demographic characteristics [
26]. The PSS is widely used in studies investigating chronic stress [
41] and was employed in one of the few existing studies of the association between monitoring and chronic stress [
19].
Acceptance: We obtained scores in the acceptance subscales of the five facets of mindfulness questionnaire (FFMQ—nonreactivity and nonjudgement subscales) [
15] and Philadelphia mindfulness scale (PHLMS—acceptance subscale) [
28]. The FFMQ consists of 39 questions on a Likert scale from 1 to 5, where 1 = never or very rarely true and 5 = very often or always true. The two FFMQ subscales were considered as separate acceptance scales and the scores of each participant were summed to compute a third index of acceptance (i.e., FFMQ acceptance total). The PHLMS consist of 20 questions on a Likert scale from 1 to 5, where 1 = never and 5 = very often. The FFMQ and PHLMS were used in the research studies cited by Lindsay and Creswell [
9], when defining acceptance in their mindfulness model. Therefore, these measures have a strong theoretical link to MAT. All questionnaires have good construct validity and reliability (FFMQ [
15,
42]; PHLMS [
28]).
Attention Monitoring: We obtained performance scores (reaction times) in the orienting and target detection subscales of the attentional networks test (ANT) [
27]. According to Lindsay and Creswell [
9], monitoring relies on target detection and orienting, two key attentional subsystems [
10,
43]. The ANT was specifically designed to measure performance in these attentional subsystems. Moreover, the ANT was used in the few existing studies of the association between monitoring and chronic stress [
19]. The duration of the ANT task is 25 min. It should be noted that the ANT can also measure performance in the third attentional subsystem of alerting. However, this subsystem is not theoretically linked to monitoring [
9] and this data were not analysed in this study. The ANT task was programmed following the indications published by Fan et al. [
27] and Westlye et al. [
44]. The task was run on the Gorilla Experiment Builder platform (see the
Section 3 for more information) and is an edited version of an open resource (
https://app.gorilla.sc/openmaterials/50646 (accessed on 23 June 2022)).
2.5. Task Procedure
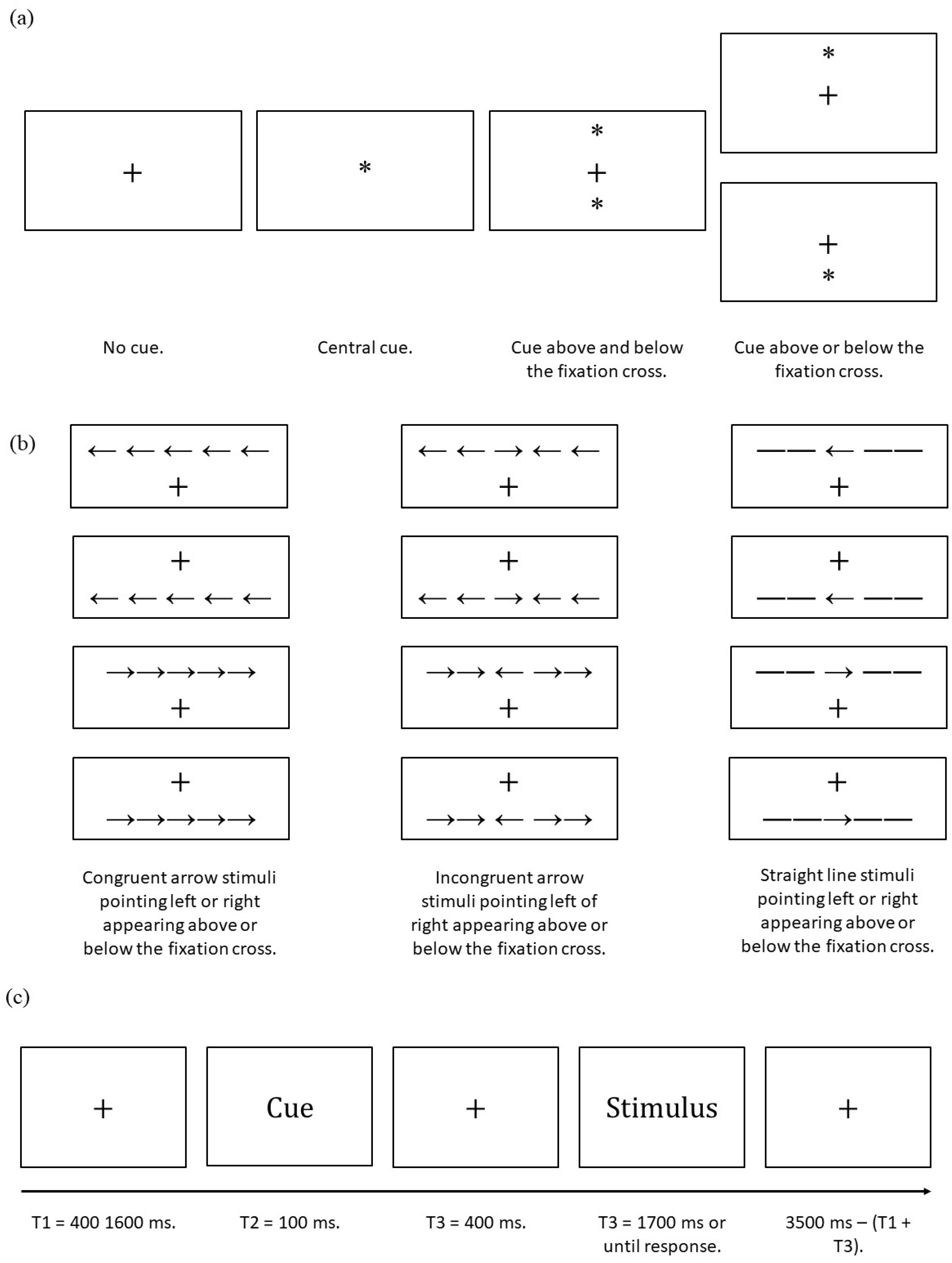
The ANT requires participants to determine whether a central arrow presented in the stimuli phase points towards the left or right. The task consists of three experimental blocks each constituted of 96 trials. Each trial consists of five events. First a fixation cross is presented (random duration 400–1600 ms). Second, an asterisk cue appears (100 ms); this may be a central cue (i.e., appears in place of the fixation cross), no cue, double cue (i.e., two cues appear, one above and one below the fixation cross); or spatial cue (i.e., cue is above or below the fixation cross). The distance of the cues from the fixation cross is the same as the distance of the stimuli (see below) from the fixation cross; this does not include the fixation cue. The spatial cue condition provides spatial information about the upcoming stimuli location with 100% validity. Third, a second fixation cross is presented (400 ms). Then, stimuli are presented (1700 ms elapses or until the participants responds). Stimuli consists of a central arrow surrounded by four distractor flankers. Distractors may be straight lines (i.e., neutral condition) or arrows. Distractor arrows may point in the same or opposite direction of the central target arrow (i.e., congruent or incongruent trials respectively), and stimuli may appear above or below the fixation cross and the arrows may point either left or right. Finally, a third fixation cross (3500 ms minus duration of the first fixation cross minus reaction time in the stimulus phase). Therefore, the ANT has four cue conditions, two target locations, three flanker conditions, and two target directions (
Figure 1). Each trial consists of a combination of these variables and is repeated twice per experimental block. Therefore, there are 96 trials per block.
Prior to the three experimental blocks, the task included two training blocks of 12 trials each. The first block presented a sample of 12 non-cued trials, while the second block presented a sample of 12 cued trials. Each block consisted of four congruent, four incongruent, and four neutral trials, balanced for arrow direction (i.e., left or right) and location (i.e., above or below the fixation cross). In the training blocks only, accuracy feedback was provided after response. Feedback consisted of a tick sign for correct responses (✓) and a cross mark for incorrect responses (×). The feedback signs appeared in the centre of the screen for 200 ms.
Arrow and line stimuli had an approximate size of 6.24 mm (i.e., 0.55° visual angle) and were separated by approximately 0.0681 mm (i.e., 0.06° visual angle). An array of five stimuli, including the separation between them, consisted of a total of approximately 3.950 cm (i.e., 3.08° visual angle). The distance between the fixation cross and stimuli array or asterisk was approximately 1.25 cm (i.e., 1.06° visual angle). All the above was designed in accordance with Fan et al. [
27]. Details about the asterisk and fixation cross size were not specified in the original article by Fan et al.; therefore, we followed the guidelines offered by Westlye et al. [
44]. Specifically, the fixation cross size was approximately 0.5 cm × 0.5 cm (i.e., 0.4407° × 0.4407° visual angle), while the asterisk diameter was approximately 0.3 cm (i.e., 0.2644° visual angle).
2.6. ANT Coefficients
To measure the efficiency in the orienting and target detection subsystems of attention, we recorded each participants’ reaction times (
RT) in determining the direction of the target arrow during the stimulus phase. Then, we computed the mean
RT for the central cue, spatial cue, incongruent trials, and congruent trials conditions. Finally, we computed our coefficients as follows:
Following the guidelines by Fan and Posner [
45], Fan et al. [
46], and Medina and Barraza [
47], we interpreted higher orienting scores as more efficient compared to lower scores, and lower target detection scores as more efficient compared to higher scores. Only the reaction times associated with a correct response were considered in the analyses. Incorrect responses and omissions were excluded [
27].
6. Discussion
This study tested the hypothesis that chronic stress is associated with impaired mindful attention monitoring and acceptance skills, as defined in the MAT by Lindsay and Creswell [
9]. Our results partially support this hypothesis. Specifically, self-reported chronic stress, measured with the PSS, was significantly negatively associated with all the self-reported acceptance measures. The effect sizes of these associations were medium or large, with the strongest association and largest effect size, in terms of absolute values, observed between PSS and the composite scale obtained by merging the two acceptance subscales of the FFMQ (i.e., FFMQ acceptance total). These results may be explained by hypothesising that people reporting higher levels of chronic stress may find MBIs helpful [
6] precisely because these interventions train their ability to regulate emotions via acceptance. Improvement in acceptance, a possible emotion regulation mechanism [
62], may then help regulate stress levels [
7] and produce the observed health benefits. Future studies could empirically test this hypothesis by means of randomized controlled trials investigating whether specific changes in acceptance, as defined by Lindsay and Creswell [
9], in people reporting higher levels of chronic stress are associated with or mediate reduced chronic stress, following an MBI.
Contrary to the predictions, our results show that self-reported chronic stress was not associated with either of the two components of mindful attention monitoring and the absolute effect sizes of these associations were trivial. Despite this, it should be noted that the confidence intervals extending from the
r effect size indicator were rather large for both monitoring components, spanning from approximately −0.2 to +0.2. This might mean that some less trivial association might exist between these constructs. However, even considering the extremes of these confidence intervals, the effect sizes of the associations between chronic stress, orienting, and target detection, appear to be small. Thus, our results do not support our speculation that MBIs may act by training impaired monitoring skills in people reporting high levels of stress. However, it may still be hypothesised that MBIs promote stress reduction by improving monitoring skills above and beyond “normative/healthy” levels in people that do not show impaired monitoring skills, but report high chronic stress levels. Preliminary support for this alternative hypothesis is given by a vast literature documenting altered or improved cognition in meditators compared to healthy non-meditators (e.g., [
63]). Alternatively, it could be hypothesised that chronic stress impairs cognition and emotion, but this effect cannot be observed behaviourally, only physiologically. Preliminary support for this alternative hypothesis is given by several publications reporting that people with stress-related illnesses (e.g., affective disorders) show differential brain activity, but not behavioural performance, during cognitive tasks, compared to controls (e.g., [
64]). Finally, it may also be hypothesised that we did not observe the predicted results because of our theoretical or operational definition of monitoring. For example, monitoring may be a function of working memory, instead of attention, as defined by Petersen and Posner [
10]. For a review on the relationship between working memory and mindfulness training see Jha et al. [
65]. Future studies may further investigate the association between chronic stress and attention monitoring, adding to the limited existing literature.
We conducted exploratory analyses to follow up the observed negative correlations between PSS and the acceptance scales and tried to determine differences in magnitude between these associations. The results of these analyses showed that the correlation between chronic stress and the composite scale—obtained by merging the two acceptance subscales of the FFMQ (i.e., FFMQ acceptance total)—was larger than the correlation between chronic stress and FFMQ nonreactivity. This may imply that FFMQ acceptance total may be a more sensitive measure of change in acceptance compared to FFMQ nonreactivity, in the context of chronic stress. However, none of the other statistical comparisons showed differences in magnitude between correlations. This may imply that any of these scales may be equally employed to successfully detect changes in acceptance skills, in the context of chronic stress studies.
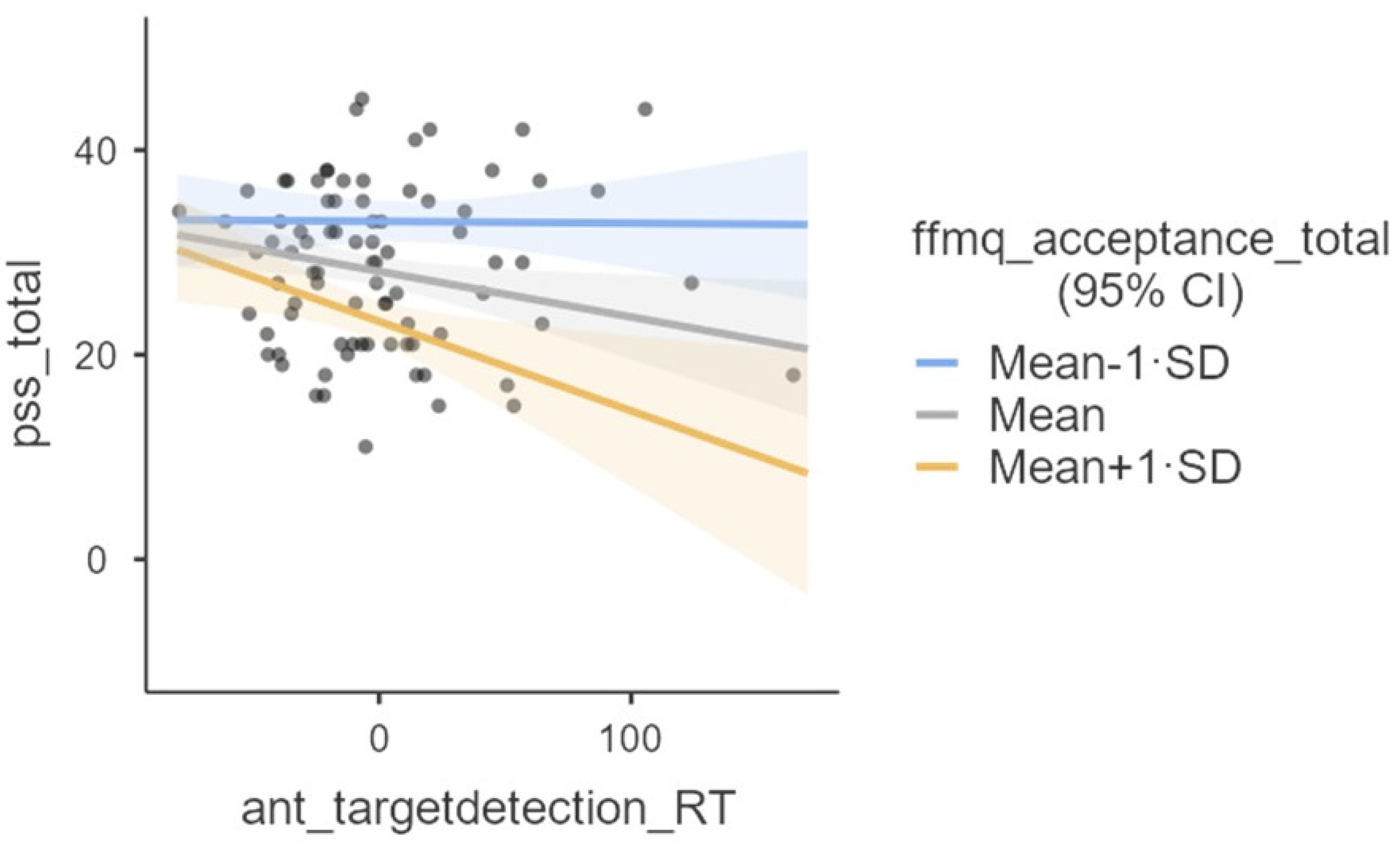
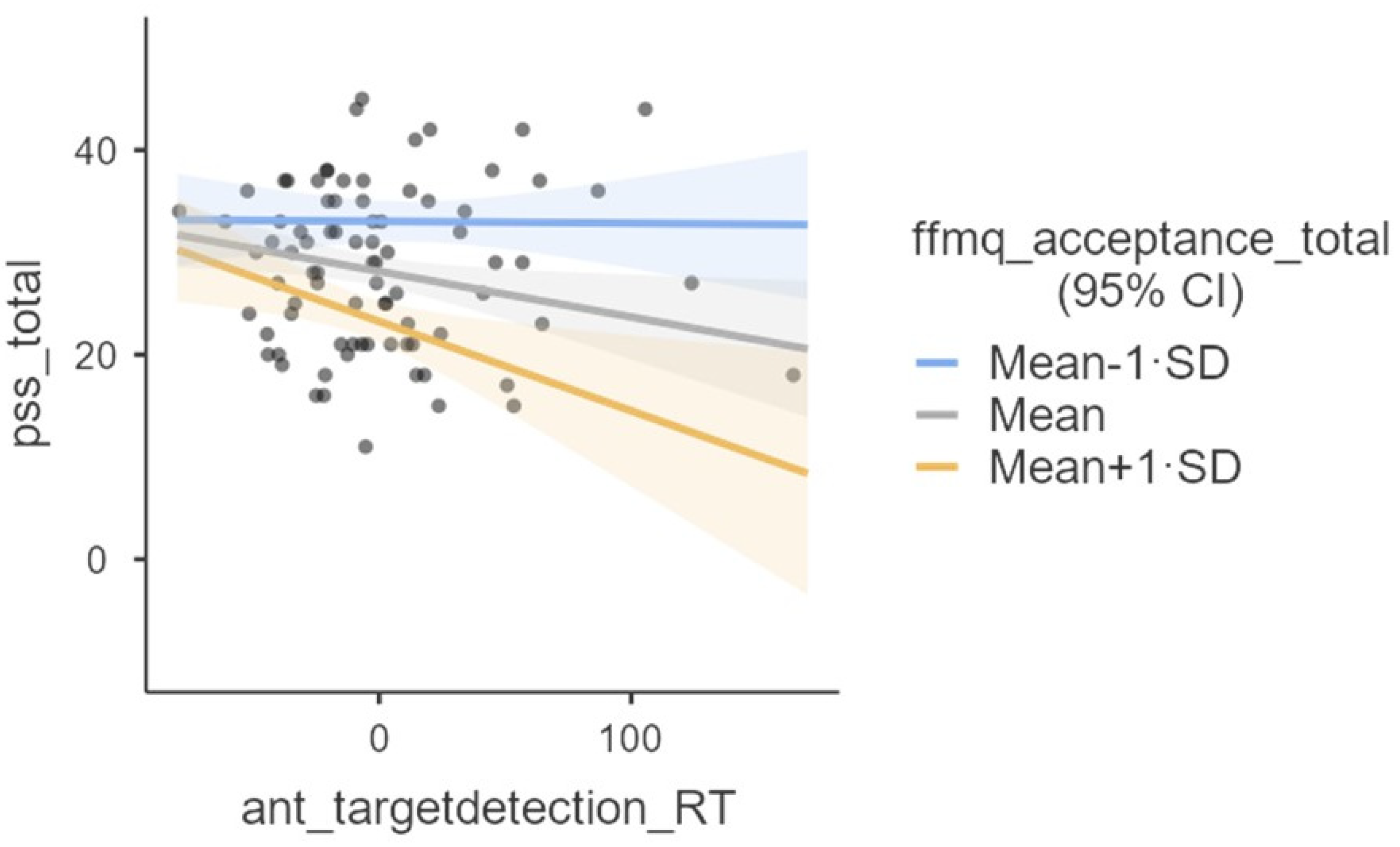
We conducted exploratory analyses to investigate whether the relationship between chronic stress (i.e., PSS scores) and monitoring (i.e., orienting and target detection separately) is moderated by acceptance (i.e., the summation of the scores of the FFMQ acceptance subscales). According to MAT, our results show that the relationship between target detection and chronic stress is moderated by acceptance. The effect size of the interaction appeared to be statistically small. However, contrary to MAT’s prediction, the association between the target detection coefficient (note that the larger this coefficient, the more inefficient the network [
45]) and chronic stress became more negative as a function of acceptance. Thus, at higher levels of acceptance, inefficient target detection is associated with lower chronic stress. These unexpected results are difficult to explain and might be due to random variability. For example, one possibility is that target detection scores might not be reflective of differences in attention efficiency, but of strategies in approaching the task which might have randomly influenced the performance of our participants [
45]. For example, people reporting lower stress levels might have preferred accuracy to speed, while the other participants might have preferred to give fast responses. Nevertheless, it is also possible that contrary to MAT’s prediction, at higher levels of acceptance, less efficient target detection is associated with lower chronic stress. Contrary to MAT predictions, we did not find a statistically significant moderation effect for our second moderation model employing orienting as a predictor, instead of target detection. The effect sizes of this non-significant interaction were trivial. Future intervention, controlled studies employing a MBI might further investigate the association of the interaction between monitoring and acceptance, and chronic stress.
Limitations
A possible limitation of this study is that we operationalised each one of our phenomena of interest only on one level of description. That is, monitoring was operationalised as behavioural performance, while acceptance and chronic stress were operationalised as self-reported questionnaire scores. Future studies may measure these phenomena on multiple levels of description. For example, acceptance may be measured with questionnaires and task-based neuroimaging [
66]. A possible second limitation of our study is the sample size, which was calculated assuming a medium effect size of the effects we investigated. As the monitoring and moderation effects sizes (but not those related to the acceptance measures) were small, a very large sample size might have allowed us to find significant results. However, it is unclear whether finding significant results for such small effect sizes would be of practical or theoretical interest [
67].




{kind=link}
{kind=link}