
Multimodal Diabetes Empowerment for Older Adults with Diabetes



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
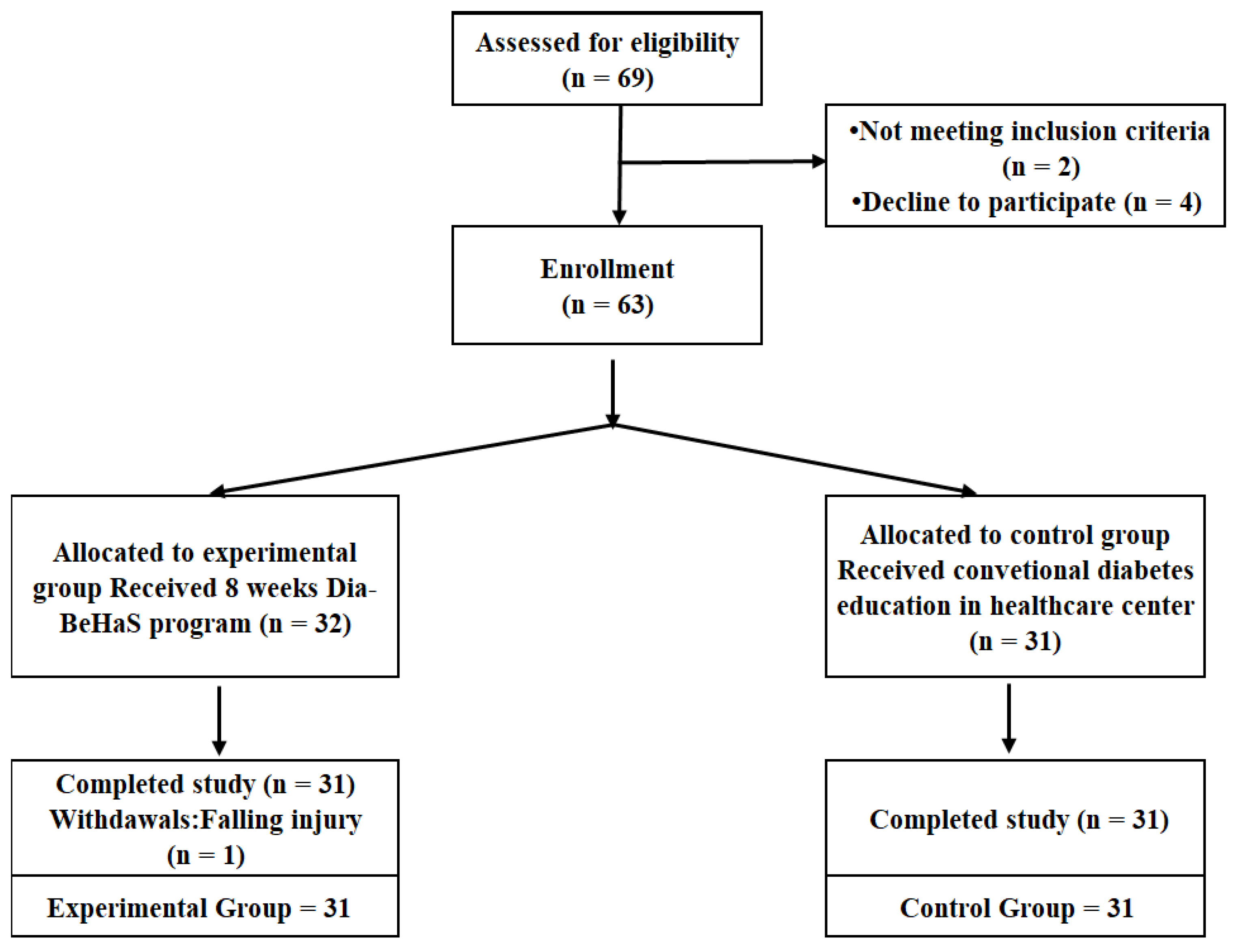
2.2. Sample and Setting
2.3. Primary and Secondary Outcomes
2.4. Process of Dia-Empower Program Development
- (a)
- (b)
- Designing the program: Program designed for 8 weeks and 8 sessions.
- (c)
- Reviewing feasibility and safety based on expert opinions: Feasibility and content validity were reviewed by experts.
- (d)
- Evaluating the program: Applied and tested the program.
2.5. Intervention (the Dia-Empower Program)
2.6. Ethical Consideration
2.7. Statistical Analysis
3. Results
3.1. Homogeneity Test between the Groups
3.2. Hypothesis 1: A Greater Change Would Be Found in the Experimental Group Compared to the Control Group in the Primary Outcome (Diabetes Self-Care and Empowerment) Scores Following the Intervention
3.3. Hypothesis 2: A Greater Change Would Be Found in the Experimental Group Compared to the Control Group in the Secondary Outcome (Body Composition and Physical Function) Scores Following the Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peric, S.; Stulnig, T.M. Diabetes and COVID-19. Wien. Klin. Wochenschr. 2020, 132, 356–361. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Report on Diabetes: Executive Summary. Available online: https://www.who.int/publications/i/item/who-nmh-nvi-16.3 (accessed on 3 August 2022).
- International Diabetes Federation. IDF Diabetes Atlas 7th Edition. Available online: https://www.diabetesatlas.org/upload/resources/previous/files/7/IDF%20Diabetes%20Atlas%207th (accessed on 3 August 2022).
- Korean Diabetes Association. Diabetes Fact Sheet in Korea 2018. Available online: https://www.diabetes.or.kr/bbs/?code=fact_sheet&mode=view&number=1546&page=1&code=fact_sheet (accessed on 3 August 2022).
- Baldoni, N.R.; Aquino, J.A.; Sanches-Giraud, C.; Oliveira, C.L.; Figueiredo, R.C.; Cardoso, C.S.; Santos, T.R.; Alves, G.C.; Fabbro, A.L.; Baldoni, A.O. Collective empowerment strategies for patients with Diabetes Mellitus: A systematic review and meta-analysis. Prim. Care Diabetes 2017, 11, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Sim, K.H.; Wang, B.R.; Noh, J.W.; Lee, M.K.; Kwon, Y.D. Diabetes education compliance and knowledge among diabetes patients: Analysis of patients who refuse diabetes education at an academic medical center. J. Korean Diabetes 2014, 15, 51–56. [Google Scholar] [CrossRef]
- Swedish Council on Health Technology. SBU Systematic Review Summaries. Dietary Treatment of Diabetes: A Systematic Review. Available online: https://pubmed.ncbi.nlm.nih.gov/28876807 (accessed on 3 August 2022).
- Kirkman, M.S.; Briscoe, V.J.; Clark, N.; Florez, H.; Haas, L.B.; Halter, J.B.; Huang, E.S.; Korytkowski, M.T.; Munshi, M.N.; Odegard, P.S.; et al. Diabetes in older adults: A consensus report. J. Am. Geriatr. Soc. 2012, 60, 2342–2356. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, R.; DiChiacchio, T.; Barker, K. Interventions for self-management of type 2 diabetes: An integrative review. Int. J. Nurs. Sci. 2019, 6, 70–91. [Google Scholar] [CrossRef]
- Wong, A.K.; Bayuo, J.; Wong, F.K.; Yuen, W.S.; Lee, A.Y.; Chang, P.K.; Lai, J.T. Effects of a nurse-led telehealth self-care promotion program on the quality of life of community-dwelling older adults: Systematic review and meta-analysis. J. Med. Internet Res. 2022, 24, e31912. [Google Scholar] [CrossRef]
- Anderson, R.M.; Funnell, M.M.; Butler, P.M.; Arnold, M.S.; Fitzgerald, J.T.; Feste, C.C. Patient empowerment: Results of a randomized controlled trial. Diabetes Care 1995, 18, 943–949. [Google Scholar] [CrossRef]
- Anderson, R.M.; Funnell, M.; Fitzgerald, J.T.; Marrero, D.G. The diabetes empowerment scale: A measure of psychosocial self-efficacy. Diabetes Care 2000, 23, 739–743. [Google Scholar] [CrossRef]
- Anderson, R.M.; Funnell, M.M.; Arnold, M. Using the empowerment approach to help patients change behavior. In Practical Psychology for Diabetes Clinicians; American Diabetes Association: Arlington County, VA, USA, 2002; pp. 3–12. [Google Scholar]
- Adolfsson, E.T.; Walker-Engström, M.; Smide, B.; Wikblad, K. Patient education in type 2 diabetes e a randomized controlled 1-year follow-up study. Diabetes Res. Clin. Pract. 2007, 76, 341–350. [Google Scholar] [CrossRef]
- Sugiyama, T.; Steer, W.N.; Wenger, N.S.; Duru, O.K.; Mangione, C.M. Effect of a community-based diabetes self-management empowerment program on mental health-related quality of life: A causal mediation analysis from a randomized controlled trial. BMC Health Serv. Res. 2015, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- Sperl-Hillen, J.; Beaton, S.; Fernandes, O.; Worley, A.V.; Vazquez-Benitez, G.; Parker, E.; Hanson, A.; Lavin-Tompkins, J.; Glasrud, P.; Davis, H.; et al. Comparative effectiveness of patient education methods for type 2 diabetes: A randomized controlled trial. Arch. Intern. Med. 2011, 171, 2001–2010. [Google Scholar] [CrossRef] [PubMed]
- McGowan, P. The relative effectiveness of self-management programs for type 2 diabetes. Can. J. Diabetes 2015, 39, 411–419. [Google Scholar] [CrossRef]
- Kim, J.I.; Lee, K.J.; Kim, S.I.; Min, S.H. Effects of BeHaS exercise program on pain, balance and fall efficacy in elderly with osteoarthritis. J. Korean Acad. Fundam. Nurs. 2007, 14, 181–188. [Google Scholar]
- Kim, H.; Kim, S.K.; Kim, J.I.; Kim, S.A.; Jun, Y.S.; Park, K.O. The converge effects of the BeHaS exercise program on health status, depression and suicidal ideation in female elderly who live alone in community. J. Korea Converg. Soc. 2018, 9, 111–119. [Google Scholar] [CrossRef]
- Park, S.Y. Effects of BeHaS Exercise Program on Health Related Physical Strength, Stress, Self-Esteem and Quality of Life in Breast Cancer Survivors; Chungnam National University: Daejeon, Korea, 2009. [Google Scholar]
- Kim, S.; Kim, S. Interpersonal caring: A theory for improved self-esteem in patients with long-term serious mental illness–I. Asian Nurs. Res. 2017, 1, 11–22. [Google Scholar] [CrossRef]
- Kim, T. Effects of BeHaS Program on Physiological, Psychological Factor, Self-Efficacy, and Self Care Behavior in Older Adults with Hypertension; Chungnam National University: Daejeon, Korea, 2009. [Google Scholar]
- Kim, S.-A. The effects of BeHaS exercise program on muscle strength and flexibility in institutionalized elders. J. Muscle Jt. Health 2011, 18, 93–102. [Google Scholar] [CrossRef]
- Park, K.O.; Lee, H.J.; Lee, Y.H.; Cho, J.H.; Kim, B.H.; Song, Y.S. Reliability and validity of Korean version of Diabetes Empowerment Scale short form. J. Korean Acad. Fundam. Nurs. 2017, 24, 296–303. [Google Scholar] [CrossRef]
- Anderson, R.M.; Funnell, M.M.; Nwankwo, R.; Gillard, M.L.; Oh, M.; Fitzgerald, J.T. Evaluating a problem-based empowerment program for African Americans with diabetes: Results of a randomized controlled trial. Ethn. Dis. 2005, 15, 671–678. [Google Scholar] [CrossRef]
- Funnell, M.M.; Brown, T.L.; Childs, B.P.; Haas, L.B.; Hosey, G.M.; Jensen, B.; Maryniuk, M.; Peyrot, M.; Piette, J.D.; Reader, D.; et al. National standards for diabetes self-management education. Diabetes care 2010, 33, S89–S96. [Google Scholar] [CrossRef]
- Carroll, C.; Patterson, M.; Wood, S.; Booth, A.; Rick, J.; Balain, S. A conceptual framework for implementation fidelity. Implement. Sci. 2007, 2, 40. [Google Scholar] [CrossRef]
- Anderson, R.M.; Fitzgerald, J.T.; Gruppen, L.D.; Funnell, M.M.; Oh, M.S. The diabetes empowerment scale-short form (DES-SF). Diabetes Care 2003, 26, 1641–1642. [Google Scholar] [CrossRef] [PubMed]
- Goh, G.; Tan, N.C.; Malhotra, R.; Padmanabhan, U.; Barbier, S.; Allen, J.C.; Østbye, T. Short-term trajectories of use of a caloric-monitoring mobile phone app among patients with type 2 diabetes mellitus in a primary care setting. J. Med. Internet Res. 2015, 17, e3938. [Google Scholar] [CrossRef] [PubMed]
- Grover, A.; Joshi, A. An overview of chronic disease models: A systematic literature review. Glob. J. Health Sci. 2015, 7, 210–227. [Google Scholar] [CrossRef]
- Boulé, N.G.; Haddad, E.; Kenny, G.P.; Wells, G.A.; Sigal, R.J. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: A meta-analysis of controlled clinical trials. JAMA 2001, 286, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.I.; Kim, S.K. Effects of the BeHaS exercise program on self-esteem, balance, and flexibility in community-dwelling adults experiencing pain. Indian J. Sci. Technol. 2015, 8, 624. [Google Scholar] [CrossRef]
- Kim, J.I.; Kim, J.Y.; Park, E.O.; Park, J.A.; Park, K.O.; Choi, Y.H. Effects of the BeHaS Program on physical factors and self-esteem of elderly women in a senior center: A pilot study. J. Korea Converg. Soc. 2020, 11, 373–383. [Google Scholar] [CrossRef]
- Oh, H.K.; Lee, E.J. The influence of self-care behaviors, empowerment and social support on glycosylated hemoglobin in patients with type 2 diabetes. J. Korean Acad. Community Health Nurs. 2017, 28, 216–225. [Google Scholar] [CrossRef][Green Version]
- Park, I.H.; Jung, Y.K. Effects of empowerment education program for the patients having rheumatoid arthritis on empowerment, health status and self-care activities. Arthritis Rheumatol. 2001, 44, 207. [Google Scholar]
- Park, C.; Song, M.; Cho, B.; Lim, J.; Song, W.; Chang, H.; Park, Y.-H. Effects of a multi-disciplinary approached, empowerment theory based self-management intervention in older adults with chronic illness. J. Korean Acad. Nurs. 2015, 45, 192–201. [Google Scholar] [CrossRef]
- Tsay, S.-L.; Hung, L.-O. Empowerment of patients with end-stage renal disease—A randomized controlled trial. Int. J. Nurs. Stud. 2004, 41, 59–65. [Google Scholar] [CrossRef]
- Schmittdiel, J.A.; Shortell, S.M.; Rundall, T.G.; Bodenheimer, T.; Selby, J.V. Effect of primary health care orientation on chronic care management. Ann. Fam. Med. 2006, 4, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-Y.; Gu, M.O. Development and effects of a motivational interviewing self-management program for elderly patients with diabetes mellitus. J. Korean Acad. Nurs. 2015, 45, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, V.; Pazos-Couselo, M.; González-Rodríguez, M.; Rodríguez-González, R. Educational programs in type 2 diabetes designed for community-dwelling older adults: A systematic review. Geriatr. Nurs. 2022, 46, 157–165. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Stages | Week | Empowerment (10 min) | Education (10 min) | Exercise (40 min) | Remarks |
|---|---|---|---|---|---|
| Dialog | 1st | Understand my body | Overview of diabetes | Body relaxation, Preparation of exercise, Main exercise, (see Supplementary Materials) Final exercise | Pre-test Opening ceremony |
| 2nd | Who is the owner of my body? | Blood sugar management/Exercise | Practice and group discussion and sharing experiences Diabetes self-care guidebook provided. Practical tasks at home and self-care checklist provided. Capacity building Action task used. | ||
| Discovery | 3rd | Find my strengths | How to medicate/manage with stress | ||
| 4th | Explain my worth | Foot care | |||
| 5th | My good habits | Smoking/Drinking | |||
| Development | 6th | Find my resources | Diabetes diet | ||
| 7th | Become a self-health motivator | Prevention of complications | |||
| 8th | Express hope for the future | Risk notification mark | Post- test & Closing ceremony |
| Characteristics | Categories | Exp. (n = 31) | Cont. (n = 31) | t or χ² | p |
|---|---|---|---|---|---|
| n (%) or Mean (±SD) | n (%) or Mean (±SD) | ||||
| Age | (years) | 71.03 (±4.11) | 71.45 (±4.76) | 0.37 | 0.712 |
| Sex | Woman | 12 (38.7) | 16 (51.6) | 1.04 | 0.444 |
| Man | 19 (61.3) | 15 (48.4) | |||
| Diabetic Complication | Yes | 17 (54.8) | 14 (45.2) | 0.58 | 0.446 |
| No | 14 (45.2) | 17 (54.8) | |||
| HbA1c | (%) | 7.59 (±0.93) | 7.25 (±0.61) | −1.75 | 0.085 |
| Education level | ≤Elementary school | 13 (41.95) | 8 (25.8) | 7.48 | 0.113 |
| Middle High school | 12 (38.7) | 16 (51.6) | |||
| ≤College | 6 (19.35) | 7 (22.6) | |||
| Having Religion | Yes | 21 (67.7) | 13 (41.9) | 4.17 | 0.073 |
| No | 10 (32.3) | 18 (58.1) | |||
| Having a job | Yes | 11 (35.5) | 9 (29.0) | 0.30 | 0.786 |
| No | 20 (64.5) | 22 (71.0) | |||
| Subjective Economic state | Stable | 10 (32.2) | 11 (35.5) | 5.62 | 0.229 |
| Moderate | 10 (32.3) | 15 (48.4) | |||
| Unstable | 11 (35.5) | 5 (16.1) | |||
| Alcohol Drinking | No | 19 (61.3) | 16 (51.7) | 9.76 | 0.534 |
| Yes | 12 (38.7) | 15 (48.3) | |||
| Smoking | Yes | 3 (9.7) | 2 (6.5) | 0.22 | 1.000 |
| No | 28 (90.3) | 29 (93.5) | |||
| Duration of DM | (years) | 15.35 (±10.91) | 13.71 (±9.26) | −0.64 | 0.524 |
| Cognitive function | (MMSE KC) | 27.99 (±1.11) | 27.75 (±1.24) | −0.82 | 0.415 |
| Perceived Health Status | Good | 6 (19.3) | 7 (22.6) | 3.06 | 0.548 |
| Fair | 11 (35.5) | 16 (51.6) | |||
| Poor | 14 (45.2) | 8 (25.8) | |||
| Health index | FBS (mg/dL) | 145.45 (±40.28) | 138.23 (±25.16) | −0.85 | 0.400 |
| HbA1c (%) | 7.59 (±0.93) | 7.25 (±0.61) | −1.75 | 0.086 | |
| SBP (mmHg) | 133.45 (±19.15) | 140.58 (±18.93) | 1.47 | 0.146 | |
| DBP (mmHg) | 75.68 (±12.61) | 79.94 (±9.69) | 1.49 | 0.141 | |
| Anthropometrics | Body weight (kg) | 63.84 (±9.39) | 64.69 (±8.18) | 0.38 | 0.712 |
| BMI | 25.24 (±3.47) | 24.71 (±2.70) | −0.66 | 0.511 | |
| Skeletal muscle mass (kg) | 21.75 (±6.22) | 24.22 (±4.31) | 1.82 | 0.074 | |
| Body fat rate (%) | 34.07 (±8.45) | 31.30 (±6.39) | −1.45 | 0.151 | |
| Physical Function | Handgrip strength (Rt.) (kg) | 24.17 (±7.00) | 24.79 (±5.49) | 0.39 | 0.698 |
| Handgrip strength (Lt.) (kg) | 22.49 (±6.33) | 24.04 (±5.93) | 0.99 | 0.327 | |
| Shoulder flexibility (Rt.) (cm) | 17.03 (±12.28) | 21.39 (±12.13) | 1.40 | 0.165 | |
| Shoulder flexibility (Lt.) (cm) | 20.29 (±9.86) | 24.16 (±11.45) | 1.43 | 0.159 | |
| SDSCA | Total | 27.84 (±13.85) | 25.90 (±4.97) | 0.17 | 0.864 |
| Diet | 13.94 (±5.82) | 12.65 (±5.81) | −0.87 | 0.386 | |
| Exercise | 5.29 (±4.58) | 6.35 (±4.79) | 0.89 | 0.375 | |
| Glucose monitoring | 4.06 (±4.73) | 2.93 (±3.08) | −1.11 | 0.270 | |
| Foot care | 4.55 (±4.23) | 6.55 (±4.86) | 1.73 | 0.089 | |
| DES | Total | 24.68 (±6.71) | 25.90 (±4.97) | 0.82 | 0.417 |
| Variables | Categories | Group | Baseline | Posttest | Changes in Score (Post-Baseline) | |
|---|---|---|---|---|---|---|
| Mean (±SD) | Mean (±SD) | Diff-Mean (±SD) | t (p) | |||
| SDSCA | Total | Exp. | 27.84 (±13.85) | 57.45 (±7.71) | 29.61 (±14.30) | −8.16 (<0.001) |
| Cont. | 28.39 (±11.00) | 32.00 (±10.25) | 3.61 (±10.49) | |||
| Diet | Exp. | 13.94 (±5.82) | 22.52 (±3.15) | 8.58 (±5.52) | 4.48 (<0.001) | |
| Cont. | 12.65 (±5.81) | 14.19 (±4.93) | 1.55 (±5.92) | |||
| Exercise | Exp. | 5.29 (±4.58) | 11.32 (±2.8) | 6.03 (±5.39) | 4.63 (<0.001) | |
| Cont. | 6.35 (±4.79) | 6.77 (±3.48) | 0.42 (±4.06) | |||
| Glucose monitoring | Exp. | 4.06 (±4.73) | 10.52 (±3.66) | 6.45 (±4.65) | 6.13 (<0.001) | |
| Cont. | 2.93 (±3.08) | 3.26 (±2.72) | 0.32 (±3.05) | |||
| Foot care | Exp. | 4.55 (±4.23) | 13.09 (±1.72) | 8.55 (±4.33) | 5.82 (<0.001) | |
| Cont. | 6.55 (±4.86) | 7.77 (±4.74) | 1.26 (±5.50) | |||
| DES | Exp. | 24.68 (±6.71) | 37.74 (±2.77) | 13.06 (±7.00) | −9.03 (<0.001) | |
| Cont. | 25.90 (±4.97) | 25.26 (±4.40) | 0.65 (±4.72) | |||
| Variables | Categories | Group | Baseline | Posttest | Changes in Score (Post-Baseline) | |
|---|---|---|---|---|---|---|
| Mean (±SD) | Mean (±SD) | Diff-Mean (±SD) | t (p) | |||
| Anthropometrics | Body weight (kg) | Exp. | 63.84 (±9.39) | 62.94 (±9.41) | −0.90 (±1.59) | 0.75 (0.454) |
| Cont. | 64.69 (±8.18) | 64.20 (±7.98) | −0.49 (±1.14) | |||
| BMI | Exp. | 25.24 (±3.47) | 24.84 (±3.51) | −0.33 (±0.62) | 1.29 (0.201) | |
| Cont. | 24.71 (±2.70) | 24.56 (±2.58) | −0.14 (±0.46) | |||
| Skeletal muscle mass (kg) | Exp. | 21.75 (±6.22) | 23.64 (±4.94) | 1.88 (±5.25) | 2.32 (0.024) | |
| Cont. | 24.22 (±4.31) | 23.84 (±4.32) | −0.38 (±1.38) | |||
| Body fat rate (%) | Exp. | 34.07 (±8.45) | 31.19 (±8.46) | −2.87 (±2.84) | 3.32 (0.002) | |
| Cont. | 31.30 (±6.39) | 31.21 (±6.52) | −0.08 (±3.70) | |||
| Physical Function | Handgrip strength (Rt.) (kg) | Exp. | 24.17 (±7.00) | 26.46 (±6.16) | 2.29 (±1.96) | −3.96 (<0.001) |
| Cont. | 24.79 (±5.49) | 25.13 (±5.15) | 0.34 (±1.93) | |||
| Handgrip strength (Lt.) (kg) | Exp. | 22.49 (±6.33) | 24.96 (±6.07) | 2.45 (±1.94) | −4.76 (<0.001) | |
| Cont. | 24.04 (±5.93) | 24.11 (±5.86) | 0.08 (±1.97) | |||
| Shoulder flexibility (Rt.) (cm) | Exp. | 17.03 (±12.28) | 11.16 (±10.56) | −5.87 (±5.43) | 5.20 (<0.001) | |
| Cont. | 21.39 (±12.13) | 21.35 (±11.39) | −0.03 (±3.09) | |||
| Shoulder flexibility (Lt.) (cm) | Exp. | 20.29 (±9.86) | 14.87 (±8.06) | −5.42 (±5.71) | 4.51 (0.001) | |
| Cont. | 24.16 (±11.45) | 23.68 (±11.13) | −0.48 (±2.13) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.; Song, Y. Multimodal Diabetes Empowerment for Older Adults with Diabetes. Int. J. Environ. Res. Public Health 2022, 19, 11299. https://doi.org/10.3390/ijerph191811299
Park K, Song Y. Multimodal Diabetes Empowerment for Older Adults with Diabetes. International Journal of Environmental Research and Public Health. 2022; 19(18):11299. https://doi.org/10.3390/ijerph191811299
Chicago/Turabian StylePark, Keumok, and Youngshin Song. 2022. "Multimodal Diabetes Empowerment for Older Adults with Diabetes" International Journal of Environmental Research and Public Health 19, no. 18: 11299. https://doi.org/10.3390/ijerph191811299
APA StylePark, K., & Song, Y. (2022). Multimodal Diabetes Empowerment for Older Adults with Diabetes. International Journal of Environmental Research and Public Health, 19(18), 11299. https://doi.org/10.3390/ijerph191811299