

Profiles of Ecosystemic Resilience and Risk: American Indian Adolescent Substance Use during the First Year of the COVID-19 Crisis

Abstract
:1. Introduction
1.1. Impact of COVID-19 on American Indian Communities
1.2. Impact of COVID-19 on AI Adolescents Health Risk Behaviors
1.3. Ecosystemic Resilience Model
1.4. Present Study
Hypotheses
2. Materials and Methods
2.1. School Sampling and Recruitment
2.2. Participants
2.3. Procedures
2.4. Measures
2.4.1. Indicators of Latent Profiles
Internal Vulnerability
Internal Assets
External Adversity
External Resources
2.4.2. Distal Outcomes
2.5. Analytical Procedures
3. Results
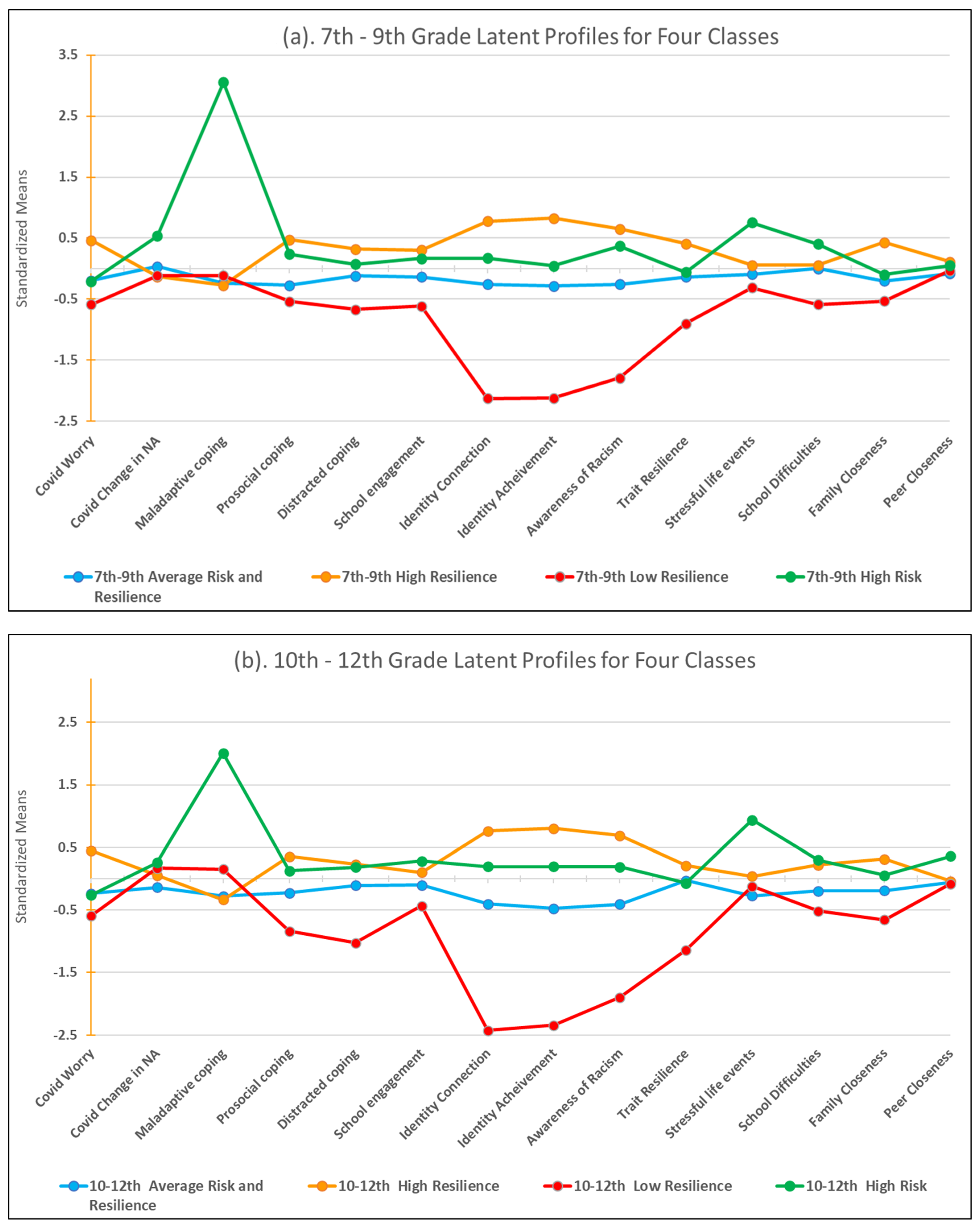
3.1. Latent Profiles of Ecosystemic Resilience
Latent Profiles
3.2. Auxiliary Analyses
3.2.1. Sex
7–9th Grade Profiles
10–12th Grade Profiles
3.2.2. Distal Outcomes: Mean Comparisons of Substance Use Changes between Profiles
Change in Alcohol Use
- 7–9th Grades
- 2.
- 10–12th Grades
Change in Cannabis Use (Smoking)
- 7–9th Grade
- 2.
- 10–12th Grades
Change in Cannabis Use (Edibles)
- 7–9th Grades
- 2.
- 10–12th Grades
4. Discussion
4.1. Ecosystemic Resilience Profiles
4.2. Inter-Profile Changes in Cannabis and Alcohol Use following the Onset of COVID-19
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Internal Vulnerabilities | Cronbach’s Alpha | Scale |
|---|---|---|
| COVID-19 Health Anxiety: How worried are you about… | 0.915 | 1 = Not worried 2 = A little worried 3 = Worried 4 = Very worried |
| …getting COVID-19? | ||
| …long-term health problems if you get COVID-19? | ||
| …a family member getting COVID-19? | ||
| …dying from COVID-19? | ||
| …a family member dying from COVID-19? | ||
| …giving someone else COVID-19? | ||
| Change in Negative Affect: Compared to before COVID-19, are you… | 0.923 | 1 = Much less 2 = Less 3 = About the same 4 = More 5 = Much more |
| ...more or less sad now? | ||
| ...more or less lonely now? | ||
| ...more or less bored now? | ||
| ...more or less depressed now? | ||
| ...more or less angry now? | ||
| ...more or less worried now? | ||
| ...more or less anxious now? | ||
| ...having more or less trouble sleeping now? | ||
| ...more or less interested in normal activities? | ||
| ...having more or less trouble concentrating? | ||
| COVID-19-Specific Maladaptive Coping: How often have you done each of the following to deal with your stress related to COVID-19? | 0.811 | 1 = Never 2 = Not very often 3 = Sometimes 4 = Often 5 = Very often |
| Drinking alcohol | ||
| Using tobacco (smoking, chewing or vaping) | ||
| Using marijuana (smoking, edibles, vaping) | ||
| Using other illegal drugs | ||
| Internal Assets | ||
| COVID-19-Specific Prosocial Coping:How often have you done each of the following to deal with your stress related to COVID-19? | 0.623 | 1 = Never 2 = Not very often 3 = Sometimes 4 = Often 5 = Very often |
| Meditation/Mindfulness practices/Prayer | ||
| Exercising | ||
| Joining in family activities like games or sport | ||
| Talking to someone about my stress (parents, school counselors, or doctors) | ||
| Volunteer work in my community | ||
| COVID-19-Specific Distracted Coping: How often have you done each of the following to deal with your stress related to COVID-19? | 0.627 | 1 = Never 2 = Not very often 3 = Sometimes 4 = Often 5 = Very often |
| Talking with friends virtually | ||
| Using social media | ||
| Watching TV/Playing video games | ||
| COVID-19-Specific School Engagement: Please rate how true each statement below is for you: | 0.761 | 1 = Not at all true 2 = A little true 3 = True 4 = Very true |
| I attend school more (either remotely or in person) than before COVID-19. | ||
| I am getting better grades now than before COVID-19. | ||
| I am enjoying school more now than before COVID-19. | ||
| Ethnic Identity Connection: For each statement below, say how close it is to your opinion using the following scale: | 0.776 | 1 = Strongly disagree 2 = Disagree 3 = Neither agree nor disagree 4 = Agree 5 = Strongly agree |
| It is important to me to think of myself as American Indian | ||
| I feel that I am part of the American Indian community. | ||
| I feel close to others in the American Indian community. | ||
| I have a lot of pride in what members of the American Indian community have achieved. | ||
| Ethnic Identity Achievement: For each statement below, say how close it is to your opinion using the following scale: | 0.798 | 1 = Strongly disagree 2 = Disagree 3 = Neither agree nor disagree 4 = Agree 5 = Strongly agree |
| It helps me when others in the American Indian community are successful. | ||
| It is important for my family and the American Indian community that I succeed in school. | ||
| If I work hard and get good grades, other American Indian people will respect me. | ||
| If I am successful, it will help the American Indian community. | ||
| Awareness of Racism: For each statement below, say how close it is to your opinion using the following scale: | 0.713 | 1 = Strongly disagree 2 = Disagree 3 = Neither agree nor disagree 4 = Agree 5 = Strongly agree |
| As an American Indian, the way I look and speak influences what others expect of me. | ||
| Some people will treat me differently because I am American Indian. | ||
| People might have negative ideas about my abilities because I am American Indian. | ||
| Things in the American Indian community are not as good as they could be because of lack of opportunity. | ||
| Trait Resilience: Please rate how much you agree with the following statements as they apply to you over the past month. | 0.887 | 0 = Not at all true 1 = Rarely true 2 = Sometimes true 3 = Often true 4 = True nearly all of the time |
| I am able to adapt when changes occur. | ||
| Under pressure, I stay focused and think clearly. | ||
| I am not easily discouraged by failure. | ||
| I try to see the humorous side of things when I am faced with problems. | ||
| I tend to bounce back after illness, injury or other hardships. | ||
| I think of myself as a strong person when dealing with life’s challenges and difficulties. | ||
| I can deal with whatever comes my way. | ||
| Having to cope with stress can make me stronger. | ||
| I believe I can achieve my goals, even if there are obstacles. | ||
| I am able to handle unpleasant or painful feelings like sadness, fear, and anger. | ||
| I am able to adapt when changes occur. | ||
| Under pressure, I stay focused and think clearly. | ||
| I am not easily discouraged by failure. | ||
| External Adversity | ||
| Stressful Life Events: In the past 12 months, did any of the following events happen to you? | NA | 0 = No 1 = Yes |
| Entered school as a new or transfer student. | ||
| Had a parent or guardian be unable to find employment. | ||
| Found out people are gossiping about you. | ||
| Had a friend attempt suicide. | ||
| Had a serious argument with a friend. | ||
| Broke up with a boyfriend/girlfriend or significant other. | ||
| Was in a serious car wreck. | ||
| Entered school as a new or transfer student. | ||
| COVID-19-Specific School Challenges: Please rate how true each statement below is for you: | 0.826 | 1 = Not at all true 2 = A little true 3 = True 4 = Very true |
| It is harder for me to focus on my schoolwork. | ||
| I am falling behind in my schoolwork more. | ||
| I am more worried about school. | ||
| External Resources | ||
| COVID-19-Specific Family Closeness: Please rate how true each statement below is for you: | 0.706 | 1 = Not at all true 2 = A little true 3 = True 4 = Very true |
| I spend more time with my family. | ||
| My family is closer. | ||
| My parents/guardians supervise my activities more. | ||
| COVID-19-Specific Peer Closeness: Please rate how true each statement below is for you: | 0.573 a | 1 = Not at all true 2 = A little true 3 = True 4 = Very true |
| I see my friends more in person since COVID-19 began. | ||
| I feel closer to my friends since COVID-19 began. | ||
| Distal Outcomes | ||
| After COVID-19 started, how much did your use of alcohol change? | NA | −2 = Decreased a lot −1 = Decreased a little 0 = No change 1 = Increased a little 2 = Increased a lot |
| After COVID-19 started, how much did your smoking of marijuana change? | NA | |
| After COVID-19 started, how much did your use of marijuana edibles change? | NA |
References
- Jones, E.; Mitra, A.; Bhuiyan, A. Impact of COVID-19 on Mental Health in Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 2470. [Google Scholar] [CrossRef]
- Richter, L. The Effects of the COVID-19 Pandemic on the Risk of Youth Substance Use. J. Adolesc. Health 2020, 67, 467–468. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Swaim, R.C.; Stanley, L.R.; Meich, R.A.; Patrick, M.E.; Crabtree, M.A.; Prince, M.A. A Comparison of COVID-19 outcomes between reservation-based American Indian and U.S. national students. Am. J. Prev. Med. Focus 2022. under review. [Google Scholar]
- Bear, C.R.; Terrill, W.P.A.; Frates, A.; Peterson, P.; Ulrich, J. Challenges for Rural Native American Students with Disabilities during COVID-19. Rural Speéc. Educ. Q. 2021, 40, 60–69. [Google Scholar] [CrossRef]
- Swaim, R.C.; Stanley, L.R. Substance Use Among American Indian Youths on Reservations Compared with a National Sample of US Adolescents. JAMA Netw. Open 2018, 1, e180382. [Google Scholar] [CrossRef]
- Fergus, S.; Zimmerman, M.A. Adolescent Resilience: A Framework for Understanding Healthy Development in the Face of Risk. Annu. Rev. Public Health 2005, 26, 399–419. [Google Scholar] [CrossRef] [PubMed]
- Waller, M.A. Resilience in ecosystemic context: Evolution of the concept. Am. J. Orthopsychiatry 2001, 71, 290–297. [Google Scholar] [CrossRef]
- Raifman, M.A.; Raifman, J.R. Disparities in the Population at Risk of Severe Illness From COVID-19 by Race/Ethnicity and Income. Am. J. Prev. Med. 2020, 59, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Gawthrop, E. The Color of Coronavirus: COVID-19 Deaths by Race and Ethnicity in the U.S. Available online: https://www.ywboston.org/wp-content/uploads/2021/07/Color-of-Coronavirus_-COVID-19-deaths-a...-race-and-ethnicity-%E2%80%94-APM-Research-Lab.pdf (accessed on 28 July 2022).
- Burki, T. COVID-19 among American Indians and Alaska Natives. Lancet Infect. Dis. 2021, 21, 325–326. [Google Scholar] [CrossRef]
- Wang, H. Why the Navajo Nation was hit so hard by coronavirus: Understanding the disproportionate impact of the COVID-19 pandemic. Appl. Geogr. 2021, 134, 102526. [Google Scholar] [CrossRef]
- Hathaway, E.D. American Indian and Alaska Native People: Social Vulnerability and COVID-19. J. Rural Health 2020, 37, 256–259. [Google Scholar] [CrossRef]
- Household Experiences in America during the Delta Variant Outbreak by Race/Ethnicity 2021. Available online: https://www.rwjf.org/en/library/research/2021/10/household-experiences-in-america-during-the-delta-variant-outbreak.html (accessed on 30 June 2022).
- Maudrie, T.L.; Lessard, K.H.; Dickerson, J.; Aulandez, K.M.W.; Barlow, A.; O’Keefe, V.M. Our Collective Needs and Strengths: Urban AI/ANs and the COVID-19 Pandemic. Front. Sociol. 2021, 6, 611775. [Google Scholar] [CrossRef]
- LaFromboise, T.D.; Hoyt, D.; Oliver, L.; Whitbeck, L.B. Family, community, and school influences on resilience among American Indian adolescents in the upper midwest. J. Community Psychol. 2006, 34, 193–209. [Google Scholar] [CrossRef]
- Doshi, S.; Jordan, A.; Kelly, K.; Solomon, D. The COVID-19 Response in Indian Country: A Federal Failure. 2020. Available online: https://www.americanprogress.org/article/covid-19-response-indian-country/ (accessed on 28 July 2022).
- Powder, J. Keys to the Navajo Nation’s COVID-19 Vaccination Success. Available online: https://publichealth.jhu.edu/2021/keys-to-the-navajo-nations-covid-19-vaccination-success (accessed on 28 July 2022).
- Scott, S.R.; Rivera, K.M.; Rushing, E.; Manczak, E.M.; Rozek, C.S.; Doom, J.R. “I Hate This”: A Qualitative Analysis of Adolescents’ Self-Reported Challenges During the COVID-19 Pandemic. J. Adolesc. Health 2020, 68, 262–269. [Google Scholar] [CrossRef]
- Hawke, L.D.; Barbic, S.P.; Voineskos, A.; Szatmari, P.; Cleverley, K.; Hayes, E.; Relihan, J.; Daley, M.; Courtney, D.; Cheung, A.; et al. Impacts of COVID-19 on youth mental health, substance use, and well-being: A rapid survey of clinical and community samples. Can. J. Psychiatry 2020, 65, 701–709. [Google Scholar] [CrossRef]
- Magson, N.R.; Freeman, J.Y.A.; Rapee, R.M.; Richardson, C.E.; Oar, E.L.; Fardouly, J. Risk and Protective Factors for Prospective Changes in Adolescent Mental Health during the COVID-19 Pandemic. J. Youth Adolesc. 2020, 50, 44–57. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.J.; Palimaru, A.I.; Dickerson, D.L.; Dong, L.; Brown, R.A.; Johnson, C.L.; Klein, D.J.; Troxel, W.M. Risk and resilience factors in Urban American Indian and Alaska Native youth during the coronavirus pandemic. Am. Indian Cult. Res. J. 2020, 44, 21–48. [Google Scholar] [CrossRef] [PubMed]
- Stanley, L.R.; Swaim, R.C.; Smith, J.K.; Conner, B.T. Early onset of cannabis use and alcohol intoxication predicts prescription drug misuse in American Indian and non-American Indian adolescents living on or near reservations. Am. J. Drug Alcohol Abus. 2020, 46, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Stanley, L.R.; Harness, S.D.; Swaim, R.C.; Beauvais, F. Rates of Substance Use of American Indian Students in 8th, 10th, and 12th Grades Living on or near Reservations: Update, 2009–2012. Public Health Rep. 2014, 129, 156–163. [Google Scholar] [CrossRef]
- Ungar, M.; Theron, L.; Murphy, K.; Jefferies, P. Researching Multisystemic Resilience: A Sample Methodology. Front. Psychol. 2021, 11, 3808. [Google Scholar] [CrossRef] [PubMed]
- Beebe, L.A.; Vesely, S.K.; Oman, R.F.; Tolma, E.; Aspy, C.B.; Rodine, S. Protective Assets for Non-use of Alcohol, Tobacco and Other Drugs among Urban American Indian Youth in Oklahoma. Matern. Child Health J. 2008, 12, 82–90. [Google Scholar] [CrossRef]
- Henson, M.; Sabo, S.; Trujillo, A.; Teufel-Shone, N. Identifying Protective Factors to Promote Health in American Indian and Alaska Native Adolescents: A Literature Review. J. Prim. Prev. 2016, 38, 5–26. [Google Scholar] [CrossRef]
- Ungar, M.; Jefferies, P. Becoming More Rugged and Better Resourced: The R2 Resilience Program’s© Psychosocial Approach to Thriving. Front. Psychol. 2021, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ungar, M. Systemic resilience: Principles and processes for a science of change in contexts of adversity. Ecol. Soc. 2018, 23, 34. [Google Scholar] [CrossRef]
- Ungar, M. Resilience across Cultures. Br. J. Soc. Work 2006, 38, 218–235. [Google Scholar] [CrossRef]
- Stiffman, A.R.; Brown, E.; Freedenthal, S.; House, L.; Ostmann, E.; Yu, M.S. American Indian Youth: Personal, Familial, and Environmental Strengths. J. Child Fam. Stud. 2007, 16, 331–346. [Google Scholar] [CrossRef]
- Braverman, M.T. Applying resilience theory to the prevention of adolescent substance abuse Author. Cent. Youth Dev. FOCUS 2001, 7, 1–12. [Google Scholar]
- Liang, L.; Ren, H.; Cao, R.; Hu, Y.; Qin, Z.; Li, C.; Mei, S. The Effect of COVID-19 on Youth Mental Health. Psychiatr. Q. 2020, 91, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Dumas, T.M.; Ellis, W.; Litt, D.M. What Does Adolescent Substance Use Look Like during the COVID-19 Pandemic? Examining Changes in Frequency, Social Contexts, and Pandemic-Related Predictors. J. Adolesc. Health 2020, 67, 354–361. [Google Scholar] [CrossRef]
- Acuff, S.F.; Tucker, J.A.; Murphy, J.G. Behavioral economics of substance use: Understanding and reducing harmful use during the COVID-19 pandemic. Exp. Clin. Psychopharmacol. 2021, 29, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Ellis, W.E.; Dumas, T.M.; Forbes, L.M. Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can. J. Behav. Sci. Rev. Can. Sci. Comport. 2020, 52, 177–187. [Google Scholar] [CrossRef]
- Howard, M.C.; Hoffman, M.E. Variable-Centered, Person-Centered, and Person-Specific Approaches. Organ. Res. Methods 2017, 21, 846–876. [Google Scholar] [CrossRef]
- Neblett, E.W.; Sosoo, E.E.; Willis, H.A.; Bernard, D.L.; Bae, J.; Billingsley, J.T. Racism, Racial Resilience, and African American Youth Development. Adv. Child Dev. Behav. 2016, 51, 43–79. [Google Scholar] [CrossRef]
- Prince, M.A.; Fidler, D.J. Analytic approaches to heterogeneity in neurogenetic syndrome research. Int. Rev. Res. Dev. Disabil. 2021, 60, 55–73. [Google Scholar] [CrossRef]
- Ferguson, S.L.; Moore, E.W.G.; Hull, D.M. Finding latent groups in observed data: A primer on latent profile analysis in Mplus for applied researchers. Int. J. Behav. Dev. 2019, 44, 458–468. [Google Scholar] [CrossRef]
- Ladouceur, C.D. COVID-19 Adolescent Symptom & Psychological Experience Questionnaire (CASPE) 2020. Available online: https://www.phenxtoolkit.org/toolkit_content/PDF/CASPE_Adolescent.pdf (accessed on 30 June 2022).
- The Coronavirus Health Impact Survey (CRISIS) V0.3, Youth Self-Report Baseline Form: Current Form 2020. Available online: https://www.phenxtoolkit.org/toolkit_content/PDF/CRISIS_Baseline_Youth.pdf (accessed on 30 June 2022).
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the connor–davidson resilience scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef]
- Goins, R.T.; Gregg, J.J.; Fiske, A. Psychometric Properties of the Connor-Davidson Resilience Scale with Older American Indians. Res. Aging 2012, 35, 123–143. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, I.E.; Seedat, S. Factor structure of the Connor-Davidson Resilience Scale in South African adolescents. Int. J. Adolesc. Med. Health 2008, 20, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Oyserman, D.; Brickman, D.; Rhodes, M. Racial-Ethnic Identity: Content and consequences for African American, Latino, and Latina youths. In Contesting Stereotypes and Creating Identities: Social Categories, Social Identities, and Educational Participation; Fuligni, A., Ed.; Russel Sage Foundation: New York, NY, USA, 2007. [Google Scholar]
- Baldwin, J.A.; Brown, B.G.; Wayment, H.; Nez, R.A.; Brelsford, K. Culture and Context: Buffering the Relationship between Stressful Life Events and Risky Behaviors in American Indian Youth. Subst. Use Misuse 2011, 46, 1380–1394. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.W.; Taylor, B.J.; Olchowski, A.E.; Cumsille, P.E. Planned missing data designs in psychological research. Psychol. Methods 2006, 11, 323–343. [Google Scholar] [CrossRef] [PubMed]
- Enders, C.K. (Ed.) Applied Missing Data Analysis; The Guilford Press: New York, NY, USA, 2022. [Google Scholar]
- Muthén, L.K. Mplus User’s Guide, 8th ed.; Muthen, L.K., Muthen, B.O., Eds.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Enders, C.K.; Bandalos, D.L. The Relative Performance of Full Information Maximum Likelihood Estimation for Missing Data in Structural Equation Models. Struct. Equ. Model. 2001, 8, 430–457. [Google Scholar] [CrossRef]
- Croux, C.; Dhaene, G.; Hoorelbeke, D. Robust standard errors for robust estimators. CES-Discuss. Pap. Ser. 2004, 3, 1–20. [Google Scholar]
- Tein, J.-Y.; Coxe, S.; Cham, H. Statistical Power to Detect the Correct Number of Classes in Latent Profile Analysis. Struct. Equ. Model. A Multidiscip. J. 2013, 20, 640–657. [Google Scholar] [CrossRef] [PubMed]
- Eid, M.; Langeheine, R.; Diener, E. Comparing Typological Structures Across Cultures By Multigroup Latent Class Analysis. J. Cross-Cultural Psychol. 2003, 34, 195–210. [Google Scholar] [CrossRef]
- Asparouhov, T.; Muthén, B. Auxiliary Variables in Mixture Modeling: Three-Step Approaches Using Mplus. Struct. Equ. Model. Multidiscip. J. 2014, 21, 329–341. [Google Scholar] [CrossRef]
- Satorra, A.; Bentler, P.M. Ensuring Positiveness of the Scaled Difference Chi-square Test Statistic. Psychometrika 2010, 75, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Miller-Graff, L.E. The Multidimensional Taxonomy of Individual Resilience. Trauma Violence Abus. 2020, 23, 660–675. [Google Scholar] [CrossRef]
- Malhi, G.S.; Das, P.; Bell, E.; Mattingly, G.; Mannie, Z. Modelling resilience in adolescence and adversity: A novel framework to inform research and practice. Transl. Psychiatry 2019, 9, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Bonanno, G.A. Psychological adjustment during the global outbreak of COVID-19: A resilience perspective. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S51–S54. [Google Scholar] [CrossRef]
- PeConga, E.K.; Gauthier, G.M.; Holloway, A.; Walker, R.S.W.; Rosencrans, P.L.; Zoellner, L.A.; Bedard-Gilligan, M. Resilience is spreading: Mental health within the COVID-19 pandemic. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S47–S48. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Mancini, A.D. Beyond resilience and PTSD: Mapping the heterogeneity of responses to potential trauma. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 74–83. [Google Scholar] [CrossRef]
- Galatzer-Levy, I.R.; Huang, S.H.; Bonanno, G.A. Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clin. Psychol. Rev. 2018, 63, 41–55. [Google Scholar] [CrossRef]
- Tingey, L.; Cwik, M.F.; Rosenstock, S.; Goklish, N.; Larzelere-Hinton, F.; Lee, A.; Suttle, R.; Alchesay, M.; Massey, K.; Barlow, A. Risk and protective factors for heavy binge alcohol use among American Indian adolescents utilizing emergency health services. Am. J. Drug Alcohol Abus. 2016, 42, 715–725. [Google Scholar] [CrossRef] [PubMed]
- McKinley, C.E.; Lilly, J. “It’s in the family circle”: Communication promoting Indigenous family resilience. Fam. Relat. 2021, 71, 108–129. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Yurkovich, E. “Close-Knit” Defines a Healthy Native American Indian Family. J. Fam. Nurs. 2013, 20, 51–72. [Google Scholar] [CrossRef]
- Tajfel, H.; Turner, J.C. An Integrative Theory of Intergroup Conflict. In The Social Psychology of Intergroup Relations; Austin, W.G., Worchel, S., Eds.; Brooks/Cole: Monterey, CA, USA, 1979; pp. 33–37. [Google Scholar]
- Brewer, M.B.; Gardner, W. Who is this "We"? Levels of collective identity and self representations. J. Pers. Soc. Psychol. 1996, 71, 83–93. [Google Scholar] [CrossRef]
- Hogg, M.A. Social Identity and Social Comparison. In Handbook of Social Comparison; Springer: Boston, MA, USA, 2000; pp. 401–421. [Google Scholar] [CrossRef]
- Altschul, I.; Oyserman, D.; Bybee, D. Racial-Ethnic Identity in Mid-Adolescence: Content and Change as Predictors of Academic Achievement. Child Dev. 2006, 77, 1155–1169. [Google Scholar] [CrossRef] [PubMed]
- Crocker, J.; Major, B. Social stigma and self-esteem: The self-protective properties of stigma. Psychol. Rev. 1989, 96, 608–630. [Google Scholar] [CrossRef]
- Smokowski, P.R.; Evans, C.B.R.; Cotter, K.L.; Webber, K.C. Ethnic Identity and Mental Health in American Indian Youth: Examining Mediation Pathways Through Self-esteem, and Future Optimism. J. Youth Adolesc. 2013, 43, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Tyser, J.; Scott, W.D.; Readdy, T.; McCrea, S.M. The Role of Goal Representations, Cultural Identity, and Dispositional Optimism in the Depressive Experiences of American Indian Youth from a Northern Plains Tribe. J. Youth Adolesc. 2013, 43, 329–342. [Google Scholar] [CrossRef]
- Brown, R.A.; Dickerson, D.L.; D’Amico, E.J. Cultural Identity Among Urban American Indian/Alaska Native Youth: Implications for Alcohol and Drug Use. Prev. Sci. 2016, 17, 852–861. [Google Scholar] [CrossRef] [Green Version]
- Kulis, S.; Napoli, M.; Marsiglia, F.F. Ethnic pride, biculturalism, and drug use norms of urban American Indian adolescents. Soc. Work Res. 2002, 26, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Vinayak, S.; Judge, J. Resilience and empathy as predictors of psychological wellbeing among adolescents. Int. J. Health Sci. Res. 2018, 8, 192–200. [Google Scholar]
- Whitesell, N.R.; Mitchell, C.M.; Kaufman, C.E.; Spicer, P.; The Voices of Indian Teens Project Team. Developmental Trajectories of Personal and Collective Self-Concept among American Indian Adolescents. Child Dev. 2006, 77, 1487–1503. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.J.; Sundberg, M.A.; Dionne, J.; Kosobuski, A.W. The Impact of COVID-19 on American Indian and Alaska Native Communities: A Call for Better Relational Models. Am. J. Public Health 2021, 111, 801–803. [Google Scholar] [CrossRef]
- Heart, M.Y.H.B.; Debruyn, L.M. The American Indian Holocaust: Healing historical unresolved grief. Am. Indian Alsk. Nativ. Ment. Health Res. 1998, 8, 56–78. [Google Scholar]
- Evans, W.; Davis, B. Exploring the Relationship between Sense of Coherence and Historical Trauma among American Indian Youth. Am. Indian Alsk. Nativ. Ment. Health Res. 2018, 25, 38–50. [Google Scholar] [CrossRef]
- Whitesell, N.R.; Voices of Indian Teens Project Team; Mitchell, C.M.; Spicer, P. A longitudinal study of self-esteem, cultural identity, and academic success among American Indian adolescents. Cult. Divers. Ethn. Minor. Psychol. 2009, 15, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Galliher, R.V.; Jones, M.D.; Dahl, A. Concurrent and longitudinal effects of ethnic identity and experiences of discrimination on psychosocial adjustment of Navajo adolescents. Dev. Psychol. 2011, 47, 509–526. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.L. Resilience among American Indian Youth: First Nation’s Youth Resilience Study; University of Minnesota: Minneapolis, MN, USA, 2001. [Google Scholar]
- Sayers, J.F.; MacDonald, K.A.; Fiske, J.-A.; Newell, M.; George, E.; Cornet, W. First Nations Women, Governance and the Indian Act: A Collection of Policy Research Reports; Status of Women Canada: Ottawa, ON, Canada, 2001. [Google Scholar]
- Heart, M.Y.H.B.; Elkins, J.; Tafoya, G.; Bird, D.; Salvador, M. Wicasa Was’aka: Restoring the Traditional Strength of American Indian Boys and Men. Am. J. Public Health 2012, 102, S177–S183. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Godfrey, J.; Moccasin, B. American Indian Fathering in the Dakota Nation: Use of Akicita as a Fatherhood Standard. Father. J. Theory Res. Pract. Men Father. 2006, 4, 49–69. [Google Scholar] [CrossRef]
- Ostaszewski, K.; Zimmerman, M.A. The Effects of Cumulative Risks and Promotive Factors on Urban Adolescent Alcohol and Other Drug Use: A Longitudinal Study of Resiliency. Am. J. Community Psychol. 2006, 38, 251–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ungar, M. A Constructionst Discourse on resilience: Multiple contexts, multiple realities among at-risk children and youth. Youth Soc. 2004, 35, 341–365. [Google Scholar] [CrossRef]
- Miech, R.; Patrick, M.E.; Keyes, K.; O’Malley, P.M.; Johnston, L. Adolescent drug use before and during U.S. national COVID-19 social distancing policies. Drug Alcohol Depend. 2021, 226, 108822. [Google Scholar] [CrossRef] [PubMed]

| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. COVID-19 Health Anxiety | - | ||||||||||||||||
| 2. COVID-19 Change in Negative Affect | −0.019 | - | |||||||||||||||
| 3. Maladaptive Coping | −0.092 | 0.197 | - | ||||||||||||||
| 4. Prosocial Coping | 0.259 | −0.090 | 0.084 | - | |||||||||||||
| 5. Distracted Coping | 0.197 | 0.055 | 0.027 | 0.411 | - | ||||||||||||
| 6. School Engagement | 0.213 | −0.155 | 0.052 | 0.230 | 0.169 | - | |||||||||||
| 7. Ethnic Identity Connection | 0.244 | −0.025 | −0.004 | 0.265 | 0.192 | 0.142 | - | ||||||||||
| 8. Ethnic Identity Achievement | 0.265 | −0.031 | −0.002 | 0.285 | 0.177 | 0.151 | 0.775 | - | |||||||||
| 9. Awareness of Racism | 0.195 | 0.064 | 0.042 | 0.187 | 0.117 | 0.120 | 0.611 | 0.677 | - | ||||||||
| 10. Trait Resilience | 0.073 | −0.128 | -0.018 | 0.348 | 0.189 | 0.142 | 0.287 | 0.287 | 0.206 | - | |||||||
| 11. Stressful Life Events | 0.033 | 0.258 | 0.283 | 0.094 | 0.118 | 0.045 | 0.071 | 0.088 | 0.164 | 0.005 | - | ||||||
| 12. School Difficulty | 0.216 | 0.223 | 0.105 | 0.065 | 0.189 | 0.032 | 0.142 | 0.150 | 0.166 | 0.007 | 0.146 | - | |||||
| 13. Family Closeness | 0.303 | −0.087 | −0.042 | 0.344 | 0.225 | 0.306 | 0.201 | 0.212 | 0.141 | 0.186 | −0.013 | 0.142 | - | ||||
| 14. Peer Closeness | −0.052 | −0.228 | 0.081 | 0.068 | 0.020 | 0.146 | 0.065 | 0.064 | 0.016 | 0.059 | 0.024 | −0.132 | 0.007 | - | |||
| 15. Change in Alcohol Use | −0.027 | 0.031 | 0.153 | 0.002 | 0.011 | −0.032 | 0.014 | 0.020 | 0.005 | 0.000 | 0.067 | 0.018 | 0.006 | 0.036 | - | ||
| 16. Change in Cannabis Use (Smoking) | −0.053 | 0.043 | 0.251 | −0.015 | 0.005 | 0.003 | −0.013 | −0.007 | −0.028 | 0.021 | 0.053 | 0.010 | −0.045 | 0.017 | 0.247 | - | |
| 17. Change in Cannabis Use (Edibles) | −0.031 | 0.002 | 0.056 | −0.004 | 0.019 | −0.004 | −0.010 | −0.013 | −0.024 | 0.048 | −0.013 | 0.020 | 0.017 | 0.030 | 0.247 | 0.593 | - |
| Grade Group | 7–9th | ||||||
|---|---|---|---|---|---|---|---|
| # of Profiles | Converge Without Errors | -LL | CF | SABIC | Entropy | Smallest Profile % | Class Assignment Probability |
| 1 | Yes | −20,097.845 | 2.019 | 40,303.889 | - | - | - |
| 2 | Yes | −19,560.895 | 2.04 | 39,287.852 | 0.686 | 35% | 0.873/0.921 |
| 3 | Yes | −19,138.897 | 1.81 | 38,501.919 | 0.801 | 7% | 0.854/0.987/0.920 |
| 4 | Yes | −18,861.622 | 1.65 | 38,005.334 | 0.796 | 7% | 0.911/0.869/0.873/0.965 |
| 5 | Yes | −18,757.901 | 1.83 | 37,855.855 | 0.766 | 7% | 0.928/0.814/0.798/0.862/0.960 |
| Grade Group | 10–12th | ||||||
| # of Profiles | Converge Without Errors | -LL | CF | SABIC | Entropy | Smallest Profile % | |
| 1 | Yes | −15,582.783 | 2.77 | 31,265.840 | - | - | - |
| 2 | Yes | −15,082.770 | 2.18 | 30,319.532 | 0.751 | 34% | 0.900/0.937 |
| 3 | Yes | −14,753.500 | 1.84 | 29,714.718 | 0.816 | 6% | 0.938/0.905/0.911 |
| 4 | Yes | −14,628.352 | 1.74 | 29,518.131 | 0.823 | 6% | 0.934/0.901/0.894/0.889 |
| 5 | Yes | −14,528.806 | 1.59 | 29,372.758 | 0.847 | 2% | 0.886/0.923/0.909/0.903/0.910 |
| 7–9th n = 1142 | 10–12th, n = 860 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ecosystemic Profiles | Average Risk and Resilience n = 588 (a) | High Resilience n = 394 (b) | Low Resilience n = 81 (c) | High Risk n = 77 (d) | Total | Average Risk and Resilience n = 379 (a) | High Resilience n = 330 (b) | Low Resilience n = 52 (c) | High Risk n = 99 (d) | Total | |
| Categorical Descriptives i | f (%) | f (%) | f (%) | f (%) | f (%) | f (%) | f (%) | f (%) | f (%) | f (%) | |
| Male | 281 (47.79) | 188 (47.72) | 58 (71.60) | 29 (37.66) | 556 (48.69) | 195 (51.45) | 121 (36.67) | 37 (71.15) | 43 (43.43) | 396 (46.05) | |
| Female | 307 (52.21) | 206 (52.28) | 23 (28.40) | 48 (62.34) | 584 (51.23) | 184 (48.55) | 209 (63.33) | 15 (28.85) | 56 (56.57) | 464 (53.95) | |
| Continuous Descriptives | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |
| Age | 13.78 (1.14) | 13.88 (0.97) | 13.98 (1.16) | 13.78 (1.02) | 13.83 (1.08) | 16.61 (0.96) | 16.65 (0.99) | 16.54 (1.39) | 16.74 (0.90) | 16.63 (1.0) | |
| Grade | 8.06 (0.85) | 8.09 (0.82) | 8.11 (0.86) | 8.05 (0.78) | 8.08 (0.83) | 10.87 (0.82) | 10.98 (0.82) | 10.77 (0.78) | 10.97 (0.76) | 10.91 (0.82) | |
| Internal Vulnerability | |||||||||||
| COVID-19 Health Anxiety | 2.55 (0.94) b,c | 3.26 (0.83) a,c,d | 2.18 (1.15) a,b,d | 2.56 (0.98) b,c | 2.78 (1.0) | 2.35 (0.95) b,c | 3.11 (0.86) a,c,d | 2.0 (1.10) a,b,d | 2.35 (0.98) b,c | 2.61 (1.01) | |
| Change in Negative Affect | 3.17 (0.89) d | 3.02 (0.93) d | 3.06 (1.19) d | 3.66 (0.98) a,b,c | 3.15 (0.95) | 3.04 (0.85) d | 3.25 (0.95) | 3.39 (1.23) | 3.42 (0.90) a | 3.19 (0.93) | |
| COVID-19-SpecificMaladaptive Coping | 1.11 (0.27) d | 1.07 (0.21) d | 1.17 (0.39) d | 3.08 (0.70) a,b,c | 1.24 (0.60) | 1.27 (0.47) c,d | 1.22 (0.39) c,d | 1.62 (1.01) a,b,d | 3.18 (0.76) a,b,c | 1.51 (0.83) | |
| Internal Assets | |||||||||||
| COVID-19-Specific Prosocial Coping | 2.11 (0.83) b,d | 2.79 (0.77) a,c | 1.92 (0.86) b,d | 2.56 (1.01) a,c | 2.36 (0.82) | 2.30 (0.71) b,c,d | 2.78 (0.82) a,c | 1.74 (0.90) a,b,d | 2.61 (0.85) a,c | 2.48 (0.83) | |
| COVID-19-Specific Distracted Coping | 3.29 (1.03) b,c | 3.78 (0.93) a,c | 2.67 (1.27) a,b,d | 3.50 (0.98) c | 3.43 (1.06) | 3.21 (1.01) b,c,d | 3.57 (0.96) a,c | 2.22 (1.16) a,b,d | 3.52 (0.94) a,c | 3.33 (1.04) | |
| COVID-19-Specific] School Engagement | 1.88 (0.82) b,c | 2.29 (0.94) a,c | 1.39 (0.61) a,b,d | 2.14 (0.93) c | 2.00 (0.89) | 1.80 (0.85) c | 1.98 (0.89) c | 1.49 (0.82) a,b,d | 2.14 (0.97) c | 1.89 (0.89) | |
| Ethnic Identity Connection | 3.43 (0.63) b,c,d | 4.49 (0.51) a,c,d | 1.60 (0.68) a,b,d | 3.85 (0.93) a,b,c | 3.70 (0.98) | 3.40 (0.61) b,c,d | 4.54 (0.49) a,c,d | 1.41 (0.51) a,b,d | 3.98 (0.75) a,b,c | 3.79 (0.97) | |
| Ethnic Identity Achievement | 3.25 (0.59) b,c,d | 4.38 (0.50) a,c,d | 1.47 (0.66) a,b,d | 3.57 (0.91) a,b,c | 3.55 (1.00) | 3.23 (0.56) b,c,d | 4.51 (0.49) a,c,d | 1.40 (0.47) a,b,d | 3.99 (0.68) a,b,c | 3.71 (1.0) | |
| Awareness of Racism | 3.05 (0.72) b,c,d | 3.98 (0.79) a,c | 1.46 (0.66) a,b,d | 3.69 (0.89) a,c | 3.32 (1.01) | 3.05 (0.70) b,c,d | 4.19 (0.73) a,c,d | 1.58 (0.72) a,b,d | 3.63 (0.81) a,b,c | 3.47 (1.01) | |
| Trait Resilience | 1.93 (0.86) b,c | 2.53 (0.84) a,c,d | 1.18 (1.19) a,b,d | 2.02 (1.12) b,c | 2.10 (0.97) | 2.41 (0.80) b,c | 2.62 (0.85) a,c | 1.34 (1.13) a,b,d | 2.35 (0.90) c | 2.43 (0.89) | |
| External Adversity | |||||||||||
| Stressful Life Events | 1.56 (1.50) d | 1.77 (1.69) d | 1.16 (1.69) d | 2.93 (1.92) a,b,c | 1.70 (1.65) | 1.22 (1.36) d | 1.66 (1.46) d | 1.42 (1.46) d | 3.11 (1.85) a,b,c | 1.62 (1.58) | |
| COVID-19-Specific School Challenges | 2.50 (1.04) c,d | 2.53 (1.03) c,d | 1.85 (0.98) a,b,d | 2.92 (1.01) a,b,c | 2.49 (1.05) | 2.26 (1.07) b,c,d | 2.77 (1.03) a,c | 1.95 (1.12) a,b,d | 2.85 (0.96) a,c | 2.50 (1.08) | |
| External Resources | |||||||||||
| COVID-19-Specific Family Closeness | 2.11 (0.83) b,c | 2.75 (0.89) a,c,d | 1.79 (0.92) a,b,d | 2.23 (0.89) b,c | 2.31 (0.92) | 1.94 (0.82) b,c | 2.43 (0.88) a,c,d | 1.52 (0.80) a,b,d | 2.18 (0.90) b,c | 2.13 (0.89) | |
| COVID-19-Specific Peer Closeness | 2.17 (0.82) b | 2.34 (0.87) a | 2.19 (0.76) | 2.29 (0.89) | 2.24 (0.92) | 2.32 (0.81) d | 2.30 (0.84) d | 2.26 (0.88) d | 2.68 (0.85) a,b,c | 2.35 (0.84) | |
| Distal Outcomes | |||||||||||
| Change in Alcohol Use | −0.09 (0.54) | −0.13 (0.53) | −0.09 (0.64) | 0.20 (1.17) | −0.08 (0.61) | −0.11 (0.65) | −0.08 (0.56) | −0.08 (0.76) | 0.37 (1.08) | −0.04 (0.70) | |
| Change in Cannabis Use: Smoking | −0.03 (0.49) | −0.12 (0.53) | 0.07 (0.56) | 0.41 (1.11) | −0.02 (0.58) | −0.37 (0.67) | −0.04 (0.71) | −0.06 (0.98) | 0.46 (1.23) | 0.02 (0.81) | |
| Change in Cannabis Use: Edibles | −0.07 (0.47) | −0.10 (0.46) | 0.01 (0.32) | 0.22 (0.96) | −0.06 (0.52) | −0.07 (0.55) | −0.12 (0.56) | −0.25 (0.83) | −0.06 (0.78) | −0.10 (0.61) | |
| 7–9th Grade | Average Risk and Resilience (a) | High Resilience (b) | Low Resilience (c) | High Risk (d) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Distal Outcome | χ2 | p | M | S.E. | M | S.E. | M | S.E. | M | S.E. |
| Change in Alcohol Use | 4.34 | 0.228 | −0.089 | 0.027 | −0.129 | 0.036 | −0.087 | 0.066 | 0.197 | 0.137 |
| Change in Cannabis Use (Smoking) | 20.21 | <0.001 | −0.031 d | 0.029 | −0.118 c,d | 0.031 | 0.070 b,d | 0.048 | 0.405 a,b,c | 0.150 |
| Change in Cannabis Use (Edibles) | 16.84 | 0.001 | −0.074 d | 0.027 | −0.103 d | 0.029 | 0.006 | 0.080 | 0.217 a,b | 0.097 |
| 10–12th Grade | Average Risk and Resilience (a) | High Resilience (b) | Low Resilience (c) | High Risk (d) | ||||||
| Distal Outcome | χ2 | p | M | S.E. | M | S.E. | M | S.E. | M | S.E. |
| Change in Alcohol Use | 34.45 | <0.001 | −0.112 d | 0.017 | −0.078 d | 0.019 | −0.076 d | 0.074 | 0.374 a,b,c | 0.101 |
| Change in Cannabis Use (Smoking) | 125.33 | <0.001 | −0.050 d | 0.036 | −0.049 d | 0.071 | −0.060 d | 0.147 | 0.528 a,b,c | 0.066 |
| Change in Cannabis Use (Edibles) | 3.63 | 0.304 | −0.066 | 0.044 | −0.124 | 0.044 | −0.066 | 0.044 | −0.055 | 0.078 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crabtree, M.A.; Stanley, L.R.; Swaim, R.C.; Prince, M.A. Profiles of Ecosystemic Resilience and Risk: American Indian Adolescent Substance Use during the First Year of the COVID-19 Crisis. Int. J. Environ. Res. Public Health 2022, 19, 11228. https://doi.org/10.3390/ijerph191811228
Crabtree MA, Stanley LR, Swaim RC, Prince MA. Profiles of Ecosystemic Resilience and Risk: American Indian Adolescent Substance Use during the First Year of the COVID-19 Crisis. International Journal of Environmental Research and Public Health. 2022; 19(18):11228. https://doi.org/10.3390/ijerph191811228
Chicago/Turabian StyleCrabtree, Meghan A., Linda R. Stanley, Randall C. Swaim, and Mark A. Prince. 2022. "Profiles of Ecosystemic Resilience and Risk: American Indian Adolescent Substance Use during the First Year of the COVID-19 Crisis" International Journal of Environmental Research and Public Health 19, no. 18: 11228. https://doi.org/10.3390/ijerph191811228
APA StyleCrabtree, M. A., Stanley, L. R., Swaim, R. C., & Prince, M. A. (2022). Profiles of Ecosystemic Resilience and Risk: American Indian Adolescent Substance Use during the First Year of the COVID-19 Crisis. International Journal of Environmental Research and Public Health, 19(18), 11228. https://doi.org/10.3390/ijerph191811228