
Work-Related Traumatic Stress Response in Nurses Employed in COVID-19 Settings

 , , ,
, , ,  ,
, 
Abstract
:
1. Introduction
1.1. Work-Related Psychosocial Hazards and Work-Related Stress Response in Healthcare Professionals Working in COVID-19 Settings
1.2. Work-Related Traumatic Stress Response in Healthcare Professionals Working in COVID-19 Settings
1.3. The Present Study: Aim and Objectives
2. Materials and Methods
2.1. Design
2.2. Study Settings and Context
2.3. Sample Size and Sampling
2.4. Participants
2.5. Variables and Measurements
2.6. Data Collection and Instrument
2.7. Ethical Issues
2.8. Data Analysis
3. Results
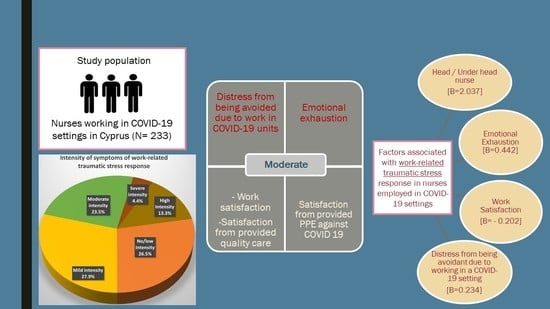
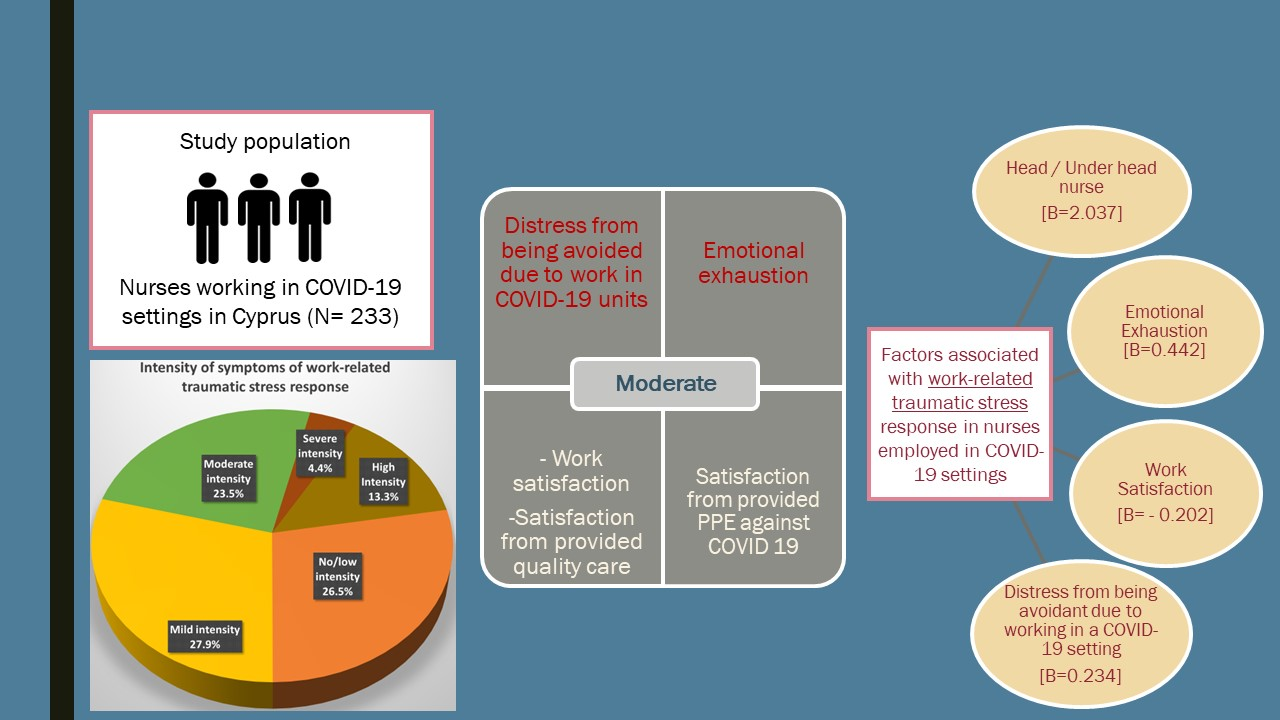
3.1. Sociodemographic, Work and Employment Characteristics of Participants
3.2. Work-Related Psychosocial Hazards and Work-Related Stress Response
3.3. Work-Related Traumatic Stress Response (Total STSS-M Scores)
3.4. Associations between STSS-M Scores and Work-Related Satisfaction and Distress
3.5. Multivariable Analysis of Predictors of Work-Related Traumatic Stress Response (STSS-M Score)
4. Discussion
4.1. Future Research Directions
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davide, A.D.; Arechy, A.R.; Buchthal, O.V.; Kaholokula, J.K.A.; Hermosura, A.H. Identifying the physical and emotional needs of health care workers in Hawai‘I during the COVID-19 pandemic. Hawaii J. Health Soc. Welf. 2022, 84, 101–107. [Google Scholar]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Tong, Z.; Guan, X.; Du, B.; Qiu, H.; Slutsky, A.S. Critical care crisis and some recommendations during the COVID-19 epidemic in China. Intensive Care Med. 2020, 46, 837–840. [Google Scholar] [CrossRef]
- Qi, M.; Li, P.; Moyle, W.; Weeks, B.; Jones, C. Physical activity, health-related quality of life, and stress among the Chinese adult population during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6494. [Google Scholar] [CrossRef] [PubMed]
- Villarreal-Zegarra, D.; Copez-Lonzoy, A.; Vilela-Estrada, A.L.; Huarcaya-Victoria, J. Depression, post-traumatic stress, anxiety, and fear of COVID-19 in the general population and health-care workers: Prevalence, relationship, and explicative model in Peru. BMC Psychiatry 2021, 21, 455. [Google Scholar] [CrossRef] [PubMed]
- Cox, T.; Griffiths, A. The nature and measurement of work-related stress: Theory and practice. In Evaluation of Human Work, 3rd ed.; Wilson, J.R., Corlett, N., Eds.; Routledge: Abingdon, UK, 2005; pp. 553–571. [Google Scholar]
- Leng, M.; Wei, L.; Shi, X.; Cao, G.; Wei, Y.; Xu, H.; Zhang, X.; Zhang, W.; Xing, S.; Wei, H. Mental distress and influencing factors in nurses caring for patients with COVID-19. Nurs. Crit. Care 2021, 26, 94–101. [Google Scholar] [CrossRef]
- Ghio, L.; Patti, S.; Piccinini, G.; Modafferi, C.; Lusetti, E.; Mazzella, M.; Del Sette, M. Anxiety, Depression and Risk of Post-Traumatic Stress Disorder in Health Workers: The Relationship with Burnout during COVID-19 Pandemic in Italy. Int. J. Environ. Res. Public Health 2021, 18, 9929. [Google Scholar] [CrossRef]
- Sanchez-Gomez, M.; Sadovyy, M.; Breso, E. Health-Care Professionals Amid the COVID-19 Pandemic: How Emotional Intelligence May Enhance Work Performance Traversing the Mediating Role of Work Engagement. J. Clin. Med. 2021, 10, 4077. [Google Scholar] [CrossRef]
- Evanoff, B.A.; Strickland, J.R.; Dale, A.M.; Hayibor, L.; Page, E.; Duncan, J.G.; Kannampallil, T.; Gray, D.L. Correction: Work-Related and Personal Factors Associated With Mental Well-Being During the COVID-19 Response: Survey of Health Care and Other Workers. J. Med. Internet Res. 2021, 4, e29069. [Google Scholar] [CrossRef]
- van den Berg, T.I.; Elders, L.A.; de Zwart, B.C.; Burdorf, A. The effects of work-related and individual factors on the Work Ability Index: A systematic review. Occup. Environ. Med. 2009, 4, 211–220. [Google Scholar] [CrossRef]
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. Social capital and sleep quality in individuals who self-isolated for 14 days during the coronavirus disease 2019 (COVID-19) outbreak in January 2020 in China. Med. Sci. Monit. 2020, 26, e923921. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Juang, Y.Y.; Su, Y.J.; Lee, H.L.; Lin, Y.H.; Chao, C.C. Facing SARS: Psychological impacts on SARS team nurses and psychiatric services in a Taiwan general hospital. Gen. Hosp. Psychiatry 2005, 27, 352–358. [Google Scholar] [CrossRef] [PubMed]
- White, D.B.; Lo, B. A framework for rationing ventilators and critical care beds during the COVID-19 pandemic. JAMA 2020, 323, 1773–1774. [Google Scholar] [CrossRef] [PubMed]
- de Cordova, P.B.; Johansen, M.L.; Grafova, I.B.; Crincoli, S.; Prado, J.; Pogorzelska-Maziarz, M. Burnout and intent to leave during COVID-19: A cross-sectional study of New Jersey hospital nurses. J. Nurs. Manag. 2022. [Google Scholar] [CrossRef]
- Labrague, L.J.; de Los Santos, J.A.A. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J. Nurs. Manag. 2021, 29, 395–403. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses′ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 8, 3286–3302. [Google Scholar] [CrossRef]
- Sheppard, K.N.; Runk, B.G.; Maduro, R.S.; Fancher, M.; Mayo, A.N.; Wilmoth, D.D.; Morgan, M.K.; Zimbro, K.S. Nursing Moral Distress and Intent to Leave Employment During the COVID-19 Pandemic. J. Nurs. Care Qual. 2022, 1, 28–34. [Google Scholar] [CrossRef]
- Maben, J.; Conolly, A.; Abrams, R.; Rowland, E.; Harris, R.; Kelly, D.; Kent, B.; Couper, K. Impact of Covid On Nurses (ICON) Survey Research Group. ‘You can′t walk through water without getting wet’ UK nurses′ distress and psychological health needs during the Covid-19 pandemic: A longitudinal interview study. Int. J. Nurs. Stud. 2022, 131, 104242. [Google Scholar] [CrossRef]
- Orrù, G.; Marzetti, F.; Conversano, C.; Vagheggini, G.; Miccoli, M.; Ciacchini, R.; Panait, E.; Gemignani, A. Secondary traumatic stress and burnout in healthcare workers during COVID-19 outbreak. Int. J. Environ. Res. Public Health 2021, 18, 337. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; pp. 271–280. [Google Scholar]
- Sanchez-Gomez, M.; Giorgi, G.; Finstad, G.L.; Urbini, F.; Foti, G.; Mucci, N.; Zaffina, S.; León-Perez, J.M. COVID-19 Pandemic as a Traumatic Event and Its Associations with Fear and Mental Health: A Cognitive-Activation Approach. Int. J. Environ. Res. Public Health 2021, 14, 7422. [Google Scholar] [CrossRef] [PubMed]
- Bride, B.E. Prevalence of secondary traumatic stress among social workers. Soc. Work 2007, 52, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Seun-Fadipe, C.T.; Akinsulore, A.A.; Oginni, O.A. Workplace violence and risk for psychiatric morbidity among health workers in a tertiary health care setting in Nigeria: Prevalence and correlates. Psychiatry Res. 2019, 272, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Theorell, T.; Hammarström, A.; Aronsson, G.; Träskman Bendz, L.; Grape, T.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Hall, C. A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health 2015, 15, 738. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, S.; Lees, T.; Lal, S. Prevalence and risk factors of depression, anxiety, and stress in a cohort of Australian nurses. Int. J. Environ. Res. Public Health 2018, 16, 61. [Google Scholar] [CrossRef]
- Colville, G.A.; Smith, J.G.; Brierley, J.; Citron, K.; Nguru, N.M.; Shaunak, P.D.; Tam, O.; Perkins-Porras, L. Coping with staff burnout and work-related posttraumatic stress in intensive care. Pediatr. Crit. Care Med. 2017, 18, e267–e273. [Google Scholar] [CrossRef]
- Junne, F.; Michaelis, M.; Rothermund, E.; Stuber, F.; Gündel, H.; Zipfel, S.; Rieger, M.A. The role of work-related factors in the development of psychological distress and associated mental disorders: Differential views of human resource managers, occupational physicians, primary care physicians and psychotherapists in Germany. Int. J. Environ. Res. Public Health 2018, 15, 559. [Google Scholar] [CrossRef]
- Tu, Z.H.; He, J.W.; Zhou, N. Sleep quality and mood symptoms in conscripted frontline nurse in Wuhan, China during COVID-19 outbreak: A cross-sectional study. Med. Baltim. 2020, 99, e20769. [Google Scholar] [CrossRef] [PubMed]
- Chatzittofis, A.; Karanikola, M.; Michailidou, K.; Constantinidou, A. Impact of the COVID-19 pandemic on the mental health of healthcare workers. Int. J. Environ. Res. Public Health 2021, 18, 1435. [Google Scholar] [CrossRef]
- d′Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-traumatic stress symptoms in healthcare workers dealing with the covid-19 pandemic: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 601. [Google Scholar] [CrossRef]
- Firew, T.; Sano, E.D.; Lee, J.W.; Flores, S.; Lang, K.; Salman, K.; Greene, M.C.; Chang, B.P. Protecting the front line: A cross-sectional survey analysis of the occupational factors contributing to healthcare workers′ infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open 2020, 10, e042752. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N.; Weston, D.; Hall, C.; Caulfield, T.; Williamson, V.; Fong, K. Mental health of staff working in intensive care during Covid-19. Occup. Med. 2021, 71, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Sinigaglia, T.; Lo Moro, G.; Rousset, S.; Cremona, A.; Bert, F.; Bert, F.; Siliquini, R. The burden of burnout among healthcare professionals of intensive care units and emergency departments during the covid-19 pandemic: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 8172. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.; Wang, M.; Song, T.; Wu, Y.; Luo, J.; Chen, L.; Yan, L. The psychological impact of covid-19 pandemic on health care workers: A systematic review and meta-analysis. Front. Psychol. 2021, 12, 626547. [Google Scholar] [CrossRef]
- Williams, R.; Kaufman, K.R. Narrative review of the COVID-19, healthcare and healthcarers thematic series. BJPsych Open 2022, 8, e34. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 9, 813–824. [Google Scholar] [CrossRef]
- STROBE, Strengthening the Reporting of Observational Studies in Epidemiology. Available online: http://www.strobe-statement.org/ (accessed on 13 June 2022).
- Christodoulou-Fella, M.; Middleton, N.; Papathanassoglou, E.D.E.; Karanikola, M.N.K. Exploration of the Association between Nurses′ Moral Distress and Secondary Traumatic Stress Syndrome: Implications for Patient Safety in Mental Health Services. Biomed. Res. Int. 2017, 2017, 1908712. [Google Scholar] [CrossRef]
- Aristidou, L.; Mpouzika, M.; Papathanassoglou, E.D.E.; Middleton, N.; Karanikola, M.N.K. Association between workplace bullying occurrence and trauma symptoms among healthcare professionals in Cyprus. Front. Psychol. 2020, 11, 575623. [Google Scholar] [CrossRef]
- Bani Issa, W.; Al Nusair, H.; AlTamimi, A.; Rababa, M.; Saqan, R.; Hijazi, H.; Al-Marzouqi, A.; Abdul Rahman, H.; Naing, L. Posttraumatic stress disorders and influencing factors during the COVID-19 pandemic: A cross-sectional study of frontline nurses. Int. Nurs. Rev. 2021, 69, 285–293. [Google Scholar] [CrossRef]
- Crowe, S.; Howard, A.F.; Vanderspank-Wright, B.; Gillis, P.; McLeod, F.; Penner, C.; Haljan, G. The effect of COVID-19 pandemic on the mental health of Canadian critical care nurses providing patient care during the early phase pandemic: A mixed method study. Intensive Crit. Care Nurs. 2021, 63, 102999. [Google Scholar] [CrossRef]
- Kackin, O.; Ciydem, E.; Aci, O.S.; Kutlu, F.Y. Experiences and psychosocial problems of nurses caring for patients diagnosed with COVID-19 in Turkey: A qualitative study. Int. J. Soc. Psychiatry 2021, 67, 158–167. [Google Scholar] [CrossRef]
- Inocian, E.P.; Cruz, J.P.; Saeed Alshehry, A.; Alshamlani, Y.; Ignacio, E.H.; Tumala, R.B. Professional quality of life and caring behaviours among clinical nurses during the COVID-19 pandemic. J. Clin. Nurs. 2021, 78, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Leitão, J.; Pereira, D.; Gonçalves, Â. Quality of work life and organizational performance: Workers′ feelings of contributing, or not, to the organization′s productivity. Int. J. Environ. Res. Public Health 2019, 16, 3803. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Chen, L.; Feng, F.; Okoli, C.T.C.; Tang, P.; Zeng, L.; Jin, M.; Zhang, Y.; Wang, J. The prevalence of compassion satisfaction and compassion fatigue among nurses: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2021, 120, 103973. [Google Scholar] [CrossRef] [PubMed]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in Spanish health personnel during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef]
- Maunder, R.; Hunter, J.; Vincent, L.; Bennett, J.; Peladeau, N.; Leszcz, M.; Sadavoy, J.; Verhaeghe, L.M.; Steinberg, R.; Mazzulli, T. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ 2003, 168, 1245–1251. [Google Scholar]
- Su, T.P.; Lien, T.C.; Yang, C.Y.; Su, Y.L.; Wang, J.H.; Tsai, S.L.; Yin, J.C. Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: A prospective and periodic assessment study in Taiwan. J. Psychiatr. Res. 2007, 41, 119–130. [Google Scholar] [CrossRef]
- Arpacioglu, S.; Gurler, M.; Cakiroglu, S. Secondary traumatization outcomes and associated factors among the health care workers exposed to the COVID-19. Int. J. Soc. Psychiatry 2021, 67, 84–89. [Google Scholar] [CrossRef]
- Chen, R.; Sun, C.; Chen, J.J.; Jen, H.J.; Kang, X.L.; Kao, C.C.; Chou, K.R. A large-scale survey on trauma, burnout, and posttraumatic growth among nurses during the COVID-19 pandemic. Int. J. Ment. Health Nurs. 2021, 30, 102–116. [Google Scholar] [CrossRef]
- Laurent, A.; Fournier, A.; Lheureux, F.; Poujol, A.L.; Deltour, V.; Ecarnot, F.; Meunier-Beillard, N.; Loiseau, M.; Binquet, C.; Quenot, J.P. Risk and protective factors for the possible development of post-traumatic stress disorder among intensive care professionals in France during the first peak of the COVID-19 epidemic. Eur. J. Psychotraumatol. 2022, 13, 2011603. [Google Scholar] [CrossRef]
- Alonso, J.; Vilagut, G.; Mortier, P.; Ferrer, M.; Alayo, I.; Aragón-Peña, A.; Aragonès, E.; Campos, M.; Cura-González, I.D.; Emparanza, J.I.; et al. Mental health impact of the first wave of COVID-19 pandemic on Spanish healthcare workers: A large cross-sectional survey. Rev. Psiquiatr. Salud Ment. 2021, 14, 90–105. [Google Scholar] [CrossRef]
- Zewudie, A.; Regasa, T.; Kebede, O.; Abebe, L.; Feyissa, D.; Ejata, F.; Feyisa, D.; Mamo, Y. Healthcare professionals′ willingness and preparedness to work during COVID-19 in selected hospitals of southwest Ethiopia. Risk Manag. Healthc. Policy 2021, 14, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Cockerham, M.; Beier, M.E.; Branson, S.; Boss, L. Nurse adaptability and post-traumatic stress disorder symptoms during the COVID-19 pandemic: The effects of family and perceived organizational support. Front. Psychol. 2022, 12, 749763. [Google Scholar] [CrossRef] [PubMed]
- Feingold, J.H.; Peccoralo, L.; Chan, C.C.; Kaplan, C.A.; Kaye-Kauderer, H.; Charney, D.; Verity, J.; Hurtado, A.; Burka, L.; Syed, S.A.; et al. Psychological impact of the COVID-19 pandemic on frontline health care workers during the pandemic surge in New York City. Chronic Stress 2021, 5, 2470547020977891. [Google Scholar] [CrossRef] [PubMed]
- Greene, T.; Harju-Seppänen, J.; Adeniji, M.; Steel, C.; Grey, N.; Brewin, C.R.; Bloomfield, M.A.; Billings, J. Predictors and rates of PTSD, depression and anxiety in UK frontline health and social care workers during COVID-19. Eur. J. Psychotraumatol. 2021, 12, 1882781. [Google Scholar] [CrossRef]
- Zhang, S.X.; Sun, S.; Afshar Jahanshahi, A.; Alvarez-Risco, A.; Ibarra, V.G.; Li, J.; Patty-Tito, R.M. Developing and testing a measure of COVID-19 organizational support of healthcare workers-results from Peru, Ecuador, and Bolivia. Psychiatry Res. 2020, 291, 113174. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Nadjidai, S.E.; Murgier, J.; Ng, C.H. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav. Immun. Health 2020, 8, 100144. [Google Scholar] [CrossRef]
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. A Systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef]
- Kim, S.H.; Schneider, S.M.; Bevans, M.; Kravitz, L.; Mermier, C.; Qualls, C.; Burge, M.R. PTSD symptom reduction with mindfulness-based stretching and deep breathing exercise: Randomized controlled clinical trial of efficacy. J. Clin. Endocrinol. Metab. 2013, 98, 2984–2992. [Google Scholar] [CrossRef]
- Tracy, D.K.; Tarn, M.; Eldridge, R.; Cooke, J.; Calder, J.D.F.; Greenberg, N. What should be done to support the mental health of healthcare staff treating COVID-19 patients? Br. J. Psychiatry 2020, 217, 537–539. [Google Scholar] [CrossRef]
- Center for the Study of Traumatic Stress. Available online: https://www.cstsonline.org (accessed on 13 June 2022).

{kind=link}
| N | Percentage (%) | |
|---|---|---|
| Gender | ||
| Male | 86 | 36.9 |
| Female | 147 | 63.1 |
| Age | ||
| Up to 35 years | 136 | 58.4 |
| 35–45 years | 60 | 25.7 |
| >45 years | 37 | 15.9 |
| City of Employment | ||
| Nicosia | 124 | 53.2 |
| Limassol | 65 | 27.9 |
| Famagusta (COVID-19 Referral Hospital) | 44 | 18.9 |
| Marital Status | ||
| Married | 157 | 67.4 |
| Unmarried | 76 | 32.6 |
| Number of Children | ||
| No children | 77 | 33.0 |
| 1–3 children | 146 | 62.7 |
| >3 children | 10 | 4.3 |
| Education | ||
| No post-graduate education | 172 | 73.8 |
| Post-graduate education | 61 | 26.2 |
| Total Work Experience in Nursing | ||
| <5 years | 12 | 5.2 |
| 5–10 years | 88 | 37.8 |
| >10 years | 133 | 57.0 |
| Ranking | ||
| Staff nurse | 218 | 93.6 |
| Head nurse/under head nurse | 15 | 6.4 |
| Total Number of Patients Treated per Work Setting | ||
| <10 patients | 175 | 75.1 |
| 10–20 patients | 38 | 16.3 |
| >20 patients | 20 | 8.6 |
| Number of Deaths per Day in the Previous Month from Any Cause | ||
| <5 | 209 | 89.7 |
| >5 | 24 | 10.3 |
| Number of Night Shifts per Month | ||
| <5 | 104 | 44.6 |
| >5 | 129 | 55.4 |
| Visual Analogue Scales | Median | Mean | St. Deviation |
|---|---|---|---|
| Degree of Experienced Satisfaction | |||
| Degree of work satisfaction | 6.00 | 6.21 | 2.16 |
| Degree of satisfaction from provided care in the last month | 7.00 | 6.87 | 2.02 |
| Degree of satisfaction from information (quality/quantity) provided about COVID-19 by the administrative office/managers of your hospital | 5.00 | 4.79 | 2.91 |
| Degree of satisfaction from the personal protective equipment against COVID-19 provided to you by your hospital | 6.00 | 6.00 | 2.29 |
| Degree of Experienced Distress | |||
| Degree of emotional exhaustion | 8.00 | 7.33 | 2.29 |
| Degree of distress experienced from being avoided due to work in a COVID-19 healthcare setting during the pandemic | 8.00 | 6.98 | 2.69 |
| Scale | Range | Distribution of STSS-M Scores in Percentiles | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-Clinical Symptoms | Clinical Symptoms | |||||||||
| M (SD) | Median | Actual Scale Range | Observed Scale Range | 25th | 50th | 75th | 90th | 95th | ||
| 45.38 (12.97) | 46.00 | 17–85 | 17–80 | Total STSS-M score | 36 | 45 | 55 | 62 | 67 | |
| Frequency (%) | 74.3% | 25.7% | ||||||||
| Work-Related Satisfaction/Distress Variables | Pearson’s r | p-Value |
|---|---|---|
| Degree of emotional exhaustion | 0.490 | <0.001 |
| Degree of professional satisfaction | −0.298 | <0.001 |
| Degree of satisfaction from provided care in the last month | −0.201 | 0.002 |
| Degree of satisfaction from information (quality/quantity) provided about COVID-19 by the administrative office/managers of your hospital | −0.204 | 0.002 |
| Degree of satisfaction from the personal protective equipment against COVID-19 provided to you by your hospital | −0.232 | <0.001 |
| Degree of distress experienced from being avoided due to work in a COVID-19 healthcare setting during the pandemic | 0.317 | <0.001 |
| p-Value | Exp(B) | 95% C.I. for EXP(B) | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Ranking Head nurse/Under head nurse Staff nurse | 0.025 | 7.669 | 1.285 | 45.755 |
| Emotional Exhaustion | 0.000 | 1.556 | 1.242 | 1.950 |
| Work Satisfaction | 0.013 | 0.817 | 0.696 | 0.959 |
| Distress Experienced from Being Avoided due to Work in a COVID-19 Wetting | 0.004 | 1.264 | 1.076 | 1.485 |
| Constant | 0.000 | 0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karanikola, M.; Mpouzika, M.; Papathanassoglou, E.; Kaikoushi, K.; Hatzioannou, A.; Leontiou, I.; Livadiotis, C.; Christophorou, N.; Chatzittofis, A. Work-Related Traumatic Stress Response in Nurses Employed in COVID-19 Settings. Int. J. Environ. Res. Public Health 2022, 19, 11049. https://doi.org/10.3390/ijerph191711049
Karanikola M, Mpouzika M, Papathanassoglou E, Kaikoushi K, Hatzioannou A, Leontiou I, Livadiotis C, Christophorou N, Chatzittofis A. Work-Related Traumatic Stress Response in Nurses Employed in COVID-19 Settings. International Journal of Environmental Research and Public Health. 2022; 19(17):11049. https://doi.org/10.3390/ijerph191711049
Chicago/Turabian StyleKaranikola, Maria, Meropi Mpouzika, Elizabeth Papathanassoglou, Katerina Kaikoushi, Anna Hatzioannou, Ioannis Leontiou, Chris Livadiotis, Nicos Christophorou, and Andreas Chatzittofis. 2022. "Work-Related Traumatic Stress Response in Nurses Employed in COVID-19 Settings" International Journal of Environmental Research and Public Health 19, no. 17: 11049. https://doi.org/10.3390/ijerph191711049
APA StyleKaranikola, M., Mpouzika, M., Papathanassoglou, E., Kaikoushi, K., Hatzioannou, A., Leontiou, I., Livadiotis, C., Christophorou, N., & Chatzittofis, A. (2022). Work-Related Traumatic Stress Response in Nurses Employed in COVID-19 Settings. International Journal of Environmental Research and Public Health, 19(17), 11049. https://doi.org/10.3390/ijerph191711049