
Consistency Analysis in Medical Empathy Intervention Research

 , and
, and
Abstract
:1. Introduction
2. Methods
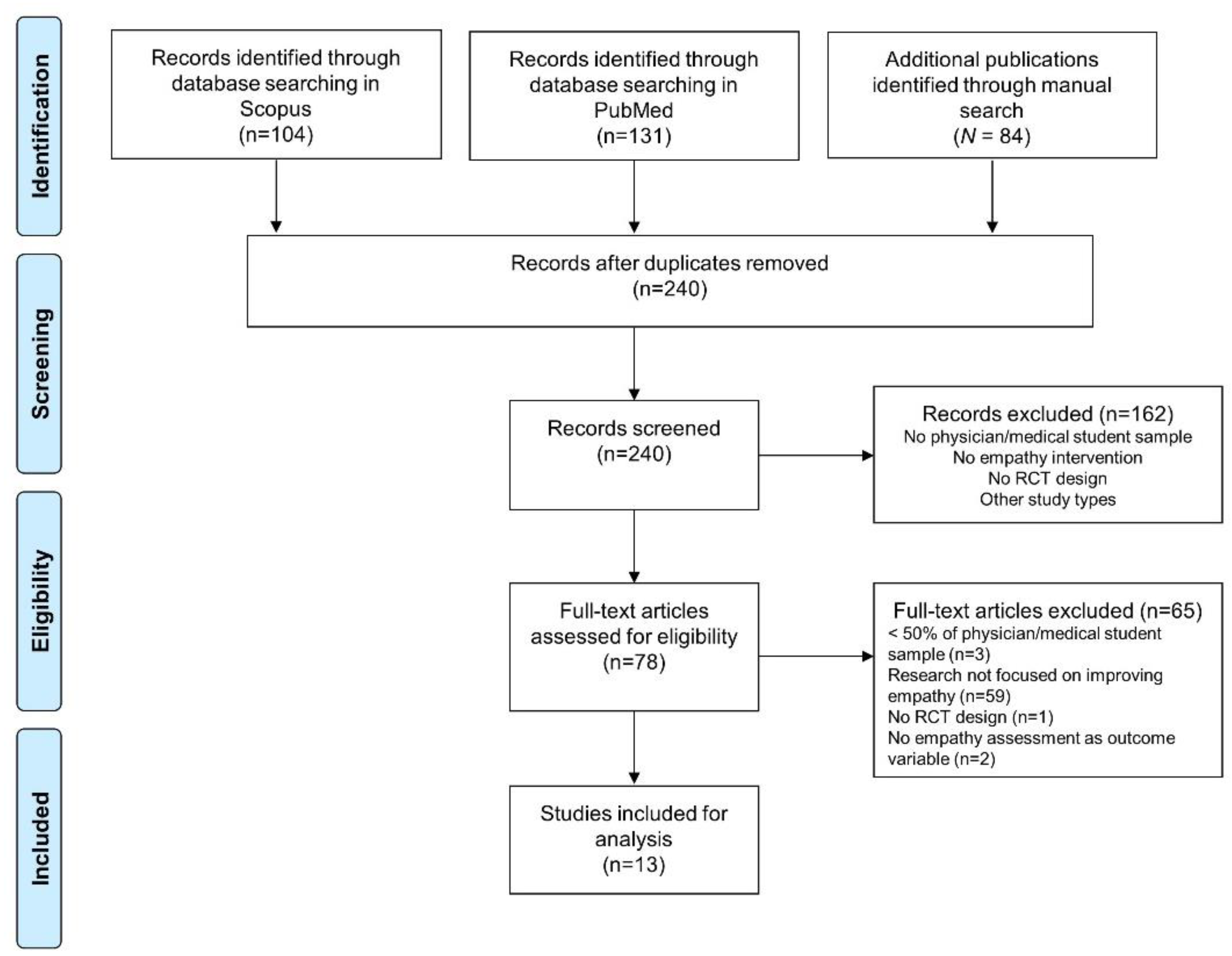
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.2.1. Dimensions of Empathy in Definition, Intervention, and Assessment Sections
2.2.2. Aspects of the KAB Model in Intervention and Assessment Sections of Empathy
2.3. Data Analysis
2.3.1. Consistency in Terms of Empathy Dimensions among Definition, Intervention, and Assessment Sections
2.3.2. Consistency in Terms of Aspects of the KAB Model between Intervention and Assessment Sections
3. Results
3.1. Empathy Dimensions
3.1.1. Definition
3.1.2. Intervention
3.1.3. Assessment
3.2. Consistency in Terms of Empathy Dimensions among Definition, Intervention, and Assessment Sections
3.2.1. Overall Consistency
3.2.2. Pairwise Comparison of the Consistency
3.3. Aspects of the KAB Model
3.3.1. Intervention
3.3.2. Assessment
3.4. Consistency in Terms of KAB Aspects between Intervention and Assessment Sections
4. Discussions
4.1. Empathy Dimensions
4.2. Aspects of the KAB Model
4.3. Evaluation of Patient Satisfaction or Trust as an Outcome Measure
4.4. Recommendations
4.4.1. An Ideal Design for Empathy Intervention Studies
4.4.2. Matching in Corresponding Sections
4.4.3. Real-World Concerns Regarding Already-Developed Measures
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Terms and Strategies
Appendix B. Categorization Criteria of Empathy Dimensions in the Definition, Intervention, and Assessment Sections
- Cognitive empathy was considered as knowing or understanding others’ thoughts or thought processes.
- Affective empathy was considered as understanding or recognizing others’ feelings or emotional states.
- Behavioral empathy was considered as performing actions, behaviors, or responses for showing understanding toward others.
- Cognitive empathy was considered as teaching participants how to understand or recognize others’ thoughts, perspectives, or thought processes.
- Affective empathy was considered as teaching participants how to understand or recognize others’ feelings or emotional states.
- Behavioral empathy was considered as teaching participants how to communicate with others or how to show their understanding to others.
- A measure was classified as assessing cognitive empathy if its item(s) aimed to evaluate or estimate one’s ability or tendency to understand or recognize others’ thoughts or thought processes.
- A measure was classified as assessing affective empathy if its item(s) aimed to evaluate or estimate one’s ability or tendency to understand or recognize others’ feelings or emotional states.
- A measure was classified as assessing behavioral empathy if its item(s) aimed to evaluate actions or behaviors that were \performed in order to show understanding to others.
Appendix C. Categorization Criteria of Knowledge–Attitude–Behavior (KAB) Aspects in Intervention and Assessment Sections
- The knowledge aspects include various forms of education delivering relevant knowledge of empathy, such as the definition of empathy, theory of empathy, or neural basis of empathy.
- The attitude aspects include activities promoting the importance of empathy or beliefs about empathy. Example activities include group discussions or lectures improving beliefs about and the importance of empathy.
- The behavior aspects include activities providing principles or practical methods to enhance empathic responses to others. Example activities include empathic communication skill workshops or emotion recognition training classes.
- The knowledge aspects include item(s) evaluating one’s knowledge of empathy, such as the definition of empathy.
- The attitude aspects include item(s) evaluating one’s beliefs about or attitudes toward empathy.
- The behavior aspects include item(s) evaluating one’s expression of empathy.
References
- Sulzer, S.H.; Feinstein, N.W.; Wendland, C.L. Assessing empathy development in medical education: A systematic review. Med. Educ. 2016, 50, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.S.; Daughtridge, R.; Sloane, P.D. Physician-patient communication in the primary care office: A systematic review. J. Am. Board Fam. Med. 2002, 15, 25–38. [Google Scholar]
- Larson, E.B.; Yao, X. Clinical empathy as emotional labor in the patient-physician relationship. JAMA 2005, 293, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Mangione, S.; Nasca, T.J.; Rattner, S.; Erdmann, J.B.; Gonnella, J.S.; Magee, M. An empirical study of decline in empathy in medical school. Med. Educ. 2004, 38, 934–941. [Google Scholar] [CrossRef]
- Pedersen, R. Empirical research on empathy in medicine—A critical review. Patient Educ. Couns. 2009, 76, 307–322. [Google Scholar] [CrossRef]
- Rogers, C.R. The necessary and sufficient conditions of therapeutic personality change. Psychotherapy 2007, 44, 240–248. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; West, C.; Zhao, X.; Novotny, P.; Kolars, J.; Habermann, T.; Sloan, J. Relationship between increased personal well-being and enhanced empathy among internal medicine residents. J. Gen. Intern. Med. 2005, 20, 559–564. [Google Scholar] [CrossRef]
- Mercer, S.W.; Reynolds, W.J. Empathy and quality of care. Br. J. Gen. Pract. 2002, 52, S9–S12. [Google Scholar]
- Levett-Jones, T.; Cant, R.; Lapkin, S. A systematic review of the effectiveness of empathy education for undergraduate nursing students. Nurse Educ. Today 2019, 75, 80–94. [Google Scholar] [CrossRef]
- Hojat, M.; Axelrod, D.; Spandorfer, J.; Mangione, S. Enhancing and sustaining empathy in medical students. Med. Teach. 2013, 35, 996–1001. [Google Scholar] [CrossRef]
- Fragkos, K.C.; Crampton, P.E.S. The Effectiveness of Teaching Clinical Empathy to Medical Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Acad. Med. 2020, 95, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.A.; Schwartz, R. Empathy present and future. J. Soc. Psychol. 2019, 159, 225–243. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; LaNoue, M. Exploration and confirmation of the latent variable structure of the Jefferson scale of empathy. Int. J. Med. Educ. 2014, 5, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Bettinghaus, E.P. Health promotion and the knowledge-attitude-behavior continuum. Prev. Med. 1986, 15, 475–491. [Google Scholar] [CrossRef]
- Schneider, B.; Cheslock, N. Measuring Results: Gaining Insight on Behavior Change Strategies and Evaluation Methods from Environmental Education, Museum, Health, and Social Marketing Programs; Coevolution Institute: San Francisco, CA, USA, 2003. [Google Scholar]
- Schrader, P.G.; Lawless, K.A. The knowledge, attitudes, & behaviors approach how to evaluate performance and learning in complex environments. Perform. Improv. 2004, 43, 8–15. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. (Eds.) JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Bonvicini, K.A.; Perlin, M.J.; Bylund, C.L.; Carroll, G.; Rouse, R.A.; Goldstein, M.G. Impact of communication training on physician expression of empathy in patient encounters. Patient Educ. Couns. 2009, 75, 3–10. [Google Scholar] [CrossRef]
- Bonvicini, K.A. Physician empathy: Impact of communication training on physician behavior and patient perceptions. In Dissertation Abstract International; University of Phoenix, School of Advanced Studies: Phoenix, AZ, USA, 2007; p. B 68/08. [Google Scholar]
- Bylund, C.L.; Makoul, G. Empathic communication and gender in the physician–patient encounter. Patient Educ. Couns. 2002, 48, 207–216. [Google Scholar] [CrossRef]
- Bunn, W.; Terpstra, J. Cultivating empathy for the mentally ill using simulated auditory hallucinations. Acad. Psychiatry 2009, 33, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Mangione, S.; Nasca, T.J.; Cohen, M.J.M.; Gonnella, J.S.; Erdmann, J.B.; Veloski, J.; Magee, M. The Jefferson Scale of Physician Empathy: Development and Preliminary Psychometric Data. Educ. Psychol. Meas. 2001, 61, 349–365. [Google Scholar] [CrossRef]
- Blatt, B.; LeLacheur, S.F.; Galinsky, A.D.; Simmens, S.J.; Greenberg, L. Does perspective-taking increase patient satisfaction in medical encounters? Acad. Med. 2010, 85, 1445–1452. [Google Scholar] [CrossRef]
- Whelan, G.P.; Boulet, J.R.; McKinley, D.W.; Norcini, J.J.; van Zanten, M.; Hambleton, R.K.; Burdick, W.P.; Peitzman, S.J. Scoring standardized patient examinations: Lessons learned from the development and administration of the ECFMG Clinical Skills Assessment (CSA). Med. Teach. 2005, 27, 200–206. [Google Scholar] [CrossRef] [PubMed]
- van Zanten, M.; Boulet, J.R.; McKinley, D. Using standardized patients to assess the interpersonal skills of physicians: Six years’ experience with a high-stakes certification examination. Health Commun. 2007, 22, 195–205. [Google Scholar] [CrossRef] [PubMed]
- USMLE. USMLE Step 2 CS Content Description and General Information Booklet: United States Medical Licensing Examination. Available online: http://www.usmle.org/Examinations/step2/step2cs_content.html. (accessed on 5 February 2009).
- Tulsky, J.A.; Arnold, R.M.; Alexander, S.C.; Olsen, M.K.; Jeffreys, A.S.; Rodriguez, K.L.; Skinner, C.S.; Farrell, D.; Abernethy, A.P.; Pollak, K.I. Enhancing communication between oncologists and patients with a computer-based training program: A randomized trial. Ann. Intern. Med. 2011, 155, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Fischer, G.; Tulsky, J.; Arnold, R. Communicating a poor prognosis. In Topics in Palliative Care; Portenoy, R., Bruera, E., Eds.; Oxford Univ Press: New York, NY, USA, 2000. [Google Scholar]
- Smith, R.C.; Hoppe, R.B. The patient’s story: Integrating the patient- and physician-centered approaches to interviewing. Ann. Intern. Med. 1991, 115, 470–477. [Google Scholar] [CrossRef]
- Suchman, A.L.; Markakis, K.; Beckman, H.B.; Frankel, R. A model of empathic communication in the medical interview. JAMA 1997, 277, 678–682. [Google Scholar] [CrossRef]
- Mercer, S.W.; Maxwell, M.; Heaney, D.; Watt, G.C. The consultation and relational empathy (CARE) measure: Development and preliminary validation and reliability of an empathy-based consultation process measure. Fam. Pract. 2004, 21, 699–705. [Google Scholar] [CrossRef]
- Riess, H.; Kelley, J.M.; Bailey, R.W.; Dunn, E.J.; Phillips, M. Empathy training for resident physicians: A randomized controlled trial of a neuroscience-informed curriculum. J. Gen. Intern. Med. 2012, 27, 1280–1286. [Google Scholar] [CrossRef]
- Mehrabian, A.; Epstein, N. A measure of emotional empathy. J. Personal. 1972, 40, 525–543. [Google Scholar] [CrossRef]
- Potash, J.S.; Chen, J.Y.; Lam, C.L.; Chau, V.T. Art-making in a family medicine clerkship: How does it affect medical student empathy? BMC Med. Educ. 2014, 14, 247. [Google Scholar] [CrossRef]
- Fields, S.K.; Mahan, P.; Tillman, P.; Harris, J.; Maxwell, K.; Hojat, M. Measuring empathy in healthcare profession students using the Jefferson Scale of Physician Empathy: Health Provider—Student version. J. Interprof. Care 2011, 25, 287–293. [Google Scholar] [CrossRef]
- Hojat, M.; Gonnella, J.S.; Nasca, T.J.; Mangione, S.; Vergare, M.; Magee, M. Physician empathy: Definition, components, measurement, and relationship to gender and specialty. Am. J. Psychiatry 2002, 159, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.; Chaudhary, N.; Kim, T.; Waller, J.L.; Wong, J.; Borish, M.; Cordar, A.; Lok, B.; Buckley, P.F. Using Virtual Patients to Teach Empathy: A Randomized Controlled Study to Enhance Medical Students’ Empathic Communication. Simul. Healthc. 2016, 11, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Buffel du Vaure, C.; Lemogne, C.; Bunge, L.; Catu-Pinault, A.; Hoertel, N.; Ghasarossian, C.; Vincens, M.E.; Galam, E.; Jaury, P. Promoting empathy among medical students: A two-site randomized controlled study. J. Psychosom. Res. 2017, 103, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Bitoun, A. Validation du Score JSPE-Medical Student© en Langue Française Dans L’évaluation de L’empathie des Étudiants en Médecine. Ph.D. Thesis, Universidad de París V Descartes, Paris, France, 2017. [Google Scholar]
- LoSasso, A.A.; Lamberton, C.E.; Sammon, M.; Berg, K.T.; Caruso, J.W.; Cass, J.; Hojat, M. Enhancing Student Empathetic Engagement, History-Taking, and Communication Skills During Electronic Medical Record Use in Patient Care. Acad. Med. 2017, 92, 1022–1027. [Google Scholar] [CrossRef]
- Kane, G.C.; Gotto, J.L.; Mangione, S.; West, S.; Hojat, M. Jefferson Scale of Patient’s Perceptions of Physician Empathy: Preliminary psychometric data. Croat. Med. J. 2007, 48, 81–86. [Google Scholar]
- Wündrich, M.; Schwartz, C.; Feige, B.; Lemper, D.; Nissen, C.; Voderholzer, U. Empathy training in medical students—A randomized controlled trial. Med. Teach. 2017, 39, 1096–1098. [Google Scholar] [CrossRef]
- Preusche, I.; Wagner-Menghin, M. Rising to the challenge: Cross-cultural adaptation and psychometric evaluation of the adapted German version of the Jefferson Scale of Physician Empathy for Students (JSPE-S). Adv. Health Sci. Educ. 2013, 18, 573–587. [Google Scholar] [CrossRef]
- Lemogne, C.; Buffel du Vaure, C.; Hoertel, N.; Catu-Pinault, A.; Limosin, F.; Ghasarossian, C.; Le Jeunne, C.; Jaury, P. Balint groups and narrative medicine compared to a control condition in promoting students’ empathy. BMC Med. Educ. 2020, 20, 412. [Google Scholar] [CrossRef]
- Chen, H.; Liu, C.; Cao, X.; Hong, B.; Huang, D.H.; Liu, C.Y.; Chiou, W.K. Effects of Loving-Kindness Meditation on Doctors’ Mindfulness, Empathy, and Communication Skills. Int. J. Environ. Res. Public Health 2021, 18, 4033. [Google Scholar] [CrossRef]
- Humphris, G.M.; Kaney, S. The Liverpool Brief Assessment System for Communication Skills in the Making of Doctors. Adv. Health Sci. Educ. 2001, 6, 69–80. [Google Scholar] [CrossRef]
- Liu, X.; Rohrer, W.; Luo, A.; Fang, Z.; He, T.; Xie, W. Doctor–patient communication skills training in mainland China: A systematic review of the literature. Patient Educ. Couns. 2015, 98, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Grossman, C.E.; Lemay, M.; Kang, L.; Byland, E.; Anderson, A.D.; Nestler, J.E.; Santen, S.A. Improv to improve medical student communication. Clin. Teach. 2021, 18, 301–306. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No. | Studies | Definition Section | Intervention Section | Assessment Section | Measures | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CE | AE | BE | CE | AE | BE | K | A | B | CE | AE | BE | K | A | B | |||
| 1. | Bonvicini et al., 2009 [18] | CE | AE | BE | -- | -- | BE | -- | -- | B | -- | -- | BE | -- | -- | B | GRS [19] ECCS [20] |
| 2. | Bunn and Terpstra 2009 [21] | CE | AE | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | A | -- | JSE-S [22] * |
| 3. | Blatt et al., 2010 [23] | -- | AE | -- | CE | AE | -- | -- | -- | -- | -- | -- | BE | -- | -- | B | Clinical skills examinations [24,25,26] |
| 4. | Tulsky et al., 2011 [27] | -- | -- | -- | -- | -- | BE | -- | -- | B | CE | AE | BE | -- | -- | B | Emotion-handling skills [28,29,30] CARE [31] |
| 5. | Riess et al., 2012 [32] | CE | AE | BE | -- | AE | BE | K | -- | B | CE | AE | BE | K | A | B | CARE [31] JSE-HP [22] * BEES [33] Neurobiology test [32] |
| 6. | Potash et al., 2014 [34] | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | A | -- | JSE-S [35,36] * |
| 7. | Foster et al., 2016 [37] | CE | AE | BE | -- | -- | BE | -- | -- | B | -- | -- | BE | -- | -- | B | ECCS [20] |
| 8. | Buffel du Vaure et al., 2017 [38] | -- | AE | BE | -- | -- | -- | -- | -- | -- | CE | AE | BE | -- | A | B | CARE [31] JSE-S (France version) [39] * |
| 9. | LoSasso et al., 2017 [40] | -- | -- | -- | -- | -- | BE | K | -- | B | CE | AE | -- | -- | A | -- | JSE-HP [22,36] * JSPPPE [41] |
| 10. | Wündrich et al., 2017 [42] | CE | AE | BE | CE | -- | BE | K | -- | B | -- | -- | BE | -- | A | B | SP-rated questionnaire [42] JSE-S (German version) [43] * |
| 11. | Lemogne et al., 2020 [44] | CE | AE | BE | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | A | -- | JSE-S (France version) [39] * |
| 12. | Chen et al., 2021 [45] | CE | AE | -- | -- | -- | -- | -- | -- | -- | CE | AE | BE | -- | A | B | LCSAS [46,47] JSE-HP [22] * |
| 13. | Grossman et al., 2021 [48] | -- | -- | -- | -- | -- | BE | -- | -- | B | -- | -- | BE | -- | -- | B | ECCS [20] |
| Total | 7 | 9 | 6 | 2 | 2 | 7 | 3 | 0 | 7 | 5 | 5 | 9 | 1 | 8 | 9 | ||
| Empathy Dimensions | KAB Aspects | |||||
|---|---|---|---|---|---|---|
| No. | Studies | Overall | Definition vs. Intervention | Intervention vs. Assessment | Definition vs. Assessment | Intervention vs. Assessment |
| 1. | Bonvicini et al., 2009 [18] | 33% | 33% | 100% | 33% | 100% |
| 2. | Bunn and Terpstra 2009 [21] | 0% | 0% | -- | 0% | 0% |
| 3. | Blatt et al., 2010 [23] | 0% | 50% | 0% | 0% | 0% |
| 4. | Tulsky et al., 2011 [27] | 0% | 0% | 33% | 0% | 100% |
| 5. | Riess et al., 2012 [32] | 67% | 67% | 67% | 100% | 67% |
| 6. | Potash et al., 2014 [34] | -- | -- | -- | -- | 0% |
| 7. | Foster et al., 2016 [37] | 33% | 33% | 100% | 33% | 100% |
| 8. | Buffel du Vaure et al., 2017 [38] | 0% | 0% | 0% | 67% | 0% |
| 9. | LoSasso et al., 2017 [40] | 0% | 0% | 0% | 0% | 0% |
| 10. | Wündrich et al., 2017 [42] | 33% | 67% | 50% | 33% | 33% |
| 11. | Lemogne et al., 2020 [44] | 0% | 0% | -- | 0% | 0% |
| 12. | Chen et al., 2021 [45] | 0% | 0% | 0% | 67% | 0% |
| 13. | Grossman et al., 2021 [48] | 0% | 0% | 100% | 0% | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.-L.; Hsieh, T.-L.; Yang, C.-W.; Chen, J.-C.; Ju, Y.-J.; Hsueh, I.-P. Consistency Analysis in Medical Empathy Intervention Research. Int. J. Environ. Res. Public Health 2022, 19, 10904. https://doi.org/10.3390/ijerph191710904
Lee M-L, Hsieh T-L, Yang C-W, Chen J-C, Ju Y-J, Hsueh I-P. Consistency Analysis in Medical Empathy Intervention Research. International Journal of Environmental Research and Public Health. 2022; 19(17):10904. https://doi.org/10.3390/ijerph191710904
Chicago/Turabian StyleLee, Meng-Lin, Ton-Lin Hsieh, Chih-Wei Yang, Jou-Chieh Chen, Yu-Jeng Ju, and I-Ping Hsueh. 2022. "Consistency Analysis in Medical Empathy Intervention Research" International Journal of Environmental Research and Public Health 19, no. 17: 10904. https://doi.org/10.3390/ijerph191710904
APA StyleLee, M.-L., Hsieh, T.-L., Yang, C.-W., Chen, J.-C., Ju, Y.-J., & Hsueh, I.-P. (2022). Consistency Analysis in Medical Empathy Intervention Research. International Journal of Environmental Research and Public Health, 19(17), 10904. https://doi.org/10.3390/ijerph191710904