
The Impact of Foehn Wind on Mental Distress among Patients in a Swiss Psychiatric Hospital

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Brief Symptom Checklist (BSCL)
2.2. Meteorological Data
2.3. Definition of the Foehn Group
2.4. Statistical Methods
- The foehn group analysis was performed (a) comparing the foehn group to the admission group and (b) comparing the foehn group to the discharge group.
- To evaluate the potential short-term associations between Foehn index events and BSCL values, we first aggregated meteorological (Foehn index) data to BSCL data defined for all patients at admission and discharge. Therefore, the data retained the typical time-series structure. This model assumed stationarity in the association and aimed to control for the long-term effects of the Foehn index data on the BSCL data.
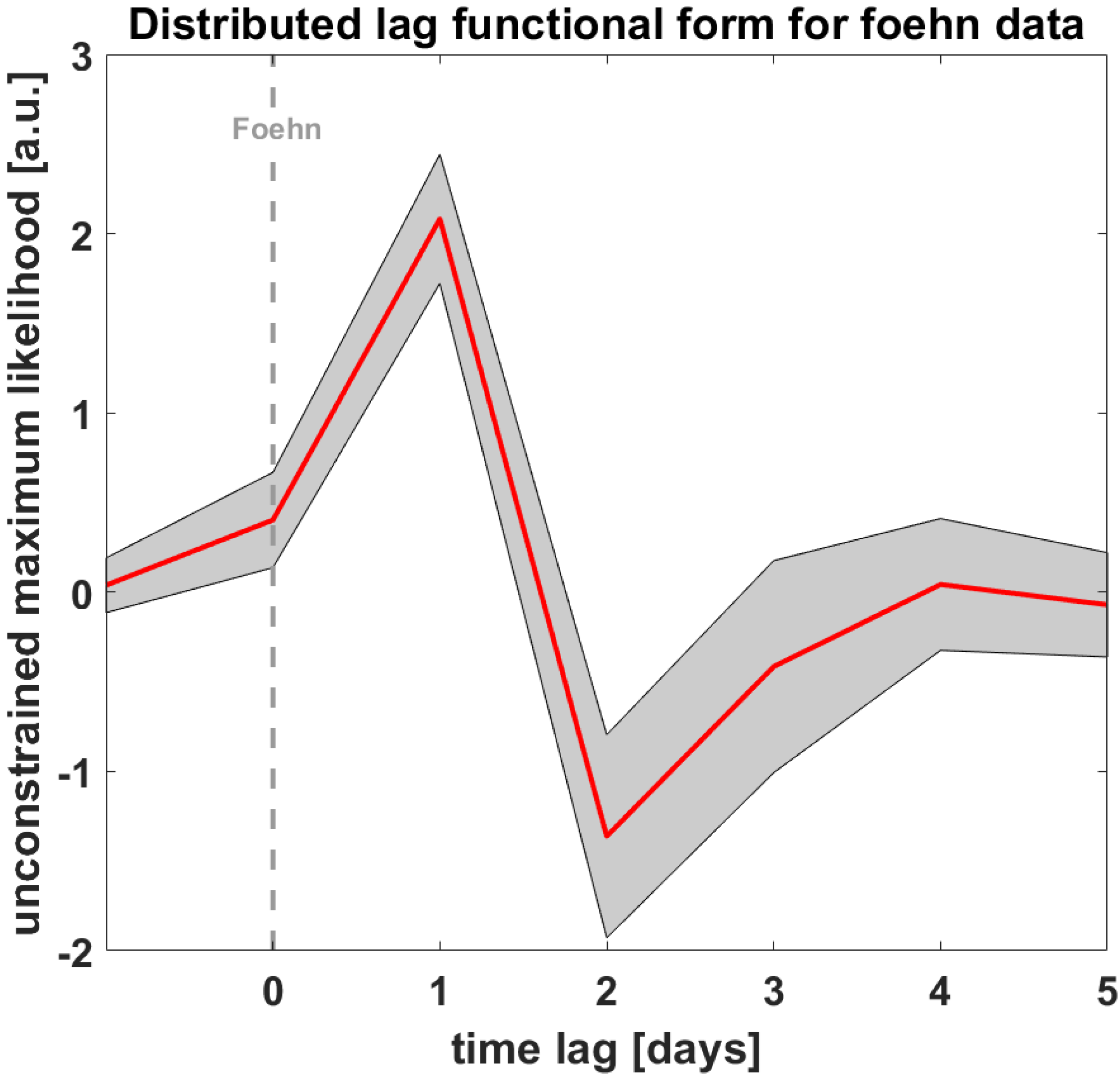
- We chose a distributed lag model (DLM) [54] to assess the potential impact of days characterized as ‘foehn’ on patients’ psychological distress symptoms, according to the BSCL, on hospitalization and discharge dates. The impact of this meteorological variable could be instantaneous and temporally lagged (e.g., Foehn index days over multiple previous days were used as predictors in a regression model for the specific outcome of interest).
- In the DLM, we included lags of the explanatory time-series as independent variables (i.e., Foehn index days). With this flexible framework, we aimed to compare different parametrizations of the exposure–response association and account for lagged dependencies. We used functions modeling the lag–response dimension with a maximum lag of seven days. Therefore, our model consisted of an unconstrained distributed lag linear model (i.e., assuming a linear association) with a maximum lag of seven days.
3. Results
3.1. Description of the Foehn Group and Non-Foehn Group (Total Admission and Total Discharge Sample)
3.2. Distributed Lag Model of foehn
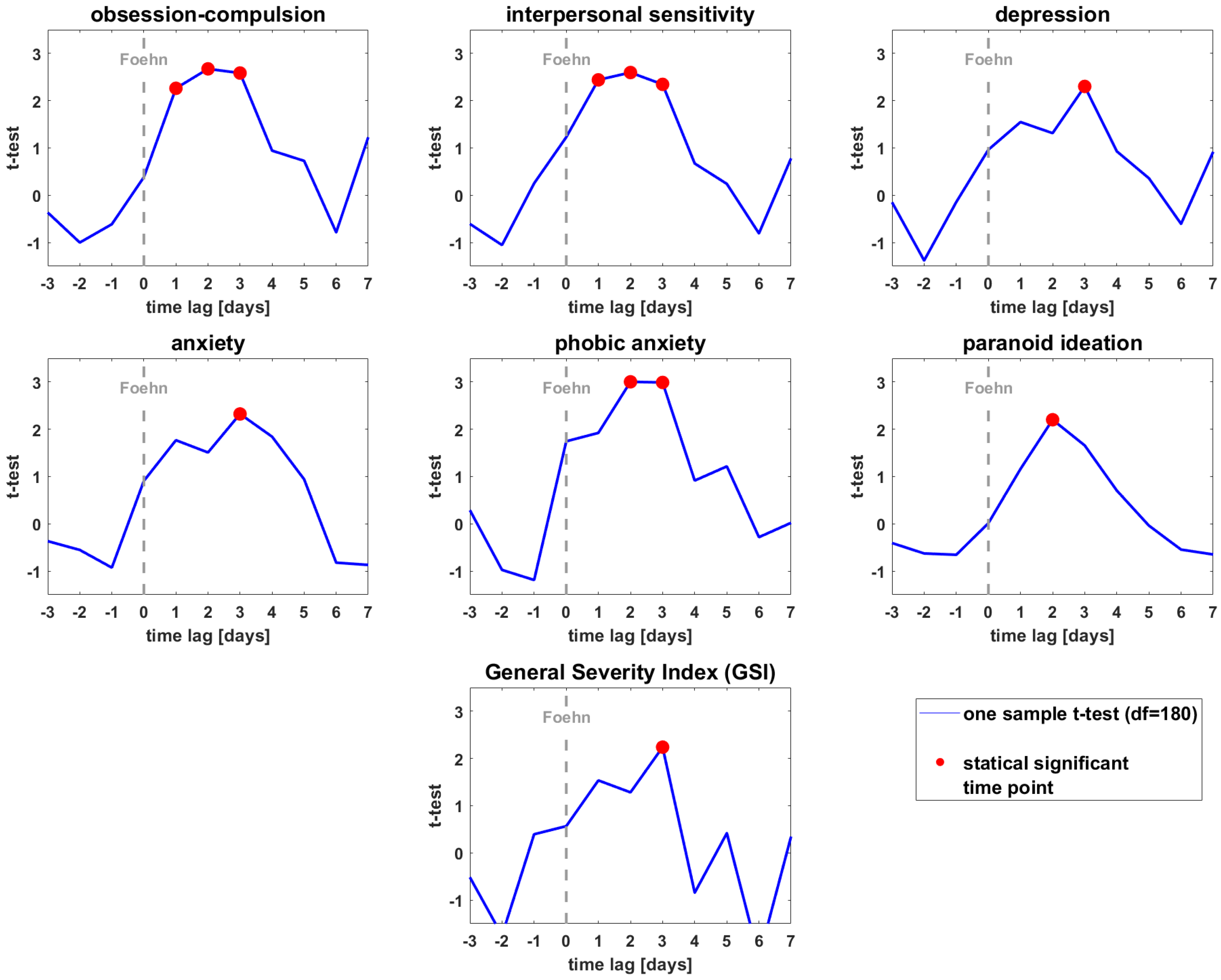
3.3. T-Test of the BSCL Variables vs. Zero
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Intergovernmental Panel on Climate Change. Global Warming of 1.5 °C: An IPCC Special Report on the Impacts of Global Warming of 1.5 °C above Preindustrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; Intergovernmental Panel on Climate Change: Paris, France, 2018.
- Bourque, F.; Willox, A.C. Climate Change: The Next Challenge for Public Mental Health? Int. Rev. Psychiatry 2014, 26, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Lawrance, E.; Thompson, R.; Fontana, G.; Jennings, N. The Impact of Climate Change on Mental Health and Emotional Wellbeing: Current Evidence and Implications for Policy and Practice. 2021. Available online: https://www.imperial.ac.uk/grantham/publications/all-publications/the-impact-of-climate-change-on-mental-health-and-emotional-wellbeing-current-evidence-and-implications-for-policy-and-practice.php (accessed on 29 April 2022).
- Cruz, J.; White, P.C.L.; Bell, A.; Coventry, P.A. Effect of extreme weather events on mental health: A narrative synthesis and meta-analysis for the UK. Int. J. Environ. Res. Public Health 2020, 17, 8581. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.; Berry, H.L.; Bennett, C.M. The importance of humidity in the relationship between heat and population mental health: Evidence from Australia. PLoS ONE 2016, 11, e0164190. [Google Scholar] [CrossRef] [PubMed]
- Frangione, B.; Rodríguez Villamizar, L.A.R.; Lang, J.J.; Colman, I.; Lavigne, E.; Peters, C.; Anisman, H.; Villeneuve, P.J.; Villeneuve, P.J. Short-term changes in meteorological conditions and suicide: A systematic review and meta-analysis. Environ. Res. 2022, 207, 112230. [Google Scholar] [CrossRef] [PubMed]
- Noelke, C.; McGovern, M.; Corsi, D.J.; Jimenez, M.P.; Stern, A.; Wing, I.S.; Berkman, L. Increasing ambient temperature reduces emotional well-being. Environ. Res. 2016, 151, 124–129. [Google Scholar] [CrossRef]
- Thompson, R.; Hornigold, R.; Page, L.; Waite, T. Associations between high ambient temperatures and heat waves with mental health outcomes: A systematic review. Public Health 2018, 161, 171–191. [Google Scholar] [CrossRef]
- Trombley, J.; Chalupka, S.; Anderko, L. Climate Change and Mental Health. Am. J. Nurs. 2017, 117, 44–52. [Google Scholar] [CrossRef]
- Hansen, A.; Bi, P.; Nitschke, M.; Ryan, P.; Pisaniello, D.; Tucker, G. Effect of heat waves on mental health in a temperate Australian city. Environ. Health Perspect 2008, 116, 1369–1375. [Google Scholar] [CrossRef]
- Vaneckova, P.; Bambrick, H. Cause-specific Hospital Admissions on Hot Days in Sydney, Australia. PLoS ONE 2013, 8, e55459. [Google Scholar] [CrossRef]
- Wang, X.; Lavigne, E.; Ouellette-Kuntz, H.; Chen, B.E. Acute impacts of extreme temperature exposure on emergency room admissions related to mental and behavioral disorders in Toronto, Canada. J. Affect. Disord. 2014, 155, 154–161. [Google Scholar] [CrossRef]
- Burke, M.; González, F.; Baylis, P.; Heft-Neal, S.; Baysan, C.; Basu, S.; Hsiang, S. Higher temperatures increase suicide rates in the United States and Mexico. Nat. Clim. Change 2018, 8, 723–729. [Google Scholar] [CrossRef]
- Pervilhac, C.; Schoilew, K.; Znoj, H.; Müller, T.J. Wetter und Suizid [Weather and Suicide: Association between Meteorological Variables and Suicidal Behavior-a Systematic Qualitative Review Article]. Nervenarzt 2020, 91, 227–232. [Google Scholar] [CrossRef]
- Cheng, S.; Plouffe, R.; Nanos, S.M.; Qamar, M.; Fisman, D.N.; Soucy, J.-P.R. The Effect of Average Temperature on Suicide Rates in Five Urban California Counties, 1999–2019: An Ecological Time Series Analysis. BMC Public Health 2021, 21, 974. [Google Scholar] [CrossRef]
- Bär, S.; Bundo, M.; de Schrijver, E.; Müller, T.J.; Vicedo-Cabrera, A.M. Suicides and Ambient Temperature in Switzerland: A Nationwide Time-Series Analysis. Swiss Med. Wkly. 2022, 152, w30115. [Google Scholar] [CrossRef]
- Bundo, M.; de Schrijver, E.; Federspiel, A.; Toreti, A.; Xoplaki, E.; Luterbacher, J.; Franco, O.H.; Müller, T.; Vicedo-Cabrera, A.M.; Müller, T.; et al. Ambient Temperature and Mental Health Hospitalizations in Bern, Switzerland: A 45-Year Time-Series Study. PLoS ONE 2021, 16, e0258302. [Google Scholar] [CrossRef]
- Bouchama, A.; Dehbi, M.; Mohamed, G.; Matthies, F.; Shoukri, M.; Menne, B. Prognostic Factors in Heat Wave Related Deaths: A Meta-Analysis. Arch. Intern. Med. 2007, 167, 2170–2176. [Google Scholar] [CrossRef]
- Hoffmann, M.S.; Oliveira, L.M.; Lobato, M.I.R.; Belmonte-de-Abreu, P. Heat stroke during long-term clozapine treatment: Should we be concerned about hot weather? Trends Psychiatry Psychother. 2016, 38, 56–59. [Google Scholar] [CrossRef]
- Mann, S.C.; Boger, W.P. Psychotropic drugs, summer heat and humidity, and hyperpyrexia: A danger restored. Am. J. Psychiatry 1978, 135, 1097–1100. [Google Scholar] [CrossRef]
- Martin-Latry, K.; Goumy, M.P.; Latry, P.; Gabinski, C.; Bégaud, B.; Faure, I.; Verdoux, H. Psychotropic drug use and risk of heatedRelated hospitalization. Eur. Psychiatry 2007, 22, 335–338. [Google Scholar] [CrossRef]
- Stöllberger, C.; Lutz, W.; Finsterer, J. Heat-rRelated side-effects of neurological and non-neurological medication may increase heatwave fatalities. Eur. J. Neurol. 2009, 16, 879–882. [Google Scholar] [CrossRef]
- Charlson, F.; Ali, S.; Benmarhnia, T.; Pearl, M.; Massazza, A.; Augustinavicius, J.; Scott, J.G. Climate change and mental health: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 4486. [Google Scholar] [CrossRef]
- WMO. International Meteorological Vocabulary; WMO: Geneva, Switzerland, 1966. [Google Scholar]
- Greve, F.; Kanz, K.-G.; Zyskowski, M.; von Matthey, F.; Biberthaler, P.; Muthers, S.; Huber-Wagner, S. Influence of Foehn Winds on the Incidence of Severe Injuries in Southern Bavaria: An Analysis of the Trauma Register DGU®. BMC Musculoskelet. Disord. 2020, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Richner, H.; Hächler, P. Understanding and forecasting alpine foehn. Ecol. In Springer Atmospheric Sciences; Springer: Berlin/Heidelberg, Germany, 2013; pp. 219–260. [Google Scholar] [CrossRef]
- Amiel, M. Geography of Health. MD 1963, 7, 109–114. [Google Scholar]
- Berg, H. Die Wirkung des Föhns auf den menschlichen Organismus. Geofisica Pura Appl. 1950, 17, 104–111. [Google Scholar] [CrossRef]
- Fletcher, R.J. “Föhn illness” and Human Biometeorology in the Chinook Area of Canada. Int. J. Biometeorol. 1988, 32, 168–175. [Google Scholar] [CrossRef]
- Kals, W.Y. Your Health, Our Moods, and the Weather; Doubleday Publishing: New York, NY, USA, 1982; Volume 1. [Google Scholar]
- Koszewska, I.; Walawender, E.; Baran, A.; Zieliński, J.; Ustrnul, Z. Foehn Wind as a Seasonal Suicide Risk Factor in a Mountain Region. Psychiatr. Psychol. Klin. 2019, 19, 48–53. [Google Scholar] [CrossRef]
- Koszewska, I.; Walawender, E.; Baran, A.; Zieliński, J.; Ustrnul, Z. The influence of foehn winds (Halny) on the occurrence of suicide in the Tatra Mountains, 1999–2014. Eur. Psychiatry 2016, 33 (Suppl. S1), S597. [Google Scholar] [CrossRef]
- Lickiewicz, J.; Piotrowicz, K.; Hughes, P.P.; Makara-Studzińska, M. Weather and Aggressive Behavior among Patients in Psychiatric Hospitals-An Exploratory Study. Int. J. Environ. Res. Public Health 2020, 17, 9121. [Google Scholar] [CrossRef]
- Rosen, S. Weathering. How the Atmosphere Conditions Your Body, Your Mind, Your Moods, and Your Health; M. Evans & Company: New York, NY, USA, 1979. [Google Scholar]
- Field, T.S.; Hill, M.D. Weather, Chinook, and stroke occurrence. Stroke 2002, 33, 1751–1757. [Google Scholar] [CrossRef]
- Maciejczak, A.; Guzik, A.; Wolan-Nieroda, A.; Wójcik, M.; Pop, T. Impact of Foehn Wind and Related Environmental Variables on the Incidence of Cardiac Events. Int. J. Environ. Res. Public Health 2020, 17, 2638. [Google Scholar] [CrossRef] [Green Version]
- Ngan, S.; Toth, C. Influence of Chinook winds and other weather patterns on neuropathic pain. Pain Med. 2011, 12, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Bundo, M.; de Schrijver, E.; Federspiel, A.; Luterbacher, J.; Franco, O.; Müller, T.; Vicedo-Cabrera, A. Impact of Foehn Winds on Mental Health Hospitalizations in Bern, Switzerland: A 35-Year Time-Series Study. ISEE Conf. Abstr. 2020, 2020. [Google Scholar] [CrossRef]
- Rehm, J.; Shield, K.D. Global burden of disease and the impact of mental and addictive disorders. Curr. Psychiatry Rep. 2019, 21, 10. [Google Scholar] [CrossRef]
- Bundesamt für Umwelt BAFU; Bericht des Bundesrates. Umwelt Schweiz 2018. 2018. Available online: https://www.bafu.admin.ch/bafu/de/home/zustand/publikationen-zum-umweltzustand/umwelt-schweiz-2018.html (accessed on 25 May 2022).
- Coverdale, J.; Balon, R.; Beresin, E.V.; Brenner, A.M.; Guerrero, A.P.S.; Louie, A.K.; Roberts, L.W. Climate Change: A Call to Action for the Psychiatric Profession. Acad. Psychiatry 2018, 42, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, S.B.; Dawson, R.J.; Kilsby, C.; Lewis, E.; Ford, A. Future heat wWaves, droughts, and floods in 571 European cities. Environ. Res. Lett. 2018, 13, 034009. [Google Scholar] [CrossRef]
- Nie, H.; Qin, T.; Yang, H.; Chen, J.; He, S.; Lv, Z.; Shen, Z. Trends Analysis of Temperature and Precipitation Extreme during Winter Wheat Growth Period in the Major Winter Wheat Planting Area of China. Atmosphere 2019, 10, 240. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Capstick, S.; et al. The 2019 report of the Lancet Countdown on Health and Climate Change: Ensuring that the health of a child born today is not defined by a changing climate. Lancet 2019, 394, 1836–1878. [Google Scholar] [CrossRef]
- Franke, G.H. SCL-90®-S. Symptom-Checklist-90®-Standard–Manual; Hogrefe: Göttingen, Germany, 2014. [Google Scholar]
- Derogatis, L. Brief Symptom Inventory (Baltimore, Clinical Psychometric Research). Psychopathology 1975, 27, 14–18. [Google Scholar]
- Franke, G.H. Symptom-Checklist-90®-Standard. In Diagnostische Verfahren in der Psychotherapie; Hogrefe Verlag Gmbh & Co.: Göttingen, Germany, 2016. [Google Scholar]
- Franke, G.H. Brief Symptom Inventory, German Version; Beltz: Göttingen, Germany, 2000. [Google Scholar]
- Hautzinger, M.; Bailer, M.; Worall, H.; Keller, F. BDI Beck-Depressions-Inventory; Pearson Assessment and Information GmbH: Frankfurt, Germany, 1995. [Google Scholar]
- Beck, A.; Steer, R. BHS. Beck Hopelessness Scale. Beck-Hoffnungslosigkeits-Skala. In Deutsche Fassung; Pearson: Frankfurt, Germany, 2015. [Google Scholar]
- MeteoSwiss. Available online: www.meteoswiss.ch (accessed on 6 May 2022).
- Köppen, W. Die Wärmezonen der Erde, nach der Dauer der heissen, gemässigten und kalten Zeit und nach der Wirkung der Wärme auf die organische Welt betrachtet. Meteorol. Z 1884, 1, 5–226. [Google Scholar]
- Köppen, W. Das Geographische System der Klimate: Mit 14 Textfiguren; Borntraeger: Berlin, Germany, 1936. [Google Scholar]
- Granger, C.W.J.; Newbold, P. Spurious Regressions in Econometrics. J. Econ. 1974, 2, 111–120. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2013. [Google Scholar]
- Chong, T.W.; Castle, D.J. Layer upon layer: Thermoregulation in schizophrenia. Schizophr. Res. 2004, 69, 149–157. [Google Scholar] [CrossRef]
- Heo, S.; Lee, W.; Bell, M.L. Suicide and associations with air pollution and ambient temperature: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 7699. [Google Scholar] [CrossRef] [PubMed]
- Lõhmus, M. Possible Biological Mechanisms Linking Mental Health and Heat-A Contemplative Review. Int. J. Environ. Res. Public Health 2018, 15, 1515. [Google Scholar] [CrossRef]
- Martinez, M.; Devenport, L.; Saussy, J.; Martinez, J. Drug-associated heat stroke. South. Med. J. 2002, 95, 799–802. [Google Scholar] [CrossRef]
- Gutiérrez-Rojas, L.; Porras-Segovia, A.; Dunne, H.; Andrade-González, N.; Cervilla, J.A. Prevalence and correlates of major depressive disorder: A systematic Systematic review. Braz. J. Psychiatry 2020, 42, 657–672. [Google Scholar] [CrossRef]
- Scott, K.M.; de Jonge, P.; Stein, D.J.; Kessler, R.C. Mental Disorders around the World: Facts and Figures from the WHO World Mental Health Surveys; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; Salazar de Pablo, G.; Il Shin, J.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: A large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 2022, 27, 281–295. [Google Scholar] [CrossRef]
- Charlson, F.; Ali, S.; Augustinavicius, J.; Benmarhnia, T.; Birch, S.; Clayton, S.; Fielding, K.; Jones, L.; Juma, D.; Snider, L.; et al. Global priorities for climate change and mental health research. Environ. Int. 2022, 158, 106984. [Google Scholar] [CrossRef]
- Kenny, G.P.; Yardley, J.; Brown, C.; Sigal, R.J.; Jay, O. Heat Stress in Older Individuals and Patients with Common Chronic Diseases. CMAJ 2010, 182, 1053–1060. [Google Scholar] [CrossRef]
- Mills, M.A.; Edmondson, D.; Park, C.L. Trauma and stress response among hurricane Katrina evacuees. Am. J. Public Health 2007, 97 (Suppl. S1), S116–S123. [Google Scholar] [CrossRef]
- Obrien, L.V.; Berry, H.L.; Coleman, C.; Hanigan, I.C. Drought as a mental health exposure. Environ. Res. 2014, 131, 181–187. [Google Scholar] [CrossRef]
- Perceval, M.; Kõlves, K.; Ross, V.; Reddy, P.; De Leo, D. Environmental factors and suicide among Australian farmers: A qualitative study. Arch. Environ. Occup. Health 2019, 74, 279–286. [Google Scholar] [CrossRef]
- Ruskin, J.; Rasul, R.; Schneider, S.; Bevilacqua, K.; Taioli, E.; Schwartz, R.M. Lack of access to medical care during hurricane sandy and mental health symptoms. Prev. Med. Rep. 2018, 10, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Sirey, J.A.; Berman, J.; Halkett, A.; Giunta, N.; Kerrigan, J.; Raeifar, E.; Artis, A.; Banerjee, S.; Raue, P.J.; Banerjee, S.; et al. Storm impact and depression among older adults living in hurricane sandy-affected areas. Disaster Med. Public Health Prep. 2017, 11, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Picou, J.S. Hudson, Hurricane Katrina, Mental Health: A Research Note on Mississippi Gulf Coast Residents. Sociol. Inq. 2010, 80, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.; Paunovic, K. WHO Health Organization Environmental Noise Guidelines for the European Region: A systematicSystematic review on environmental noise and quality of life, well-being, and mental health. Int. J. Environ. Res. Public Health 2018, 15, 2400. [Google Scholar] [CrossRef] [PubMed]
- Hegewald, J.; Schubert, M.; Freiberg, A.; Romero Starke, K.; Augustin, F.; Riedel-Heller, S.G.; Zeeb, H.; Seidler, A.; Seidler, A. Traffic noise and mental health: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 6175. [Google Scholar] [CrossRef]
- Monazzam Esmaielpour, M.R.; Zakerian, S.A.; Abbasi, M.; Balochkhaneh, F.; Kordmiri, S.H. Investigating the effect of noise exposure on mental disorders and the work ability index among industrial workers. Noise Vib. Worldw. 2022, 53, 3–11. [Google Scholar] [CrossRef]
- Zare Sakhvidi, F.; Zare Sakhvidi, M.J.; Mehrparvar, A.H.; Dzhambov, A.M. Environmental Noise Exposure and Neurodevelopmental and Mental Health Problems in Children: A Systematic Review. Curr. Environ. Health Rep. 2018, 5, 365–374. [Google Scholar] [CrossRef]
- Brink, M.; Schäffer, B.; Vienneau, D.; Foraster, M.; Pieren, R.; Eze, I.C.; Cajochen, C.; Probst-Hensch, N.; Röösli, M.; Wunderli, J.M.; et al. A Survey on Exposure-Response Relationships for Road, Rail, and Aircraft Noise Annoyance: Differences between Continuous and Intermittent Noise. Environ. Int. 2019, 125, 277–290. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| ICD Code | Frequency | Percent |
|---|---|---|
| F32.1 | 56 | 30.8% |
| F33.1 | 40 | 22% |
| F10.2 | 19 | 10.4% |
| F33.2 | 13 | 7.1% |
| ICD Code | Frequency | Percent |
|---|---|---|
| F33.1 | 2001 | 19.1% |
| F32.1 | 1792 | 17.1% |
| F33.2 | 1210 | 11.6% |
| F10.2 | 1079 | 10.4% |
| ICD Code | Frequency | Percent |
|---|---|---|
| F33.1 | 1996 | 19.2% |
| F32.1 | 1792 | 17.1% |
| F33.2 | 1210 | 11.6% |
| F10.2 | 1087 | 10.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikutta, C.A.; Pervilhac, C.; Znoj, H.; Federspiel, A.; Müller, T.J. The Impact of Foehn Wind on Mental Distress among Patients in a Swiss Psychiatric Hospital. Int. J. Environ. Res. Public Health 2022, 19, 10831. https://doi.org/10.3390/ijerph191710831
Mikutta CA, Pervilhac C, Znoj H, Federspiel A, Müller TJ. The Impact of Foehn Wind on Mental Distress among Patients in a Swiss Psychiatric Hospital. International Journal of Environmental Research and Public Health. 2022; 19(17):10831. https://doi.org/10.3390/ijerph191710831
Chicago/Turabian StyleMikutta, Christian A., Charlotte Pervilhac, Hansjörg Znoj, Andrea Federspiel, and Thomas J. Müller. 2022. "The Impact of Foehn Wind on Mental Distress among Patients in a Swiss Psychiatric Hospital" International Journal of Environmental Research and Public Health 19, no. 17: 10831. https://doi.org/10.3390/ijerph191710831
APA StyleMikutta, C. A., Pervilhac, C., Znoj, H., Federspiel, A., & Müller, T. J. (2022). The Impact of Foehn Wind on Mental Distress among Patients in a Swiss Psychiatric Hospital. International Journal of Environmental Research and Public Health, 19(17), 10831. https://doi.org/10.3390/ijerph191710831