
Effect of Short- to Long-Term Exposure to Ambient Particulate Matter on Cognitive Function in a Cohort of Middle-Aged and Older Adults: KoGES



Abstract
:1. Introduction
2. Materials and Methods
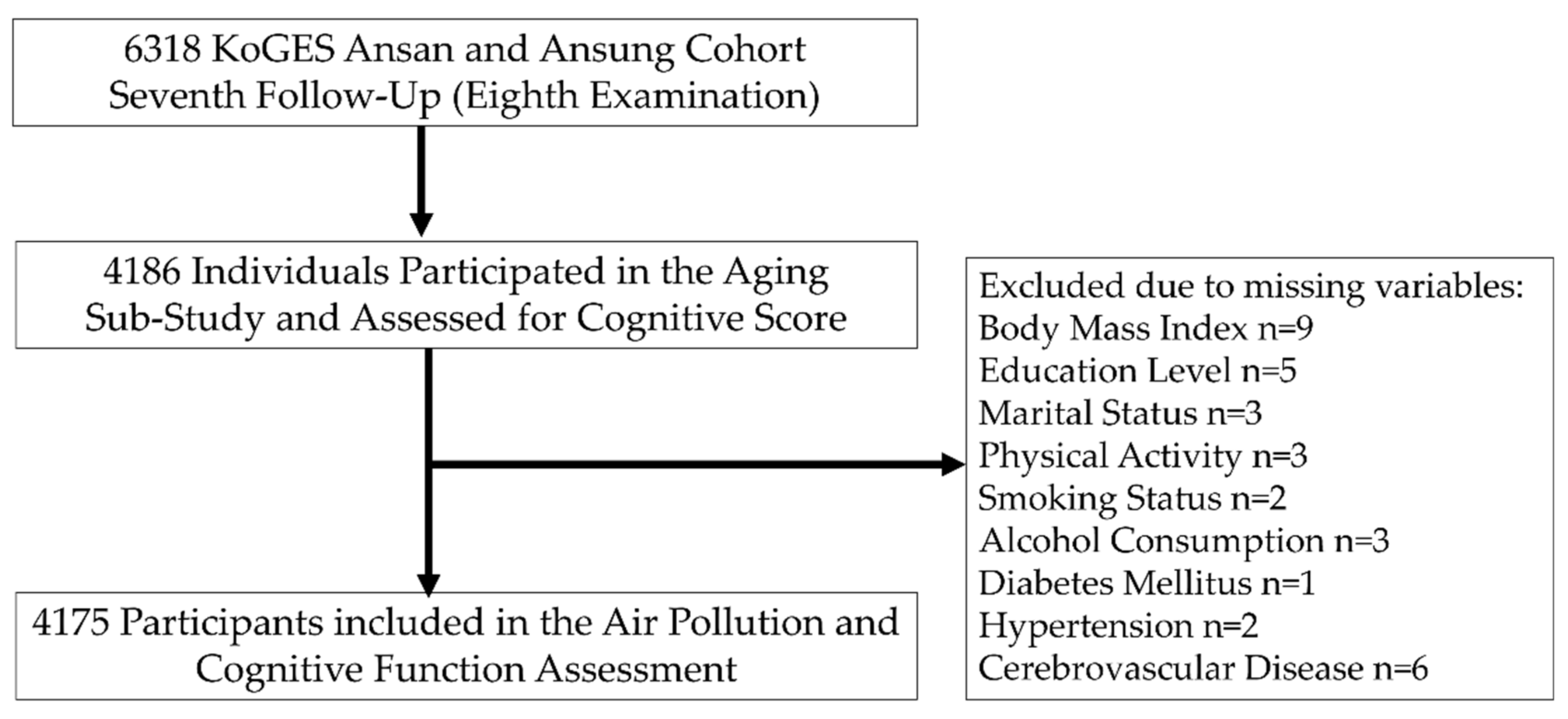
2.1. Study Population
2.2. Cognitive Function Assessment
2.3. Ambient Particulate Matters
- Short-term air pollution exposure data included PM2.5 and PM10 exposures on the date of the visit (day 1), and the average of 2-, 3-, 4-, 5-, 6-, 7-, 8-, 9-, 10-, 11-, 12-, 13-, and 14-day counting from the date of each participant’s study visit;
- Medium-term air pollution exposure data included average PM2.5 and PM10 exposure levels over 1, 3, and 6 months;
- Long-term air pollution exposure data included average PM2.5 and PM10 exposures over 1, 2, and 3 years.
2.4. Potential Covariates
2.5. Statistical Analysis
3. Results
Study Sample Characteristics
4. Discussion
4.1. Principal Findings
4.2. In the Context of the Current Literature
4.3. Potential Physiological Mechanisms
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feng, S.; Gao, D.; Liao, F.; Zhou, F.; Wang, X. The health effects of ambient PM2. 5 and potential mechanisms. Ecotoxicol. Environ. Saf. 2016, 128, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R. Estimates and 25-year trends of the Global Burden of Disease attributable to ambient air pollution: An analysis of data from the global burden of diseases study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- World Health Organization. Ambient (Outdoor) Air Pollution. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 26 July 2022).
- Du, Y.; Xu, X.; Chu, M.; Guo, Y.; Wang, J. Air particulate matter and cardiovascular disease: The epidemiological, biomedical and clinical evidence. J. Thorac. Dis. 2016, 8, E8. [Google Scholar]
- Bates, J.T.; Fang, T.; Verma, V.; Zeng, L.; Weber, R.J.; Tolbert, P.E.; Abrams, J.Y.; Sarnat, S.E.; Klein, M.; Mulholland, J.A. Review of acellular assays of ambient particulate matter oxidative potential: Methods and relationships with composition, sources and health effects. Environ. Sci. Technol. 2019, 53, 4003–4019. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Report On The Environment—Particulate Matter Emissions. Available online: https://www.epa.gov/roe/ (accessed on 13 April 2022).
- Qin, S.; Li, B.; Wang, X.; Huang, H.; Zeng, M.; Xiao, F.; Xu, X. Metal element detection and carcinogenicity risk assessment of PM2. 5 samples. Environ. Toxicol. Chem. 2020, 39, 1273–1276. [Google Scholar] [CrossRef]
- Li, Z.; Wen, Q.; Zhang, R. Sources, health effects and control strategies of indoor fine particulate matter (PM2.5): A review. Sci. Total Environ. 2017, 586, 610–622. [Google Scholar] [CrossRef] [PubMed]
- Air Korea. Air Pollutants. Available online: https://www.airkorea.or.kr/web/airmatter?Pmenu_No=130 (accessed on 13 April 2022).
- Almetwally, A.A.; Bin-Jumah, M.; Allam, A.A. Ambient air pollution and its influence on human health and welfare: An overview. Environ. Sci. Pollut. Res. 2020, 27, 24815–24830. [Google Scholar] [CrossRef] [PubMed]
- Major Population Indicators (Ratio, Population Growth Rate, Population Structure, Dependency Ratio, Etc.)/NationwideFuture Population Estimation, National Statistical Office (Reference: 02-2012-9114, 042-481-2261). Available online: https://kosis.kr/statHtml/statHtml.do?mode=tab&orgid=101&tblid=DT_1BPA002 (accessed on 13 April 2021).
- Peeples, L. How air pollution threatens brain health. Proc. Natl. Acad. Sci. USA 2020, 117, 13856–13860. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.-G.; Group, K. Cohort profile: The Korean genome and epidemiology study (koges) consortium. Int. J. Epidemiol. 2017, 46, E20. [Google Scholar] [CrossRef]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 2016, CD011145. [Google Scholar] [CrossRef]
- Kang, Y.; Na, D.-L.; Hahn, S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Kim, H.; Noh, J.; Noh, Y.; Oh, S.S.; Koh, S.-B.; Kim, C. Gender difference in the effects of outdoor air pollution on cognitive function among elderly in Korea. Front. Public Health 2019, 7, 375. [Google Scholar] [CrossRef]
- Hwang, M.-J.; Sung, J.; Yoon, M.; Kim, J.-H.; Yun, H.-Y.; Choi, D.-R.; Koo, Y.-S.; Oh, K.; Yun, S.; Cheong, H.-K. Establishment of the Korea National Health and Nutrition Examination Survey air pollution study dataset for the researchers on the health impact of ambient air pollution. Epidemiol. Health 2021, 43, e2021015. [Google Scholar] [CrossRef] [PubMed]
- Koo, Y.; Choi, D.; Yun, H.; Yoon, G.; Lee, J. A development of PM concentration reanalysis method using cmaq with surface data assimilation and MAIAC AOD in Korea. J. Korean Soc. Atmos. Environ. 2020, 36, 558–573. [Google Scholar] [CrossRef]
- Tian, X.; Fang, Z.; Liu, W. decreased humidity improves cognitive performance at extreme high indoor temperature. Indoor Air 2021, 31, 608–627. [Google Scholar] [CrossRef]
- Zhou, X.; Cao, Z.; Ma, Y.; Wang, L.; Wu, R.; Wang, W. Concentrations, correlations and chemical species of PM2.5/PM10 based on published data in China: Potential implications for the revised particulate standard. Chemosphere 2016, 144, 518–526. [Google Scholar] [CrossRef]
- Cai, W. Fitting generalized additive models with the gam procedure. In Sas 9.2, Sas Global Forum; Sas Institute Inc.: Cary, NC, USA, 2008. [Google Scholar]
- Weuve, J.; Bennett, E.E.; Ranker, L.; Gianattasio, K.Z.; Pedde, M.; Adar, S.D.; Yanosky, J.D.; Power, M.C. Exposure to air pollution in relation to risk of dementia and related outcomes: An updated systematic review of the epidemiological literature. Environ. Health Perspect. 2021, 129, 96001. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Han, J.; Kim, S.H.; Suk, H.W.; Park, J.E.; Lee, D.Y. Impact of Long-Term Exposure to Air Pollution on Cognitive Decline in Older Adults Without Dementia. J. Alzheimer’s Dis. 2022, 86, 553–563. [Google Scholar] [CrossRef]
- Gao, X.; Coull, B.; Lin, X.; Vokonas, P.; Spiro, A.; Hou, L.; Schwartz, J.; Baccarelli, A.A. Short-term air pollution, cognitive performance and nonsteroidal anti-inflammatory drug use in the Veterans Affairs Normative Aging Study. Nat. Aging 2021, 1, 430–437. [Google Scholar] [CrossRef]
- Chen, M.-C.; Wang, C.-F.; Lai, B.-C.; Hsieh, S.-W.; Chen, S.-C.; Hung, C.-H.; Kuo, C.-H. Air pollution is associated with poor cognitive function in taiwanese adults. Int. J. Environ. Res. Public Health 2021, 18, 316. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, T.; Lv, Y.; Kraus, V.B.; Zhang, Y.; Mao, C.; Yin, Z.; Shi, W.; Zhou, J.; Zheng, T. Fine particulate matter and poor cognitive function among Chinese older adults: Evidence from a community-based, 12-year prospective cohort study. Environ. Health Perspect. 2020, 128, 67013. [Google Scholar] [CrossRef]
- Maji, K.J.; Dikshit, A.K.; Deshpande, A. Disability-adjusted life years and economic cost assessment of the health effects related to PM2.5 and PM10 pollution in mumbai and delhi, in india from 1991 to 2015. Environ. Sci. Pollut. Res. 2017, 24, 4709–4730. [Google Scholar] [CrossRef]
- Mehmood, T.; Tianle, Z.; Ahmad, I.; Li, X.; Shen, F.; Akram, W.; Dong, L. Variations of PM2.5, PM10 Mass Concentration and Health Assessment in Islamabad, Pakistan. Iop Conf. Ser. Earth Environ. Sci. 2018, 133, 012031. [Google Scholar]
- Celo, V.; Yassine, M.M.; Dabek-Zlotorzynska, E. Insights into Elemental Composition and Sources of Fine and Coarse Particulate Matter in Dense Traffic Areas in Toronto and Vancouver, Canada. Toxics 2021, 9, 264. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. Particulate Matter (PM2.5) Trends. Available online: https://www.epa.gov/air-trends/particulate-matter-pm25-trends (accessed on 13 April 2022).
- Duchesne, J.; Gutierrez, L.-A.; Carrière, I.; Mura, T.; Chen, J.; Vienneau, D.; de Hoogh, K.; Helmer, C.; Jacquemin, B.; Berr, C. Exposure to ambient air pollution and cognitive decline: Results of the prospective Three-City cohort study. Environ. Int. 2022, 161, 107118. [Google Scholar] [CrossRef]
- Air Korea. Atmospheric Environment Standards. Available online: https://www.airkorea.or.kr/web/contents/contentview/?Pmenu_No=133&cntnts_No=7 (accessed on 13 April 2022).
- World Health Organization. Who Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide And Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Matthews, F.; Marioni, R.; Brayne, C. Examining the influence of gender, education, social class and birth cohort on MMSE tracking over time: A population-based prospective cohort study. BMC Geriatr. 2012, 12, 45. [Google Scholar] [CrossRef] [PubMed]
- Lövdén, M.; Fratiglioni, L.; Glymour, M.M.; Lindenberger, U.; Tucker-Drob, E.M. Education and cognitive functioning across the life span. Psychol. Sci. Public Interest 2020, 21, 6–41. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Kim, G.; Park, S. Widowhood status as a risk factor for cognitive decline among older adults. Am. J. Geriatr. Psychiatry 2018, 26, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.-R.; Wei, R.; Cheng, B.-J.; Wang, A.-J.; Li, X.-D.; Li, H.-B.; Sun, L.; Du, J.; Sheng, J.; Liu, K.-Y. The association of marital status with cognitive function and the role of gender in Chinese community-dwelling older adults: A cross-sectional study. Aging Clin. Exp. Res. 2021, 33, 2273–2281. [Google Scholar] [CrossRef]
- Barnes, J.N. Exercise, cognitive function, and aging. Adv. Physiol. Educ. 2015, 39, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Cournot, M.; Marquie, J.; Ansiau, D.; Martinaud, C.; Fonds, H.; Ferrieres, J.; Ruidavets, J. Relation between body mass index and cognitive function in healthy middle-aged men and women. Neurology 2006, 67, 1208–1214. [Google Scholar] [CrossRef]
- Mons, U.; Schöttker, B.; Müller, H.; Kliegel, M.; Brenner, H. History of lifetime smoking, smoking cessation and cognitive function in the elderly population. Eur. J. Epidemiol. 2013, 28, 823–831. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, D.Y.; Lee, B.C.; Jung, M.H.; Kim, H.; Choi, Y.S.; Choi, I.-G. Alcohol and cognition in the elderly: A review. Psychiatry Investig. 2012, 9, 8–16. [Google Scholar] [CrossRef]
- Mansur, R.B.; Lee, Y.; Zhou, A.J.; Carmona, N.E.; Cha, D.S.; Rosenblat, J.D.; Bruins, R.; Kakar, R.; Rasgon, N.L.; Lovshin, J.A. Determinants of cognitive function in individuals with type 2 diabetes mellitus: A meta-analysis. Ann. Clin. Psychiatry 2018, 30, 38–50. [Google Scholar]
- Birns, J.; Kalra, L. Cognitive function and hypertension. J. Hum. Hypertens. 2009, 23, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Kalaria, R.N. Cerebrovascular disease and mechanisms of cognitive impairment: Evidence from clinicopathological studies in humans. Stroke 2012, 43, 2526–2534. [Google Scholar] [CrossRef] [PubMed]
- Asher, A.; Myers, J.S. The effect of cancer treatment on cognitive function. Clin. Adv. Hematol. Oncol. 2015, 13, 441–450. [Google Scholar] [PubMed]
- Miller, M.R.; Newby, D.E. Air pollution and cardiovascular disease: Car sick. Cardiovasc. Res. 2020, 116, 279–294. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimer’s Dement. 2015, 11, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Elbaz, A.; Dugravot, A.; Head, J.; Shipley, M.; Hagger-Johnson, G.; Kivimaki, M.; Singh-Manoux, A. Impact of smoking on cognitive decline in early old age: The Whitehall II cohort study. Arch. Gen. Psychiatry 2012, 69, 627–635. [Google Scholar] [CrossRef]
- Yao, Y.; Wang, K.; Xiang, H. association between cognitive function and ambient particulate matters in middle-aged and elderly chinese adults: Evidence from the China Health and Retirement Longitudinal Study (CHARLS). Sci. Total Environ. 2022, 828, 154297. [Google Scholar] [CrossRef]
- Zalakeviciute, R.; López-Villada, J.; Rybarczyk, Y. Contrasted effects of relative humidity and precipitation on urban PM2.5 pollution in high elevation urban areas. Sustainability 2018, 10, 2064. [Google Scholar] [CrossRef]
- Li, Y.; Chen, Q.; Zhao, H.; Wang, L.; Tao, R. Variations in PM10, PM2.5 and PM1.0 in an urban area of the Sichuan Basin and their relation to meteorological factors. Atmosphere 2015, 6, 150–163. [Google Scholar] [CrossRef]
- Shou, Y.; Huang, Y.; Zhu, X.; Liu, C.; Hu, Y.; Wang, H. A Review of the possible associations between ambient PM2.5 exposures and the development of alzheimer’s disease. Ecotoxicol. Environ. Saf. 2019, 174, 344–352. [Google Scholar] [CrossRef] [PubMed]
- California Air Resources Board. Inhalable Particulate Matter and Health (PM2.5 and PM10). Available online: https://ww2.arb.ca.gov/resources/inhalable-particulate-matter-and-health#:~:text=on%20particle%20size.-,pm2.tissue%20damage%2c%20and%20lung%20inflammation (accessed on 13 April 2022).
- Calderón-Garcidueñas, L.; Ayala, A. Air Pollution, Ultrafine Particles, and Your brain: Are Combustion Nanoparticle Emissions and Engineered Nanoparticles Causing Preventable Fatal Neurodegenerative Diseases and Common Neuropsychiatric Outcomes? Environ. Sci. Technol. 2022, 56, 6847–6856. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.-S.; Ryu, M.H.; Carlsten, C. Ultrafine particles: Unique physicochemical properties relevant to health and disease. Exp. Mol. Med. 2020, 52, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Querol, X.; Alastuey, A.; Rodriguez, S.; Plana, F.; Mantilla, E.; Ruiz, C.R. Monitoring of PM10 and PM2.5 around primary particulate anthropogenic emission sources. Atmos. Environ. 2001, 35, 845–858. [Google Scholar] [CrossRef]
- Morawska, L.; Zhang, J.J. Combustion sources of particles. 1. Health relevance and source signatures. Chemosphere 2002, 49, 1045–1058. [Google Scholar] [CrossRef]
- Oudin, A.; Forsberg, B.; Adolfsson, A.N.; Lind, N.; Modig, L.; Nordin, M.; Nordin, S.; Adolfsson, R.; Nilsson, L.-G. Traffic-related air pollution and dementia incidence in northern Sweden: A longitudinal study. Environ. Health Perspect. 2016, 124, 306–312. [Google Scholar] [CrossRef]
- Guan, Q.; Liu, Z.; Yang, L.; Luo, H.; Yang, Y.; Zhao, R.; Wang, F. Variation in PM2.5 source over megacities on the ancient Silk Road, northwestern China. J. Clean. Prod. 2019, 208, 897–903. [Google Scholar] [CrossRef]
- Sinharay, R.; Gong, J.; Barratt, B.; Ohman-Strickland, P.; Ernst, S.; Kelly, F.J.; Zhang, J.J.; Collins, P.; Cullinan, P.; Chung, K.F. Respiratory and cardiovascular responses to walking down a traffic-polluted road compared with walking in a traffic-free area in participants aged 60 years and older with chronic lung or heart disease and age-matched healthy controls: A randomised, crossover study. Lancet 2018, 391, 339–349. [Google Scholar]
- Gerlofs-Nijland, M.E.; Bokkers, B.G.; Sachse, H.; Reijnders, J.J.; Gustafsson, M.; Boere, A.J.F.; Fokkens, P.; Leseman, D.L.; Augsburg, K.; Cassee, F.R. Inhalation Toxicity profiles of particulate matter: A comparison between brake wear with other sources of emission. Inhal. Toxicol. 2019, 31, 89–98. [Google Scholar] [CrossRef]
- Han, B.; Xu, J.; Zhang, Y.; Li, P.; Li, K.; Zhang, N.; Han, J.; Gao, S.; Wang, X.; Geng, C. Associations of Exposure to Fine Particulate Matter Mass and Constituents with Systemic Inflammation: A Cross-Sectional Study of Urban Older Adults in China. Environ. Sci. Technol. 2022, 56, 7244–7255. [Google Scholar] [CrossRef]
- Cherbuin, N.; Walsh, E.; Baune, B.; Anstey, K. Oxidative stress, inflammation and risk of neurodegeneration in a population sample. Eur. J. Neurol. 2019, 26, 1347–1354. [Google Scholar] [CrossRef]
- Kermani, M.; Jonidi Jafari, A.; Gholami, M.; Arfaeinia, H.; Shahsavani, A.; Fanaei, F. Characterization, possible sources and health risk assessment of PM2.5-bound Heavy Metals in the most industrial city of iran. J. Environ. Health Sci. Eng. 2021, 19, 151–163. [Google Scholar] [CrossRef]
- Li, F.; Yan, J.; Wei, Y.; Zeng, J.; Wang, X.; Chen, X.; Zhang, C.; Li, W.; Chen, M.; Lü, G. PM2.5-bound heavy metals from the major cities in China: Spatiotemporal distribution, fuzzy exposure assessment and health risk management. J. Clean. Prod. 2021, 286, 124967. [Google Scholar] [CrossRef]
- Zhao, Z.; Luo, X.-S.; Jing, Y.; Li, H.; Pang, Y.; Wu, L.; Chen, Q.; Jin, L. In Vitro assessments of bioaccessibility and bioavailability of PM2.5 trace metals in respiratory and digestive systems and their oxidative potential. J. Hazard. Mater. 2021, 409, 124638. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Liu, H.; Alattar, M.; Jiang, S.; Han, J.; Ma, Y.; Jiang, C. The preferential accumulation of heavy metals in different tissues following frequent respiratory exposure to PM2.5 in rats. Sci. Rep. 2015, 5, 16936. [Google Scholar] [CrossRef]
- Mold, M.J.; O’Farrell, A.; Morris, B.; Exley, C. Aluminum and tau in neurofibrillary tangles in familial Alzheimer’s disease. J. Alzheimer’s Dis. Rep. 2021, 5, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Fadel, M.; Ledoux, F.; Seigneur, M.; Oikonomou, K.; Sciare, J.; Courcot, D.; Afif, C. Chemical profiles of PM2.5 emitted from various anthropogenic sources of the Eastern Mediterranean: Cooking, wood burning, and diesel generators. Environ. Res. 2022, 211, 113032. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, A. Neurological disorders from ambient (urban) air pollution emphasizing UFPM and PM2.5. Curr. Pollut. Rep. 2016, 2, 203–211. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, Q.; Ma, J.; Zhao, Y. PM2.5 Impairs neurobehavior by oxidative stress and myelin sheaths injury of brain in the rat. Environ. Pollut. 2018, 242, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Jankowska-Kieltyka, M.; Roman, A.; Nalepa, I. The Air We Breathe: Air Pollution as a Prevalent Proinflammatory Stimulus Contributing to Neurodegeneration. Front. Cell. Neurosci. 2021, 15, 647643. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ou, C.; Magana-Arachchi, D.; Vithanage, M.; Vanka, K.S.; Palanisami, T.; Masakorala, K.; Wijesekara, H.; Yan, Y.; Bolan, N. Indoor particulate matter in urban households: Sources, pathways, characteristics, health effects, and exposure mitigation. Int. J. Environ. Res. Public Health 2021, 18, 11055. [Google Scholar] [CrossRef]
- Liu, C.; Zhang, Y. Relations between indoor and outdoor PM2.5 and constituent concentrations. Front. Environ. Sci. Eng. 2019, 13, 5. [Google Scholar] [CrossRef]
- Wang, K.; Chen, F.-E.; Au, W.; Zhao, Z.; Xia, Z.-L. Evaluating the feasibility of a personal particle exposure monitor in outdoor and indoor microenvironments in Shanghai, China. Int. J. Environ. Health Res. 2019, 29, 209–220. [Google Scholar] [CrossRef]
- Onat, B.; Stakeeva, B. Personal exposure of commuters in public transport to PM2. 5 and fine particle counts. Atmos. Pollut. Res. 2013, 4, 329–335. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Mean or N | Standard Deviation or % | |
|---|---|---|---|
| Age (years) | 67.8 | 7.9 | |
| Sex (%) | |||
| Women | 2305 | 55.2 | |
| Men | 1870 | 44.8 | |
| Age Group (%) | |||
| 50–65 years | 1665 | 39.9 | |
| 65–75 years | 1483 | 35.5 | |
| Above 75 years | 1027 | 24.6 | |
| BMI (kg/m2) | 24.5 | 3.3 | |
| BMI Group (%) a | |||
| Underweight | 111 | 2.7 | |
| Normal Weight | 1287 | 30.8 | |
| Overweight | 1069 | 25.6 | |
| Obese | 1708 | 40.9 | |
| Marital Status (%) | |||
| Married | 3293 | 78.9 | |
| Separated or Divorced | 96 | 2.3 | |
| Widowed | 764 | 18.3 | |
| Others (e.g., Single, Living Together) | 22 | 0.5 | |
| Education Level (%) | |||
| Below Elementary School | 879 | 21.1 | |
| Elementary School | 1307 | 31.3 | |
| Middle and High School | 1525 | 36.5 | |
| College and Above | 464 | 11.1 | |
| Season (%) | |||
| Spring | 1118 | 26.8 | |
| Summer | 1561 | 37.4 | |
| Fall | 1236 | 29.6 | |
| Winter | 260 | 6.2 | |
| Geographical Location (%) | |||
| Ansan | 1567 | 37.5 | |
| Ansung | 2608 | 62.5 | |
| Physical Activity (%) | |||
| No | 2982 | 71.4 | |
| Yes | 1193 | 28.6 | |
| Alcohol Consumption (%) | |||
| Never | 2356 | 56.4 | |
| Former | 318 | 7.6 | |
| Moderate Drinker | 1166 | 27.9 | |
| Heavy Drinker | 335 | 8.0 | |
| Smoking Status (%) | |||
| Never | 2750 | 65.9 | |
| Former | 1007 | 24.1 | |
| Current | 418 | 10.0 | |
| Diabetes Mellitus (%) | |||
| No | 3255 | 78.0 | |
| Yes | 920 | 22.0 | |
| Hypertension (%) | |||
| No | 1977 | 47.4 | |
| Yes | 2198 | 52.7 | |
| Cerebrovascular Disease | |||
| No | 3876 | 92.8 | |
| Yes | 299 | 7.2 | |
| Hyperlipidemia (%) | |||
| No | 2341 | 56.1 | |
| Yes | 1834 | 43.9 | |
| Cancer (%) | |||
| No | 3688 | 88.3 | |
| Yes | 487 | 11.7 | |
| K-MMSE Score | 25.9 | 3.6 | |
| K-MMSE Category (%) b | |||
| Normal Cognitive Function | 3249 | 77.8 | |
| Decreased Cognitive Function | 926 | 22.2 | |
| Average Values | PM2.5 (µg/m3) | PM10 (µg/m3) | ||
|---|---|---|---|---|
| Mean | Standard Deviation | Mean | Standard Deviation | |
| 1-Day | 26.0 | 13.0 | 47.0 | 21.3 |
| 2-Day | 26.0 | 11.8 | 46.6 | 19.0 |
| 3-Day | 25.9 | 10.7 | 46.5 | 17.5 |
| 4-Day | 25.9 | 9.8 | 46.7 | 16.6 |
| 5-Day | 25.9 | 9.1 | 46.9 | 15.4 |
| 6-Day | 25.9 | 8.5 | 47.1 | 14.6 |
| 1-Week | 25.9 | 8.0 | 47.2 | 13.9 |
| 8-Day | 25.8 | 7.6 | 47.2 | 13.3 |
| 9-Day | 25.7 | 7.3 | 47.1 | 12.7 |
| 10-Day | 25.7 | 7.2 | 47.2 | 12.5 |
| 11-Day | 25.7 | 7.1 | 47.2 | 12.4 |
| 12-Day | 25.7 | 7.0 | 47.2 | 12.4 |
| 13-Day | 25.7 | 7.0 | 47.2 | 12.4 |
| 2-Week | 25.8 | 7.0 | 47.3 | 12.4 |
| 1-Month | 26.3 | 6.2 | 48.1 | 10.8 |
| 3-Month | 27.2 | 5.4 | 50.2 | 9.2 |
| 6-Month | 28.2 | 4.7 | 52.0 | 5.9 |
| 1-Year | 27.7 | 4.1 | 50.6 | 2.6 |
| 2-Year | 28.1 | 4.3 | 51.5 | 3.0 |
| 3-Year | 28.7 | 4.4 | 52.4 | 3.5 |
| Average Variables | PM2.5 (µg/m3) | PM10 (µg/m3) | ||||||
|---|---|---|---|---|---|---|---|---|
| r | p-Value | Age-Adjusted r | p-Value | r | p-Value | Age-Adjusted r | p-Value | |
| 1-Day | −0.06 | 0.0002 | −0.02 | 0.24 | 0.002 | 0.89 | 0.01 | 0.35 |
| 2-Day | −0.08 | <0.0001 | −0.04 | 0.02 | −0.01 | 0.37 | 0.0003 | 0.99 |
| 3-Day | −0.10 | <0.0001 | −0.05 | 0.001 | −0.02 | 0.17 | −0.01 | 0.74 |
| 4-Day | −0.10 | <0.0001 | −0.06 | 0.0003 | −0.02 | 0.20 | −0.004 | 0.81 |
| 5-Day | −0.11 | <0.0001 | −0.06 | 0.0003 | −0.02 | 0.26 | −0.002 | 0.90 |
| 6-Day | −0.11 | <0.0001 | −0.05 | 0.001 | −0.02 | 0.21 | 0.002 | 0.92 |
| 1-Week | −0.11 | <.0001 | −0.05 | 0.001 | −0.02 | 0.24 | 0.01 | 0.70 |
| 8-Day | −0.12 | <0.0001 | −0.06 | 0.0003 | −0.02 | 0.14 | 0.01 | 0.74 |
| 9-Day | −0.13 | <0.0001 | −0.06 | <0.0001 | −0.03 | 0.06 | 0.002 | 0.91 |
| 10-Day | −0.14 | <0.0001 | −0.06 | <0.0001 | −0.03 | 0.04 | 0.003 | 0.83 |
| 11-Day | −0.14 | <0.0001 | −0.07 | <0.0001 | −0.03 | 0.03 | 0.004 | 0.79 |
| 12-Day | −0.14 | <0.0001 | −0.07 | <0.0001 | −0.04 | 0.02 | 0.005 | 0.77 |
| 13-Day | −0.14 | <0.0001 | −0.07 | <0.0001 | −0.03 | 0.02 | 0.004 | 0.78 |
| 2-Week | −0.14 | <0.0001 | −0.06 | <0.0001 | −0.03 | 0.03 | 0.01 | 0.73 |
| 1-Month | −0.16 | <0.0001 | −0.06 | 0.0002 | −0.04 | 0.02 | 0.02 | 0.22 |
| 3-Month | −0.18 | <0.0001 | −0.05 | 0.002 | −0.02 | 0.22 | 0.05 | 0.001 |
| 6-Month | −0.22 | <0.0001 | −0.07 | <0.0001 | −0.04 | 0.01 | 0.04 | 0.01 |
| 1-Year | −0.32 | <0.0001 | −0.18 | <0.0001 | −0.29 | <0.0001 | −0.16 | <0.0001 |
| 2-Year | −0.35 | <0.0001 | −0.19 | <0.0001 | −0.33 | <0.0001 | −0.18 | <0.0001 |
| 3-Year | −0.35 | <0.0001 | −0.19 | <0.0001 | −0.34 | <0.0001 | −0.19 | <0.0001 |
| Average Value | Interquartile Range | Effect Size a | Standard Error a | p-Value | 95% Confidence Interval | P for Linearity b | ||
|---|---|---|---|---|---|---|---|---|
| PM2.5 (µg/m3) | ||||||||
| 1-Day | 15.7 | −0.05 | 0.06 | 0.39 | −0.16 | 0.06 | 0.70 | |
| 2-Day | 13.6 | −0.10 | 0.05 | 0.07 | −0.20 | 0.01 | 0.30 | |
| 3-Day | 13.0 | −0.16 | 0.06 | 0.005 | −0.28 | −0.05 | 1.00 | |
| 4-Day | 12.3 | −0.20 | 0.06 | 0.001 | −0.32 | −0.09 | 0.61 | |
| 5-Day | 11.7 | −0.23 | 0.06 | 0.0004 | −0.35 | −0.10 | 1.00 | |
| 6-Day | 11.5 | −0.24 | 0.07 | 0.0004 | −0.38 | −0.11 | 0.71 | |
| 1-Week | 11.2 | −0.27 | 0.07 | 0.0002 | −0.41 | −0.13 | 0.19 | |
| 8-Day | 10.4 | −0.28 | 0.07 | <0.0001 | −0.42 | −0.14 | 0.02 | |
| 9-Day | 10.1 | −0.30 | 0.07 | <0.0001 | −0.44 | −0.16 | 0.85 | |
| 10-Day | 9.6 | −0.31 | 0.07 | <0.0001 | −0.45 | −0.18 | 0.02 | |
| 11-Day | 9.3 | −0.34 | 0.07 | <0.0001 | −0.48 | −0.21 | 0.44 | |
| 12-Day | 9.1 | −0.36 | 0.07 | <0.0001 | −0.49 | −0.22 | 0.61 | |
| 13-Day | 9.3 | −0.38 | 0.07 | <0.0001 | −0.52 | −0.24 | 0.26 | |
| 2-Week | 9.3 | −0.38 | 0.07 | <0.0001 | −0.52 | −0.24 | 0.09 | |
| 1-Month | 8.4 | −0.49 | 0.08 | <0.0001 | −0.65 | −0.32 | 0.56 | |
| 3-Month | 7.6 | −0.68 | 0.11 | <0.0001 | −0.89 | −0.46 | 0.45 | |
| 6-Month | 7.9 | −0.84 | 0.12 | <0.0001 | −1.08 | −0.60 | 0.11 | |
| 1-Year | 7.3 | −0.82 | 0.15 | <0.0001 | −1.12 | −0.52 | 0.35 | |
| 2-Year | 8.9 | −1.24 | 0.21 | <0.0001 | −1.65 | −0.82 | 0.11 | |
| 3-Year | 9.4 | −1.16 | 0.23 | <0.0001 | −1.61 | −0.70 | 0.04 | |
| PM10 (µg/m3) | ||||||||
| 1-Day | 25.1 | 0.05 | 0.06 | 0.37 | −0.06 | 0.16 | 0.58 | |
| 2-Day | 22.0 | 0.01 | 0.06 | 0.86 | −0.10 | 0.12 | 0.17 | |
| 3-Day | 20.7 | −0.05 | 0.06 | 0.39 | −0.17 | 0.06 | 0.53 | |
| 4-Day | 19.6 | −0.08 | 0.06 | 0.19 | −0.20 | 0.04 | 0.33 | |
| 5-Day | 18.6 | −0.10 | 0.07 | 0.14 | −0.23 | 0.03 | 0.10 | |
| 6-Day | 17.8 | −0.10 | 0.07 | 0.17 | −0.24 | 0.04 | 0.53 | |
| 1-Week | 17.9 | −0.10 | 0.08 | 0.18 | −0.25 | 0.05 | 0.61 | |
| 8-Day | 18.3 | −0.13 | 0.08 | 0.12 | −0.29 | 0.03 | 0.15 | |
| 9-Day | 18.4 | −0.15 | 0.09 | 0.10 | −0.32 | 0.03 | 0.48 | |
| 10-Day | 17.6 | −0.13 | 0.09 | 0.14 | −0.30 | 0.04 | 0.65 | |
| 11-Day | 17.5 | −0.15 | 0.09 | 0.09 | −0.32 | 0.02 | 0.47 | |
| 12-Day | 17.9 | −0.17 | 0.09 | 0.06 | −0.35 | 0.01 | 0.15 | |
| 13-Day | 18.0 | −0.20 | 0.09 | 0.03 | −0.38 | −0.02 | 0.09 | |
| 2-Week | 18.2 | −0.21 | 0.09 | 0.02 | −0.39 | −0.03 | 0.12 | |
| 1-Month | 18.5 | −0.41 | 0.14 | 0.004 | −0.69 | −0.13 | 0.24 | |
| 3-Month | 16.0 | −0.63 | 0.18 | 0.001 | −0.99 | −0.27 | 0.20 | |
| 6-Month | 9.3 | −0.43 | 0.15 | 0.003 | −0.72 | −0.14 | 0.40 | |
| 1-Year | 4.7 | −0.46 | 0.12 | 0.0002 | −0.70 | −0.21 | 0.75 | |
| 2-Year | 6.1 | −0.76 | 0.16 | <0.0001 | −1.07 | −0.44 | 0.37 | |
| 3-Year | 7.2 | −0.85 | 0.18 | <0.0001 | −1.20 | −0.49 | 0.64 | |
| Average Variables | Interquartile Range | Effect Size a | Standard Error a | p-Value | Adjusted R2 | Order Entered for PM | Entered Order | |
|---|---|---|---|---|---|---|---|---|
| PM2.5 (µg/m3) | ||||||||
| 1-Day | 15.69 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 2-Day | 13.63 | −0.09 | 0.05 | 0.07 | 0.37 | 7 | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking, PM2.5 | |
| 3-Day | 13.02 | −0.14 | 0.05 | 0.01 | 0.38 | 7 | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking, PM2.5 | |
| 4-Day | 12.31 | −0.17 | 0.06 | 0.002 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 5-Day | 11.70 | −0.18 | 0.06 | 0.002 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 6-Day | 11.52 | −0.18 | 0.06 | 0.003 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 1-Week | 11.16 | −0.18 | 0.06 | 0.003 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 8-Day | 10.36 | −0.18 | 0.06 | 0.002 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 9-Day | 10.11 | −0.20 | 0.06 | 0.001 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 10-Day | 9.59 | −0.20 | 0.06 | 0.001 | 0.38 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 11-Day | 9.33 | −0.21 | 0.06 | 0.0003 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 12-Day | 9.04 | −0.21 | 0.06 | 0.0002 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 13-Day | 9.25 | −0.22 | 0.06 | 0.0002 | 0.38 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 2-Week | 9.30 | −0.21 | 0.06 | 0.0003 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 1-Month | 8.42 | −0.21 | 0.06 | 0.001 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM2.5, Smoking | |
| 3-Month | 7.60 | −0.15 | 0.07 | 0.02 | 0.37 | 7 | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking, PM2.5 | |
| 6-Month | 7.89 | −0.35 | 0.08 | <0.0001 | 0.38 | 5 | Education, Age, Physical Activity, Diabetes, PM2.5, Marital Status, Smoking, BMI | |
| 1-Year | 7.27 | −0.88 | 0.09 | <0.0001 | 0.39 | 4 | Education, Age, PM2.5, Physical Activity, Diabetes, Marital Status, Smoking, BMI | |
| 2-Year | 8.93 | −1.09 | 0.10 | <0.0001 | 0.39 | 3 | Education, Age, PM2.5, Physical Activity, Diabetes, Marital Status, Smoking, BMI | |
| 3-Year | 9.35 | −1.12 | 0.10 | <0.0001 | 0.39 | 3 | Education, Age, PM2.5, Physical Activity, Diabetes, Marital Status, Smoking, BMI | |
| PM10 (µg/m3) | ||||||||
| 1-Day | 25.07 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 2-Day | 21.98 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 3-Day | 20.70 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 4-Day | 19.64 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 5-Day | 18.59 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 6-Day | 17.82 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 1-Week | 17.94 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 8-Day | 18.30 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 9-Day | 18.37 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 10-Day | 17.57 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 11-Day | 17.50 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 12-Day | 17.92 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 13-Day | 18.01 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 2-Week | 18.22 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 1-Month | 18.49 | - | - | - | 0.37 | Not Entered | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking | |
| 3-Month | 15.95 | 0.27 | 0.08 | 0.001 | 0.37 | 6 | Education, Age, Physical Activity, Diabetes, Marital Status, PM10, Smoking | |
| 6-Month | 9.31 | 0.18 | 0.07 | 0.01 | 0.37 | 7 | Education, Age, Physical Activity, Diabetes, Marital Status, Smoking, PM10 | |
| 1-Year | 4.69 | −0.73 | 0.09 | <0.0001 | 0.38 | 3 | Education, Age, PM10, Physical Activity, Diabetes, Marital Status, Smoking, BMI | |
| 2-Year | 6.07 | −0.93 | 0.10 | <0.0001 | 0.39 | 3 | Education, Age, PM10, Physical Activity, Diabetes, Marital Status, Smoking, BMI | |
| 3-Year | 7.15 | −1.04 | 0.10 | <0.0001 | 0.39 | 3 | Education, Age, PM10, Physical Activity, Diabetes, Marital Status, Smoking, BMI | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.J.; Kim, J.H.; Song, D.S.; Lee, K. Effect of Short- to Long-Term Exposure to Ambient Particulate Matter on Cognitive Function in a Cohort of Middle-Aged and Older Adults: KoGES. Int. J. Environ. Res. Public Health 2022, 19, 9913. https://doi.org/10.3390/ijerph19169913
Lee JJ, Kim JH, Song DS, Lee K. Effect of Short- to Long-Term Exposure to Ambient Particulate Matter on Cognitive Function in a Cohort of Middle-Aged and Older Adults: KoGES. International Journal of Environmental Research and Public Health. 2022; 19(16):9913. https://doi.org/10.3390/ijerph19169913
Chicago/Turabian StyleLee, Jane J., Ji Hyun Kim, Dae Sub Song, and Kyoungho Lee. 2022. "Effect of Short- to Long-Term Exposure to Ambient Particulate Matter on Cognitive Function in a Cohort of Middle-Aged and Older Adults: KoGES" International Journal of Environmental Research and Public Health 19, no. 16: 9913. https://doi.org/10.3390/ijerph19169913
APA StyleLee, J. J., Kim, J. H., Song, D. S., & Lee, K. (2022). Effect of Short- to Long-Term Exposure to Ambient Particulate Matter on Cognitive Function in a Cohort of Middle-Aged and Older Adults: KoGES. International Journal of Environmental Research and Public Health, 19(16), 9913. https://doi.org/10.3390/ijerph19169913